")
Back to Journals » Clinical Ophthalmology » Volume 18
Real-World Evidence of the Long-Term Effectiveness of 0.2 μg/Day Fluocinolone Acetonide Implant in Persistent and Recurrent Diabetic Macular Edema – A Single Center Study
Authors Soares RM , Ferreira CC , Fernandes JDS, Madeira C, Silva LMA, Saraiva E, Ribeiro L, Fonseca S
Received 10 December 2023
Accepted for publication 15 February 2024
Published 16 April 2024 Volume 2024:18 Pages 1057—1066
DOI https://doi.org/10.2147/OPTH.S382920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ricardo Machado Soares,* Catarina Cunha Ferreira,* Joana da Silva Fernandes, Carolina Madeira, Luís MA Silva, Eduardo Saraiva, Lígia Ribeiro, Sofia Fonseca
Department of Ophthalmology - Centro Hospitalar Vila Nova de Gaia e Espinho, Porto, Portugal
*These authors contributed equally to this work
Correspondence: Ricardo Machado Soares, Department of Ophthalmology, Centro Hospitalar Vila Nova de Gaia e Espinho, EPE, Rua Conceição Fernandes, S/N, 4434-502, Vila Nova de Gaia, Porto, Portugal, Tel +351 915045174, Email [email protected]
Purpose: To report the long-term functional, anatomical and safety outcomes of 0.2 μg/day fluocinolone acetonide 0.19mg in patients with persistent or recurrent diabetic macular edema (DME).
Methods: Retrospective, observational, single-center study of patients with recurrent or persistent DME. All patients received 0.2 μg/day of fluocinolone acetonide 0.19mg, and data were collected at baseline and months 1, 3, 6, 12, 24 and 36 after implantation. Outcomes measured included best-corrected visual acuity (BCVA), central macular thickness (CMT), intraocular pressure (IOP), and safety outcomes.
Results: A total of 28 eyes from 28 patients were included. The mean age was 66.5 years (95% CI 62.8– 70.2) with a mean duration of DME of 8.8 years (95% CI 7.7– 10.0). Only two eyes were phakic. Mean follow-up was 25.4 months (95% CI 21.2– 29.6). Mean BCVA at baseline was 48.6 ETDRS letters (95% CI 41.3– 55.8) and improved as early as month 1 of follow-up with a mean gain in BCVA of 7.8 (95% CI 4.3– 11.3) ETDRS letters (p< 0.001). Statistically significant improvements in BCVA were also observed at months 6, 12 and 24. At baseline, patients had a mean CMT of 530.5μm (95% CI 463.0– 598.0), and a decrease in CMT was observed, starting at the first month of follow-up (mean CMT reduction of − 170.5μm, 95% CI − 223.8– − 117.1; p< 0.001). Statistically significant decreases in CMT were also observed at months 6, 12, 24, and 36, with the maximum decrease observed at month 12 (p< 0.001). Mean IOP at baseline was 16.4mmHg (95% CI 15.3– 17.5) and nine eyes (32.1%) had an IOP ≥ 21mmHg during follow-up.
Conclusion: Our results support the effectiveness and safety profile of fluocinolone acetonide. Although additional long-term real-world evidence is required, fluocinolone acetonide may represent a safe strategy for daily, low-dose, sustained and localized release to the posterior segment of the eye, providing both functional and anatomical benefits in DME.
Keywords: diabetic macular edema, intravitreal implant, best corrected visual acuity, intravitreal corticosteroid, sub-optimal response
Introduction
Diabetic macular edema (DME) is a major cause of vision impairment in patients with diabetic retinopathy (DR).1 The current standard of care for DME treatment includes short-acting intravitreal injections of anti-vascular endothelial growth factors (VEGF), such as bevacizumab (off-label use), ranibizumab, aflibercept and brolucizumab, which might be combined with laser photocoagulation.2,3 In cases of persistent or recurrent DME, the administration of intravitreal corticosteroids, such as dexamethasone and triamcinolone acetonide, has been regarded as an important second-line therapy,4 or first-line in patients who are not suitable for intravitreal anti-VEGF treatment.5 One of the key benefits of intravitreal corticosteroids is addressing the multiple cytokines and inflammation pathways underlying DME,6–10 reducing vascular permeability and suppressing angiogenesis while avoiding systemic adverse events.11,12 Nonetheless, these added benefits may be offset by an increased intraocular pressure (IOP) and acceleration of cataract formation.8
Fluocinolone acetonide 0.19mg (FAc; ILUVIEN®) is a non-biodegradable polyamide drug delivery system micro-implant that continuously releases 0.2µg of FAc per day over a period of 3 years. Currently, the FAc implant is approved for the treatment of chronic DME insufficiently responsive to other therapies and prevention of relapse in recurrent non-infectious posterior uveitis.13–15 The FAME studies were the first to report the efficacy and safety of the 0.2 μg/day FAc implant in DME, followed by other clinical trials and real-world studies confirming similar benefits.7,16–20 Notwithstanding the available literature, there is still a significant knowledge gap concerning the implant’s long-term effects on DME. In the present study, we report the long-term functional, anatomical and safety outcomes of the 0.2 μg/day FAc implant in patients with persistent or recurrent DME.
