")
Back to Journals » Advances in Medical Education and Practice » Volume 14
Problem Based Learning in Medical Education: Handling Objections and Sustainable Implementation
Authors Lim WK
Received 14 October 2023
Accepted for publication 17 December 2023
Published 28 December 2023 Volume 2023:14 Pages 1453—1460
DOI https://doi.org/10.2147/AMEP.S444566
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Video abstract presented by Lim.
Views: 143
William K Lim
Department of Paraclinical Sciences, Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak, Kota Samarahan, Sarawak, 94300, Malaysia
Correspondence: William K Lim, Email [email protected]
Abstract: The introduction of problem-based learning (PBL) in 1969 is considered the greatest innovation in medical education of the past 50 years. Since then, PBL has been implemented in different educational settings across virtually all health professions. However, some PBL schools gradually faced resistance from academic staff who were more familiar with traditional teacher-centred curricula. At times this has resulted in reversion to tradition or compromise whereby PBL is implemented within a lecture-based curriculum. Resistance can also emerge in a traditional school when a PBL curriculum is being considered for implementation. One of the first signs of this erosion is doubts about PBL raised in the form of objections or criticisms. This perspective review describes eight objections raised to assert why PBL is inferior or untenable. The background to each objection is provided together with evidence-informed rebuttals derived from professional practice and the published literature. Best practices are discussed for sustainable management of a PBL-based curriculum. A well-implemented PBL curriculum with appropriate and cost-effective infrastructure, training, teaching-learning activities, and assessment will position schools to harness the full benefit of PBL in training medical and health professionals.
Keywords: problem-based learning, lecture-based curriculum, educational philosophy, facilitator, traditional lectures
Introduction
In 1969, the medical school at McMaster University in Canada implemented a new curriculum philosophy which became known as problem-based learning (PBL). Since then, over fifty years of educational research have borne out its theoretical bases, worldwide efficacy, and continuing relevance.1–3 However, the average faculty’s view of PBL is more likely influenced by its implementation at their institution, which may not be all positive. The greatest challenge for an innovative teaching-learning approach such as PBL is the risk of it being dismantled, or more commonly sidelined by lecture-based teaching, after the founders or designers leave. The first three Malaysian medical schools that employed PBL from inception of the school all reported resistance from faculty after the first student cohort had graduated.4–6 An older school that incorporated PBL drifted back to tradition for a time when key faculty left.7 For this same reason a special PBL programme in China was terminated.8 In Norway, faculty opposition against a new full PBL curriculum resulted in implementation of a partial version.9 Examples of failed PBL curricula were also reported in New Zealand, Singapore and the Philippines.10,11 The first sign of resistance is usually the emergence of doubts, apprehensions, and criticisms about PBL. In this perspective review, 8 objections to PBL (Table 1) are presented and refuted. The objective is to enable PBL practitioners to handle objections while providing recommended best practices to underpin a sustainable PBL curriculum.
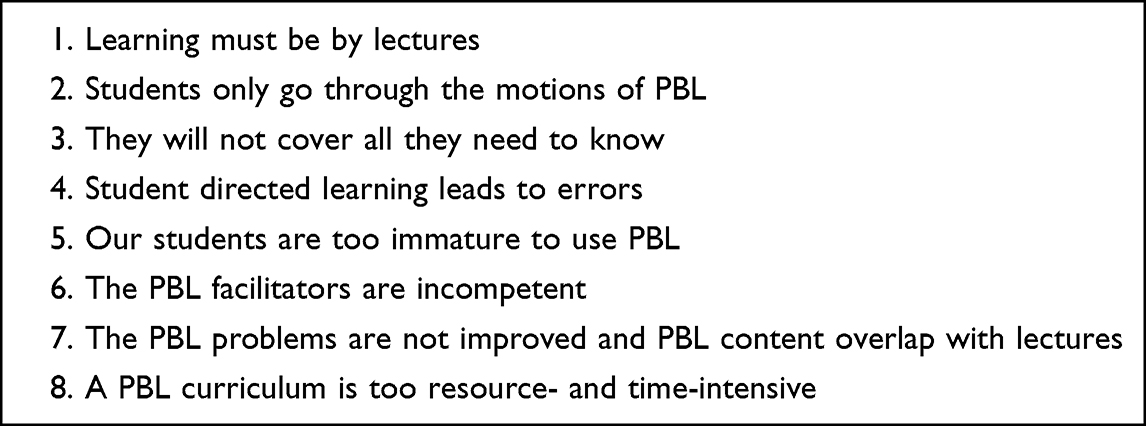 |
Table 1 Eight Objections to PBL |
Learning Must Be by Lectures
There is no pure PBL curriculum that is without lectures.12 PBL rose partly because traditional lecture-based curricula did not promote knowledge retention but the students were memorizing, then forgetting.13 A study on the value of lectures in a PBL curriculum found lectures not useful for knowledge transmission but helps clarify the problems and the place of the unit in the whole curriculum.14 Best-practice exemplars of Asian PBL programmes have been observed to limit lectures to only 4 or 5 hours a week.11 The hallmark of a PBL curriculum is that most teaching-learning activities are compatible with the PBL philosophy of active, contextual, or collaborative learning which will foster deep understanding, long-term knowledge retention and retrieval. In a PBL curriculum, students see the problem first while other classes are coordinated with the problem, but allowing sufficient time for self-directed learning.15 The limited lectures in a PBL curriculum are not used for “covering” core content but other specific purposes, and are preferably interactive.16
