")
Back to Journals » Clinical Interventions in Aging » Volume 19
Rate-Pressure Product is a Novel Predictor for Short- and Long-Term Mortality in Patients with Acute Coronary Syndrome Undergoing Primary PCI/Immediate Invasive Strategy
Authors Zhou J, Li YJ, Zhou XD, Wang LJ
Received 15 November 2023
Accepted for publication 14 February 2024
Published 23 March 2024 Volume 2024:19 Pages 571—579
DOI https://doi.org/10.2147/CIA.S449905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Jian Zhou,1 Ya-Jie Li,2 Xiao-Dong Zhou,3 Li-Juan Wang1
1Department of Cardiology, The Heart Center, Zhe Jiang Hospital, Hangzhou, 310012, People’s Republic of China; 2Psychiatry Department, Fuyang District Third People’s Hospital, Hangzhou, 311400, People’s Republic of China; 3Department of Cardiology, The Heart Center, The First Affiliated Hospital of Wenzhou Medical University, Zhejiang, 325000, People’s Republic of China
Correspondence: Jian Zhou, Department of Cardiology, Zhe Jiang Hospital, 12 Lingyin Road, Xihu Qu, Hangzhou, 310012, People’s Republic of China, Tel +86-517-8798-7373, Email [email protected]
Background: Rate-pressure product (RPP) calculated by multiplying heart rate by systolic blood pressure, is a convenient indicator closely associated with cardiac work or myocardial oxygen consumption. It has been reported to relate strongly to important indices of cardiovascular risk in patients with myocardial ischemia. However, its relationship with short- and long-term mortality in patients with acute coronary syndrome (ACS) undergoing primary PCI/immediate invasive strategy has not been defined.
Methods: This study analyzed 1301 consecutive ACS patients who had undergone primary PCI, between January 2018 and September 2021. Patients with systolic BP < 90 mmHg were excluded to avoid the confounding effect of cardiogenic shock. RPP values were collected on admission and were divided into four groups: RPP ≤ 7.4, 7.4 ≤ 8.8, 8.8 < 8.8 < RPP8, and RPP > 10.8. Clinical endpoints were in-hospital cardiac and long-term all-cause mortality. The predictive performance was assessed by C-statistic, multivariate analysis and survival analysis.
Results: Multivariate analysis showed that these in the highest vs lowest category of RPP (> 10.8 vs ≤ 7.4) had OR of 4.33 (95% CI=1.10 − 17.01; P = 0.036) in in-hospital cardiac mortality and 3.15 (95% CI=1.24 − 8.00; P = 0.016) in long-term all-cause mortality. In C-statistic analyses, RPP was a strong predictor in ACS, STEMI or UA/NSTEMI group for in-hospital cardiac mortality (AUC = 0.746, 95% CI = 0.722– 0.770, p < 0.001) and long-term all-cause mortality (AUC = 0.701, 95% CI = 0.675– 0.725, p < 0.001). The Kaplan–Meier event rate for long-term survival of RPP > 10.8 was significantly lower than that of RPP ≤ 10.8.
Conclusion: RPP showed a positive association with in-hospital cardiac or long-term all-cause mortality in ACS patients undergoing primary PCI/immediate invasive strategy, and RPP > 10.8 can be as an independent predictor.
Keywords: rate-pressure product, acute coronary syndrome, short-and long-term mortality
Background
Cardiac work transforms mechanical energy provided by glucose oxidation-derived ATP into kinetic and potential energy of the blood thereby allowing provision of oxygen and nutrients to bodily tissues. Said myocardial oxygen consumption-driven cardiac work is mainly determined by mean wall tension, heart rate and ejection interval1–3 with the latter two being closely associated. It is difficult to directly measure myocardial consumption. However, ventricular wall tension is proportional to systolic pressure rendering the product of heart rate and systolic pressure, the rate-pressure product (RPP) calculated by multiplying heart rate by systolic blood pressure, an easily calculated indicator of cardiac work or myocardial oxygen consumption. Increased myocardial oxygen consumption has been proven to play a significant role in the pathogenesis of myocardial ischemia during daily life4,5 and the unmet myocardial oxygen consumption demand in myocardial ischemia is a significant predictor of adverse prognosis and cardiac mortality.6,7 RPP is strongly related with cardiovascular risk in hypertension patients8 and has a close relationship with heart failure patients.9 For coronary artery disease (CAD) patients, RPP is associated with myocardial perfusion imaging findings using gated single photon emission computed tomography imaging with dipyridamole stress and the occurrence of ischemic events has been shown to be related closely to increases in the RPP.8,10 However, the usefulness of RPP in risk stratification for occurrence of short- and long-term mortality, has not been established in ACS patients undergoing primary PCI, which is the subject of the present study.
