")
Back to Journals » International Journal of Women's Health » Volume 16
Prevalence, Characteristics, and Treatment Pattern of Menstrual-Related Headache Among Undergraduate Health Sciences Students at Addis Ababa University, Ethiopia
Authors Ali HE, Tadesse TA , Beyene DA , Gebremariam GT
Received 12 December 2023
Accepted for publication 15 April 2024
Published 20 April 2024 Volume 2024:16 Pages 707—716
DOI https://doi.org/10.2147/IJWH.S454357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Habiba Ejabo Ali,1 Tamrat Assefa Tadesse,1 Dessale Abate Beyene,2 Girma Tekle Gebremariam1
1Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Pharmacy, Asrat Woldeyes Health Science Campus, Debre Berhan University, Debre Berhan, Ethiopia
Correspondence: Girma Tekle Gebremariam, Email [email protected]
Background: Menstrual-related headache (MRH) is the most prevalent health condition among young females that limits productivity and social life. However, the magnitude of the problem and its characteristics have not been studied in Ethiopia.
Objective: This study aimed to assess the prevalence, characteristics, and treatment of MRH among undergraduate female students at the College of Health Sciences, Addis Ababa University, Ethiopia.
Methods: A cross-sectional study was conducted among undergraduate female students from May to June 2023. A random sample of 1000 females were approached who fulfilled the eligibility criteria using the online electronic method. Descriptive statistics were used to summarize participant characteristics. Multivariate logistic regression analysis was performed to identify factors associated with the severity of pain. All statistical analyses were performed using SPSS version 26. A p-value ≤ 0.05 was considered statistically significant.
Results: Of the 1000 students who approached online, 757 were included in the final analyses. The prevalence of MRH was (86, 11.4%) and 32.6% of them has experienced the headache before two to three days of menses. The median number of days of missed social activities and reduced productivity was three and one day, respectively. Being single was 6.24 times more likely to have severe MRH (AOR = 6.24, 95% CI: 2.73– 14.26, p=0.001) and pharmacy students were less likely (AOR = 0.31, 95% CI: 0.16– 0.61, p = 0.001) to have severe pain.
Conclusion: Our findings illustrated that MRH among young female students adversely affects students’ productivity and social life. This demands interventions to reduce the impact and should pay attention in the future, particularly to create awareness to enhance screening and rendering various treatment options for the target population.
Keywords: prevalence, characteristics, menstrual-related headache, treatment pattern, Ethiopia
Introduction
Headache is a common neurological disorder that is associated with a significant burden worldwide and affects productivity, social, and daily routines adversely. However, it has been underestimated, underrecognized, and undertreated worldwide.1,2 Headache compliance is highly associated with menstruation among young women.3 According to the World Health Organization (WHO), an estimated 50% of young women have an increased risk of experiencing menstrual-related headaches (MRH).4 It is commonly encountered during menstruation and primarily occurs owing to a decline in estrogen during the menstrual cycle, and the attack significantly increases during the first days of menstruation.1,5,6 Despite the attacks among studies, the attack is 2.5 folds higher during the premenstrual window, and the onset of migraine is earlier in patients with a first-degree family history.7–9 On the other hand, menstrual migraine can be divided into two types according to ICHD-3: pure menstrual migraine and menstrual related migraine. Compared to non-menstrual attacks, menstrual migraine attacks tend to be more severe, longer-lasting and less responsive to treatment, resulting in a significant reduction of the quality of life for the affected women (Table 1).10,11
 |
Table 1 ICHD-III Criteria to Classify Headache Type |
In young women, one subtype of primary headache may change to other subtypes over time in the same individual during the menses. Consequently, appropriate diagnosis and characterization of headaches is difficult and sexual maturation influences the occurrence and characteristics of primary headaches.12–14 Premenstrual headaches increase linearly with a marked worsening of pain intensity and duration during premenstrual headache attacks.15 The precipitating factors such as prostaglandins increases days before menses and this induces pain. Moreover, diet, nutritional status, oral contraceptive usage, and hormone replacement treatment are important triggers of headache pain in young women.16,17 As a result, women have more severe headaches during the premenstrual period than during other times of the month, and identifying those factors will have a profound role in the management of MRH.18,19 Particularly menstrual-related migraine usually last longer and are characterized by symptoms, such as throbbing or pulsating headaches, sensitivity to light, nausea, fatigue, and dizziness.9 These can significantly affect the overall quality of life, school attendance, and academic performance of female college students compared with non-menstrual headache attacks and the lower efficacy of abortive medications.7,20
Given this high burden among young women, early and targeted intervention is crucial to prevent MRH from becoming a chronic condition.21 Currently, available pharmacological treatments for MRH include triptans, nonsteroidal anti-inflammatory drugs, and hormonal therapy has been used often to reduce the pain.22,23 However, administration of hormonal therapy could exacerbate MRH due to hormonal fluctuations and increase the risk of vascular diseases, such as stroke, heart disease, and vascular mortality.24 Besides, study has shown that non-invasive vagus nerve stimulation can be used as prophylaxis, and the number of MRH days per month was significantly reduced by 50% compared to the baseline, however it is not used commonly.25 Hence, careful diagnosis and management are essential to prevent serious consequences such as overuse of medication and withdrawal from daily activities.26 However, evidence on the burden of MRH in those population groups has not yet been well studied.27,28 Similarly, in Ethiopia, limited studies have been conducted on the burden and management pattern of MRH. Our study aimed, therefore, to assess the prevalence, characteristics, and treatment patterns of MRH among undergraduate female students at Addis Ababa University. Such a study has the advantage of identifying precipitating factors that influence the frequency and severity of MRH and thereby helping to provide effective individualized therapy to improve overall quality of life.