Methods
Study Design
Retrospective, observational, single-center study conducted at the Department of Ophthalmology of Centro Hospitalar Vila Nova de Gaia e Espinho, Portugal. Patients with recurrent or persistent DME (ICD11 – Diabetic macular oedema – 9B71.02) treated with a single 0.2 μg/day FAc intravitreal implant between January 2016 and December 2021 were included. This study was conducted following the ethical standards of the institutional and national research committee and the latest amendment of the Helsinki Declaration for biomedical research.
Study Criteria and Ophthalmologic Evaluation
Patients included in the study had persistent or recurrent DME, and they were treated with a single 0.2 μg/day FAc intravitreal implant. Prior to FAc implant, all patients were initially treated with a loading dose of anti-VEGF intravitreal injections and, after that, according to a treat-and-extend protocol or intravitreal steroid injection in a pro-renata regimen. Regarding the no-therapy time frame, every patient waited at least 4 weeks since the last intravitreal treatment. Persistent DME was defined as eyes having a central macular thickness (CMT) >300μm and decrease in CMT ≤10% after 6 months of follow-up, despite receiving a minimum of 4 out of the potential 6 protocol-mandated intravitreal anti-VEGF treatments during this period. Additionally, to be included in the study, at least one year of follow-up after the injection of the FAc implant was required. Patients with concomitant ocular disease that could cause macular edema or decrease in visual acuity, including history of vitreoretinal disease, age-related macular degeneration, retinal vein occlusion, uveitis, history of intraocular surgery or laser photocoagulation in the previous 3 months, and media opacities that compromised the quality of spectral-domain optical coherence tomography (SD-OCT, Spectralis, Heidelberg Engineering, Heidelberg, Germany) scan images were excluded.
Baseline demographics and previous treatments to Fac implant (i.e: intravitreal anti-VEGF and corticosteroids, focal/macular grid laser photocoagulation, panretinal laser photocoagulation and vitrectomy/cataract phacoemulsification) were collected.
Patients were evaluated at the baseline visit (which corresponded to the visit prior to FAc implant injection) and at months 1, 6, 12, 24 and 36 after Fac implantation. In each visit, patients underwent a comprehensive ophthalmologic examination including (1) best-corrected visual acuity (BCVA) using ETDRS letter chart, (2) slit-lamp anterior segment and dilated fundus biomicroscopy evaluation (3) IOP measurement and (4) SD-OCT . The evolution of CMT was recorded from the retinal thickness ETDRS grid (center 1-mm), evaluated through SD-OCT.
In cases where the anatomical outcomes subsequent to the follow-up of FAc implantation were not attained, the discretionary adjudication of employing rescue intravitreal injections and/or implementing macular laser photocoagulation was relegated to the purview of the attending clinician, guided by the informed choices made by the patient. Use of IOP-lowering drugs, need for surgery (eg: cataract phacoemulsification, glaucoma surgery) and additional adjuvant therapy after Fac implant were recorded.
Assessments and Outcomes
Outcomes measured included BCVA, CMT, and IOP in the time points established at months 1, 6, 12, 24, 36 and last observation (last month of follow-up). All outcome variables were compared to the baseline at these time points. BCVA improvement was considered when visual acuity changed ≥5 letters from baseline. Stabilized/improved vision was considered when visual gains or losses were within 4 letters.21,22 Visual outcomes were reported by percentage of patients achieving improvement of ≥5, 10 or 15 ETDRS letters, and percentage of patients with vision stability. Differences in CMT reduction and IOP were evaluated in the primary time points. The percentage of patients with CMT ≤315µm and reduction of CMT >20% at last observation, and the percentage of eyes that had IOP ≥21mmHg at any given point during follow-up were reported.
