")
Back to Journals » Vascular Health and Risk Management » Volume 19
Prevalence and Factors Associated with Hypertension Among HIV Positive Patients on Antiretroviral Therapy: A Hospital-Based Cross-Sectional Study in Rwanda
Authors Uwanyirigira D, Biracyaza E , Uzabakiriho I, Omolo J, Hakizayezu F, Nzayirambaho M
Received 26 September 2023
Accepted for publication 21 December 2023
Published 27 December 2023 Volume 2023:19 Pages 857—870
DOI https://doi.org/10.2147/VHRM.S442108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Donatha Uwanyirigira,1,2 Emmanuel Biracyaza,3,4 Innocent Uzabakiriho,2 Jared Omolo,5 François Hakizayezu,1 Manasse Nzayirambaho1
1Department of Epidemiology and Biostatistics, University of Rwanda, Kigali, Rwanda; 2Byumba District Hospital, Ministry of Health, Byumba, Rwanda; 3School of Rehabilitation, Faculty of Medicine, Université de Montréal, Quebec, Montréal; 4Center for Interdisciplinary Research in Rehabilitation of Greater Montreal (CRIR), Institut Universitaire Sur la Réadaptation En Déficience Physique de Montréal, Quebec, Canada; 5Field Epidemiology Training Program (FELTP), Centers for Disease Control and Prevention (CDC) in Rwanda, Kigali, Rwanda
Correspondence: Donatha Uwanyirigira, Tel +250788459752, Email [email protected]
Introduction: The human immunodeficiency virus (HIV) and the use of antiretroviral therapy (ART) are influential elements contributing to hypertension, which is a public health concern particularly in sub-Saharan Africa where its underdiagnosis and limited investigation persist. Moreover, hypertension prevails at higher rates among individuals living with HIV (PLWH) in comparison to the general population. Therefore, our study determined the prevalence of hypertension and its associated factors among PLWH who are undergoing ART treatment at Byumba District Hospital.
Methods: A cross-sectional study design was conducted among 406 PLWH over the age of 14 years who were undergoing ART within the HIV department. We performed statistical analyses using STATA version 13. Significant independent variables identified in the bivariate analysis were further exported in a multivariable logistic regression model to ascertain their association with hypertension. This model elucidated factors associated with hypertension, presenting outcomes through odds ratios and their respective 95% confidence intervals, with statistical significance set at p < 0.05.
Results: The prevalence of hypertension was 24.7%, which means that roughly 1 in 4 PLWH were hypertensive. Notably, individuals aged 41 years and above demonstrated a significant association with heightened hypertension [AOR = 4.49; 95% CI = 2.45– 8.21, p < 0.001] in contrast to those aged between 14 and 40 years. Additionally, smokers [AOR = 12.12; 95% CI = 4.48– 32.74, p < 0.001] and individuals with a family history of hypertension [AOR = 4.28; 95% CI = 1.01– 18.13, p = 0.049] demonstrated a higher likelihood of hypertension than their counterparts. Moreover, alcohol consumers [AOR = 5.5; 95% CI = 2.75– 10.9, p < 0.001] had an increased likelihoods of hypertension compared to non-drinkers. Lastly, diabetics were almost 6 times more likely to be hypotensive [AOR = 4.50; 95% CI = 2.55– 7.95, p = 0.018] when compared to those without diabetes.
Conclusion: Our findings strongly underscore the urgency for the implementation of targeted programs aimed at enhancing awareness and comprehension of the factors and potential complications tied to hypertension among PLWH. Such programs could be integrated into routine HIV care services to provide patients with the information and skills required to manage their hypertension effectively.
Keywords: hypertension, prevalence, people with human immunodeficiency virus, antiretroviral therapy, Byumba hospital
Introduction
The Human Immunodeficiency Virus (HIV) poses a significant global public health threat, with its increasing association with cardiovascular complications, cerebral-vascular incidents, and vasculopathy over the past two decades.1 These HIV-related complications contribute to elevated mortality and morbidity rates in both developed and developing countries.2,3 Hypertension, a top contributor to cardiovascular diseases and a global leading cause of death, is notably prevalent among individuals with diabetes, with over 45% of diabetic patients succumbing to complications related to hypertension.4–6 To combat this health concern, antiretroviral therapy (ART) plays a essential role in enhancing the quality of life for people living with HIV (PLWH).7,8 Globally, recent reports indicated 38.4 million people living with HIV (PLWH) of which 25.4 million PLWH access to ART. This pandemic remains harmful in Sub-Saharan African (SSA) region where one in 25 adults has been living with HIV accounting two-thirds of global cases.9,10 Prior studies stated that hypertension remains inadequately addressed and diagnosed within the rural areas from SSA.7,8 Additionally, studies have shown that individuals on ART are prone to alterations in lipoprotein density cholesterol (HDL) or high-density lipoprotein levels, elevating their hypertension risk.11 The target to achieve the third Sustainable Development Goal (SDG-3) is to reduce HIV/AIDS prevalence by 90% by 2030. This necessitates intensive efforts on hypertension management and the spread of sexually transmissible infections.12
Although the prevalence of hypertension among PLWH is relatively lower in SSA and Asia compared to North America, Europe, and South America, the impact is more pronounced in SSA.8,13 The World Health Organization (WHO) forecasts an increase in non-communicable diseases (NCDs), with hypertension driving complications such as diabetes, stroke, and ischemic heart diseases.8 While only 16.2% of individuals in SSA countries have hypertension, a significant proportion consists of HIV-positive patients.7,14 In Rwanda, hypertension prevalence was 15.6%, rising with age.15,16