Methods
Study Population
Total of 1458 consecutive ACS patients were included in this retrospective study cohort between January 2018 and September 2021, and patients were transferred from inpatient wards or admitted from the community to cardiac catheter room to undergo primary PCI/immediate invasive strategy. Exclusion criteria: patients systolic BP < 90 mm Hg (n = 63), obvious arrhythmia (n = 29), diagnostic limitations (n = 54) or incomplete procedures (n = 9). Inclusion criteria: Patients with unstable angina (UA)/non-ST-segment elevation myocardial infarction (NSTEMI) or STEMI (n = 1301) according to American College of Cardiology/American Heart Association guidelines.11 This study has been approved by Medical Ethics Committee of Zhejiang Hospital (Approval No. 2017(5K)). This study was conducted in accordance with the declaration of Helsinki. Due to the retrospective nature of the study, the requirement of patient consent for inclusion was waived from the Ethics Committee of Zhe Jiang Hospital. Patient personal privacy and data confidentiality has been upheld.
Clinical Data and Definitions
The demographic and medical history data were included in this study, such as age, sex, and hypertension. Invasive data were collected from cardiac catheterization laboratory records, such as double/triple-vessel disease, use of thrombus aspiration, corrected TIMI frame count (CTFC). Treatment post PCI data including use of intra-aortic balloon pump (IABP) and vasoactive drugs. Admission laboratory data were collected, including alanine aminotransferase (ALT), MB isoenzyme of creatine kinase (CK-MB), brain natriuretic peptide (BNP), creatinine (Cr), and lactic acid. RPP (heart rate*systolic blood pressure*10−3 mmHg/B/M) values were collected on admission. Patients were divided into four groups in accordance with the cutoff values of ROC for long-term all-cause and in-hospital cardiac mortality: RPP ≤ 7.4, 7.4 ≤ 8.8, 8.8 < RPP ≤ 10.8, and RPP > 10.8. The study primary outcomes were long-term all-cause and in-hospital cardiac mortality. Clinical follow-up of all patients was assessed by phone interviews or direct hospital visits, with mean duration of 23 months.
Statistical Analysis
Continuous variables are presented as mean ± SD and analyzed by Kruskal–Wallis tests. Categorical variables are represented as counts and proportions (%) and analyzed by Pearson chi-square tests. C-statistic defined as the area under the receiver operating characteristic (ROC-AUC) curve was used to assess the predictive value of RPP. The in relation to outcomes. Kaplan–Meier event curves with Log rank test was used for the survival distributions between groups. Cox proportional-hazards regression and logistic regression model were used for univariate and multivariate regression analyses of long-term all-cause and in-hospital cardiac mortality, respectively. Results were shown as odds ratios (ORs) or hazard ratios (HRs) with associated 95% confidence intervals (CIs). A value of p < 0.05 was defined for statistical significance, and all tests were two-sided. SPSS version 21.0 (SPSS Inc., Chicago, IL, USA) and MedCalc version 12.0 (MedCalc Software, Mariakerke, Belgium) were used for statistical analysis.