Statistical Analysis
For descriptive purposes of the study sample, counts and proportions are presented. The Shapiro–Wilk test was performed to evaluate the normality of the distributions. Symmetrical variables are described using means and 95% confidence intervals (CI). The Wilcoxon test was used to compare quantitative variables between the baseline and each follow-up time point. Statistical analysis was conducted using SPSS statistical software (IBM SPSS statistics package version 28, Armonk, NY, USA), and significance was set at α=0.05.
Results
Baseline Characteristics and Follow-Up
A total of 28 eyes from 28 patients treated with 0.2 μg/day FAc implant were included. Baseline characteristics are presented in Table 1. Patients had a mean age of 66.5 years (95% CI 62.8–70.2) and a mean duration of DME of 8.8 years (95% CI 7.7–10.0). Only two eyes (7.1%, N=2 patients) were phakic. All patients had previously undergone anti-VEGF injections (mean of 9.0; 95% CI 6.3–11.8), intravitreal corticosteroid injections (mean of 4.3; 95% CI 3.5–5.2) and panretinal photocoagulation. Additionally, 21 eyes (75%) had undergone focal/grid laser photocoagulation, eight eyes (28.6%) had undergone prior vitrectomy and eight patients (28.6%) were receiving IOP-lowering medication due to glaucoma diagnosis.
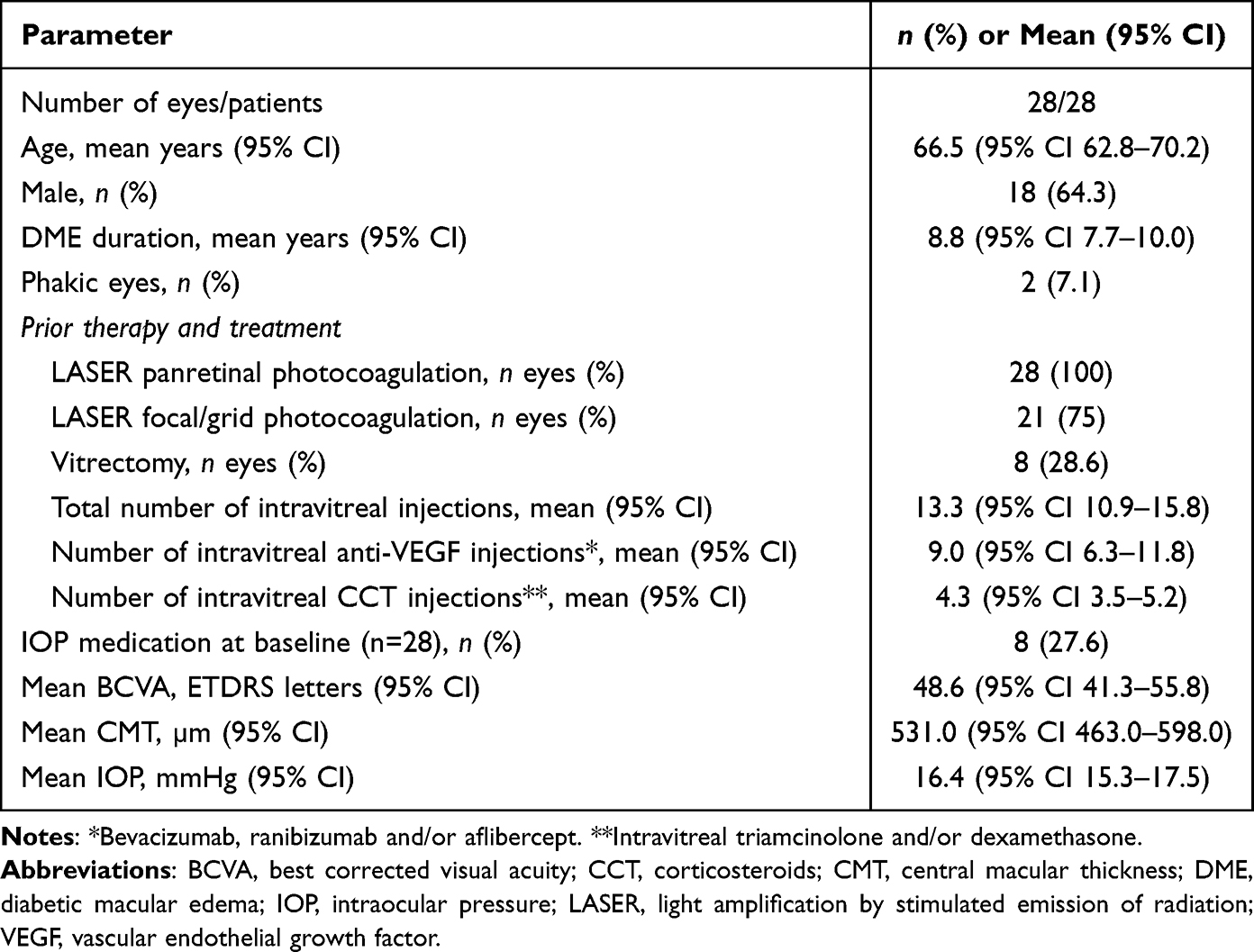 |
Table 1 Demographic and Clinical Characteristics of the Study Population at the Time of FAc Implant |
Mean follow-up duration was 25.4 months (95% CI 21.2–29.6). From the initial cohort, 100% completed the 12-month follow-up, 19 patients (67.9%) had a follow-up of at least 24 months, and 13 patients (46.4%) had a complete follow-up of 36 months. Four patients were lost to follow-up (two deaths and two missed appointments). Table 2 summarizes the follow-up and management of the overall study population. During follow-up, both phakic patients underwent cataract surgery (12 and 15 months after FAc implant) and two eyes (7.1%) received additional panretinal photocoagulation. Five patients (17.9%) received rescue therapy, including intravitreal injections of anti-VEGF (4 eyes, 14.3%) and corticosteroid (2 eyes, 7.1%).
