")
Back to Journals » Cancer Management and Research » Volume 14
Quality of Life and Its Associated Factors Among Cancer Patients Receiving Chemotherapy at Oncology Hospitals in Vietnam After the Third Wave of the COVID-19 Pandemic
Authors Nguyen HTH , Duong KL , Nguyen ST, Trinh Q, Hoang HTL, Phung TQ, Lin HW, Nguyen HTL
Received 9 April 2022
Accepted for publication 30 July 2022
Published 11 August 2022 Volume 2022:14 Pages 2429—2444
DOI https://doi.org/10.2147/CMAR.S370034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Hanh TH Nguyen,1,2 Khanh Linh Duong,2 Son T Nguyen,2 Quy Trinh,2 Hao TL Hoang,3 Toan Q Phung,4 Hsiang-Wen Lin,1,5 Huong TL Nguyen2
1School of Pharmacy and Graduate Institute, China Medical University, Taichung, Taiwan; 2Department of Clinical Pharmacy, Hanoi University of Pharmacy, Hanoi, Vietnam; 3Pharmacy Department, Hanoi Oncology Hospital, Hanoi, Vietnam; 4Pharmacy Department, Vietnam National Cancer Hospital, Hanoi, Vietnam; 5Department of Pharmacy, China Medical University Hospital, Taichung, Taiwan
Correspondence: Huong TL Nguyen, Hanoi University of Pharmacy, 13-15 Le Thanh Tong, Hoan Kiem, Hanoi, Vietnam, Tel +84 904 308 406, Fax +84 243 826 4464, Email [email protected]
Purpose: This study aimed to evaluate the health-related quality of life (HRQOL) of cancer patients receiving chemotherapy and identify associated factors affecting the HRQOL after the third wave of the COVID-19 pandemic in Vietnam.
Patients and Methods: Patients with solid cancers receiving chemotherapy at two oncology hospitals in Vietnam during April and May 2021 were included. The European Organisation for Research and Treatment of Cancer Core Quality of Life Questionnaire version 3 was used to measure the HRQOL. Three questions were asked to explore patients’ concern levels about contracting COVID-19, delaying chemotherapy, or not controlling cancer well. One question was used to explore whether patients were concerned about cancer progression or COVID-19 infection more, or equally, or had no concern about both. Multiple regression models were conducted to examine factors associated with the global health status (GHS) score.
Results: Of 270 included patients, mean (Standard deviation [SD]) GHS was 56.7 (20.8). Among the functional statuses, social functioning (SF) had the lowest score of 63.6 (29.2). The symptoms with the highest means were insomnia and fatigue, obtaining the score of 38.5 (31.7) and 37.3 (29.2), respectively. The mean of financial difficulties was 54.1 (32.2). In univariate analysis, high concerns about contracting COVID-19, delaying chemotherapy, not controlling cancer well, or more concern about either cancer or COVID-19 over the other were associated with worse GHS, physical functioning, emotional functioning, and SF. In multivariate analysis, those concerns and no income were significantly related to lower GHS scores besides the non-modifiable factors, such as female gender and some cancer types.
Conclusion: Patients at the high concern levels, or with more concern about either cancer or COVID-19 over the other had poorer HRQOL. Interventions to address the concerns are required to improve their HRQOL, particularly for women, those without income, or with some specific cancers.
Keywords: chemotherapy, COVID-19, EORTC QLQ-C30, quality of life, low economic status
Introduction
Cancer is an important cause of morbidity and mortality worldwide with an estimated 19.3 million new cases and 10 million deaths from cancer in 2020.1 It is even projected to have 28.4 million new cases in 2040.1 While improving overall survival and disease-free survival have always been the primary focus of cancer treatment, health-related quality of life (HRQOL) is considered as one of the important outcomes. From patients’ perspective, many cancer patients prefer improving HRQOL rather than improving the length of life, and their current HRQOL could affect their choices of subsequent treatment.2 Clinicians also perceive HRQOL as important as survival when making the decision about cancer patients’ treatment plans.3 Additionally, HRQOL can help predict the prognosis or decide on supportive treatment for cancer patients.4
HRQOL is a multidimensional construct evaluated by patients using aspects related to their health statuses, including physical, emotional, social, and cognitive functions, and symptoms and side effects of therapy.3 When severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has spread globally, causing the coronavirus disease 2019 (COVID-19) pandemic, cancer patients’ HRQOL could have deteriorated because many aspects of their daily life and health statuses have been dramatically impacted.5 Importantly, studies have shown that cancer patients were more likely to be infected with COVID-19 because they seemed sicker, and had a higher mortality risk.6–8 Further, the fear for COVID-19 and anxiety have indirectly impacted cancer patients’ psychological health.8,9
In reality, cancer patients receiving chemotherapy have to periodically visit the hospital either for a health check-up and/or receiving chemotherapy or other therapies. Their frequent hospital visits would increase the risk of COVID-19 infection due to the higher rates of transmission at hospitals.10,11 Particularly, chemotherapy is commonly recognized as an immune-compromising treatment.8,12 Thus, patients on chemotherapy can struggle with the dilemma of continuing their chemotherapy but increasing the risk of infection or staying at home to delay their cancer treatments. Either choice could make them worried and affect their levels of HRQOL. Furthermore, chemotherapy is considered one of the most influential cancer treatments in terms of HRQOL (ie, positive and negative directions) through its effect of alleviating cancer symptoms or resulting adverse effects.13–15
Some studies have explored the influence of the COVID-19 pandemic on HRQOL among cancer patients in several countries.16–20 While the studies conducted in the Netherlands or Poland have demonstrated negative impacts of the COVID-19 pandemic on HRQOL,17,18 a study in Denmark by Jeppesen et al and another study by Kurzhals et al in Germany have shown preserved HRQOL.16,20 These HRQOL-related studies have been conducted in European countries with the mixed results due to their geographical variations in the rates of COVID-19 cases or different control approaches of local governments for the pandemic management. In contrast, no studies on the influence of COVID-19 on cancer patients’ HRQOL in Vietnam have been available yet.