In the days when print was scarce, lecturing was the only viable method of teaching.17 However, students attending a typical lecture cannot sustain their attention for too long. Attempting to reflect upon what was heard will stop further listening. Charismatic lecturers that can inspire and hold attention are few and far between. Hence, the most common activity in the lecture hall is to taking notes, without much thinking. Lecturing assumes knowledge is a quantity that can be transmitted. The reality that students typically experience is more consistent with the constructivist notion that knowledge cannot be transferred by a teacher, but has to be constructed by the learners themselves.18 Lecture givers sometimes justify the effectiveness of lecturing by the ability of students to pass the exam. However, if the students do not actively study the notes after the lecture, much of the contents would be irretrievably lost. When lectures are excessive, some students will not be able to catch up. In contrast, students benefit from active and collaborative approaches like PBL because learning occurs in the classroom and with help from peers. A large meta-analysis of undergraduate STEM students comparing traditional lecturing versus active learning found active learning methods to produce higher scores and lower failure rates.19 A commentary on this study stated that any college or university teaching its STEM courses by traditional lectures is providing an inferior education to its students.20
Students taught by lectures prepare for exams typically by going over the notes repeatedly. This is surface learning which does not foster knowledge retention after the exam. PBL learning begins by using prior knowledge to understand a new problem. Cognitive psychology shows new information is retained best if it can be organized around known reference points.21 PBL’s self-directed acquisition of knowledge is active learning as it involves intentional engagement and purposeful observation of knowledge resources with critical reflection on its applicability to the problem.22 In contrast to passive hearing of lectures, active learning produces longer retention through generating distinctive sensorimotor associations that encode the event in the memory for later retrieval.23 After self-directed learning, PBL students reconvene to put together their independent findings - this active process of elaboration helps transfer information into long term memory.24 Additionally, PBL trigger problems based on authentic workplace scenarios should aid the transfer of knowledge to the clinical context, compared to learning from the textbook.
In tandem with the rise of PBL in the last 50 years, education has shifted to learner-centred approaches, competency-based and outcome-based learning. One result is that faculty are no longer dispensers of information but take the role of advisors, mentors and guides.25 Approaches such as PBL (and not lecturing) are used where the program learning outcomes include future ready graduates with 21st century skills such as creativity, problem solving, communication, teamwork, and lifelong learning. Our students grew up in the internet era where a vast amount of updated knowledge is readily available. The most important skill they need now is not listening to lectures or rote learning, but the ability to ask the right questions, acquire knowledge from the right sources and apply it to the problem. In the words of education reformer John Dewey: “If we teach today’s students as we taught yesterday’s, we rob them of tomorrow”.26
Students Only Go Through the Motions of PBL
Traditional lecture-based curricula are characterized by a high number of lectures. When a traditional school adopts PBL, one noticeable change is a significant reduction in lectures to enable independent and active learning.7 Schools inaugurated with a PBL curriculum will have a relatively lower number of lectures. However, in either case, if the number of lectures were to increase,4,5 PBL learning will be severely impacted. If the timetable is packed with lectures, there is little time for independent study. Every hour of lecture requires several hours of study and revision without which the content would be forgotten. When lectures increase beyond a tipping point, students do not have enough time for the self-directed learning required by each PBL problem. In such a dysfunctional PBL curriculum,27 students may study each PBL topic superficially, or allocate topics among group members. Some may obtain notes from their seniors to give an appearance of self-study. Others will be mostly silent or speak minimally upon prompting. Intervention by the facilitator will not be able to help because the source of the problem is not the students but the implementation of PBL on top of a lecture-packed curriculum.