Earlier research has comprehensively documented a range of factors that contribute to hypertension among PLWH. These factors encompass various behavioural aspects, including poor nutritional habits, non-compliance with prescribed treatments, alcohol consumption, and smoking.17,18 Moreover, the frequencies of clinical visits and engagement in physical activity, including sports participation, have been recognized as contributing factors.19,20 Socio-demographic factors, such as place of residence or urbanization, age, gender, education, and marital status, also influence the occurrence of hypertension among PLWH. For instance, hypertension tends to be more prevalent among adult PLWH compared to their younger counterparts.21 This health concern is intricately linked with clinical factors, such as longer duration of HIV infection, a family history of hypertension, low CD4 cell count, elevated viral loads, diabetes, an extended duration of HIV infection, and specific medication use, often in conjunction with ART.22,23 Additionally, a higher body mass index has been identified as another risk factor for hypertension. Notably, the utilization of ART has previously been acknowledged as a contributing factor underlying hypertension among PLWH.7,24
Previous studies underscore the fact that a considerable number of individuals are unaware of their hypertension status.19,25 Rwanda is positioned among countries undergoing developmental transitions, with a heightened focus on the epidemiology of hypertension. This health concern has been recognized as a multifaceted catalyst for diverse health complications, contributing to increased morbidity and mortality in the absence of early preventive measures and treatments. Within the Rwandan population, a study conducted in 2013 revealed a prevalence of 36.1% of cardiovascular disease (CVD) among workers, of which approximately 33% were unaware of their hypertension diagnosis.15 Moreover, the context of HIV infection has shown associations with subclinical atherosclerosis indicators, including markers of endothelial dysfunction, escalated arterial stiffness, and atherosclerotic progression.26,27 These factors collectively increase the vulnerability of individuals to hypertension, particularly when combined with other recognized hypertension risk factors, such as being aged 45 years and above, being male, engaging in smoking and alcohol use, grappling with obesity and diabetes, maintaining a sedentary lifestyle, and possessing a family history of hypertension.28–30
Poorly controlled hypertension stands as a significant contributor to cardiovascular disease not only in HIV patients but also general population of sub-Sahara Africa.31,32 This exerts a profound impact on overall health outcomes.33 The increasing adoption and adherence to ART among PLWH might hold potential in addressing this prevalent health issue. As hypertension is a substantial risk factor of cardiovascular disease, understanding its prevalence and its determinants among PLWH assumes paramount importance for policymakers and the affected community. Yet, despite the awareness of hypertension as a public health concern, a critical research gap persists particularly in the rural settings of Rwanda. This study aims to fill this critical gap by rigorously examining the prevalence of hypertension and its associated factors among HIV patients at Gicumbi District Hospital. By researching into this underexplored area, our purpose is to establish a deeper understanding and potentially uncover essential insights that can inform targeted interventions and healthcare strategies tailored to this specific population.
Methods
Study Design
A hospital-based cross-sectional study was conducted among all people with HIV attending ART in the department of HIV at the Byumba District Hospital located in Gicumbi District.
Study Settings and Participants
The study was conducted at Byumba District Hospital in Gicumbi District whereas this District is located in Northern Province of Rwanda. Byumba District Hospital oversees 25 health centres; this District Hospital is located in Byumba District, Northern Province of Rwanda, which accommodates a population of 428,203 segmented into 21 administrative Sectors. As for the inclusion criteria, the study encompassed PLWH who were at least 14 years of age and had been on ART for a minimum of 6 months within the study area. Those who declined participation for any reason, and individuals with incomplete information in their medical records were also excluded.
Sample Size
We used Cochran formula to determine a sample size for this study.34 This formula was applied in consideration of the following statistical parameters; 95% of confidence intervals (zα/2=1.96), 5% of statistical significance (d = 0.05), 5% non-response rate, and taking the prevalence (50%) of hypertension (p = 0.50, q = 1-p). Hence, the total sample size of 406 participants was randomly enrolled in this study from 669 HIV positive on ART who were under ART at Byumba District Hospital.
Data Collection
Data collection was performed by the general nurse under supervision of the first author of this study. In addition to that, a simple random sampling technique was used to recruit study participants during their follow-up visits; the study participants were drawn by lottery from the total patients on follow-up from their registries.
Study Variables
Dependent variable of the study is hypertension status (having hypertension according to the definition or not having hypertension). Hypertension is according to self-reported ongoing antihypertensive treatment, or systolic blood pressure (SBP ≥ 140 mmHg) and diastolic blood pressure (DBP ≥ 90 mmHg).35 Our independent variables included socio-demographic variables (such as age, sex, religion, education level, marital status, occupation and social category,36 behavioral variables such as smoking and alcohol use. Social category (also known as Ubudehe category) refers to a traditional classification system in Rwanda used to categorize households based on socio-economic status. This classification helps in identifying vulnerable households and allocating resources and support accordingly. The categories range from 1 to 4, with the first category representing the most economically challenged households and the fourth category representing the most prosperous ones. This system also plays a significant role in various aspects of social welfare, resource allocation, and development programs in Rwanda.37 Smokers were defined as those who had consumed at least one cigarette or other local tobacco product within the previous 24 months before the data collection. Based on the frequency and volume of alcohol consumed during a normal drinking week, alcohol consumption was dichotomously classified as yes (for those who consume alcohol) and no (who never consume alcohol).