In Vietnam, the reported number of COVID-19 cases from the beginning of the pandemic till April 2021 was relatively low (ie, 2631 confirmed cases including 910 cases in the third wave, and 35 death cases were reported, but none was reported in the third wave of the pandemic),21 as compared to that in other countries (eg, the European countries or nearby countries, such as Malaysia or Philippines, with thousands of new cases/week).22 At that time, a small number of the population (approximately 52,000 people), comprising people in the first priority groups, eg, health-care workers and front-line workers, were given the first COVID-19 vaccine shot.21 In contrast, cumulative 15 million people have been placed under quarantine, in which infected people, those in direct contact with an infected person, or people from abroad were required to undergo a 14-day central quarantine. Other strict measurements in response to the pandemic, including lockdown in some targeted communities and social distancing at the subnational level determined based on the local outbreak situation and risk assessment, have also been applied.21
At the time of the third wave of the COVID-19 pandemic in Vietnam, HRQOL of cancer patients receiving active chemotherapy treatments could be affected due to the concerns of local transmission and roll planning of strategies in policies responding to the pandemic among the not vaccinated population. Therefore, we conducted this study in Vietnam to evaluate the HRQOL of cancer patients receiving chemotherapy and examine the associations between HRQOL and socio-demographic factors, as well as concerns about COVID-19 infection or cancer-related problems, during the pandemic.
Methods
Study Design and Settings
A cross-sectional, observational study in two specialized oncology hospitals in Hanoi (the capital of Vietnam) during April and May 2021 was conducted. These two oncology hospitals served a high volume of patients for the residents in Hanoi and other northern provinces of Vietnam.
Patients and Recruitment
During the study period, all cancer patients admitted to the aforementioned two hospitals for chemotherapy treatment represented the target population. Particularly, those who were diagnosed with solid tumors, admitted for systemic chemotherapy from the second cycle onwards, and aged 18-year-old and older were included. Those patients who were diagnosed with two concurrent cancers, had received other treatment modalities, such as targeted therapy, immunotherapy, hormone therapy, and radiation therapy, between the prior chemotherapy cycle and the interview, refused to participate or did not have the ability to independently answer the questionnaires with paper and pen (eg, who cannot read and write in Vietnamese, or need family members’ help to answer, or have uncontrolled psychiatric disorders) were excluded from the analysis.
The following formula was used to calculate the sample size: N = Z1-α/22 SD2/d2,23 with type 1 error of 0.05 (ie, Z1-α/2 is 1.96), the standard deviation (SD) of 24.2 according to the reference values supplied by the EORTC Quality of life group for cancer patients at all stages, and d, the absolute error, was decided at 5% of the reference mean (61.3).24 Although a sample of 240 patients was required, we expanded it to 25% more expected samples to avoid the failure of data collection or missing data. Finally, 300 patients were expected for data collection.
During the COVID-19 pandemic, patients’ direct contact was restricted once a while, especially when certain levels of lockdown and social distancing were required in Vietnamese hospitals. Therefore, we tried to recruit as many patients as possible throughout the time allowed for patients to be contacted directly. Eventually, the study enrollment was stopped in May 2021 when new COVID-19 cases were reported in Hanoi, and the hospitals’ restriction for patient contact was applied.
Data Collection and Questionnaire
Patients who agreed to join the study were asked to complete a self-reported questionnaire with paper and pencil after they signed the informed consent. This study was approved by the Ethics Committee of Hanoi Oncology Hospital (Approval number: 43-QĐ/HĐĐĐ). The questionnaire included the demographic characteristics (eg, age, sex, marital status, education, occupation, monthly personal income, living areas, and insurance coverage), their quality of life using the EORTC QLQ-C30 version 3,25 and four questions regarding their concerns of COVID-19 and chemotherapy treatment. It took approximately 30 minutes to complete the whole questionnaire.
As for demographic characteristics, age was categorized into three groups: ≤40 years (young adults), more than 40–60 years (middle-aged adults), and >60 years (older adults). For monthly personal income, patients were asked to choose among the levels of income, including no income, having an income of <5 million VND (approximately equivalent to 220 USD), or having income from 5 million VND, with the cut-off point being decided based on the rounded up national minimum wage at the study time. Patients were asked about living in Hanoi city where the hospitals were located, or in other provinces.