Methods
Study Setting, Design, and Population
This cross-sectional study was conducted among undergraduate female students from May to June 2023 at the College of Health Sciences (CHS) of Addis Ababa University, in Ethiopia. The CHS has the largest tertiary teaching hospital in the Tikur Anbessa Specialized Hospital (TASH). The CHS teaches more than 5000 students, and about 2300 students are enrolled in the undergraduate program.
Sample Size and Sampling Procedure
A random sample of 1000 female undergraduate students who fulfilled the eligibility criteria was approached during the study period. At least one history of headache episodes during their lifetime was considered a criterion to say the woman had MRH. However, those who had not experienced headaches or were unwilling to participate were excluded from the study.
Data Collection Procedure and Tool
Information on sociodemographic and MRH characteristics was collected using a pre-tested, self-administered questionnaire through online electronic methods, such as Google Forms. The purpose and procedure of the study were explained to all participants on the online data collection form. Virtual informed consent was obtained from all study participants, and personal identifiers were not collected. In addition, the completeness and consistency of the data were checked daily, and an amendment was made in consultation with senior supervisors.
The data collection tool comprises four main sections. The first section assessed sociodemographic characteristics, and the second contained the characteristics of MRH and its relationship with menstruation. The International Classification of Headaches Disorders (ICHD-III) was used to classify the types of primary headaches encountered.29 The third and fourth sections were about the impact of headaches on their daily routines using the Migraine Disability Assessment Scale (MIDAS)30 and the treatment used by the participants, respectively.
Statistical Analyses
Descriptive statistics (frequency, mean with standard deviation, and percentage) were used to summarize the demographic and MRH characteristics of the participants. Furthermore, univariate and multivariate logistic regression analyses were performed to identify factors associated with MRH pain severity. Statistical analyses were performed using Statistical Package for the Social Sciences (IBM Corporation, Armonk, NY, USA) version 26. All statistical tests were performed at a level of significance of p-value <0.05.
Ethical Clearance
Ethical clearance was obtained from the Ethical Review Committee of the School of Pharmacy, College of Health Sciences, Addis Ababa University, Ethiopia. Furthermore, our study was performed in accordance with the principles stated in the Declaration Helsinki. The participants were requested to provide informed consent before participating in the study. The study participants were assured of the confidentiality of the information they provided by the research team. Privacy was maintained by avoiding study participants’ identifiers (name, phone number), and the data were analysed in aggregate.
Results
Sociodemographic Characteristics of the Participants
One thousand female undergraduate students who fulfilled the eligibility criteria participated in the survey, and 757 completed the survey, which was included in the final data analyses. One-third of the participants were medical students; the majority (664, 87.7%) were in the age range of 20 to 25, and nearly three-fourths of them were studying year three and above (Table 2).