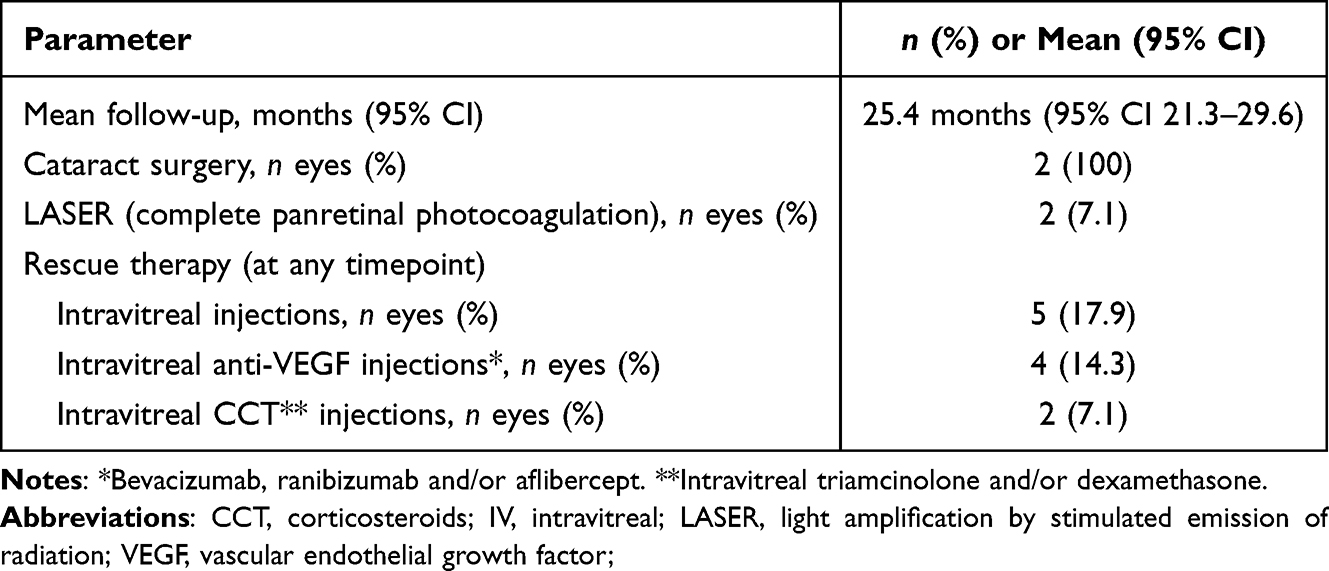 |
Table 2 Follow-Up and Management of Diabetic Macular Edema (DME) Patients from Baseline to Last Observation |
Visual Acuity
The main visual acuity outcomes are presented in Figure 1. Absolute values of BCVA, CMT and IOP are reported in Table 3. The mean BCVA at baseline was 48.6 ETDRS letters (95% CI 41.3–55.8). Improvement in BCVA was observed early at month 1 of follow-up, with a mean change in BCVA of 7.8 (95% CI 4.3–11.3) ETDRS letters (p<0.001) compared to baseline. Statistically significant differences in BCVA were also reported at different time points of follow-up compared to baseline, including months 6 (mean 9.1, 95% CI 4.4–13.8 ETDRS letters; p=0.001), 12 (mean 8.7, 95% CI 4.1–13.4 ETDRS letters; p=0.003), and 24 (mean 7.7, 95% CI 1.7–13.8 ETDRS letters; p=0.014) (Figure 1A). At 36 months of follow-up, there was a trend for BCVA improvement (mean 6.6, 95% CI −0.9–14.0 ETDRS letters) when compared to baseline, although this difference was not statistically significant (p=0.107).