After at least 15 minutes of relaxation, we adopted a sitting position and used an automatic or validated oscillometer device to measure (OMRON HEM-7322U) SBP and DBP. In accordance with the 2018 ESC recommendations, three measures were made in each arm at 5-minute intervals.35 Weight of the study participant was measured in light clothing and without shoes, and height was calculated to the nearest 0.1 cm using a stadiometer. Weight (kg)/height was used to determine the body mass index (BMI) (m2). BMI was divided into four categories: underweight (BMI = 18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (BMI=25-29.9 kg/m2), and obese (BMI = 30 kg/m2). According to the WHO 2020 guidelines, adequate physical activity is defined as 150 minutes of moderate or vigorous activity each week, or at least 75 minutes of each.8 In our study, we used “Physical Activity Logs or Diaries” to gauge the physical activities of our research participants. These logs served as a means for participants to meticulously document their daily or weekly activities, noting the duration and intensity of each. This method enabled us to ascertain whether individuals were actively involved in physical activities (recorded as 1 = active) or not (recorded as 0 = less active). The assessment of these logs involved specific criteria: (a) the frequency of participation in physical activities, (b) the duration of each activity session, (c) the intensity level of the activities, (d) ensuring that the recorded activities aligned with the definition of physical activity (eg, exercises, sports, recreational pursuits, household chores, walking), and (e) the consistency of participants in engaging in physical activities within a predetermined timeframe (eg, weekly) to qualify as regular practitioners. Further, we categorized individuals as physically active if they met the following conditions: (a) involvement in physical activities on a minimum of 3 days per week, (b) each activity session lasting at least 20 minutes, and (c) participation in activities ranging from moderate to vigorous intensity. In addition to physical activity, diabetes was defined as having a fasting blood glucose level of 126 mg/dL (7 mmol/L)38 or higher, or if you are currently taking diabetes medication. Clinical data such as HIV infection duration, ART duration, HIV clinical stages, and ART regimen types were collected. Respondents with viral loads of 1000 copies/mL were considered to have viral suppression, whereas viral loads of 50 copies/mL are considered undetectable Further, a self-report questionnaire was used to collect socio-demographic and behavioural variables. Clinical examinations and laboratory tests (such as viral loads, CD4, and ART regimen) were performed. Clinical data were extracted from the medical records from HIV unit.
Statistical Analyses
The data from the field was entered into an excel sheet. The STATA version 13 was used for descriptive and analytical analyses. Descriptive statistics were used to summarize, organize sample characteristics, describe research variables and document response rate where frequency tables were presented. Cross tabulations and proportions between independent and dependent variables were performed. Bivariate logistic regression analysis was performed based on crude odds ratios (COR) to examine the significant variables of hypertension among study participants. Additionally, all statistical significant variables in bivariate logistic regression analysis were exported into multivariate logistic regression models that determined the adjusted odds ratios for the factors associated with hypertension. The significance of the findings was set at p < 0.05 and 95% of confidence intervals was considered.
Results
Basic Characteristics of the Study Participants