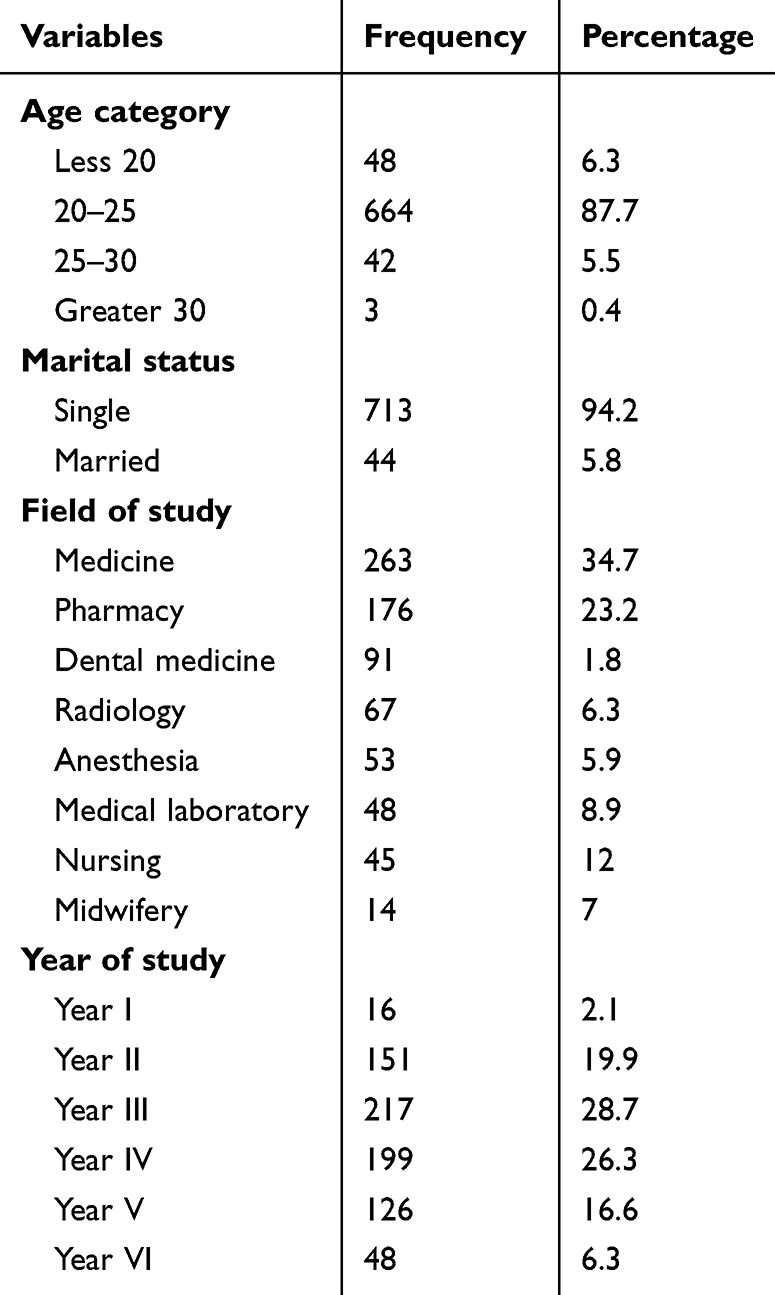 |
Table 2 Sociodemographic Characteristics of the Study Participants (N=757) |
Prevalence and Characteristics of MRH Among the Participants
The episodes of headache in undergraduate female students were two to three times a month among 337 (44.5%) participants, followed by once a month in 225 (29.7%) of them. Our finding illustrated that among those who had experienced headache, (11.4%) of them reported MRH. The majority (51,59.3%) of them had a family history of recurrent MRH, and 25 (29.1%) had at least 2 or more MRH attacks in the past year. Moreover, from those identifying MRH, 48 (55.8%) of the participants had experienced the headache attack during menses and 34 (39.5%) of the study they had experienced during every cycle. The most frequently reported symptoms associated with MRH were nausea and vomiting (28, 32.6%) and photophobia (20, 23.3%), respectively. In the present study, the most common triggering factors for MRH were menstruation itself (56, 65.1%), followed by sleep disturbances (20, 23.3%). The MRH was predominantly bilateral in terms of anatomical location (66, 76.7%) while in terms of quality of pain was throbbing/sharp stabbing accounts 60.4%. Furthermore, 50% of the study participants rated their level of pain as mild, and the remaining 29% and 20.9% reported moderate and severe pain, respectively (Table 3).
 |
Table 3 Prevalence and Characteristics of MRH Among Participants |
Burden of MRH on Daily Routine Activities
Based on the MIDAS, the impact of headaches on students’ lives was higher on the number of days of reduced productivity (work or school) and days of missed housework within the past three months with a mean (SD) of 3.41±2.07 and 3.16±3.55, respectively (Table 4).
 |
Table 4 Burden of MRH Among Undergraduate Female Students |
Treatment Pattern of Menstrual-Related Headache Among the Participants
Among the participants who experienced MRH, more than half of them (45, 52.3%) have had medical consultations. Most of them (74,86%) were relieved from pain when they took prescription-only or over-the-counter (OTC) medications, of which ibuprofen (54.6%) and paracetamol (35.6%) were the most widely used analgesic medications. Moreover, 68 (79.1%) opt for sleeping in a quiet environment to avoid light (Table 5).