 |
Table 3 Absolute Values of BCVA, CMT and IOP at Selected Timepoints |
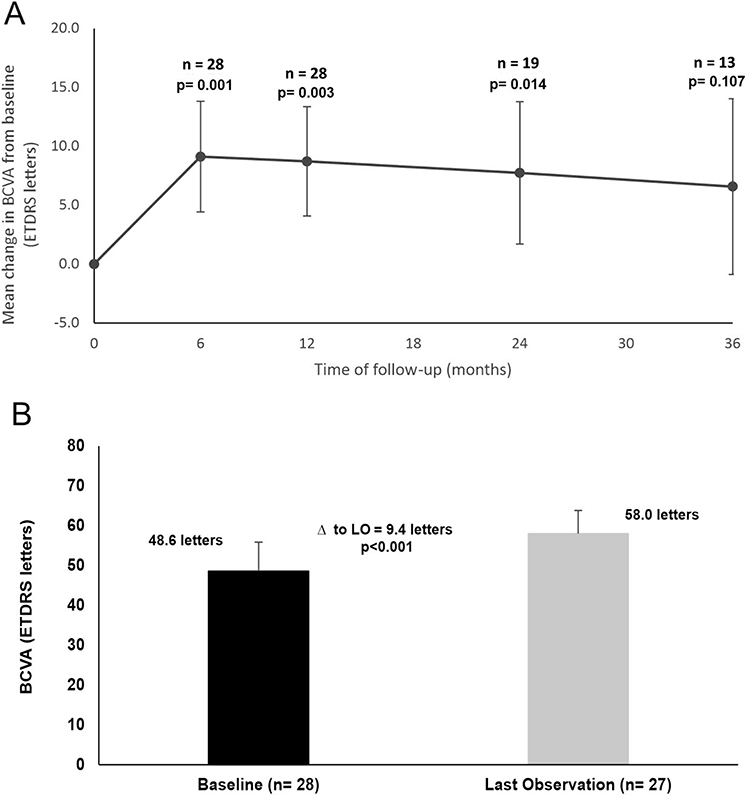 |
Figure 1 Change in BCVA in ETDRS from baseline to 36 months of follow-up (A) and the last observation (LO; (B). Notice the increase in vision from baseline to month 6 and the progressive decrease to month 36. |
At last observation, most of the eyes (n=23, 82%) maintained (n=6, 21%) or gained vision. Patients had a BCVA of 58.0 ETDRS letters (95% CI 52.2–63.8), which corresponded to a significant gain of 9.5 ETDRS letters (95% CI 5.1–13.9, p<0.001) compared to baseline (Figure 1B). Moreover, a gain of ≥5 letters from baseline to the last observation was achieved in 17 eyes (60.7%). Out of these, 14 eyes (50%) eyes achieved a ≥10 letter gain with 10 of these eyes (35.7%) achieving a ≥15 letter gain. When stratifying for patients with a 36-month follow-up, 10 of 13 patients (76.9%) maintained or gained vision. Of these, six (46.1%) patients gained ≥5 letters from baseline and four (30.8%) patients gained ≥10 letters, of which 3 (23.1%) gained ≥15 letters.
Central Macular Thickness
At baseline, patients had a mean CMT of 530.5 µm (95% CI 463.0–598.0) (Table 1). After the FAc implant, a decrease in CMT was observed, starting at the first month of follow-up (mean CMT reduction −170.5µm, 95% CI −223.8– −117.1; p<0.001). Changes in CMT observed at months 6 (−173.7µm, 95% CI −226.6– −120.9), 12 (−219.1µm, 95% CI −293.0– −145.2), 24 (−177.8µm, 95% CI −258.5– −97.1) and 36 (−188.7µm, 95% CI −285.4– −92.0) were significantly different when compared to baseline (p<0.005, Figure 2A). The maximum decrease in CMT was observed at month 12 (p<0.001). At the last observation, 15 eyes (53.6%) presented a CMT ≤315µm, and 22 patients (78.6%) had a decrease in CMT ≥20% compared to baseline. The mean change of CMT from baseline to last observation was −212.1µm, 95% CI −275.2– −149.1 (p<0.001, Figure 2B). Figure 3 depicts the CMT evolution of some patients with 36-month follow-up.