As for patients’ quality of life, the EORTC QLQ-C30 version 3 in Vietnamese language was offered by the EORTC Quality of Life Group, where the items evaluate GHS, five functions (physical functioning [PF], role functioning [RF], emotional functioning [EF], cognitive functioning [CF], and social functioning [SF]), eight symptoms (fatigue, nausea and vomiting, pain, dyspnea, insomnia, appetite loss, constipation, and diarrhea), and financial difficulties. The scores ranged from 0 to 100, with the higher scores representing better global quality of life and functions but the worse symptoms and financial difficulties.26 These scores would be reported for the whole study population and compared across patients’ characteristics. The difference in GHS score of 4–10 points was considered minimally clinically relevant.27 The Cronbach’s alpha for multi-item scales (GHS, five functions, fatigue, pain, and nausea or vomiting) were calculated. The value of the GHS scale was 0.93, and those of the other functional and symptom scales ranged from 0.76 to 0.89, except for CF (0.58) and SF (0.68).
Four questions were created by the research team after compiling the items from literature18,28–30 and the clinical experiences from hospital settings to understand patients’ concerns during the COVID-19 pandemic. The first three questions asked patients about how much they were concerned regarding the potential of contracting COVID-19, delaying their cancer treatment, and controlling cancer not well if their chemotherapy is delayed with five choices as follows: 0 (no concern), 1 (slightly concerned), 2 (quite concerned), 3 (concerned), and 4 (very concerned). Choices 1 and 2 were grouped as low concern category, and choices 3 and 4 were considered high concern category. The fourth question asked whether patients were concerned more about cancer progression or COVID-19 infection with the four following options: more concerned about cancer, more concerned about getting COVID-19, equally concerned, or not concerned at all (no concern). The face validity and content validity were performed by the research team before delivering the questionnaire at the practicing sites. Meanwhile, patients’ clinical characteristics, eg, cancer site, stage, the sequence of chemotherapy, and the previous cancer treatment, were also collected from the corresponding medical records.
Statistical Analysis
Descriptive statistics was used to describe patients’ socio-demographic, clinical data, quality of life scores, and concerns related to cancer treatment and/or the COVID-19 pandemic. The mean and SD were used for the continuous variables, and percentages/frequencies were used for categorical variables. The mean of GHS and functional scores was compared across patients’ socio-demographic characteristics, clinical characteristics, and levels of concerns using the independent samples t-test or a general linear model. Then, multiple linear regression models were performed with GHS as a dependent variable and factors with p values <0.15 in the univariate analysis as independent variables. The responses to the four COVID-19 pandemic-related questions were the individual independent variables used to explore their associations with GHS in the separate models because these factors might be correlated with one another. Multicollinearity among the variables in the multivariate models was explored based on variable inflation factors (VIFs). If VIF is greater than a common threshold of 5, specific management (ie, dropping a variable) would be decided based on related variables. The statistical significance was set at a two-sided p-value of <0.05 for the analysis.
Results
Patient Characteristics
Afterward, 296 copies of the questionnaires were delivered to patients who agreed to join the study. While 10 patients did not complete the entire questionnaire and 16 received other treatment during the previous cycles, finally, 270 participants were included in the data analysis. Of included patients, 51% aged 41–60 years (Table 1). Females accounted for roughly 62% of patients, and nearly a half reported to have no income (46.7%). However, almost all patients (96.6%) had insurance covering their treatments for 80–100% of expenses.
 | 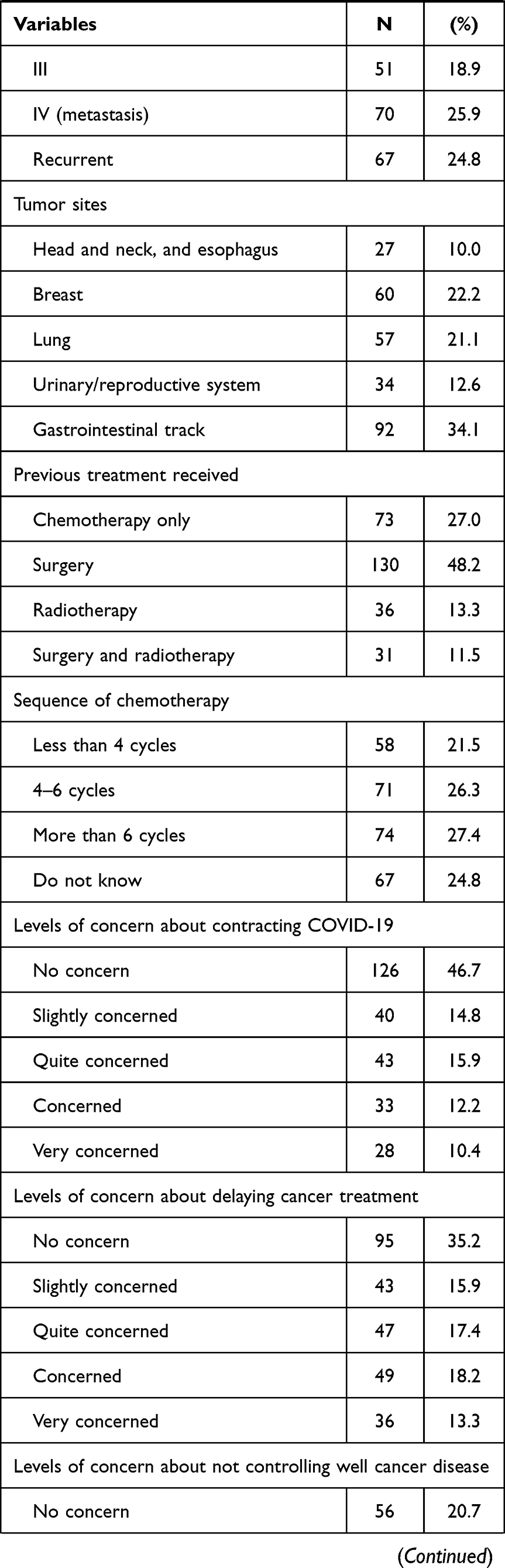 |  |
Table 1 Patient Characteristics (N = 270) |
The most common cancer was gastrointestinal cancer (34.1%), followed by breast cancer (22.2%) and lung cancer (21.1%). Patients with metastases and recurring diseases accounted for 25.9% and 24.8%, respectively, and those in the early stages and stage 3 accounted for 30.4% and 18.9%, respectively. Almost half of the patients received surgery before beginning chemotherapy (48.2%). As for the sequence of current chemotherapy, the distribution was similar in the different cycles of chemotherapy (<4 cycles, 4–6 cycles, >6 cycles, or did not know their cycle sequence).