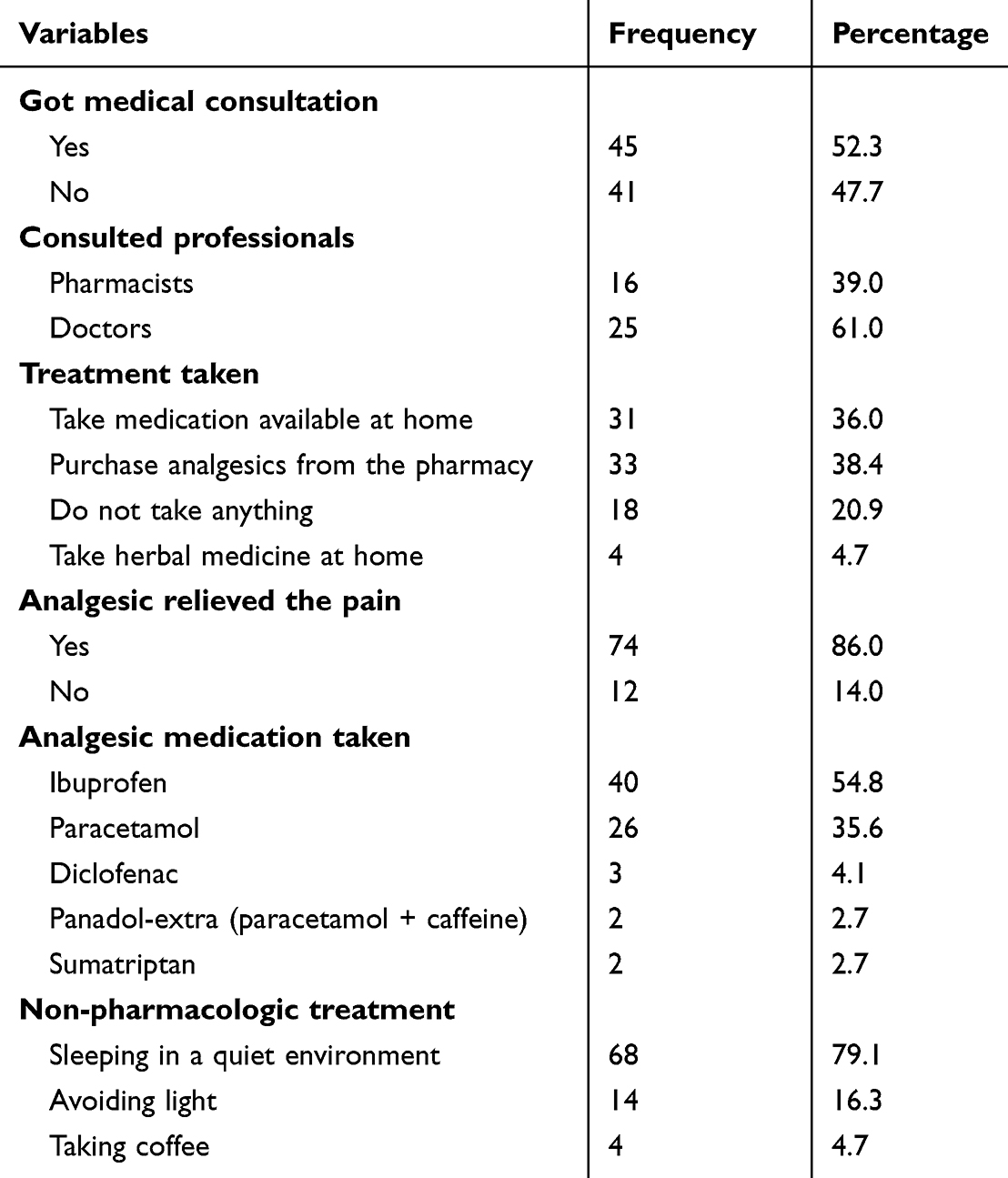 |
Table 5 Treatment Pattern of MRH Among Undergraduate Female Students (N=86) |
Factors Associated with Menstrual-Related Headache
Univariate analysis revealed that five variables were correlated with pain severity. Furthermore, to identify factors associated with the pain severity of MRH, a multivariate binary regression analysis using cross-validation with the hierarchical regression method was conducted and showed that three variables (marital status, family income, and field of study) were significantly associated with pain severity. Being single was 6.24 times more likely (AOR = 6.24, 95% CI: 2.73–14.26, p-value = 0.001) to have severe MRH than married ones, and those students who have household income between 15,000 and 30,000 ETB were 4.65 times more likely (AOR = 4.65, 95% CI: 2.22–9.71, p-value = 0.001) to have severe pain, and those whose family monthly income between 30,000 and 45,000 ETB was 2.85 times more likely (AOR = 2.65, 95% CI: 1.48–5.48, p-value = 0.002) to have severe pain. In addition, pharmacy students were less likely to have experienced severe pain (AOR = 0.31, 95% CI: 0.16–0.61, p-value = 0.001) than students studying medicine (Table 6).