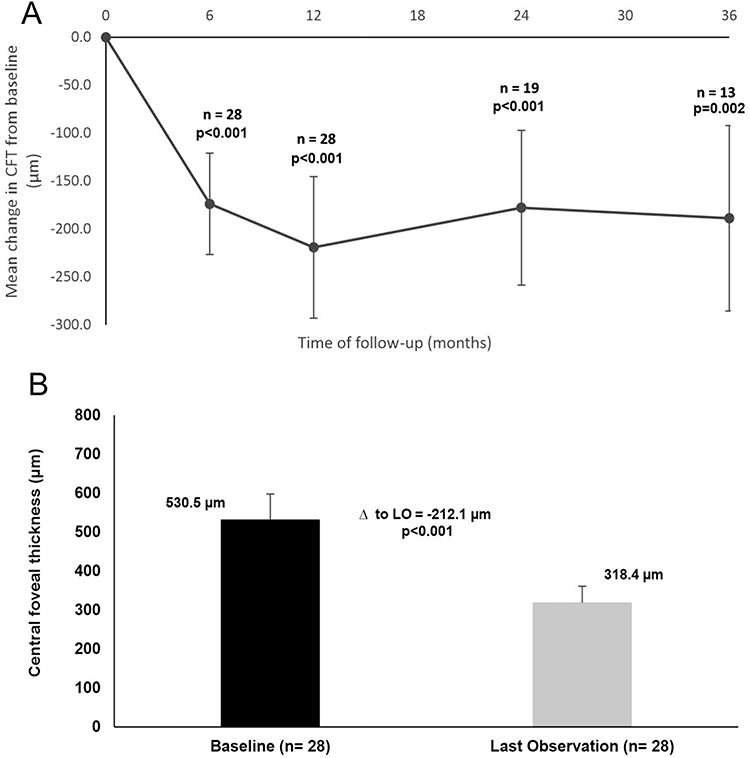 |
Figure 2 Changes in CMT from baseline to 36 months of follow-up (A) and to last observation (B). Notice the decrease in CMT from baseline to month 6 and the relative stability of the CMT over the 36 months. |
 |
Figure 3 Representation of the CMT evolution through SD-OCT in three patients with 36-month follow-up. CMT and BCVA data are presented. Important to note that case 2 developed a cataract after FAc implant and was submitted to cataract phacoemulsification during a 12–24-month follow-up. |
Intraocular Pressure
Figure 4 represents the IOP over follow-up for patients treated with the 0.2 μg/day FAc implant. Mean IOP at baseline was 16.4mmHg (95% CI 15.3–17.5), and there were no statistically significant differences at any timepoint or last observation versus baseline (p>0.05; Figure 4). Nine eyes (32.1%) had an IOP ≥21mmHg during follow-up and 12 eyes (42.9%) received IOP-lowering medication during follow-up. Of these, seven patients (58.0%) were already under ocular hypotensive treatment for glaucoma at baseline. None of the eyes required IOP-lowering surgery.
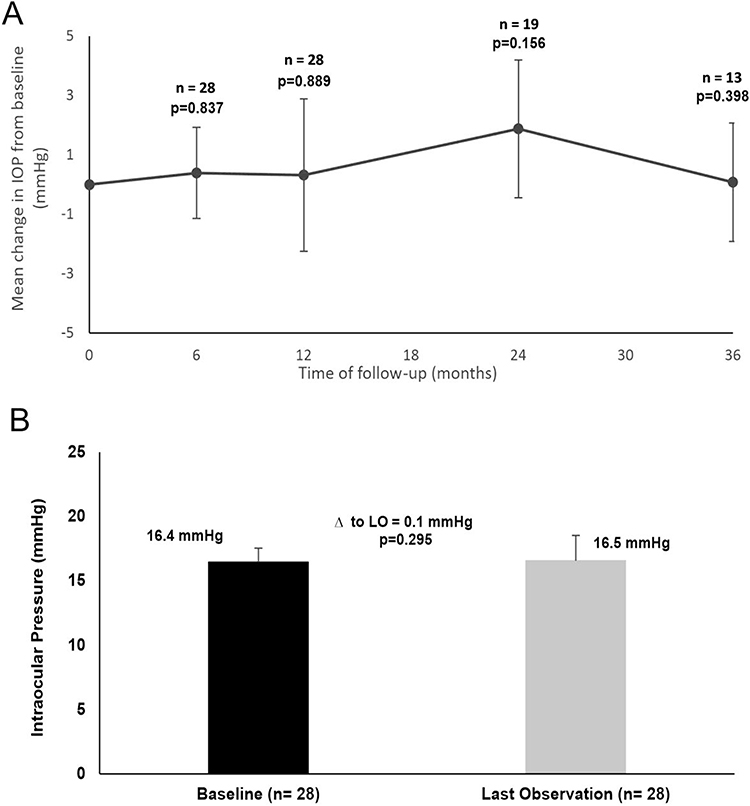 |
Figure 4 Changes in IOP from the baseline to 36 months of follow-up (A) and the last observation (B). Notice that, despite the slight increase, IOP was relatively stable during the 36-month follow-up. |
Discussion
This study aimed to report the functional, anatomic and safety-related long-term outcomes of a single 0.2 μg/day FAc implant injection administered in 28 patients with persistent and recurrent DME. In our study, rapid and significant visual and anatomical outcomes were achieved in most patients within one month of treatment with persistent functional and anatomical gain along 36 months of follow-up. This is in line with previous studies of the Portuguese population, with similar early significant gains in vision.23
Regarding BCVA, a significant functional improvement was noted at 36 months and last observation, with 76.9% and 82.1% (respectively) of the studied population achieving stable or improved vision. This represents a numerical improvement compared to the FAME trial, where only 28% of the study population achieved similar visual gains after 24 and 36 months of follow-up.24 Additionally, when comparing to the IRISS and Medisoft studies, we also report a numerically higher number of patients with stable or improved vision at 36 months (76% vs 71% and 72%, respectively).25,26 Despite not being significantly different compared to baseline, our functional results at 36 months (increase of 6.6 ETDRS letters) also seem to be slightly superior to the ones presented in the IRISS, Medisoft, and PALADIN studies, where patients achieved an improvement of 4.6 (baseline of 52.2 to 57.1 letters), 4.1 (baseline of 52.2 to 57.1 letters), and 3.6 letters (baseline of 62.3 to 65.9 letters), respectively. However, it is important to note that this is probably due to the larger sample of these studies, and because our patients had a lower baseline BCVA (48.6 letters).