Another reason students only go through the motions of PBL is when the assessment is traditional and hence misaligned with the outcomes and philosophy of PBL. In a lecture-based, exam-centered curriculum, the test items are usually isolated facts with little problem-solving or integration of basic science with clinical sciences. When it is possible to pass the exam with simple factual recall, PBL students do not have incentive for deep discussions involving problem solving and critical thinking. In lecture-based curricula, frequent summative assessments are seen as necessary to motivate learning. In reality these assessments are more likely to stop new learning while steering students towards memorization of notes. Hence, if there is a summative quiz just before PBL, many students will spend more time on the quiz than learn for PBL. Finally, if lectures were to increase in a PBL curriculum, the proportion of assessment items from lectures will also increase4 until eventually it becomes possible to pass the entire exam without studying PBL content. This will demotivate students from even attending PBL sessions, much less to study for it.
In line with PBL learning, students should be tested on important big concepts, correlation of basic sciences to clinical observations, and clinical reasoning. Since PBL is problem-based, assessment should be similarly structured. The use of clinical scenarios in test questions can test recognition of key words, ability to generate hypotheses, multidisciplinary integration and clinical application. Modified essay questions are suitable for this, using scenarios the students had not received before. However, the questions must be checked that they are testing problem solving rather than simple factual recall. Multiple choice questions (MCQs) have been criticized for testing isolated facts but it can be constructed to assess cognitive skills, including problem solving and application by using a question stem scenario.28 Extended matching questions with options that can be used more than once or not at all, can be based on several clinical scenarios – this can test higher order thinking skills with less of the guessing and cue seeking associated with MCQs.29 Finally, the reporting of final results as pass-fail rather than a range of grades is consistent with the PBL approach of fostering collaboration rather than competition.30 Hence, assessment compatible with PBL motivates students to fully engage in PBL, rather than just going through the motions of doing it.
They Will Not Cover All They Need to Know
The 20th century saw a knowledge explosion, especially in the fields of genetics, molecular and cellular biology. One result is basic scientists adding new knowledge to their preclinical teaching, some of which may not even be needed by an intern. As the increase in medical knowledge is exponential, it is not possible to keep adding more material or time to the curriculum. The most critical skill to learn is how to find and apply information to solve new problems, not remembering voluminous information with a limited “shelf life”.31 It was estimated that by 2020, medical knowledge will double every 73 days.32 In some fields, what was taught in the first year might be obsolete by the time of graduation. Some of the information our students will need is yet to be discovered. The mindset that all new knowledge must continually be added to the curriculum will lead to over-bloated curricula with an overwhelming number of assessment items.
Medical education today is no longer for producing students who can recall long lists of undigested facts. Educators trained in the past tend to see the new curricula as “dumbing down” teaching in anatomy and laboratory sciences.33 However, it is an illusion that by covering a topic in a lecture, it can be retained until it is needed. One year after taking three medical first year basic science courses, knowledge loss was found to range from 13% to 47%.34 In contrast, knowledge gained using the PBL approach is not declarative but working knowledge that can be applied back to the clinical context. Furthermore, PBL learning does not proceed via textbook chapters but problem case - different disciplines are understood in combination and not in isolation. PBL learning is consistent with the learning approach expected of students now, which involves asking questions, searching for answers, and evaluating the information found. In the process, it produces critical 21st century skills such as critical thinking, problem solving and interpersonal skills.