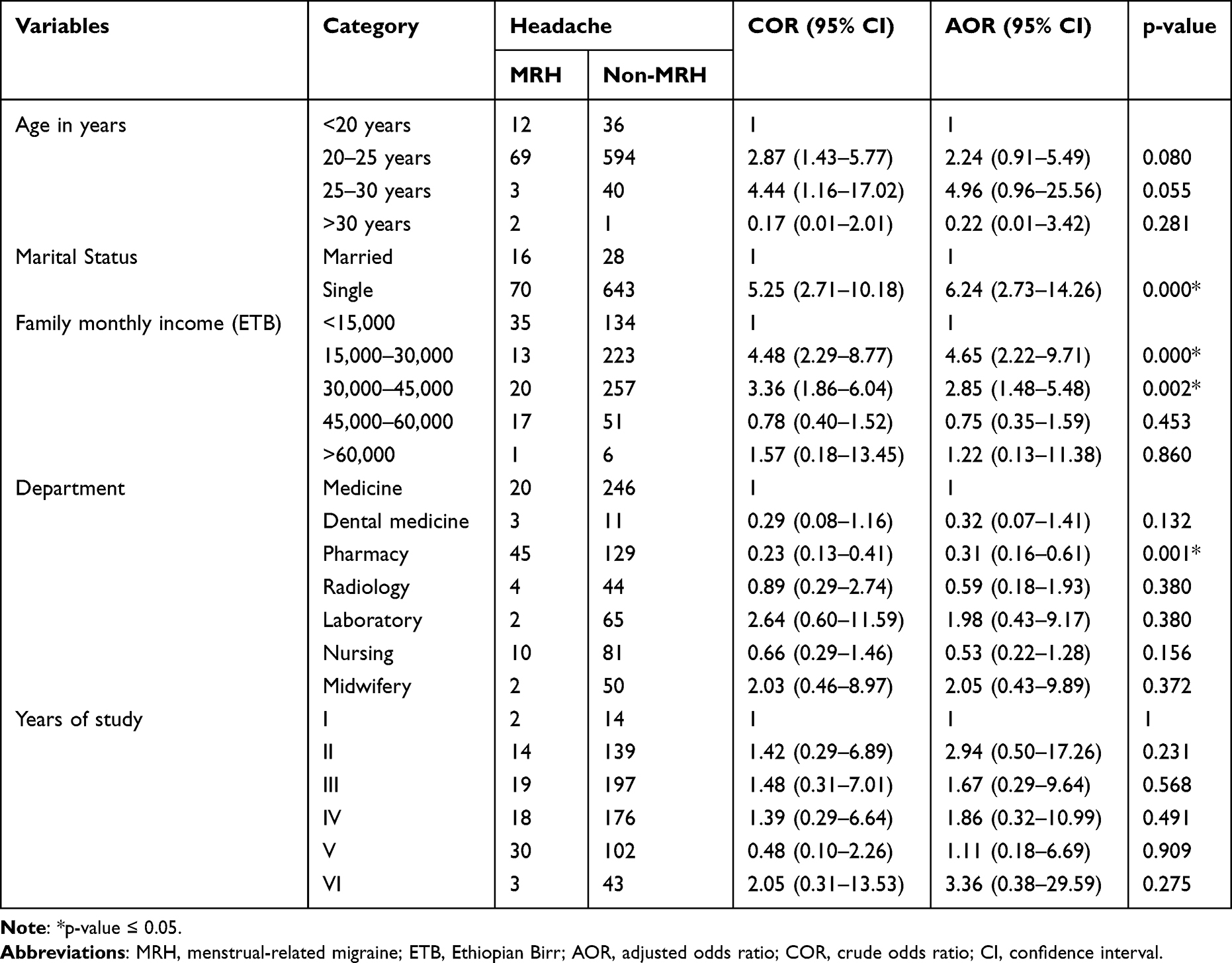 |
Table 6 Factors Associated with MRH Pain Severity Among the Participants |
Discussion
The primary objective of this study was to assess the prevalence, characteristics, and treatment patterns of MRH among undergraduate female students at the College of Health Sciences of Addis Ababa University. Our findings demonstrated that MRH prevalence was 11.4% among those who had ever experienced headache in their lifetime, and 50% of the participants reported mild pain. Being single, having a higher household income, and being a medical student were associated with the severity of MRH pain.