Overall, the sustained functional improvement with the 0.2 μg/day FAc implant was accompanied by a significant decrease in CMT up to 12 months, followed by stability or improvement until 36 months. In fact, despite the lack of significance in BCVA change at month 36, patients still experienced a significant CMT reduction. These results support previous findings on the long-term effects of 0.2 μg/day FAc implant in DME that reveal that the sustained delivery of FAc contributes not only to anatomical benefits and visual gains but also to the preservation of vision, as the implant promotes a reduction of the inflammation responsible for retinal cell death and loss of vision.7,18,21,27 Our study reports that significant anatomical benefits still occur long term, with 53.6% of patients achieving ≤315µm CMT and a decrease in CMT ≥20% compared to baseline at the last observation. Once again, despite following the same pattern, our results at month 36 were superior to the PALADIN study (CMT decrease of 60.69μm: baseline of 386.10 to 325.41μm), respectively.25
By reducing inflammation, intravitreal corticosteroids act in the three main lesion pathways of DME, namely neurodegeneration, edema and ischemia. This has been documented in several studies where the 0.2 μg/day FAc implant reduced the expression of IL-6, IP-10, MCP-1, and CD54 and stabilized the rate of neurodegeneration of retinal ganglion cells.10,28 In contrast, VEGF and placental growth factor levels are not significantly affected by the implant.10 Even though there is limited information regarding the need for combined treatment in DME, a possible association therapy of intravitreal anti-VEGF and corticosteroids is still controversial.29 In this study, a need for additional therapies during follow-up was observed. However, our data reveals that only five eyes (17.9%) required additional intravitreal anti-VEGF and/or corticosteroid injections, highlighting the effectiveness of the FAc implant in the studied population. This is in line with previous real-world evidence in which 30% of DME cases needed supplemental therapy following treatment with an FAc implant.30
Despite the described functional and anatomical results, specialists need to consider the risks associated with implant insertion (ie, anterior chamber dislocation) and long-term adverse events such as ocular hypertension and the development of cataracts.13 Previous studies have reported IOP increases during the follow-up of patients with FAc implants.16,19 Our study shows, however, that IOP remained stable during follow-up, with mean changes to the baseline showing no statistical significance (p>0.05) at any timepoint, and only 32.1% of the studied eyes presenting IOP above 21mmHg during follow-up, highlighting the safety profile of the FAc implant. Additionally, although 42.9% (12 eyes) received IOP-lowering medication during follow-up, seven of these patients were already under ocular hypotensive drugs for glaucoma, which may pose a possible risk factor for increased steroid response.25,26 Although we do not report any need for IOP-lowering surgery, the proportion of eyes receiving IOP-lowering treatment in this study is numerically higher compared to the IRISS (35.1%), Medisoft (28.9%), and PALADIN (22.3%) studies.25,26,31 Regarding other possible adverse events, the implant was well tolerated, with no reported complications related to its insertion or dislocation during follow-up.