A total of 406 PLWH took part in this study. The average age of the participants was 37.91 age (SD = 2.12). A notable proportion (50.5%) of these participants fell into the age group of 40 years or younger. The sex distribution showed that the majority (52.2%, n = 212) were females, while approximately three-quarters (75.4%) were engaged in farming activities as their primary source of income. In terms of religious affiliation, a significant percentage (84.4%) identified as Christians, and more than half (56.9%) were married. Educational background analysis revealed that nearly 68% of the PLWH had received primary school education. Additionally, findings indicated that 35.9% of the participants were consumers of alcohol, 7.4% were smokers, 28.6% reported being physically inactive, and 46.1% were classified as overweight or obese. Furthermore, the study unveiled that 62.3% of the participants had been living with HIV for more than 3 years, and 67.5% had been on ART for over a year. Ultimately, the study reported a prevalence of hypertension at 22.4% (Table 1).
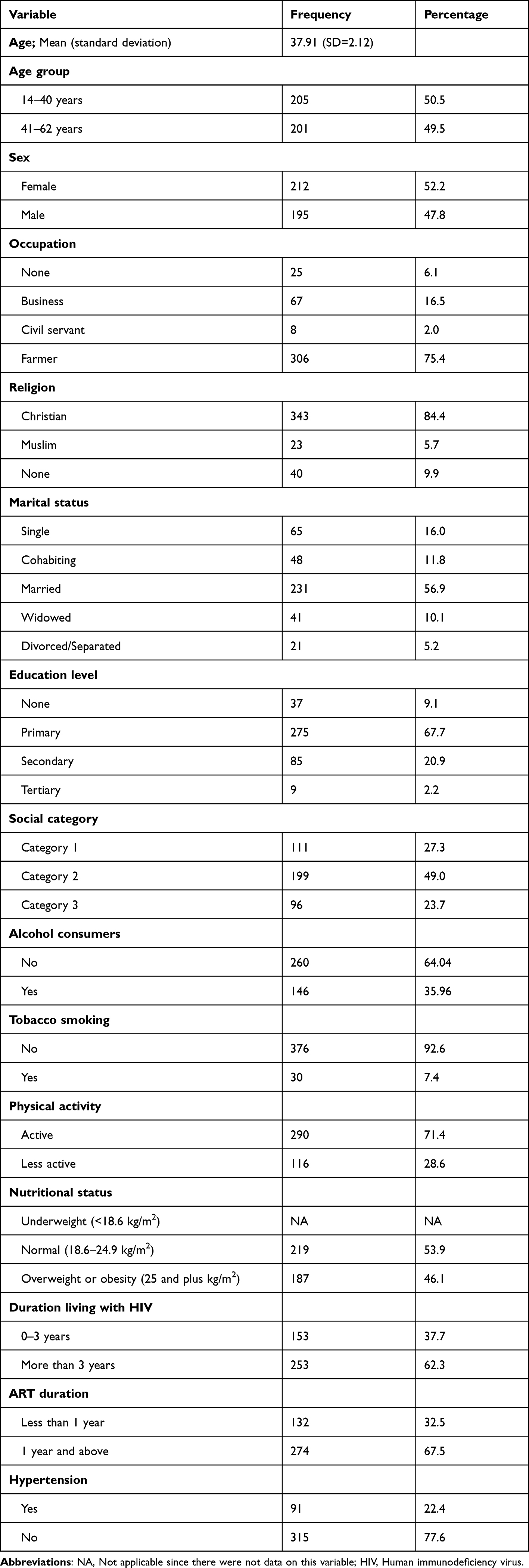 |
Table 1 Descriptive Statistics of Socio-Demographic, Lifestyle and Clinical Characteristics of the Study Participants (n=406) |
Prevalence and Bivariate Analysis of Factors Associated with Hypertension
Our results from the bivariate logistic regression analyses revealed significant associations between hypertension and variables including that age, BMI, smoking, alcohol use, living with diabetes and family history of hypertension. Being aged over 41 years was notably associated with an increase hypertension risk [COR = 3.29; 95% CI = 1.98–5.46] compared to those under 41 years. Smoking [COR = 12.24; 95% CI (5.23; 28.63)] and alcohol use [COR = 2.33; 95% CI = 1.45–3.75] were significantly associated with hypertension. Further, PLWH with overweight or obesity presented a significant association with hypertension [COR = 3.29; 95% CI = 1.98–5.46] relative to those without excess weight. Individuals with a history of diabetes were more prone to hypertension [COR = 2.1; 95% CI = 1.83–5.8] than their counterparts without such a diagnosis (Table 2).
 |
Table 2 Prevalence of Hypertension by Socio-Demographic, Lifestyle and Clinical Characteristics and Bivariate Analysis of Factors Associated Hypertension |
Multivariate Logistic Regression Models for the Associated Factors of Hypertension
The findings from multivariate logistic regression models demonstrated that BMI, age, family history of hypertension, smoking, and living with diabetes were noteworthy risk factors associated with hypertension. Specifically, individuals aged 41 years and older showed significantly greater odds of hypertension in comparison to those aged between 14 and 40 years [AOR = 4.49; 95% CI = 2.45–8.21, p < 0.001]. Further, smokers were more likely to be hypertensive [AOR = 12.12; 95% CI = 4.48–32.74, p < 0.001] compared to non-smokers counterparts. Those who reported alcohol consumption were nearly six times more likely to experience hypertension [AOR = 5.5; 95% CI = 2.75–10.9, p < 0.001] than non-consumers of alcohol. Similarly, individuals with a family history of hypertension were at higher likelihoods to be hypertensive [AOR = 4.28; 95% CI = 1.01–18.13, p = 0.049] than those without such a history. Additionally, diabetics were nearly 6 times more likely to experience hypertension [AOR = 4.50; 95% CI = 2.55–7.95, p = 0.018] than their counterparts. Lastly, PLWH with overweight or obesity presented almost more likelihoods to be hypertensive [AOR = 1.91; 95% CI = 1.11–3.3, p = 0.020] compared to those with normal BMI. Regarding clinical data, the results on CD4 indicated that patients with >400 copies/mL [AOR = 0.84; 95% CI = 0.71–0.99, p < 0.001] and 200–400 copies/mL [AOR = 0.62; 95% CI = 0.43–0.89, p < 0.001] had lower likelihoods of hypertension compared to those with <200 copies/mL. However, our findings showed that hypertension was not associated with VL and ART regimen (Table 3).
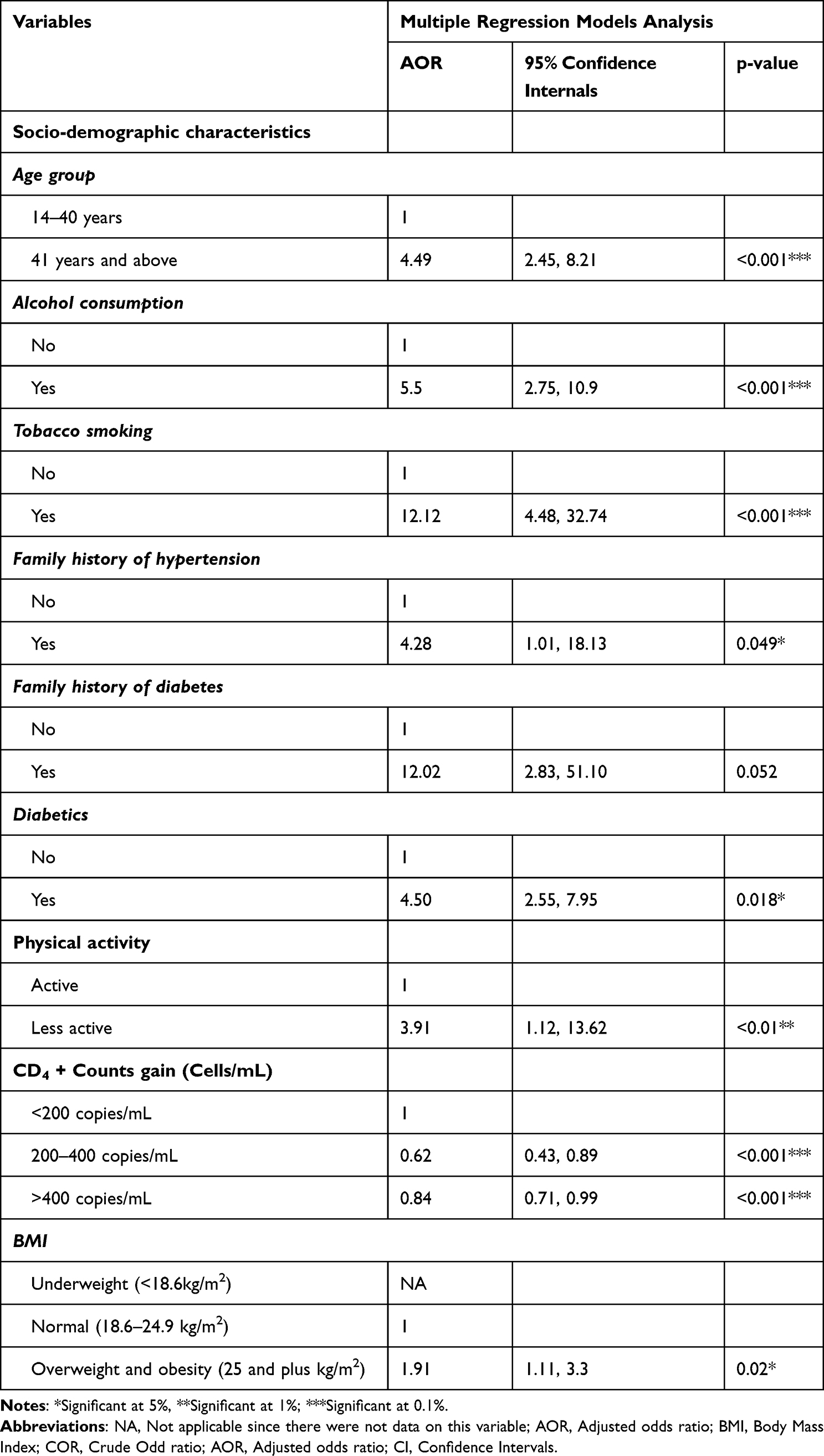 |
Table 3 Multivariate Analysis for the Associated Factors of Hypertension in PLWH |
Discussion