In this study, the prevalence of MRH among those who had experienced headache was 11.4%, which is comparable with the study among a cohort of senior secondary school girls in Nigeria with a prevalence rate of 14.2%.28 Nevertheless, it is lower than the study conducted in Norway (21%) and Saudi Arabia (32.5%).31,32 The reason for the variation in the prevalence of MRH between studies could be explained by racial and study setting differences.14 Studies have shown that a significant difference in migraine prevalence between distinct racial groups.33–35 Besides, nutritional habits, variations in weather and climate were also contributing factors for MRH.28,36 In our findings, definite and probable menstrual-related migraine were 22.5% which is higher than a study conducted in the United Kingdom, and Yugoslavia that reported 7.6%,37 and 12.6%,38 respectively. However, studies conducted in Brazil and Spain have reported that the prevalence of MRH among young women was 69.2% and 45.14%,39,40 respectively. The evidence highlights that MRH was not assessed by a neurologist in this study and was self-reported by the participants, which might have increased the magnitude of MRH in this study. Furthermore, genetic vulnerability, cultural, and environmental factors could account for the variations in prevalence of the MRH across different young women.41–43
Moreover, menstruation itself was reported by 65.1% of the participants as a major triggering factor for the headache attack, which is similar to a population-based study (60%).17,44 In the present study, sleep disturbance and exam stress were the most significant triggering factors for MRH. Similarly, another study reported that psychological stress, smoking, menstruation, contraceptive pills, hunger/skipping meals, and consumption of coffee, chocolate, and aged cheese were precipitating factors for MRH.32 Furthermore, MRH attacks occurred in 48 (55.8%) of the respondents during menses within 2–3 days before menses; however, in other studies, the frequency of MRH attacks increased during the 2 days before menstruation.17,28 The higher prevalence in our population study is expected due to their young ages and stressful academic lives.
Regarding headache characteristics, 50% of our medical students with MRH had moderate to severe intensity of their attacks, which is lower than that found in other studies.14,45 This study showed that most participants reported mild disability (MIDAS grades I and II). This is in agreement with a study conducted somewhere else.46 In this study, 47.7% of the students sought medical attention for MRH, which is significantly higher than the 12% reported in Saudi Arabia.32 This may be explained by the large percentage of students taking OTC medications, which was supplemented by a study conducted in the United Arab Emirates.47 In our study, 54.8% were taking ibuprofen, followed by 35.6% paracetamol, to relieve the pain, a finding that is in agreement with those revealed from various studies.32 The reason for using these medications could be explained by their low price, safety, and fewer GIT side effects, in addition to their availability as an over-the-counter medication.48 Medical and single students in older grades showed significantly higher levels of pain severity in this study. This finding is in line with a study conducted among Saudi female students at Taif University.32
This study has certain limitations. As this study was cross-sectional, it may be difficult to establish causal relationships. Furthermore, the nature and types of headaches experienced by participants were not confirmed by a neurologist, and the prevalence may not be conclusive. However, the strength of this study lies in the fact that there is little MRH-specific data from Ethiopia. Consideration of studies in small and specific headache populations has the added advantage of helping to identify factors that influence the frequency and severity of headaches, allowing effective planning and organization of health services.
Conclusions
MRH is prevalent among female students and adversely affects their productivity in school and social life. Menstruation, sleep disturbances, exam stress, and strong odors have been reported as triggering factors, regardless of the type of menstrual-related headache. The most commonly reported pain intensity was described as mild and was mainly treated with ibuprofen. Interventions to reduce the impact of MRH should pay attention in the future, particularly to create awareness to enhance screening and rendering various treatment options for the target population.
Abbreviations
AAU, Addis Ababa University; CHS, College of Health Sciences; CNS, Central Nervous System; HRT, Hormone replacement treatment; ICHD-IV, International Classification of Headaches Disorders; MIDAS, Migraine Disability Assessment scale; MRH, Menstrual-Related Headaches; MRM, Menstrual Related Migraine; OTC, Over-The-counter medications; WHO, World Health Organization, VAS, Visual analog scale.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author at a reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was not received from any organization and the authors are from a low-income country.
Disclosure
The authors declare that there are no competing interests in this work.
References
1. Steiner TJ, Birbeck GL, Jensen RH, Katsarava Z, Stovner LJ, Martelletti P. Headache disorders are third cause of disability worldwide. J Headache Pain. 2015;16(1):15–17. doi:10.1186/s10194-015-0544-2
2. Stovner LJ, Hagen K, Jensen R, et al. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007;27(3):193–210. doi:10.1111/j.1468-2982.2007.01288.x
3. Na W, Liu H, Liu Y, Wang X, Yu S. The role of purity and frequency in the classification of perimenstrual headache. BMC Neurol. 2023;23(1):1–8. doi:10.1186/s12883-023-03268-6
4. Moy G, Vikas G. Menstrual-Related Headache - StatPearls - Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/Accessed on September 10, 2023.
5. Raffaelli B, Do TP, Chaudhry BA, Ashina M, Amin FM, Ashina H. Menstrual migraine is caused by estrogen withdrawal: revisiting the evidence. J Headache Pain. 2023;24(1):1–10. doi:10.1186/s10194-023-01664-4
6. Reddy N, Desai MN, Schoenbrunner A, Schneeberger S, Janis JE. The complex relationship between estrogen and migraines: a scoping review. Syst Rev. 2021;10(1):1–13. doi:10.1186/s13643-021-01618-4
7. Pringsheim T, Davenport WJ. Prevalence of migraine on each day of the natural menstrual cycle. Headache. 2007;47(2):341. doi:10.1111/j.1526-4610.2006.00711.x
8. Olesen J. Headache classification committee of the International Headache Society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211.