Results
Clinical Data of All Patients
Total of 1301 ACS patients were divided into four groups: RPP ≤ 7.4 (n = 331), 7.4 ≤ 8.8 (n = 344), 8.8 < RPP ≤ 10.8 (n = 345), and RPP > 10.8 (n = 281). Baseline characteristics and in-hospital outcomes were detailed in Table 1. As compared with patients with RPP ≤ 10.8, those with RPP > 10.8 were at higher risk with: greater proportion of hypertension, diabetes mellitus, high Killip classification, ST-segment elevation myocardial infarction and low left ventricular ejection fraction, and more frequent use of vasoactive drugs and intra-aortic balloon pump. In addition, in laboratory test, patients with RPP>10.8 had higher levels of MB isoenzyme of creatine kinase, alanine aminotransferase, creatinine, brain natriuretic peptide, and lactic acid as compared with patients with RPP≤10.8.
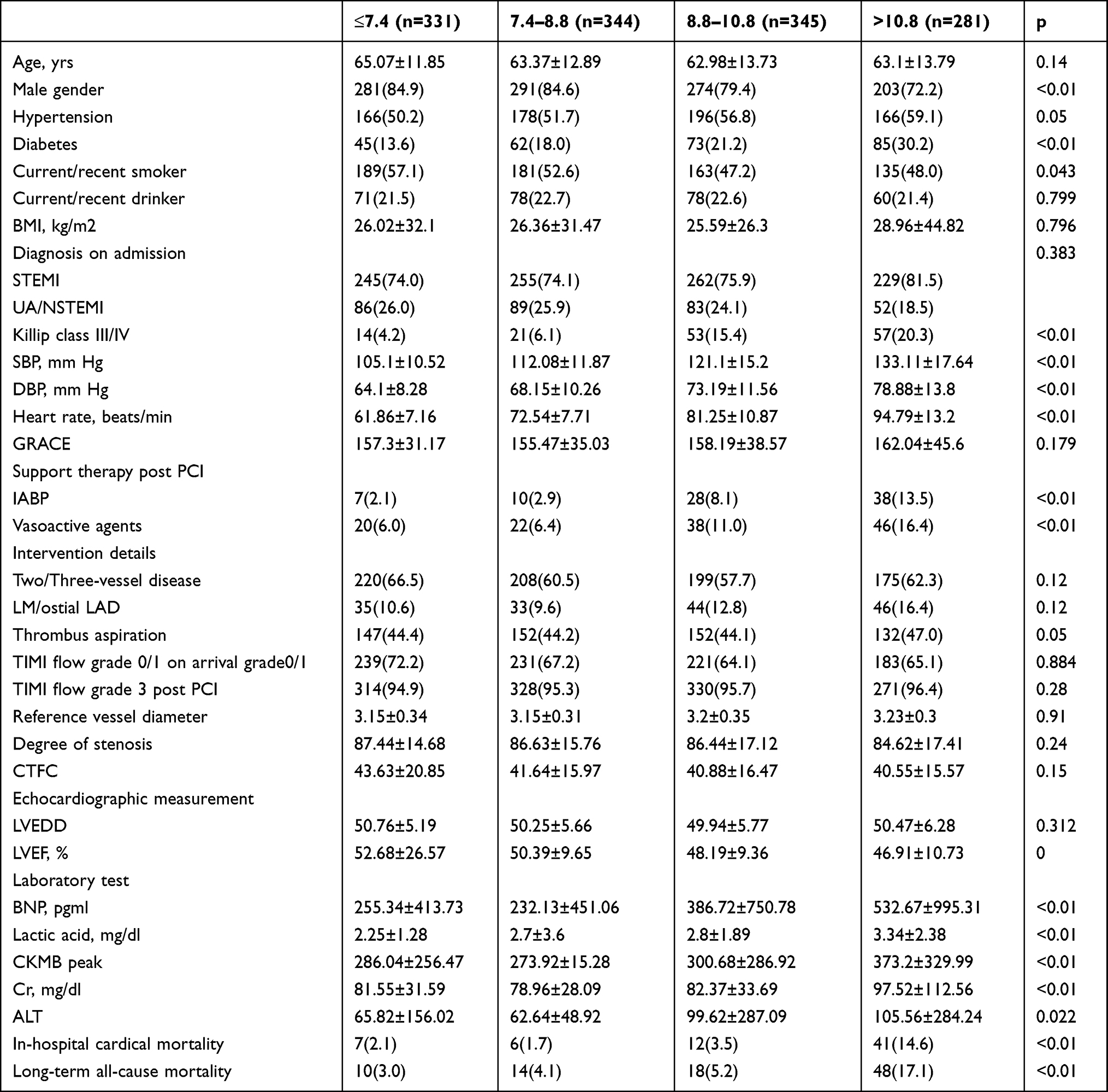 |
Table 1 Baseline Characteristics of the Study Population, N (%), or means±SD |
Risk of Primary Outcomes
Prediction of in-Hospital Cardiac Mortality
The in-hospital cardiac mortality of 1301 patients was 5.1% (66 patients; Table 1). Some variables showed significant effects on in-hospital cardiac mortality after univariate analysis: Killip class III/IV, age, gender, two-vessel or three-vessel disease, left main or anterior descending branch opening, vasoactive drugs, intra-aortic balloon pump, lactic acid, TIMI flow grade 3 post PCI, ALT, Cr, CKMB peak, and BNP levels. In multivariable analysis, the following independent risk factors were revealed: age (OR: 1.07, 95% CI: 1.02–1.11, P = 0.002), Killip class III/IV (OR: 6.91, 95% CI: 2.54–18.84, P < 0.001), left main or anterior descending branch opening (OR: 2.88, 95% CI: 1.16–7.18, P = 0.023), levels of lactic acid (OR: 1.41, 95% CI: 1.28–1.55, P = 0.027), vasoactiveagents (OR: 2.91, 95% CI: 1.07–7.90, P = 0.023) and RPP > 10.8 (OR: 4.33, 95% CI: 1.10–17.01, P = 0.036) (Table 2). The ROC-AUC of RPP for predicting in-hospital cardiac mortality was 0.746 (95% CI = 0.722–0.770, p < 0.001) with cutoff value of 10.7 (sensitivity = 0.649 and specificity = 0.792) (Figure 1A). In consideration of the population study is a mixture of differing types of ACS, we divided the population into STEMI group (991 patients; 76.2%) and UA/NSTEMI group (310 patients; 23.8%) (Table 1). The ROC-AUC of RPP for predicting in-hospital cardiac mortality in STEMI group was 0.763 (95% CI = 0.735–0.789, p < 0.001) with cutoff value of 10.7 (sensitivity = 0.705 and specificity = 0.777) (Figure 1B). The ROC-AUC of RPP for predicting in-hospital cardiac mortality in UA/NSTEMI group was 0.691 (95% CI = 0.636–0.743, p < 0.001) with cutoff value of 11.6 (sensitivity = 0.462 and specificity = 0.914) (Figure 1C).