The prevalence of hypertension was 22.4% which is higher than the prevalence reported in Burundi, Tanzania, Uganda, among individuals living with HIV.5,7,38,39 The prevalence was significantly highly prevalent in men than in females. Further, our results indicated that the prevalence of hypertension is higher among people aged more than 41 years. These results are comparable to the previous documented a high prevalence of hypertension among HIV positive patient.40–42 These results highlight the disparity in the magnitude of hypertension among persons living with HIV in SSA countries which may associated with a number of reasons such as genetic and socio-economic conditions, duration of disease and clinical outcomes, behavioural issues, types of therapies received and study settings. These results collaborated with the prior studies.7,22,43
Among the participants whose blood pressure was measured before the survey, approximately 15% exhibited elevated hypertension levels, falling within a risky weight range. Notably, individuals categorized as overweight or obese demonstrated a higher likelihood of hypertension in comparison to those with a normal BMI. These findings are consistent with earlier research that reported that individuals with a obesity or overweight were more likely to be hypertensive26,44 whereas those with underweight were a lower risk to experience hypertension compared those with normal weight.7,26,45 These outcomes align with prior studies that have also highlighted an increased hypertension risk among HIV patients who are overweight or obese when contrasted with those with a normal BMI.46,47 Moreover, the prevalence of hypertension was significantly higher among participants aged 40 and above. These results were in concurrence with the conclusions drawn by several other researchers.29,48 This implies that individuals aged 41 or older greater likelihoods of developing hypertension than those who were younger, aligning with the observations of other researchers who also noted a substantial rise in blood pressure starting from the age of 40.43,49
Our findings indicated that smokers were at a higher likelihoods developing hypertension than the non-smokers. These results are consistent with previous research,41,50,51 although they differ from the findings of a study conducted in Burundi.7 Further, our results revealed that participants with diabetes had greater odds to be hypertensive than their counterparts. These results are in alignment with findings from earlier studies.7,48,52 Interestingly, our study did not identify a noteworthy association between hypertension and factors such as gender, education, marital status, and social category. Nevertheless, these factors have been previously published as risk factors for hypertension.23,41 It is plausible that the absence of such an association could be attributed to the limitations of a relatively small sample size and the nature of our cross-sectional institutional study. While prior studies reported that duration under ART contribute as a factor of hypertension,53 our study found no association between duration and hypertension.
Our findings uncovered a surprising inverse relationship between CD4 counts and hypertension among our HIV patient cohort, wherein individuals with CD4 counts exceeding 400 copies/mL and those within the range of 200–400 copies/mL exhibited a notably reduced likelihood of hypertension compared to those with counts below 200 copies/mL. These results align with previous studies54 that have suggested a potential link between higher CD4 counts and a diminished risk of hypertension. Additionally, our analysis of VL revealed no significant association with hypertension, contrary to some prior research.55 Despite existing literature proposing ART regimens as potential contributors to hypertension among HIV patients,56 our study did not establish a significant correlation between specific ART regimens and hypertension. Understanding these divergent trends between VL and CD4 counts concerning hypertension in HIV patients could benefit from an exploration of existing literature focused on the intricate interplay between immune status, VL, and cardiovascular health outcomes within similar populations. Comparatively, exploring studies that examine the influence of VL and varied ART strategies on hypertension in HIV populations might offer additional perspectives or confirmatory evidence to contextualize our findings.