9. Murtaza M, Kisat M, Daniel H, Sonawalla AB. Classification and clinical features of headache disorders in Pakistan: a retrospective review of clinical data. PLoS One. 2009;4(6):1–8. doi:10.1371/journal.pone.0005827
10. Zhang H, Qi JZ, Zhang ZH. Comparative efficacy of different treatments for menstrual migraine: a systematic review and network meta-analysis. J Headache Pain. 2023;24(1):1–9. doi:10.1186/s10194-023-01625-x
11. Van Casteren DS, Verhagen IE, Van Der Arend BWH, Van Zwet EW, Maassenvandenbrink A, Terwindt GM. Comparing perimenstrual and nonperimenstrual migraine attacks using an e-diary. Neurology. 2021;97(17):E1661–71. doi:10.1212/WNL.0000000000012723
12. Monteith TS, Sprenger T. Tension type headache in adolescence and childhood: where are we now? Curr Pain Headache Rep. 2010;14(6):424–430. doi:10.1007/s11916-010-0149-z
13. Onan D, Younis S, Wellsgatnik WD, et al. Debate: differences and similarities between tension-type headache and migraine. J Headache Pain. 2023;24(1):1–16. doi:10.1186/s10194-023-01614-0
14. Oraby MI, Soliman RH, Mahmoud MA, Elfar E, Abd ElMonem NA. Migraine prevalence, clinical characteristics, and health care-seeking practice in a sample of medical students in Egypt. Egypt J Neurol Psychiatry Neurosurg. 2021;57(1). doi:10.1186/s41983-021-00282-8
15. Vetvik KG, MacGregor EA, Lundqvist C, Russell MB. Symptoms of premenstrual syndrome in female migraineurs with and without menstrual migraine. J Headache Pain. 2018;19(1). doi:10.1186/s10194-018-0931-6
16. Lipton RB, Bigal ME. Migraine: epidemiology, impact, and risk factors for progression. Headache. 2005;45(SUPPL. 1). doi:10.1111/j.1526-4610.2005.4501001.x
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24(9):707–716. doi:10.1111/j.1468-2982.2004.00741.x
18. Vetvik KG, MacGregor EA. Menstrual migraine: a distinct disorder needing greater recognition. Lancet Neurol. 2021;20(4):304–315. doi:10.1016/S1474-4422(20)30482-8
19. Pringsheim T, Davenport WJ, Dodick D. Acute treatment and prevention of menstrually related migraine headache: evidence-based review. Neurology. 2008;70(17):1555–1563. doi:10.1212/01.wnl.0000310638.54698.36
20. Zwart JA, Dyb G, Holmen TL, Stovner LJ, Sand T. The prevalence of migraine and tension-type headaches among adolescents in Norway. The Nord-Trøndelag Health Study (Head-HUNT-Youth), a large population-based epidemiological study. Cephalalgia. 2004;24(5):373–379. doi:10.1111/j.1468-2982.2004.00680.x
21. Lay CL, Broner SW. Adolescent issues in migraine: a focus on menstrual migraine. Curr Pain Headache Rep. 2008;12(5):384–387. doi:10.1007/s11916-008-0065-7
22. Allais G, Chiarle G, Sinigaglia S, Benedetto C. Menstrual migraine: a review of current and developing pharmacotherapies for women. Expert Opin Pharmacother. 2018;19(2):123–136. doi:10.1080/14656566.2017.1414182
23. Mannix LK. Menstrual-related pain conditions: dysmenorrhea and migraine. J Women’s Heal. 2008;17(5):879–891. doi:10.1089/jwh.2007.0440
24. Cupini LM, Corbelli I, Sarchelli P. Menstrual migraine: what it is and does it matter? J Neurol. 2021;268(7):2355–2363. doi:10.1007/s00415-020-09726-2
25. Andrasik F, Grazzi L, D’Amico D, et al. Mindfulness and headache: a “new” old treatment, with new findings. Cephalalgia. 2016;36(12):1192–1205. doi:10.1177/0333102416667023
26. Shehnaz SI, Agarwal AK, Khan N. A systematic review of self-medication practices among adolescents. J Adolesc Heal. 2014;55(4):467–483. doi:10.1016/j.jadohealth.2014.07.001
27. Parekh N, Stevenson JM, Schiff R, et al. Can doctors identify older patients at risk of medication harm following hospital discharge? A multicentre prospective study in the UK. Br J Clin Pharmacol. 2018;84(10):2344–2351. doi:10.1111/bcp.13690
28. Adebayo PB, Otubogun FM, Akinyemi RO. Menstrual-related headaches among a cohort of African adolescent girls. J Pain Res. 2020;13:143–150. doi:10.2147/JPR.S207620
29. Goadsby PJ, Evers S. International classification of headache disorders - ICHD-4 alpha. Cephalalgia. 2020;40(9):887–888. doi:10.1177/0333102420919098
30. Stewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN. Validity of the Migraine Disability Assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain. 2000;88(1):41–52. doi:10.1016/S0304-3959(00)00305-5
31. Vetvik KG, MacGregor EA, Lundqvist C, Russell MB. Self-reported menstrual migraine in the general population. J Headache Pain. 2010;11(2):87–92. doi:10.1007/s10194-010-0197-0
32. Desouky D, Zaid H, Taha A. Depression among Saudi female students in Taif University. J Egypt Public Health Assoc. 2019;7(1):1–9.