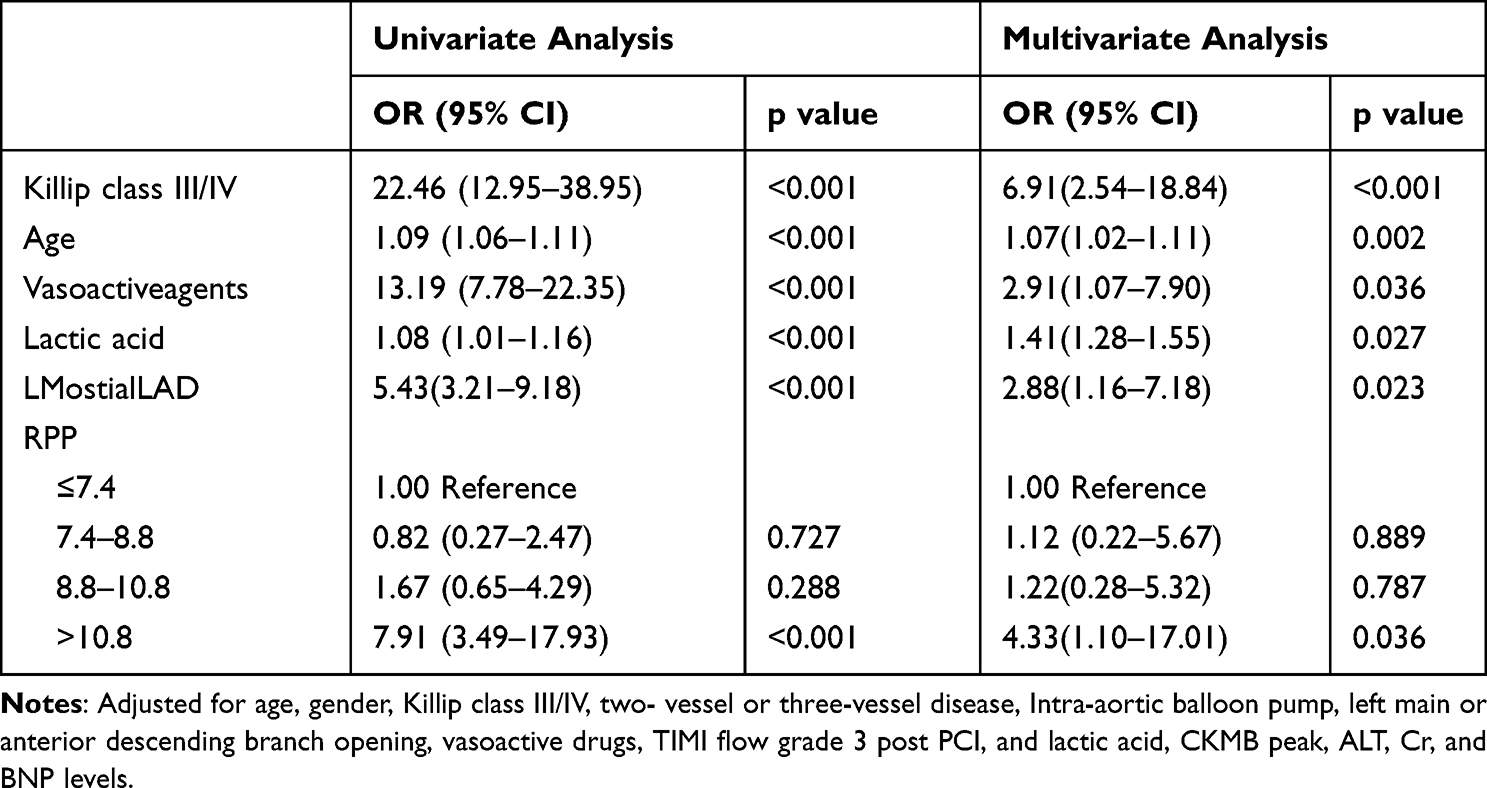 |
Table 2 Effects of Multiple Variables on in-Hospital the Cardiac Mortality in Univariate and Multivariate Analyses |
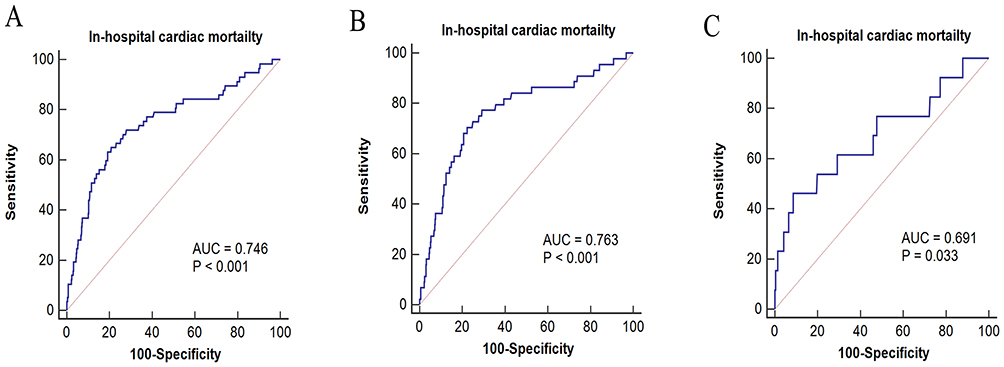 |
Figure 1 ROC-AUC of RPP for in-hospital cardiac mortality in ACS (A), STEMI (B) and UA/NSTEMI group (C). |
Prediction of Long-Term All-Cause Mortality
The long-term all-cause mortality of 1301 patients was 6.92% (90 patients; Table 1). Some variables showed significant effects on long-term all-cause mortality after univariate analysis: Killip class III/IV, age, gender, two-vessel or three-vessel disease, left main or anterior descending branch opening, vasoactive drugs, Intra-aortic balloon pump, lactic acid, TIMI flow grade 3 post PCI, ALT, Cr, CKMB peak, and BNP levels. In multivariable analysis, the following independent risk factors were revealed: age (OR: 1.07, 95% CI: 1.04–1.10, P < 0.001), Killip class III/IV (OR: 4.31, 95% CI: 2.15–8.64, P < 0.001), levels of lactic acid (OR: 1.08, 95% CI: 1.03–1.13, P = 0.001), intra-aortic balloon pump (OR: 2.62, 95% CI: 1.25–5.48, P = 0.011) and RPP > 10.8 (OR: 3.15, 95% CI: 1.24–8.00, P = 0.016) (Table 3). The ROC-AUC of RPP for predicting long-term all-cause mortality was 0.701 (95% CI = 0.675–0.725, p < 0.001) with cutoff value of 10.85 (sensitivity = 0.53 and specificity = 0.81) (Figure 2A). The Kaplan–Meier event rate for long-term survival of RPP > 10.8 was significantly lower than that of RPP ≤ 10.8 (p < 0.01) (Figure 3A). The population was divided into STEMI group (991 patients; 76.2%) and UA/NSTEMI group (310 patients; 23.8%) (Table 1). The ROC-AUC of RPP in STEMI group for predicting long-term all-cause mortality was 0.695 (95% CI = 0.665–0.723, p < 0.001) with cutoff value of 10.9 (sensitivity = 0.578 and specificity = 0.795) (Figure 2B). The Kaplan–Meier event rate for long-term survival of RPP > 10.8 was significantly lower than that of RPP ≤ 10.8 (p < 0.01) (Figure 3B). The ROC-AUC of RPP in UA/NSTEMI group for predicting long-term all-cause mortality was 0.725 (95% CI = 0.672–0.774, p < 0.001) with cutoff value of 10.3 (sensitivity = 0.539 and specificity = 0.806) (Figure 2C). The Kaplan–Meier event rate for long-term survival of RPP > 10.8 was significantly lower than that of RPP ≤ 10.8 (p < 0.01) (Figure 3C).