Strengths and Limitations
This study has a significant strength due to its substantial sample size and its innovative nature within the health facility from the rural area. Notably, our research derives its conclusions from a sample that is representative of individuals aged between 14 and 41 years in the study area. While these strengths are commendable, it is essential to acknowledge certain limitations that warrant discussion. Firstly, the authors could not generalise the findings to all people with HIV in Rwanda because it was a hospital-based study. Secondly, a cross-sectional design of this study impedes its capacity to establish causal relationships between hypertension and its associated factors. Thirdly, certain crucial factors such as socio-demographic variables (eg, place of residence), comorbidities, clinical aspects (such as stroke, viral loads, ART regimen, CD4 counts), psychological influences, socio-cultural factors, and nutritional considerations were not included in our data collection. Lastly, the limitation lies in the small count of participants below the age of 40. This resulted in the formation of two age brackets: one encompassing 14 to 40-year-olds as adolescents and young adults, and the other involving individuals above 40 years old categorized as adults. This grouping of adolescents and adults within the first age group is conceded as a limitation.
Conclusions
Our study constitutes the initial documentation of a significantly heightened occurrence of hypertension among individuals living with HIV. Our findings have illuminated the jeopardy that hypertension imposes upon HIV-positive individuals in the investigated region. The results we have derived signify that hypertension stands as a formidable public health concern for PLWH within the rural facility where our study was conducted. We have founded that age, smoking, alcohol consumption, smoking, overweight and obesity, as well as living with diabetes, emerge as pivotal factors contributing to the prevalence of hypertension in this population. These findings accentuate the importance for the integration of hypertension management into the routine care provided to individuals with HIV. Such integration holds the potential to mitigate adverse ramifications and enhance cardiovascular well-being among those undergoing ART. Besides, longitudinal studies are recommended to explore how incidence of hypertension changes over-time, and examine causality of hypertension and identify additional factors of hypertension. There is a need of the research on the impact of specific ART regimens on the development, management of hypertension. This could involve investigating whether certain types of antiretroviral medications or combinations are more strongly linked to hypertension, as well as considering how the duration of ART might affect hypertension. This will provide valuable insights for healthcare providers in tailoring treatment plans and interventions for HIV-positive patients with hypertension.
Data Sharing Statement
The datasets used and/or analysed during this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Informed consent was obtained from all participants involved in this study. Participants aged 18 years or older provided both oral and written informed consent forms before their inclusion in the research. For participants below 18 years old, their assent to participate to the study was obtained alongside consent forms from their caregivers. Ethics approval for this study was granted by the Institutional Review Board of the College of Medicine and Health Sciences at the University of Rwanda (reference number: 378/CMHS IRB/2018). The study adhered to the principles outlined in the Helsinki Declaration. Further, authorization for the study was also acquired from the Ministry of Health through Rwanda Biomedical Center (RBC), which facilitated the provision of informed consent forms on behalf of the participants. Prior to data collection, the researchers provided a comprehensive explanation of the study’s objectives, potential benefits, and the selection criteria to the participants. They were explicitly informed of their right to withdraw from the research at any point without facing any consequences. Throughout the data collection process, strict adherence to confidentiality measures was ensured. All data collection procedures were conducted anonymously and in line with ethical standards.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Authors declare that they have no competing interests.
References
1. Bello SI, Ojieabu WA. Hypertension and related risk factors among clients on combined antiretroviral therapy in Nigeria. J Pharm Pharma Sci. 2017;9(4):4–10. doi10.21065/1920-4159.1000252
2. World Health Organization (WHO). HIV/AIDS Fact Sheet; 2021. Available from: http://www.who.int/news-room/fact-sheets/detail/hiv-aids.
3. Seidu A-A, Opoku Ahinkorah B, Louis Kobina Dadzie JKT, et al. A multi-country cross-sectional study of self-reported sexually transmitted infections among sexually active men in sub-Saharan Africa. BMC Public Health. 2020;20:1884. doi:10.1186/s12889-020-09996-5
4. Rücker SCM, Tayea A, Bitilinyu-Bangoh J, et al. High rates of hypertension, diabetes, elevated low-density lipoprotein cholesterol, and cardiovascular disease risk factors in HIV-infected patients in Malawi. Aids. 2018;32(2):253–260. doi:10.1097/QAD.0000000000001700
5. Lubega G, Mayanja B, Lutaakome J, Abaasa A, Thomson R, Lindan C. Prevalence and factors associated with hypertension among people living with HIV/AIDS on antiretroviral therapy in Uganda. Pan Afr Med J. 2021;38. doi:10.11604/pamj.2021.38.216.28034
6. Diouf A, Cournil A, Ba-Fall K, et al. Diabetes and hypertension among patients receiving antiretroviral treatment since 1998 in senegal: prevalence and associated factors. Isrn Aids. 2012;2012:1–8. doi:10.5402/2012/621565
7. Harimenshi D, Niyongabo T, Preux PM, Aboyans V, Desormais I. Hypertension and associated factors in HIV-infected patients receiving antiretroviral treatment in Burundi: a cross-sectional study. Sci Rep. 2022;12(1):1–8. doi:10.1038/s41598-022-24997-7
8. Abbafati C, Abbas KM, Abbasi-Kangevari M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1223–1249. doi:10.1016/S0140-6736(20)30752-2
9. Badacho AS, Mahomed OH. Prevalence of hypertension and diabetes and associated risk factors among people living with human immunodeficiency virus in Southern Ethiopia. Front Cardiovasc. 2023;10:1173440. doi:10.3389/fcvm.2023.1173440
10. World Health Organization. Estimated Number of People (All Ages) Living with HIV; 2022. Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/estimated-number-of-people--living-with-hiv#:~:text=SituationandtrendsIn2022,–31.2million%5Din.