33. Stewart WF, Lipton RB, Liberman J. Variation in migraine prevalence by race. Neurology. 1996;47(1):52–59. doi:10.1212/WNL.47.1.52
34. Loder S, Sheikh HU, Loder E. The prevalence, burden, and treatment of severe, frequent, and migraine headaches in US minority populations: statistics from national survey studies. Headache. 2015;55(2):214–228. doi:10.1111/head.12506
35. Abtahi SH, Esfahanian F, Akbari M, Roomizadeh P, Neshat S. Headache—a challenge across medical students’ life: a systematic review and meta-analysis. Acta Neurol Belg. 2023;123(3):785–801. doi:10.1007/s13760-023-02274-2
36. Crawford MJ, Lehman L, Slater S, et al. Menstrual migraine in adolescents. Headache. 2009;49(3):341–347. doi:10.1111/j.1526-4610.2009.01347.x
37. Vetvik KG, MacGregor EA, Lundqvist C, Russell MB. Prevalence of menstrual migraine: a population-based study. Cephalalgia. 2014;34(4):280–288. doi:10.1177/0333102413507637
38. Dzoljic E, Sipetic S, Vlajinac H, et al. Prevalence of menstrually related migraine and nonmigraine primary headache in female students of Belgrade University. Headache. 2002;42(3):185–193. doi:10.1046/j.1526-4610.2002.02050.x
39. Fernández-Martínez E, Onieva-Zafra MD, Abreu-Sánchez A, et al. Menstrual migraine among Spanish university students. J Pediatr Nurs. 2021;56:e1–6. doi:10.1016/j.pedn.2020.06.013
40. Tavares IS, Germano AP, Bordini CA. Prevalence of menstrually-related migraine in a population of students from a municipal university center in the interior of Brazil. Headache Medicine. 2021;12(1):29–34. doi:10.48208/HeadacheMed.2021.6
41. Al-Hassany L, Haas J, Piccininni M, Kurth T, Maassen Van Den Brink A, Rohmann JL. Giving researchers a headache – sex and gender differences in migraine. Front Neurol. 2020;11:1–16. doi:10.3389/fneur.2020.549038
42. Kim BK, Chu MK, Yu SJ, et al. Prevalence rates of primary headache disorders and evaluation and treatment patterns among Korean neurologists. J Clin Neurol. 2022;18(5):571–580. doi:10.3988/jcn.2022.18.5.571
43. Grangeon L, Lange KS, Waliszewska-Prosół M, et al. Genetics of migraine: where are we now? J Headache Pain. 2023;24(1):1–23. doi:10.1186/s10194-023-01547-8
44. Pavlović JM, Stewart WF, Bruce CA, et al. Burden of migraine related to menses: results from the AMPP study. J Headache Pain. 2015;16(1). doi:10.1186/s10194-015-0503-y.
45. Holla R, Darshan BB, Ying YZ, et al. Clinical characteristics and associated disability of headache among medical undergraduates. Indian J Public Heal Res Dev. 2019;10(8):647–650. doi:10.5958/0976-5506.2019.01960.0
46. Chia V, Bogdanov A, Yusuf A, Kallenbach L. Characteristics of migraine patients with Migraine Disability Assessment (MIDAS) scores in real-world clinical practice. Cephalalgia Rep. 2020;3:1–7. doi:10.1177/2515816320928463
47. Rustom A, Audi F, Al Samsam H, Nour R, Mursi AM, Mahmoud I. Migraine awareness, prevalence, triggers, and impact on university students: a cross-sectional study. Egypt J Neurol Psychiatry Neurosurg. 2022;58(1). 10.1186/s41983-022-00555-w.
48. Abdo SA, Amood Al-Kamarany M, Alzoubi KH, Al-Maktari MT, Al-Baidani AH. Primary headache in Yemen: prevalence and common medications used. Neurol Res Int. 2014;2014:1–6. doi:10.1155/2014/808126
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.