The majority of enrolled patients were concerned about contracting COVID-19 (53.3%), delaying cancer treatment (64.8%), or not controlling cancer well (79.3%) to various extents. While 41.5% and 38.2% of the patients reported that they had equal concerns about cancer progression and acquiring COVID-19 or more concern about the former, respectively, relatively few patients reported that they had more concern about COVID-19 (8.9%) or had no concern about both cancer and COVID-19 (11.5%).
Health-Related Quality of Life According to EORTC QLQ-C30
As for EORTC-C30 scores, GHS had a mean (SD) of 56.7 (20.8), and individual functional scales from the lowest to highest (mean ± SD) were SF (63.6 ± 29.2), RF (71.3 ± 28.6), PF (78.7 ± 20.4), EF (79.4 ± 23.0), and CF (80.5 ± 21.3) (Table 2). Insomnia, fatigue, and loss of appetite were the symptoms that had the highest scores of 38.5 (31.7), 37.3 (24.9) and 35.1 (30), respectively, while the score for diarrhea was at the lowest, 8.4 (19.4). The mean score for financial difficulties was 54.1 (32.2).
 |
Table 2 The Mean Global Health Status, Functional and Symptom Scores (N = 270) |
The Mean Difference in Health-Related Quality of Life Among Patients with Different Characteristics
In the univariate analysis, the mean GHS scores were significantly higher in males than that in females (p = 0.014), and among those who had personal income compared to those with no income (p = 0.020) (Table 3). Patients who were not concerned about either cancer or COVID-19 had a significantly higher GHS score than those who were concerned about either both or one of the issues (p = 0.015). In contrast, the GHS scores were significantly lower among those who were highly concerned about contracting COVID-19 (p = 0.005), delaying cancer treatment (p = 0.006), or not controlling cancer well (p < 0.001). As for the functional status, the lower score of EF was statistically associated with many socio-clinical factors (ie, age of ≤40 years, female gender, higher education, and living outside Hanoi), but CF was associated with female gender only. There were similar patterns of the associations between the lower scores of PF, EF, and SF with patients’ high concerns about COVID-19 and/or cancer chemotherapy treatment than the counterparts (all p < 0.05). Meanwhile, the mean RF scores were not significantly different among patients with different levels of concern, but those patients with high concern about contracting COVID-19 tended to have lower scores of CF than those with low concern level or no concern at all (p = 0.002). The associations of the socio-clinical factors and concerns with GHS and functional scores were also tested by non-parametric methods with almost similar findings (Supplementary Table S1).
 |  |  |
Table 3 Comparison of Means of Global Health Status and Functional Scales According to Patient Characteristics and Concerns During the COVID-19 Pandemic (N = 270) |
Regarding the scores of symptoms and financial difficulties, higher scores of nausea and vomiting were statistically associated with many social demographic and clinical factors (eg, younger age, female gender, education level of high school and above, living outside Hanoi, working as an employee or merchant, or having <4 cycles of chemotherapy) (all p < 0.05) (Supplementary Table S2). Mean scores of insomnia were also higher among female patients and those living outside Hanoi but lower in those working as an employee or merchant (all p < 0.05). Meanwhile, patients who aged ≤60 years, lived outside Hanoi, had no income, and suffered from breast cancer were statistically associated with more financial difficulties.
While all concerns were not significantly associated with dyspnea and insomnia, mostly the high concern levels showed significant relations with higher means of the remaining symptoms. Being more concerned about cancer progression over COVID-19 infection was also associated with significantly higher means of fatigue and appetite loss compared to the other groups (ie, more concern about COVID-19 infection, equal concern, or no concern). All the concerns were associated with financial difficulties with the higher means in the higher concern levels or in patients concerned more about cancer progression than COVID-19 infection.