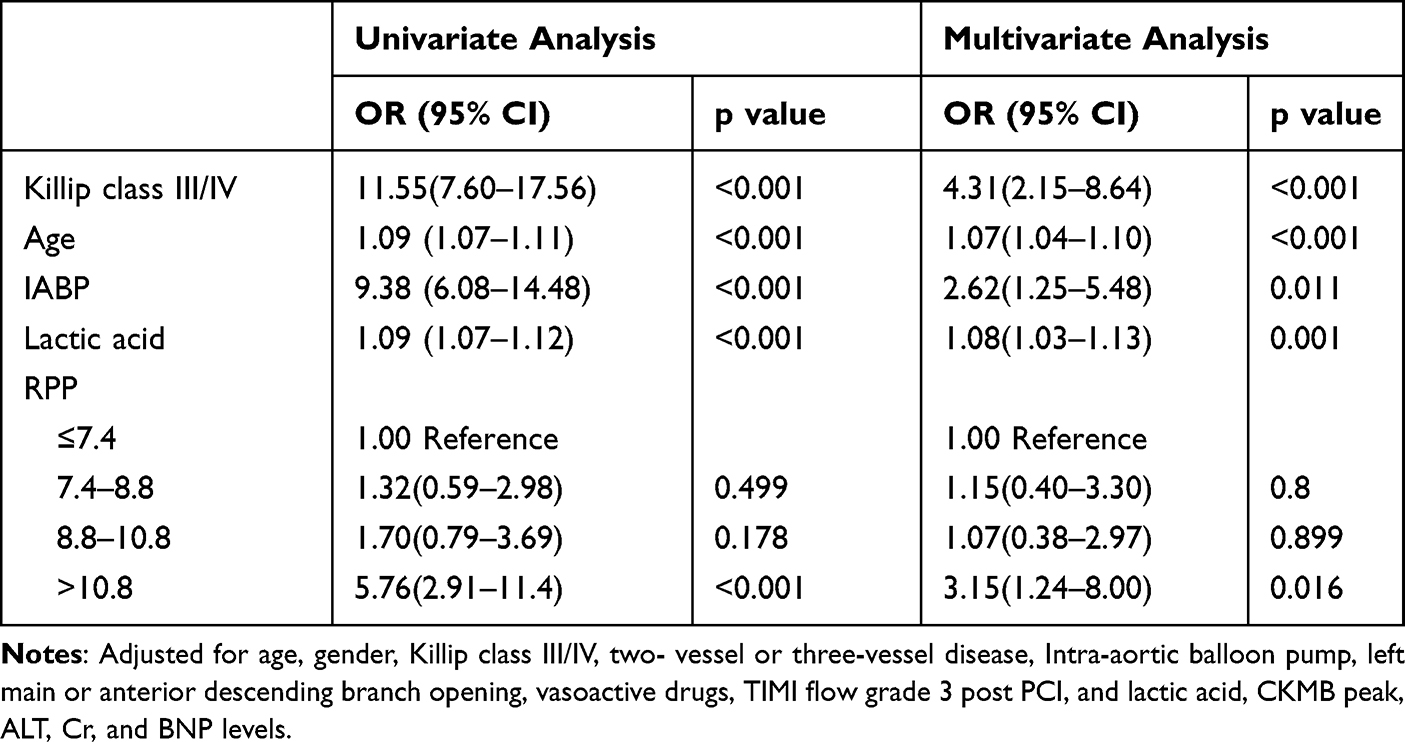 |
Table 3 Effects of Multiple Variables on Long-Term Mortality in Univariate and Multivariate Analyses |
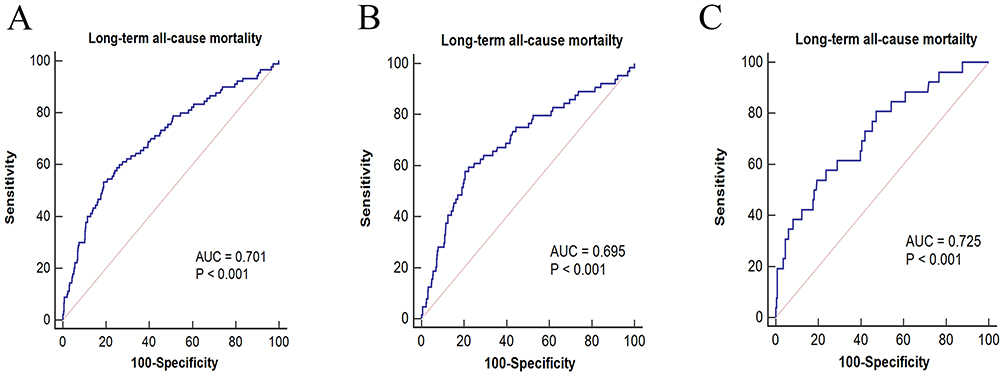 |
Figure 2 ROC-AUC of RPP for long-term all-cause mortality in ACS (A), STEMI (B) and UA/NSTEMI group (C). |
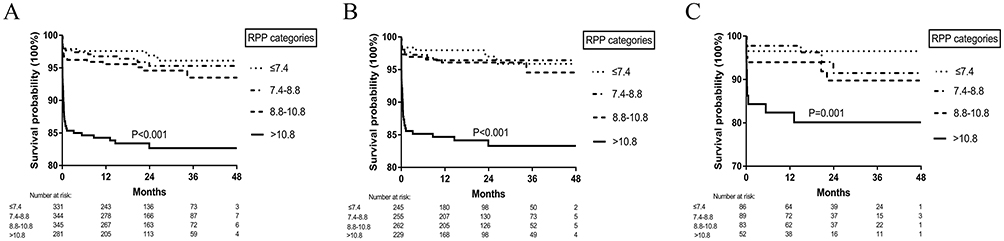 |
Figure 3 Kaplan–Meier plot of long-term survival probability of in ACS (A), STEMI (B) and UA/NSTEMI group (C). |
Discussion
For ACS patients undergoing primary PCI/immediate invasive strategy, the relationship between RPP, and in-hospital cardiac or long-term all-cause mortality followed a positive association. Patients with RPP > 10.8 had higher mortality than those of RPP ≤ 10.8. After multivariable analysis, RPP > 10.8 was an independent positive predictor of in-hospital cardiac or long-term all-cause mortality.
Heart rate has been associated with prognosis in ACS patients. In the study by Sripal Bangalore and Franz H. Messerli of ACS patients, a fast heart rate portended an increased risk of cardiovascular events including in-hospital all-cause mortality and stroke.12 Higher resting heart rate has been associated with worse short-and long-term outcomes in ACS patients.13 And pharmacologic interventions that slow down heart rate, such as β-blockers, reduce mortality and improve outcomes.14 Previous studies showed that increased systolic blood pressure is the dominant risk factor for stroke, coronary heart disease, and heart failure.15–17 Jun Shiraishi has showed that the relationship between admission systolic blood pressure and in-hospital mortality followed a J-shaped curve (higher event rates at low and high systolic blood pressure) in acute myocardial infarction patients undergoing primary percutaneous coronary intervention.18 Heart rate and blood pressure increase significantly in most patients with myocardial ischemia, and increased myocardial oxygen consumption plays a significant role in the pathogenesis of myocardial ischemia during daily life.4,5 In multivariate analysis controlling for age, sex, and clinical descriptions of angina, the presence of ischemia on ambulatory monitoring was a significant predictor of adverse prognosis and cardiac mortality during daily life with coronary