Hence, in 1993 the UK General Medical Council (GMC) required medical schools to revise curricula by defining a core of factual information kept to the essential minimum.35 This core fundamentals and principles could be identified from a list of clinical index situations that an intern needs to be competent in, or from a list of clinical tasks during the clinical training years.33 Additionally and consistent with PBL, curriculum design and delivery must take into account modern educational theory and current research.36 The basic medical sciences must be integrated with clinical sciences, with small group learning and opportunities for self-directed learning. There must be training in interpersonal skills to help in relating to patients. Last, the graduate is to be a lifelong learner rather than a finished product, who must adapt to advances in medical knowledge.
Student-Directed Learning Leads to Errors
The traditional model of teaching perceives students as novices who need to be taught by experts, much like empty vessels waiting to be passively filled with information. This line of thinking would conclude that if students were to take ownership of their own learning, they are likely to generate errors in knowledge. Surprisingly, a meta-analysis of undergraduate STEM education showed classes with traditional lecturing were 1.5 times more likely to fail than were students in classes with active learning.19 The ability to remember information is the result of the learner reviewing and studying it a sufficient number of times37 rather than a direct transfer of knowledge from an expert to a novice.
Evidence does not show PBL’s student-directed learning approach leads to errors. A scoping review covering studies over 30 years and six continents comparing PBL versus traditional lecture-based teaching found PBL students’ knowledge retention and academic performance were not worse, and in many studies were better.2 A meta-analysis comparing the graduates of medical schools using PBL versus traditional curricula found physicians from PBL schools had greater competencies especially in communication skills, coping with uncertainty and self-directed continuing learning.38
PBL is sometimes erroneously perceived as students studying on their own. PBL students are not left to themselves but placed in a constructivist learning environment, which has been defined as ‘a place where learners may work together and support each other as they use a variety of tools and information resources in their guided pursuit of learning goals and problem-solving activities’.39 Students are provided with a room equipped with information resources and whiteboards to support intellectual discourse. They are given an ill-structured problem that will trigger them to study relevant topics in the curriculum. They are with a facilitator who acts as a coach to help the group process. There is expert guidance embedded, such as in lectures and practical sessions, that provides the required background or complementary information. These work together in tandem to reduce the cognitive load. Hence, PBL students are not left on their own but guided in an environment with various scaffolds that maximize learning.40
Our Students are Too Immature to Use PBL
PBL may have been initially implemented in post-baccalaureate programs, but it is now used at almost all educational levels, even in grade school. A comparison of a 4th grade science course taught by PBL versus direct instruction found that PBL students achieved comparable scores but stayed engaged longer, generated more problem-solving strategies and more viewed themselves as scientists.41 PBL is not limited by age but rather it is the natural way humans learn from a young age- by encountering problems first. PBL is not an approach for mature students but a way to become mature learners.
Like in many parts of the world, the undergraduate medical programs in Malaysia admits candidates from pre-university studies. These students come from schools that mostly practised didactic teaching. Yet, when they encountered the more student-centred approach in medical schools, it was observed that the vast majority were able to adapt quickly.42 Even for Asians who are perceived to be quiet in the classroom – it was noticed that once they see their opinions are valued, they become more vocal to contribute.43 Students often cope with change better than their teachers. Our students grew up in a very rapidly changing world. They understand the need to change their way of learning because national educational systems are moving from a teacher-centred approach to one that produces human capital who can be innovative thinkers and creative problem solvers.
The PBL Facilitators are Incompetent
Of all the inputs necessary for a PBL curriculum, the most difficult to prepare for are the facilitators. An inept facilitator can hinder student learning or turn PBL into a didactic session. Hence, attempts at PBL can fail for lack of properly trained facilitators.44 For faculty that have spent years in conventional teaching, the most critical element of facilitator training is in pedagogy – the current understanding of how knowledge is created and the resultant shifts in the role of the teacher in the classroom. Hence, training in the educational philosophy of PBL must come first before the steps for conducting a PBL session.