Multivariate Analysis Exploring the Factors Associated with GHS
In the multivariable linear regression models aiming to explore the associated factors with GHS, the four concerns about COVID-19 and/or cancer chemotherapies were tested one at a time for four models as follows: concern about contracting COVID-19 (model 1), concern about delaying chemotherapy because of COVID-19 (model 2), concern about not controlling cancer well if chemotherapy is delayed (model 3), and concern about cancer progression or contracting COVID-19 more (model 4) (Table 4). No collinearity was observed in these models. After controlling for other factors, female patients tended to have lower GHS scores, except for model 3 (p = 0.053), and those who had no personal income or were diagnosed with cancers other than that in the urinary/reproductive system tended to report poorer GHS (all p < 0.05). Those patients who showed high concerns tended to have decremental GHS scores by 8.9, 9.1, and 11.5 points as compared to those who showed no concern in models 1, 2 and 3, respectively (p-values = 0.006, 0.004, and 0.001, respectively). Those patients who were concerned about either their cancer or infection of COVID-19 had points decreased by 10.9 or 14.0 than those who did not show any concern at all in model 4.
 |
Table 4 Multiple Linear Regression Analysis of Factors Associated with Global Health Status (N = 270) |
Discussion
This is the first study to describe HRQOL patterns among cancer patients receiving chemotherapy during the COVID-19 pandemic in North Vietnam. Indeed, those patients who were concerned about contracting COVID-19, delaying cancer treatment due to the COVID-19 pandemic, and its negative impacts on cancer control tended to report poor scores of HRQOL.
The mean GHS measured by EORTC QLQ-C30 after the third wave of the COVID-19 pandemic in Vietnam in the current study was relatively low (56.7, SD = 20.8) on the scale of 100 for perfect health as compared with that reported among patients with all types and stages of cancer (61.3, SD = 24.2),24 or general population norm in Western countries (66.1, SD = 21.7).31 While 3.8 million new cases and 64,000 deaths due to COVID-19 globally in the last week of March 2021 were reported,32 the third COVID-19 wave in Vietnam was almost ended with a low volume of confirmed cases and without death cases.21 None of the enrolled patients in this study were ever infected with COVID-19. However, almost all people were not protected by the vaccines; thus, strict strategies, eg, central quarantine, social distancing or lockdown were applied.21 These might have led to patients’ fear, distress, financial difficulties, or other barriers to their daily life activities and cancer treatment process, which, therefore, might cause impaired HRQOL.
The negative influences of the pandemic on HRQOL were demonstrated through the negative associations of the concerns with GHS or functioning scores. In terms of GHS, the concerns related to their cancer and COVID-19 during the pandemic were significantly associated with their worse scores of GHS in both univariate and multivariate analyses. These findings were consistent with that in the prior studies.16,33 In this current study, those patients who were highly concerned about COVID-19 or cancer or showed more concern about either disease reported relatively lower scores of GHS by roughly 10 points, which was commonly assumed as clinically significant.27 Therefore, it is supposed that these patients’ HRQOL could be substantially improved if they were identified in advance and taken care of more efficiently during the pandemic.
In terms of functional status, the current study demonstrated that cancer patients with high concerns had lower EF and PF scores. While no evidence of the influence of the concerns on the PF was found, similar findings about EF have been demonstrated in previous studies, showing that the distress caused by the COVID-19 pandemic could negatively impair cancer patients’ EF scores.34,35 A wide spread of anxiety, distress, and deterioration in mental health during the COVID-19 pandemic was also observed in the general population.36 In comparison, cancer patients could show more concerns because they were more vulnerable to infections and might have a worse prognosis in case of infection.6–8 Those cancer patients on active treatment need to visit hospitals regularly to receive chemotherapy injections. In this case, they can not only exposure themselves to hospital settings with high transmission rates but also might result in an immune-compromised status due to the cytotoxic effects of chemotherapies.8,10–12 As a result, we assumed they were worried about the aforementioned uncertainty that could deteriorate their EF. All these findings highlighted the importance of emotional support for those cancer patients during the pandemic.
On the other hand, SF seemed to be influenced by the pandemic as well. The mean SF score was not only the lowest compared to other functions but also negatively associated with the concerns related to the pandemic. It is assumed that the worst scores of SF might be associated with the recommendations of not gathering or rigorous restrictions taken during the pandemic. Notably, several communities in the North of Vietnam were under lockdown before the study.21 A prior study has shown a significant decline in social function among breast cancer patients on active treatment in the Netherlands during the COVID-19 pandemic.35 Additionally, those patients with the concerns about COVID-19 had worse scores of SF in this study, indicating that their concerns might prevent them from social activities.
Given that the HRQOL was negatively associated with patients’ concerns about the COVID-19 pandemic, one potential explanation for the relatively low GHS score in this study could be that enrolled patients were of low socioeconomic status in a developing country (ie, Vietnam). In fact, the mean GHS in the current study was similar to that of Vietnamese cancer patients reported one year after cancer diagnosis in a study conducted in eight low- and middle-income countries in 2017.37 It was also comparable to the findings from the studies performed in other developing countries, including Malaysia (53.3, SD = 21.4), and Ethiopia (52.7, SD = 20.1), during the time without COVID-19.38,39 In contrast, such GHS score was lower than the reference score offered by EORTC group for cancer patients or that conducted in other countries with higher income, ie, Brazil, Germany, Denmark, or Italy, regardless of the presence of the COVID-19 pandemic.16,24,40,41 Moreover, recent studies exploring the impact of COVID-19 on cancer patients’ HRQOL have shown mixed results with the deterioration of overall quality of life in a study conducted in the Netherlands but preserved overall quality of life in studies in Denmark and Germany.16,17,20 Therefore, the influences of the pandemic seem uncertain, and poor HRQOL appeared to be linked to socioeconomic disparities rather than the COVID-19 pandemic alone.