11. Yunan X. A Global Prevalence of Hypertension Among People Living with HIV: A Systematic Review. Univ Florida, Gainesv; 2017.
12. Assefa Y, Gilks CF. Ending the epidemic of HIV/AIDS by 2030: will there be an endgame to HIV, or an endemic HIV requiring an integrated health systems response in many countries? Lancet. 2022;100:273–277. doi:10.1016/j.ijid.2020.09.011
13. Nduka C, Stranges S, Sarki AM, et al. Evidence of increased blood pressure and hypertension risk among people living with HIV on antiretroviral therapy: a systematic review with meta-analysis. J Hum Hypertens. 2015;30(6):355–362. doi:10.1038/jhh.2015.97
14. Manavalan P, Madut DB, Hertz JT, et al. Hypertension burden and challenges across the hypertension treatment cascade among adults enrolled in HIV care in northern Tanzania. J Clin Hypertens. 2020;22(8):1518–1522. doi:10.1111/jch.13929
15. Nahimana M-R, Nyandwi A, Muhimpundu MA, et al. A population-based national estimate of the prevalence and risk factors associated with hypertension in Rwanda: implications for prevention and control. BMC Public Health. 2018;18(2):1–11. doi:10.1186/s12889-017-4536-9
16. Sander L, Newell K, Ssebbowa P, et al. Hypertension, cardiovascular risk factors and antihypertensive medication utilisation among HIV-infected individuals in Rakai, Uganda; 2015:20.
17. Van Zoest RA, Van Den Born BJH, Reiss P. Hypertension in people living with HIV. Curr Opin HIV AIDS. 2017;12(6):513–522. doi:10.1097/COH.0000000000000406
18. Cosimo M. Lifestyle and hypertension: an evidence-based review. J Hypertens Manag. 2018;4:1.
19. Yao L, Lu M, Dai H, et al. Lifestyle and risk of hypertension: follow-up of a young pre-hypertensive cohort. Int J Med Sci. 2015;12(7):605–612. doi:10.7150/ijms.12446
20. Akinlua JT, Meakin R, Umar AM, Freemantle N, Reboldi G. Current prevalence pattern of hypertension in Nigeria: a systematic review. PLoS One. 2015;10(10):1–18. doi:10.1371/journal.pone.0140021
21. Odukoya O, Badejo O, Sodeinde K, Olubodun T. Behavioral risk factors for hypertension among adults living with HIV accessing care in secondary health facilities in Lagos State, Nigeria. J Fam Med Prim Care. 2017;6(2):169–170.
22. Tsuro U, Oladimeji KE, Pulido-Estrada GA, Apalata TR. Risk factors attributable to hypertension among HIV-infected patients on antiretroviral therapy in selected rural districts of the Eastern Cape Province, South Africa. Int J Environ Res Public Health. 2022;19(18):11196. doi:10.3390/ijerph191811196
23. Nguyen KA, Peer N, Mills EJ, Kengne AP. Burden, determinants, and pharmacological management of hypertension in HIV-positive patients and populations: a systematic narrative review. AIDS Rev. 2015;17(2):83–95.
24. Musekwa R, Hamooya BM, Koethe JR, Nzala S, Masenga SK. Prevalence and correlates of hypertension in HIV-positive adults from the Livingstone Central Hospital, Zambia. Pan Afr Med J. 2021;39. doi:10.11604/pamj.2021.39.237.29718
25. Perin J, Mulick A, Yeung D, et al. Global, regional, and national causes of under-5 mortality in 2000–19: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet Child Adolesc Heal. 2022;6(2):106–115. doi:10.1016/S2352-4642(21)00311-4
26. Semeere AS. Hypertension and associated risk factors in individuals infected with HIV on antiretroviral therapy at an urban HIV clinic in Uganda. Lancet Glob Heal. 2014;2. doi:10.1016/S2214-109X(15)70045-8
27. Rodríguez-Arbolí E, Mwamelo K, Kalinjuma AV, et al. Incidence and risk factors for hypertension among HIV patients in rural Tanzania – a prospective cohort study. PloS one. 2017:630. doi:10.1371/journal.pone.0172089
28. IFPMA. HYPERTENSION: putting the Pressure on the silent Killer; May; 2016.
29. MoH. Rwanda Non communicable: risk, Factors Diseases Report. 2015.
30. Davis K, Perez-Guzman P, Hoyer A, et al. Association between HIV infection and hypertension: a global systematic review and meta-analysis of cross-sectional studies. BMC Med. 2021;19(1). doi:10.1186/s12916-021-02112-3
31. Isaac Derick K, Khan Z. Prevalence, Awareness, Treatment, Control of Hypertension, and Availability of Hypertension Services for Patients Living With Human Immunodeficiency Virus (HIV) in Sub-Saharan Africa (SSA): a Systematic Review and Meta-analysis. Cureus. 2023;15(4):1–16. doi:10.7759/cureus.37422
32. Okello S, Muhihi A, Mohamed SF, et al. Hypertension prevalence, awareness, treatment, and control and predicted 10-year CVD risk: a cross-sectional study of seven communities in East and West Africa (SevenCEWA). BMC Public Health. 2020;20(1):1–13. doi:10.1186/s12889-020-09829-5
33. Bayaraa N, Azahar NM, Kitaoka K, Kobayashi Y, Yano Y. African Control of Hypertension through Innovative Epidemiology and a Vibrant Ecosystem (ACHIEVE): a holistic approach for hypertension control in Africa. J Hum Hypertens. 2023. doi:10.1038/s41371-023-00845-7
34. Cochran WG. Sampling Techniques. Vol. 3.
35. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–3104. doi:10.1097/HJH.0000000000001940
36. ESIOBU E. The rise of homegrown ideas and grassroots voices: new directions in social policy in Rwanda; 2017. Available from: www.econstor.eu.