heart disease patients.6 The RPP, defined as heart rate multiplied by blood pressure, is a convenient and simple reference index to indirectly reflect cardiac work load and myocardial oxygen consumption and it relates strongly to important indices for cardiovascular morbidity and mortality in patients with myocardial ischemia. In the study by Karaye KM,9 there was a close relationship between RPP and heart failure with indices for LV wall tension including interventricular septal thickness, LV end-diastolic dimension and N-terminal B-type natriuretic peptide level. Development of heart failure leads to hemodynamics disturbance and excessive sympathetic activity. The nerve endings and adrenal medulla release a large amount of adrenaline and norepinephrine into the blood to maintain cardiac output by accelerating heart rate and enhancing myocardial contraction, which in turn promotes cardiac remodeling and aggravates heart failure generating a vicious circle.19 As many of you known, the RPP is an index of myocardial metabolism that correlates closely with myocardial hemodynamics. The fractional flow reserve (FFR) and instantaneous wave-free ratio (iFR) correlate well and are similar coronary functional indexes, although they differ in some respects. The study20 has found that RPP is closely related to FFR and instantaneous iFR, and even affects the ability of iFR to evaluate the degree of ischemia. Although the study21 has found that the recovery of RPP after exercise is a potent predictor of cardiac death in patients with coronary artery disease (CAD) and type 2 diabetes (T2D), the association of RPR and short- and long-term all-cause mortality has however not been well described in ACS patients. Our results found a positive association between RPP and in-hospital cardiac or long-term all-cause mortality. RPP is an independent predictor of long-term prognosis in patients with CAD who underwent PCI.22 A low RPP reactivity was associated with increased risk of cardiovascular death or nonfatal myocardial infarction in patients with stable CAD.23 Patients with RPP > 10.8 had higher mortality than those of RPP ≤ 10.8, indicating that higher heart rate and blood pressure or more cardiac work was needed to provide effective blood supply for basic metabolism.