The financial difficulties reported by patients in this study might also link to the associations between low economic status and poor GHS. The mean score of the financial difficulties in this study (54.1) was comparable with that in other developing country,39 and relatively higher than that in the developed countries (ranging from 5.8 to 19).16,41,42 Especially, approximately half of the patients in this study reported having no income, which could be because they encountered severe symptoms of diseases or frequent treatments, which may prevent them from working. Another possibility could be that the COVID-19 pandemic resulted in more financial issues for the patients, similar to what it caused worldwide. These findings demonstrated a heavy economic burden of the study population, which could have led to impaired HRQOL. Indeed, this study revealed that no personal income was an independent factor associated with worse GHS. These findings were consistent with the previous studies conducted in Vietnam or eight Southeast Asian countries (including Vietnam), which found poor economic situations or financial difficulties of cancer patients as predictors for impaired HRQOL.37,43
Besides the economic problems or concerns during the COVID-19 pandemic, gender and cancer sites were identified as the associated factors, but not cancer stage, in which more advanced stages have been associated with poorer QOL in previous studies.44,45 The included patients could independently answer the questionnaire, suggesting that their health status could be similar between the advanced and early stages. Besides, cancer patients in Vietnam might have low health literacy and perceive cancer as a catastrophic disease regardless of the stages;46 therefore, they might be concerned about cancer of all stages similarly. The finding about gender was in line with the previous studies explaining that female cancer patients tended to have worse HRQOL.43,47 Female patients, in fact, seemed to be more worried during the pandemic.16,19 Therefore, more efforts should be taken to assist these patients in solving their concerns about cancer treatments during the COVID-19 pandemic to improve their HRQOL.
Patients in this study had the highest scores for insomnia and fatigue (38.5 and 37.3, respectively) when compared to the other symptoms. These findings were similar to that in the previous study regardless of high or low GHS scores.41,42 These two symptoms were truly associated with the deterioration of GHS among cancer patients receiving chemotherapy.48–51 While the other common acute adverse events of chemotherapy, eg, nausea and vomiting, or diarrhea, obtained relatively lower scores in this study, one of the explanations could be because patient interviews were at the beginning of a cycle of treatment when the side effects of the previous cycle had subsided.
Some limitations in this study should be acknowledged. First, it included individuals who visited the hospital for treatment following a COVID-19 out-break, which could comprise those who were more concerned about cancer treatment. Second, there was no available controlled data for the study population without the COVID-19 pandemic, and low socioeconomic status could be a reason for poor HRQOL. Therefore, poor HRQOL in this study could not be attributed to the pandemic. Nevertheless, the concerns about COVID-19 were the factors significantly associated with GHS, which was the objective of this study. If HRQOL before the pandemic was available, studies to compare HRQOL before and after the pandemic should be considered to ensure the impact of the pandemic on HRQOL. Third, the questions used to explore patients’ concerns were developed by the research team and considered as an individual item but not a scale (with a summary score for three or four questions), which could introduce bias. However, we could observe consistent patterns of associations between these concerns and GHS score in both univariate and multivariate analyses and the scores of functional scales in the univariate analysis. These may reflex the reliable associations between patients’ concerns and HRQOL.
Conclusion
As in other developing countries, the GHS of Vietnamese cancer patients receiving chemotherapy was low, and financial difficulties were high, particularly among patients with concerns about COVID-19 infection and cancer treatment. These concerns also had detrimental influences on physical, emotional, and social function scores. Therefore, interventions to address these concerns, such as patient counseling and education, should be introduced to promote HRQOL during the pandemic, especially for the more fragile patients, such as female patients, those with no income, or those with some specific types of cancer. Moreover, HRQOL should be measured more frequently or as a part of routine practice for it to be addressed timely.
Data Sharing Statement
While the cleaned data are included in the article, further reasonable request can be directed to the corresponding author.
Ethics Statement
The patients provided their written informed consent to participate in this study. This study was approved by the Ethics Committee of Hanoi Oncology Hospital (Approval number: 43-QĐ/HĐĐĐ), and all procedures involving human participants were performed in accordance with the Declaration of Helsinki.