Faculty from lecture-based curricula may find it unnerving to be in a class studying topics outside their specialty, making them no longer authoritative figures. They may lack the ability to forge a good working relationship with students in a small group. Most will certainly not know how to help students activate prior knowledge, encourage elaboration, or improve communication. These are areas new facilitators need to be trained in, in addition to the PBL philosophy. Existing facilitators need a refresher on PBL philosophy before going into advanced topics. As an example, the Sherbrooke Medical School (Canada) prepares PBL facilitators by offering a 2-day workshop in educational principles, a 1-year basic training in medical pedagogy, a 1-day workshop on PBL and 3-day training in PBL facilitating.45 At the China Medical University (Taiwan), every year the Centre for Faculty Development conducts two whole-day workshops in PBL theory and demonstration, and three half-day workshops on specific PBL topics such as group dynamics management, trigger writing and PBL assessment.46
Faculty training is critical for PBL schools, not least for having sufficient competent facilitators. The regularity of the workshops and its pedagogic focus makes it crucial for the training to be supported by professional medical educators, or the university’s academic development unit. The need for such training and possibly funding for it means the school head needs to be supportive of the PBL philosophy and possesses the administrative, financial, and political commitment to maintain PBL. Strong and innovative leadership is particularly required where the pressure to revert to tradition is always present.47 Conversely, the lack of such administrative support will see the demise of PBL.48 A funded and functioning PBL facilitator training programme is crucial for faculty to imbibe the PBL philosophy and maximize learning in PBL groups.
The PBL Problems are Not Improved and PBL Content Overlap with Lectures
In traditional lecture-based curricula, courses and teachers are organized into departments and programs that offer courses, but which rarely communicate with one another.49 Upon adoption of PBL, the preclinical curriculum is usually organised into Blocks, Modules or Units, with two or three PBL sessions a week for groups to work on a problem trigger. There are instances where a PBL Coordinator or Committee is appointed but with no jurisdiction over lecture content and other classes still delivered by faculty from self-governing departments. In such schools, faculty may be largely unaware of what students are learning via PBL and hence deliver lectures on the same topics. This curtails active student acquisition of knowledge, resulting in regurgitation of lecture notes during PBL sessions. In such a setup, trigger problems are typically reused without review, and PBL content not tested in exams because one Committee (much less one Coordinator) is insufficient to review or write test questions for all the Blocks in the course.
PBL’s integrated learning cuts across departmental boundaries. The content of the weekly problems cannot be repeated in other classes. Multidisciplinary PBL embedded in an integrated block system requires a different support system. PBL schools have addressed this by implementing Block Committees, also variously called Curriculum Design or Planning Group.50,51 This consists of basic scientists from each represented discipline and the relevant clinician32 with possibly a curriculum coordinator who provides expertise in education.51 This multidisciplinary team maps topics, produces content, sequences material, selects pedagogy, assigns staff to teach and coordinates assessment items. They edit or rewrite trigger problems and produce a Facilitator Guide for each problem case. This Guide explains the clinical scenario, learning objectives, relationship with other teaching inputs, ways to prompt students towards the key points and how to pace the discussion. They also design supporting classes using the most appropriate pedagogy, which can include lectures.52 They ensure the trigger learning objectives are coordinated with and not duplicated by other classes such as laboratory or clinical skill sessions, seminars, or computer guided instruction. The instructors of these classes are briefed on how the PBL problem relates to the week objectives and other classes. Lecture givers are given the expected content and their lectures are monitored for effectiveness.
PBL content is often not assessed because while every class has an instructor who teaches and assesses, PBL belongs to no one person. The Block Committee, having knowledge of the Block’s content, is in a good position to map the assessment topics. They can ensure that the assessment is compatible with PBL’s learning approach and importantly, commission the writing of questions on PBL content. Last, the Committee collects student feedback to allow them to continually re-evaluate, redesign and reimplement each Block, guided by feedback. Hence, a Block-based infrastructure is required to sustain a functioning PBL curriculum.
A PBL Curriculum is Too Resource- and Time-Intensive
There is a perception that a PBL curriculum will cost too much in terms of infrastructure costs and staff time. However, there are ways to optimize costs and time. Comparison studies have shown PBL curricula to be cost-feasible. In terms of infrastructure, PBL groups require a room each. For existing schools, there is no need to build new rooms because the currently available rooms can be used judiciously. Some schools repurpose rooms for PBL while others make do with a limited number of rooms by holding PBL sessions at different times for different groups. The number of rooms can be kept in check by having no less than 8 students per group. A new medical school found that construction of 8 PBL rooms represented only 4.6% of overall infrastructure costs.53 For this school that employed part-time facilitators, almost 90% of recurring costs were for facilitator salaries- this outlay does not apply for schools whose facilitators are full-time academic staff.