HALP (hemoglobin, albumin, lymphocyte, and platelet) may be a significant independent predictor of in-hospital mortality in patients with STEMI treated with primary PCI.24 The white blood cell count to mean platelet volume ratio is associated with syntax score in patients with STEMI.25 In the study by Alan Hinderliter,4 patients with myocardial ischemia during daily activities tended to develop electrocardiographic changes at a lower exercise heart rate and RPP than those without ischemia. In patients with myocardial ischemia, the systolic pressure increased slowly during exercise because of impaired left ventricular function, while it increased significantly in healthy people. Compared with healthy people, patients with myocardial ischemia often show higher RPP at rest and lower RPP during exercise. In this process, heart rate and blood pressure play important roles as bridges. Patients in the high RPP group belong to the high myocardial oxygen consumption group. For this group, in addition to opening criminal blood vessels as soon as possible to reduce further myocardial damage, risk factors (such as hypertension) should be controlled as soon as possible, and β-blocker drugs should be added as soon as possible to control heart rate and reduce myocardial oxygen consumption in a standardized way. And long-term standardized follow-up to adjust medications in real time to address the changes that occur. This is the first study to our knowledge to document a close relationship between RPP and in-hospital cardiac or long-term all-cause mortality.
Limitations
There are several limitations. Firstly, as a retrospective and observational study at a single center, full adjustment for potential confounders and selection bias were precluded, so multicenter studies with less restrictive inclusion/exclusion criteria, larger sample sizes, and various assessment timings are needed to validate and extend the results of this study. Secondly, heart rate and blood pressure values should be estimated by ambulatory monitoring, because they were affected by the many adjustments to the potential and ongoing medical conditions of patients before admission. Thirdly, besides long-term all-cause mortality, more long-term outcomes also should include heart failure, stroke, post-discharge re-infarction, and cardiac arrest to increase their clinical relevance.
Conclusions
In this study, the relationship between RPP, and in-hospital cardiac or long-term all-cause mortality followed a positive association with increased event rates at high groups in ACS patients undergoing primary PCI. After multivariable analysis and survival analysis, RPP > 10.8 can be as an independent predictor for in-hospital cardiac and long-term all-cause mortality.
Abbreviations
PCI, percutaneous coronary intervention; RPP, rate pressure product; ACS, acute coronary syndrome; STEMI, ST-segment elevation myocardial infarction; UA/NSTEMI, unstable angina/non-ST-segment elevation myocardial infarction; ROC-AUC, the area under the receiver operating characteristic curve; ATP, adenosine triphosphate; CAD, coronary artery disease; CTFC, corrected TIMI frame count; IABP, intra-aortic balloon pump; Cr, creatinine; ALT, alanine aminotransferase; BNP, brain natriuretic peptide; CKMB, MB isoenzyme of creatine kinase; TIMI, thrombolysis in myocardial infarction; SPSS, statistical product and service solutions; Ors, ratios; HRs, hazard ratios; CIs, confidence intervals; iFR, instantaneous wave-free ratio; FFR, fractional flow reserve; T2D, type 2 diabetes.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Nagpal S, Walia L, Lata H, Sood N, Ahuja GK. Effect of exercise on rate pressure product in premenopausal and postmenopausal women with coronary artery disease. Indian J Physiol Pharmacol. 2007;51(3):279–283.