37. Nshutinzima AJ, Biracyaza E, Muhayisa A, Mukarusanga I, Mutabaruka J. Family determinants of substance use among Rwandan youths: a case study of Gitagata Rehabilitation Centre. J Subst Use. 2023;1–9. doi:10.1080/14659891.2023.2284945
38. Murwanashyaka J de D, Ndagijimana A, Biracyaza E, Sunday FX, Umugwaneza M. Non-adherence to medication and associated factors among type 2 diabetes patients at clinique medicale fraternite, Rwanda: a cross-sectional study. BMC Endocr Disord. 2022;22(1):1–14. doi:10.1186/s12902-022-01133-0
39. Lukas K, Markos E, Belayneh F, Habte A, Torpey K. The magnitude of hypertension and associated factors among clients on highly active antiretroviral treatment in Southern Ethiopia, 2020: a hospital-based cross-sectional study. PlosOne. 2021;10(6):e0258576. doi:10.1371/journal.pone.0258576
40. Saito A, Karama M, Kamiya Y. HIV infection, and overweight and hypertension: a cross-sectional study of HIV-infected adults in Western Kenya. Trop Med Health. 2020;48(1). doi:10.1186/s41182-020-00215-w
41. Gebrie A, Gebremedhin S. Hypertension among people living with human immunodeficiency virus receiving care at referral hospitals of Northwest Ethiopia: a cross-sectional study. PLoS One. 2020;15(8):1–13. doi:10.1371/journal.pone.0238114
42. Badru O, Oduola T, Abdulrazaq A, Peter C. Prevalence and predictive factors of hypertension among people living with HIV in Kebbi State, Nigeria: a cross-sectional study. J Assoc Nurses AIDS Care. 2020;33(1):e6–e14. doi:10.1097/JNC.0000000000000309
43. Mulugeta H, Afenigus AD, Haile D, et al. Incidence and predictors of hypertension among HIV patients receiving art at public health facilities, northwest Ethiopia: a one-year multicenter prospective follow-up study. HIV/AIDS - Res Palliat Care. 2021;13:889–901. doi:10.2147/HIV.S329838
44. Sewale Y, Afenigus AD, Haile D, Shiferaw WS. Magnitude of hypertension and associated factors among human immunodeficiency virus positive adults receiving anti-retroviral therapy at Debre Markos referral hospital, northwest, Ethiopia. HIV/AIDS - Res Palliat Care. 2020;12:629–637. doi:10.2147/HIV.S280630
45. Mbuthia GW, Magutah K, Mcgarvey ST. The Prevalence and Associated Factors of Hypertension among HIV Patients. Int J Hypertens. 2021;15:5544916. doi:10.1155/2021/5544916
46. Anwer Z. Hypertension management in diabetic patients. Eur Rev Med Pharmacol Sci. 2011;15:1.
47. Njeru JIW. Prevalence and associated risk factors for hypertension among HIV positive patients attending comprehensive care centre at Thika District hospital, Kenya, 2008 James Ian Wathuta Njeru A Thesis Submitted in Partial Fulfillment for the Degree of Master of; 2009.
48. Mbuthia GW, Magutah K, Mcgarvey ST, Moreira TMM. The prevalence and associated factors of hypertension among HIV patients. Int J Hypertens. 2021;2021:1–8. doi:10.1155/2021/5544916
49. Fiseha T, Belete AG, Dereje H, Dires A. Hypertension in HIV-infected patients receiving antiretroviral therapy in Northeast Ethiopia. Int J Hypertens. 2019;2019:1–7. doi:10.1155/2019/4103604
50. Jacques B, Joliana P. Prevalence of hypertension among working adults in Rwanda. Iran J Publ Heal. 2013;42(8).
51. Olin BR. Hypertension: the Silent Killer: updated JNC-8 Guideline Recommendations; 2018.
52. CADTH. Peer support for diabetes, heart disease and HIV/AIDS: a Review of the clinical effectiveness, cost-effectiveness, and guidelines. PubMed. 2013.
53. Zewudie BT, Geze Tenaw S, Solomon M, et al. The magnitude of undiagnosed hypertension and associated factors among HIV-positive patients attending antiretroviral therapy clinics of Butajira General Hospital, Gurage Zone, Southern Ethiopia. SAGE Open Med. 2022;10:1–7. doi:10.1177/20503121221094454
54. Dzudie A, Hoover D, Kim HY, et al. Hypertension among people living with HIV/ AIDS in Cameroon: a cross-sectional analysis from Central Africa International Epidemiology Databases to Evaluate AIDS. PLoS One. 2021;16(7):1–17. doi:10.1371/journal.pone.0253742
55. Dechasa M, Nigussie S, Jambo A, et al. The magnitude of hypertension and its contributing factors among patients receiving antiretroviral therapy in public hospitals in Harar City, Eastern Ethiopia: A Cross-Sectional Study. Integr Blood Press Control. 2023;16:81–93. doi:10.2147/ibpc.s433907
56. Lukas K, Markos E, Belayneh F, Habte A, Torpey K. The magnitude of hypertension and associated factors among clients on highly active antiretroviral treatment in Southern Ethiopia, 2020: a hospital-based cross-sectional study. PLoS One. 2021;16(10):1–15. doi:10.1371/journal.pone.0258576
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.