While a lecture can be given by one staff to a large number of students, a PBL curriculum requires one staff per small group of students. Nevertheless, a projection made by one school showed that for a PBL curriculum, the time faculty will spend on educational activities was similar to a traditional subject-based curriculum (17.41 hours per student per week for PBL versus 17.85 hours for traditional).54 Hence though PBL schools can incur higher costs, many schools implement PBL in a cost-feasible manner.
Conclusion
PBL is a whole curriculum philosophy requiring all curricular elements to support active or collaborative learning. This is often at odds with the traditional model of lecture-based teaching delivered by departments. Without complementary organizational infrastructure, teaching-learning activities and assessment methods, faculty often develop resistance towards PBL. PBL practitioners who face such opposition need to handle objections with evidence-based reasons to foster faculty buy-in for PBL. With institutional support, investment in staff pedagogic training and appropriate organizational structure, PBL can be implemented cost-effectively and sustainably to produce adept health professionals for the 21st century.
Ethics Approval Statement
Ethics approval was not required for this research based on review of published and publicly reported literature.
Acknowledgments
The support of Universiti Malaysia Sarawak in the submission of this work is acknowledged.
Disclosure
The author has no competing interests to declare that are relevant to the content of this article.
References
1. Wood DF. Problem based learning. BMJ. 2008;336(7651):971. doi:10.1136/bmj.39546.716053.80
2. Trullas JC, Blay C, Sarri E, Pujol R. Effectiveness of problem-based learning methodology in undergraduate medical education: a scoping review. BMC Med Educ. 2022;22(1):104. doi:10.1186/s12909-022-03154-8
3. Marra R, Jonassen DH, Palmer B, Luft S. Why problem-based learning works: theoretical foundations. J Excell Coll Teach. 2014;25(3–4):221–238.
4. Roslani AM, Sein KT, Nordin R. Review of the phase I and phase II teaching programmes in the school of medical sciences, universiti Sains Malaysia. Med J Malaysia. 1989;44(1):75–82.
5. Malik AS, Malik RH. The undergraduate curriculum of faculty of medicine and health sciences, universiti Malaysia Sarawak in terms of Harden’s 10 questions. Med Teach. 2002;24(6):616–621. doi:10.1080/0142159021000063934
6. Yee HY. Evolution of PBL in the international medical University. IeJSME. 2012;6:S38–S47. doi:10.56026/imu.6.Suppl1.S38
7. Azila NMA, Sim SM. 馬來西亞醫學院校“問題導向學習”之現況. [The status of problem-based learning in the medical schools in Malaysia]. J Med Educ. 2005;9(2):121–130. Chinese. doi:10.6145/jme.200506_9(2).0002
8. Kwan CY. A thorny path: the developmental course of problem-based learning for health sciences education in Asia. Adv Health Sci Educ Theory Pract. 2019;24(5):893–901. doi:10.1007/s10459-019-09920-6
9. Karlsen KA, Vik T, Westin S. Det problembaserte legestudiet i Trondheim--ble det slik det var planlagt? [The problem-based medical curriculum in Trondheim--did it turn out as planned?]. Tidsskr nor Laegeforen. 2000;120(19):2269–2273. Norwegian.
10. Schwartz PL, Loten EG, Miller AP. Curriculum reform at the University of Otago Medical School. Acad Med. 1999;74(6):675–679. doi:10.1097/00001888-199906000-00014
11. Servant VFC. The many roads to problem-based learning: a cross-disciplinary overview of PBL in Asian institutions. In: Mohd-Yusof A, Borhan de G, Kolmos P, editors. PBL Across Cultures. Allborg University Press; 2013:395.