2. Arya A, Maleki M, Noohi F, Kassaian E, Roshanali F. Myocardial oxygen consumption index in patients with coronary artery disease. Asian Cardiovasc Thorac Ann. 2005;13(1):34–37. doi:10.1177/021849230501300108
3. Kronenberg MW, Cohen GI, Leonen MF, Mladsi TA, Di Carli MF. Myocardial oxidative metabolic supply-demand relationships in patients with nonischemic dilated cardiomyopathy. J Nucl Cardiol. 2006;13(4):544–553. doi:10.1016/j.nuclcard.2006.04.002
4. Hinderliter A, Miller P, Bragdon E, Ballenger M, Sheps D. Myocardial ischemia during daily activities: the importance of increased myocardial oxygen demand. J Am Coll Cardiol. 1991;18(2):405–412. doi:10.1016/0735-1097(91)90593-X
5. Deedwania PC, Carbajal EV. Role of myocardial oxygen demand in the pathogenesis of silent ischemia during daily life. Am J Cardiol. 1992;70(16):19F–24F. doi:10.1016/0002-9149(92)90185-2
6. Rocco MB, Nabel EG, Campbell S, et al. Prognostic importance of myocardial ischemia detected by ambulatory monitoring in patients with stable coronary artery disease. Circulation. 1988;78(4):877–884. doi:10.1161/01.CIR.78.4.877
7. Deedwania PC, Carbajal EV. Silent ischemia during daily life is an independent predictor of mortality in stable angina. Circulation. 1990;81(3):748–756. doi:10.1161/01.CIR.81.3.748
8. White WB. Heart rate and the rate-pressure product as determinants of cardiovascular risk in patients with hypertension. Am J Hypertens. 1999;12(2 Pt 2):50S–5S. doi:10.1016/S0895-7061(98)00280-5
9. Karaye KM, Akintunde AA. The significance of rate pressure product in heart failure patients. Int Cardiovascular Forum J. 2013;1(1):
10. Ansari M, Javadi H, Pourbehi M, et al. The association of rate pressure product (RPP) and myocardial perfusion imaging (MPI) findings: a preliminary study. Perfusion. 2012;27(3):207–213. doi:10.1177/0267659112436631
11. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients with Unstable Angina). J Am Coll Cardiol. 2000;36:970–1062. doi:10.1016/s0735-1097(00)00889-5
12. Bangalore S, Messerli FH, Ou F-S, et al. The association of admission heart rate and in-hospital cardiovascular events in patients with non-ST-segment elevation acute coronary syndromes: results from 135 164 patients in the CRUSADE quality improvement initiative. Eur Heart J. 2010;31(5):552–560. doi:10.1093/eurheartj/ehp397
13. Saraiva F, Antonio N, Lourenco C, et al. Heart rate and prognosis in acute coronary syndromes. Rev Port Cardiol. 2010;29(7–8):1101–1119.
14. Yusuf S, Peto R, Lewis J, Collins R, Sleight P. Beta blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis. 1985;27(5):335–371. doi:10.1016/S0033-0620(85)80003-7
15. Stamler J, Stamler R, Neaton JD. Blood pressure, systolic and diastolic, and cardiovascular risks. US population data. Arch Intern Med. 1993;153(5):598–615. doi:10.1001/archinte.1993.00410050036006
16. Psaty BM, Furberg CD, Kuller LH, et al. Association between blood pressure level and the risk of myocardial infarction, stroke, and total mortality: the cardiovascular health study. Arch Intern Med. 2001;161(9):1183–1192. doi:10.1001/archinte.161.9.1183
17. Haider AW, Larson MG, Franklin SS, Levy D, Framingham Heart S. Systolic blood pressure, diastolic blood pressure, and pulse pressure as predictors of risk for congestive heart failure in the Framingham Heart Study. Ann Internal Med. 2003;138(1):10–16. doi:10.7326/0003-4819-138-1-200301070-00006
18. Shiraishi J, Kohno Y, Sawada T, et al. Prognostic impact of systolic blood pressure at admission on in-hospital outcome after primary percutaneous coronary intervention for acute myocardial infarction. J Cardiol. 2012;60(2):139–144. doi:10.1016/j.jjcc.2012.02.008
19. Napoli C, Casamassimi A, Crudele V, Infante T, Abbondanza C. Kidney and heart interactions during cardiorenal syndrome: a molecular and clinical pathogenic framework. Future Cardiol. 2011;7(4):485–497. doi:10.2217/fca.11.24
20. Ebihara S, Otsuki H, Arashi H, Yamaguchi J, Hagiwara N. Rate pressure products affect the relationship between the fractional flow reserve and instantaneous wave-free ratio. J Interv Cardiology. 2020;10:1–8.
21. Kiviniemi AM, Kenttä TV, Lepojärvi S, et al. Recovery of rate-pressure product and cardiac mortality in coronary artery disease patients with type 2 diabetes. Diabetes Res Clin Pract. 2019;150:150–157. doi:10.1016/j.diabres.2019.03.007
22. Jiang ZH, Aierken A, Wu TT, Zheng YY, Ma YT, Xie X. Rate pressure product as a novel predictor of long-term adverse outcomes in patients after percutaneous coronary intervention: a retrospective cohort study. BMJ Open. 2023;13(4):e067951. doi:10.1136/bmjopen-2022-067951
23. Moazzami K, Cheung B, Sullivan S, et al. Hemodynamic reactivity to mental stress in patients with coronary artery disease. JAMA Network Open. 2023;6(10):e2338060. doi:10.1001/jamanetworkopen.2023.38060
24. Karakayali M, Omar T, Artac I, et al. The prognostic value of HALP score in predicting in-hospital mortality in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Coronary Artery Disease. 2023;34(7):483–488. doi:10.1097/MCA.0000000000001271
25. Karakayali M, Timor OMAR, Artac I, et al. The white blood cell count to Mean Platelet Volume Ratio (WMR) is associated with syntax score in patients with ST-segment elevation myocardial infarction. Kafkas J Med Sci. 2023;13(2):173–178. doi:10.5505/kjms.2023.98512
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.