Acknowledgments
The authors wish to thank the pharmacists in the participated hospitals for their valuable support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Shrestha A, Martin C, Burton M, Walters S, Collins K, Wyld L. Quality of life versus length of life considerations in cancer patients: a systematic literature review. Psycho Oncol. 2019;28(7):1367–1380. doi:10.1002/pon.5054
3. Bottomley A. The cancer patient and quality of life. Oncologist. 2002;7(2):120–125. doi:10.1634/theoncologist.7-2-120
4. Fallowfield L. Quality of life: a new perspective for cancer patients. Nat Rev Cancer. 2002;2(11):873–879. doi:10.1038/nrc930
5. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020;91(1):157–160. doi:10.23750/abm.v91i1.9397
6. Chavez-MacGregor M, Lei X, Zhao H, Scheet P, Giordano SH. Evaluation of COVID-19 mortality and adverse outcomes in US patients with or without cancer. JAMA Oncol. 2022;8(1):69–78. doi:10.1001/jamaoncol.2021.5148
7. Meng Y, Lu W, Guo E, et al. Cancer history is an independent risk factor for mortality in hospitalized COVID-19 patients: a propensity score-matched analysis. J Hematol Oncol. 2020;13(1):75. doi:10.1186/s13045-020-00907-0
8. Liang W, Guan W, Chen R, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21(3):335–337. doi:10.1016/S1470-2045(20)30096-6
9. Momenimovahed Z, Salehiniya H, Hadavandsiri F, Allahqoli L, Günther V, Alkatout I. Psychological distress among cancer patients during COVID-19 pandemic in the world: a systematic review. Front Psychol. 2021;12:682154. doi:10.3389/fpsyg.2021.682154
10. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
11. Yu J, Ouyang W, Chua MLK, Xie C. SARS-CoV-2 transmission in patients with cancer at a tertiary care hospital in Wuhan, China. JAMA Oncol. 2020;6(7):1108–1110. doi:10.1001/jamaoncol.2020.0980
12. American Association for Cancer Research. COVID-19 more frequent, severe in cancer patients. Cancer Discov. 2020;10(6):Of1. doi:10.1158/2159-8290.CD-NB2020-032
13. Glimelius B, Hoffman K, Sjödén PO, et al. Chemotherapy improves survival and quality of life in advanced pancreatic and biliary cancer. Ann Oncol. 1996;7(6):593–600. doi:10.1093/oxfordjournals.annonc.a010676
14. Binotto M, Reinert T, Werutsky G, Zaffaroni F, Schwartsmann G. Health-related quality of life before and during chemotherapy in patients with early-stage breast cancer. Ecancermedicalscience. 2020;14:1007. doi:10.3332/ecancer.2020.1007
15. Ramasubbu SK, Pasricha RK, Nath UK, Rawat VS, Das B. Quality of life and factors affecting it in adult cancer patients undergoing cancer chemotherapy in a tertiary care hospital. Cancer Rep. 2021;4(2):e1312. doi:10.1002/cnr2.1312
16. Jeppesen SS, Bentsen KK, Jørgensen TL, et al. Quality of life in patients with cancer during the COVID-19 pandemic – a Danish cross-sectional study (COPICADS). Acta Oncol. 2021;60(1):4–12. doi:10.1080/0284186X.2020.1830169
17. Bartels M, Gal R, van der Velden JM, Verhoeff JJC, Verlaan JJ, Verkooijen HM. Impact of the COVID-19 pandemic on quality of life and emotional wellbeing in patients with bone metastases treated with radiotherapy: a prospective cohort study. Clin Exp Metastasis. 2021;38(2):209–217. doi:10.1007/s10585-021-10079-x
18. Ciążyńska M, Pabianek M, Szczepaniak K, et al. Quality of life of cancer patients during coronavirus disease (COVID-19) pandemic. Psycho Oncol. 2020;29(9):1377–1379. doi:10.1002/pon.5434
19. Baffert K-A, Darbas T, Lebrun-Ly V, et al. Quality of life of patients with cancer during the COVID-19 pandemic. Vivo. 2021;35(1):663–670. doi:10.21873/invivo.12306
20. Kurzhals JK, Klee G, Busch H, et al. The impact of the Covid-19 pandemic on quality of life in skin cancer patients. PLoS One. 2021;16(8):e0255501. doi:10.1371/journal.pone.0255501
21. World Health Organization. COVID-19 in viet nam situation report 36; 2021. Available from: https://www.who.int/vietnam/internal-publications-detail/covid-19-in-viet-nam-situation-report-36.
22. World Health Organization. COVID-19 weekly epidemiological update; 2021. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update—16-february-2021.
23. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
24. EORTC Quality of Life Group. EORTC QLQ-C30 reference values. Available from: https://www.eortc.org/app/uploads/sites/2/2018/02/reference_values_manual2008.pdf.
25. Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365–376. doi:10.1093/jnci/85.5.365
26. Fayers PM, Bjordal K, Groenvold M, Curran D, Bottomley A; on behalf of the EORTC Quality of Life Group. The EORTC QLQ-C30 Scoring Manual.
27. Cocks K, King MT, Velikova G, Martyn St-James M, Fayers PM, Brown JM. Evidence-based guidelines for determination of sample size and interpretation of the European Organisation for the Research and Treatment of Cancer quality of life questionnaire core 30. J Clin Oncol. 2011;29(1):89–96. doi:10.1200/JCO.2010.28.0107
28. Ghosh J, Ganguly S, Mondal D, Pandey P, Dabkara D, Biswas B. Perspective of oncology patients during COVID-19 pandemic: a prospective observational study from India. JCO Global Oncol. 2020;6:844–851. doi:10.1200/GO.20.00172
29. Gultekin M, Ak S, Ayhan A, et al. Perspectives, fears and expectations of patients with gynaecological cancers during the COVID-19 pandemic: a Pan-European study of the European Network of Gynaecological Cancer Advocacy Groups (ENGAGe). Cancer Med. 2021;10(1):208–219. doi:10.1002/cam4.3605
30. Sigorski D, Sobczuk P, Osmola M, et al. Impact of COVID-19 on anxiety levels among patients with cancer actively treated with systemic therapy. ESMO Open. 2020;5(5):e000970. doi:10.1136/esmoopen-2020-000970
31. Nolte S, Liegl G, Petersen MA, et al. General population normative data for the EORTC QLQ-C30 health-related quality of life questionnaire based on 15,386 persons across 13 European countries, Canada and the United States. Eur J Cancer. 2019;107:153–163. doi:10.1016/j.ejca.2018.11.024
32. World Health Organization. Weekly epidemiological update on COVID-19-30 March 2021; 2021. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19—31-march-2021.