12. Kwan C-Y, Tam L. 評論:混雜型問題導向學習–顧其名可知其義? [Commentary: hybrid PBL-What is in a Name?]. J Med Educ. 2009;13(3):216–223. Chinese. doi:10.6145/jme.200909_13(3).0007
13. Camp G. Problem-based learning: a paradigm shift or a passing fad?. Med Educ Online. 1996;1(1):4282. doi:10.3402/meo.v1i.4282
14. van Berkel H, Schmidt H. On the additional value of lectures in a problem-based curriculum. Educ Health. 2005;18(1):45–61. doi:10.1080/13576280500042648
15. Albanese MA, Mitchell S. Problem-based learning: a review of literature on its outcomes and implementation issues. Acad Med. 1993;68(1):52–81. doi:10.1097/00001888-199301000-00012
16. Fyrenius A, Bergdahl B, Silén C. Lectures in problem-based learning—Why, when and how? An example of interactive lecturing that stimulates meaningful learning. Med Teach. 2005;27(1):61–65. doi:10.1080/01421590400016365
17. Schmidt HG, Wagener SL, Smeets GA, Keemink LM, van der Molen HT. On the Use and misuse of lectures in higher education. Health Professions Educ. 2015;1(1):12–18. doi:10.1016/j.hpe.2015.11.010
18. Prince MJ, Felder RM. Inductive teaching and learning methods: definitions, comparisons, and research bases. J Eng Educ. 2006;95(2):123–138. doi:10.1002/j.2168-9830.2006.tb00884.x
19. Freeman S, Eddy SL, McDonough M, et al. Active learning increases student performance in science, engineering, and mathematics. Proc Natl Acad Sci U S A. 2014;111(23):8410–8415. doi:10.1073/pnas.1319030111
20. Wieman CE. Large-scale comparison of science teaching methods sends clear message. Proc Natl Acad Sci U S A. 2014;111(23):8319–8320. doi:10.1073/pnas.1407304111
21. Afflerbach PP. The influence of prior knowledge on expert readers’ main idea construction strategies. Read Res Q. 1990;25(1):31–46. doi:10.2307/747986
22. Graffam B. Active learning in medical education: strategies for beginning implementation. Med Teach. 2007;29(1):38–42. doi:10.1080/01421590601176398
23. Markant DB, Ruggeri A, Gureckis TM, Xu F. Enhanced memory as a common effect of active learning. Mind Brain Educ. 2016;10(3):142–152. doi:10.1111/mbe.12117
24. Khalil MK, Elkhider IA. Applying learning theories and instructional design models for effective instruction. Adv Physiol Educ Apr. 2016;40(2):147–156. doi:10.1152/advan.00138.2015
25. Gruppen LD. Outcome-based medical education: implications, opportunities, and challenges. Korean J Med Educ. 2012;24(4):281–285. doi:10.3946/kjme.2012.24.4.281
26. Ledertoug MM, Paarup N. Engaging Education: the Foundation for Wellbeing and Academic Achievement. In: Kern ML, Wehmeyer ML, editors. The Palgrave Handbook of Positive Education. Springer International Publishing; 2021:441–472.
27. Lim WK. Dysfunctional problem-based learning curricula: resolving the problem. BMC Med Educ. 2012;12:89. doi:10.1186/1472-6920-12-89
28. Azer SA. Assessment in a problem‐based learning course: twelve tips for constructing multiple choice questions that test students’ cognitive skills. Biochem Mol Biol Educ. 2003;2003:31.
29. Fenderson BA, Damjanov I, Robeson MR, Veloski JJ, Rubin E. The virtues of extended matching and uncued tests as alternatives to multiple choice questions. Hum Pathol. 1997;28(5):526–532. doi:10.1016/s0046-8177(97)90073-3
30. White CB, Fantone JC. Pass-fail grading: laying the foundation for self-regulated learning. Adv Health Sci Educ Theory Pract. 2010;15(4):469–477. doi:10.1007/s10459-009-9211-1
31. Hughes IE, Wood EJ. Does problem-based learning work? And whose fault is it if it doesn’t? A response to the article by R. H. Glew. Biochem Mol Biol Educ. 2003;31(4):257–259. doi:10.1002/bmb.2003.494031040247
32. Densen P. Challenges and opportunities facing medical education. Trans Am Clin Climatol Assoc. 2011;122:48–58.
33. Burge SM. Undergraduate medical curricula: are students being trained to meet future service needs?. Clin Med Lond. 2003;3(3):243–246. doi:10.7861/clinmedicine.3-3-243
34. D’Eon MF. Knowledge loss of medical students on first year basic science courses at the University of Saskatchewan. BMC Med Educ. 2006;6:5. doi:10.1186/1472-6920-6-5
35. Tomorrow’s Doctors. Recommendations on Undergraduate Medical Curriculum (General Medical Council); 1993.
36. Tomorrow’s Doctors. Recommendations on Undergraduate Medical Curriculum (General Medical Council); 2009.
37. Ebbinghaus H. Memory: a Contribution to Experimental Psychology. Anna Neurosci. 2013;20(4). doi:10.5214/ans.0972.7531.200408
38. Koh GC, Khoo HE, Wong ML, Koh D. The effects of problem-based learning during medical school on physician competency: a systematic review. CMAJ. 2008;178(1):34–41. doi:10.1503/cmaj.070565
39. Wilson BG. Constructivist Learning Environments: Case Studies in Instructional Design. Educational technology Publications; 1996.
40. Hmelo-Silver CE, Duncan RG, Chinn CA. Scaffolding and Achievement in Problem-Based and Inquiry Learning: a Response to Kirschner, Sweller, and. Educ Psychologist. 2007;42(2):99–107. doi:10.1080/00461520701263368
41. Drake KN, Long D. Rebecca’s in the dark: a comparative study of problem-based learning and direct instruction/experiential learning in two 4th-grade classrooms. J Element Sci Educ. 2009;21(1):1–16. doi:10.1007/BF03174712
42. Lim VK. Medical education in Malaysia. Med Teach. 2008;30(2):119–123. doi:10.1080/01421590801942102
43. Azila NMA, Sim SM, Tan CPL, Alhady SF. Problem-based Learning (PBL): making an impact in Education. J Health Translat Med. 1999;4(2):94–103. doi:10.22452/jummec.vol4no2.6
44. Walton HJ, Matthews MB. Essentials of problem-based learning. Med Educ. 1989;23(6):542–558. doi:10.1111/j.1365-2923.1989.tb01581.x
45. Grand’Maison P, Des Marchais JE. Preparing faculty to teach in a problem-based learning curriculum: the Sherbrooke experience. CMAJ. 1991;144(5):557–562.
46. L-T W, Hsu L-C, Sun -S-S, H-C W, M-G T, Kwan C-Y. The change of student perception toward PBL in a medical school with a hybrid-PBL preclinical curriculum in Taiwan. J Med Educ. 2012;16(3):97–113. doi:10.6145/jme.201209_16(3).0001
47. Des Marchais JE. A student-centred, problem-based curriculum: 5 years’ experience. CMAJ. 1993;148(9):1567–1572.
48. Achike FI. 醫學課程問題導向學習效益之維持. [Sustaining the effectiveness of PBL in a medical curriculum]. J Med Educ. 2003;7(3):298–302. Chinese. doi:10.6145/jme.200309_7(3).0011
49. Barr RB, Tagg J. From teaching to learning — a new paradigm for undergraduate education. Change. 1995;27(6):12–26. doi:10.1080/00091383.1995.10544672
50. Servant-Miklos VFC. Fifty years on: a retrospective on the world’s first problem-based learning programme at McMaster University Medical School. Health Professions Educ. 2019;5(1):3–12. doi:10.1016/j.hpe.2018.04.002
51. Armstrong EG. A Hybird Model of Problem-based Learning. In: Boud G, editor. The Challenge of Problem-Based Learning.
52. Taylor D, Miflin B. Problem-based learning: where are we now?. Med Teach. 2008;30(8):742–763. doi:10.1080/01421590802217199
53. Finucane P, Shannon W, McGrath D. The financial costs of delivering problem-based learning in a new, graduate-entry medical programme. Med Educ. 2009;43(6):594–598. doi:10.1111/j.1365-2923.2009.03373.x
54. Hamdy H, Agamy E. Is running a problem-based learning curriculum more expensive than a traditional subject-based curriculum?. Med Teach. 2011;33(9):e509–e514. doi:10.3109/0142159x.2011.599451
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.