33. Younger E, Smrke A, Lidington E, et al. Health-related quality of life and experiences of sarcoma patients during the COVID-19 pandemic. Cancers. 2020;12(8):2288. doi:10.3390/cancers12082288
34. Falcone R, Grani G, Ramundo V, et al. Cancer care during COVID-19 era: the quality of life of patients with thyroid malignancies. Front Oncol. 2020;10. doi:10.3389/fonc.2020.01128
35. Bargon CA, Batenburg MCT, van Stam LE, et al. Impact of the COVID-19 pandemic on patient-reported outcomes of breast cancer patients and survivors. JNCI Cancer Spectr. 2020;5(1):pkaa104. doi:10.1093/jncics/pkaa104
36. Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. 2020;89:531–542. doi:10.1016/j.bbi.2020.05.048
37. Kimman M, Jan S, Monaghan H, Woodward M. The relationship between economic characteristics and health-related quality of life in newly diagnosed cancer patients in Southeast Asia: results from an observational study. Qual Life Res. 2015;24(4):937–949. doi:10.1007/s11136-014-0828-z
38. Subramaniam S, Kong Y-C, Chinna K, et al. Health-related quality of life and psychological distress among cancer survivors in a middle-income country. Psycho Oncol. 2018;27(9):2172–2179. doi:10.1002/pon.4787
39. Abegaz TM, Ayele AA, Gebresillassie BM. Health related quality of life of cancer patients in Ethiopia. J Oncol. 2018;2018:1467595. doi:10.1155/2018/1467595
40. Moreira DP, Simino GPR, Reis IA, Santos M, Cherchiglia ML. Quality of life of patients with cancer undergoing chemotherapy in hospitals in Belo Horizonte, Minas Gerais State, Brazil: does individual characteristics matter? Cad Saude Publica. 2021;37(8):e00002220. doi:10.1590/0102-311x00002220
41. Hinz A, Mehnert A, Dégi C, Reissmann DR, Schotte D, Schulte T. The relationship between global and specific components of quality of life, assessed with the EORTC QLQ-C30 in a sample of 2019 cancer patients. Eur J Cancer Care. 2017;26(2):e12416. doi:10.1111/ecc.12416
42. Gallo O, Bruno C, Locatello LG, et al. The impact of the COVID-19 pandemic on the quality of life of head and neck cancer survivors. Support Care Cancer. 2021;29(11):6297–6304. doi:10.1007/s00520-021-06198-6
43. Quang BV, Minh LD, Quyen LTL, Mai DNL, Dat NT, Giang KB. Quality of life among newly admitted patients to cancer hospital in Vietnam and associated factors. Health Psychol Open. 2020;7(2):2055102920953049. doi:10.1177/2055102920953049
44. Kokkonen K, Tasmuth T, Lehto JT, et al. Cancer patients’ symptom burden and health-related quality of life (HRQoL) at tertiary cancer center from 2006 to 2013: a cross-sectional study. Anticancer Res. 2019;39(1):271–277. doi:10.21873/anticanres.13107
45. Azmawati MN, Najibah E, Hatta MD, Norfazilah A. Quality of life by stage of cervical cancer among Malaysian patients. Asian Pac J Cancer Prev. 2014;15(13):5283–5286. doi:10.7314/APJCP.2014.15.13.5283
46. Dai Minh L, Quang BV, Ngoc Le Mai D, et al. Health literacy of newly-admitted cancer patients in Vietnam: difficulties understanding treatment options and processing health-related information. Health Serv Insights. 2022;15:11786329211067325. doi:10.1177/11786329211067325
47. Laghousi D, Jafari E, Nikbakht H, Nasiri B, Shamshirgaran M, Aminisani N. Gender differences in health-related quality of life among patients with colorectal cancer. J Gastrointest Oncol. 2019;10(3):453–461. doi:10.21037/jgo.2019.02.04
48. Charalambous A, Kouta C. Cancer related fatigue and quality of life in patients with advanced prostate cancer undergoing chemotherapy. Biomed Res Int. 2016;2016:3989286. doi:10.1155/2016/3989286
49. Muthanna FMS, Karuppannan M, Hassan BAR, Mohammed AH. Impact of fatigue on quality of life among breast cancer patients receiving chemotherapy. Osong Public Health Res Perspect. 2021;12(2):115–125. doi:10.24171/j.phrp.2021.12.2.09
50. Liu L, Fiorentino L, Rissling M, et al. Decreased health-related quality of life in women with breast cancer is associated with poor sleep. Behav Sleep Med. 2013;11(3):189–206. doi:10.1080/15402002.2012.660589
51. Chen ML, Yu CT, Yang CH. Sleep disturbances and quality of life in lung cancer patients undergoing chemotherapy. Lung Cancer. 2008;62(3):391–400. doi:10.1016/j.lungcan.2008.03.016
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.