As different studies keep providing data to support the sustained three-year release of FAc with positive outcomes,7,15 benefits to disease management can be envisioned, including an increase in patients’ compliance and a decrease in the development of ocular adverse events, such as endophthalmitis and traumatic cataracts alongside a positive impact on the economic burden related to DME.32
One of the strengths of this study is the evaluation of the effectiveness of the Fac implant in a real-life setting, without excluding patients with prior treatments for DME. This contrasts with the FAME trial in which eyes that had previously undergone vitrectomy were excluded.
Our study presents some limitations, namely its retrospective nature, which means its reliability relies on the precision of clinical record maintenance. Additionally, a possible selection bias could have occurred, as all patients had previously undergone corticosteroid injections, possibly excluding those with high corticosteroid sensitivity for IOP rise. Moreover, we reported differences in follow-up time between patients, with only 46.4% completing 36 months of follow-up. Nevertheless, the mean follow-up observation of 25 months is numerically superior to most studies found in the literature. Finally, due to the nature of the disease, there is a relatively small sample size in this study which may restrict the generalizability of the results.
In this study, we evaluated the long-term results of the FAc implant for the treatment of chronic DME. Despite the heterogeneity of the studied population and potential adverse events, our results support the effectiveness and safety profile of the implant. Although additional long-term real-world evidence is required, the sustained release of FAc may represent a safe strategy for daily, low-dose, sustained and localized release of FAc to the posterior segment of the eye, providing both functional and anatomical benefits in DME.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ding J, Wong TY. Current epidemiology of diabetic retinopathy and diabetic macular edema. Curr Diab Rep. 2012;12(4):346–354. doi:10.1007/s11892-012-0283-6
2. Adan A, Cabrera F, Figueroa MS, et al. Clinical-decision criteria to identify recurrent diabetic macular edema patients suitable for fluocinolone acetonide implant therapy (ILUVIEN((R))) and follow-up considerations/recommendations. Clin Ophthalmol. 2020;14:2091–2107. doi:10.2147/OPTH.S252359
3. Coelho J, Malheiro L, Melo Beirao J, Meireles A, Pessoa B. Real-world retrospective comparison of 0.19 mg fluocinolone acetonide and 0.7 mg dexamethasone intravitreal implants for the treatment of diabetic macular edema in vitrectomized eyes. Clin Ophthalmol. 2019;13:1751–1759. doi:10.2147/OPTH.S201611
4. Bressler NM, Beaulieu WT, Glassman AR, et al. Persistent macular thickening following intravitreous aflibercept, bevacizumab, or ranibizumab for central-involved diabetic macular edema with vision impairment: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2018;136(3):257–269. doi:10.1001/jamaophthalmol.2017.6565
5. Estebainha R, Goldhardt R, Falcao M. A new approach for diabetic macular edema treatment: review of clinical practice results with 0.19 mg fluocinolone acetonide intravitreal implant including vitrectomized eyes. Curr Ophthalmol Rep. 2020;8(1):1–10. doi:10.1007/s40135-020-00225-1
6. Boyer DS, Yoon YH, Belfort R, et al. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology. 2014;121(10):1904–1914. doi:10.1016/j.ophtha.2014.04.024
7. Campochiaro PA, Brown DM, Pearson A, et al. Sustained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabetic macular edema. Ophthalmology. 2012;119(10):2125–2132. doi:10.1016/j.ophtha.2012.04.030
8. Das A, McGuire PG, Rangasamy S. Diabetic macular edema: pathophysiology and novel therapeutic targets. Ophthalmology. 2015;122(7):1375–1394. doi:10.1016/j.ophtha.2015.03.024
9. Wells JA, Glassman AR; Diabetic Retinopathy Clinical Research N. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193–1203.
10. Deuchler SK, Schubert R, Singh P, et al. Vitreous cytokine levels following the administration of a single 0.19 mg fluocinolone acetonide (ILUVIEN®) implant in patients with refractory diabetic macular edema (DME)-results from the ILUVIT study. Graefes Arch Clin Exp Ophthalmol. 2022;260(8):2537–2547. doi:10.1007/s00417-00022-05564-00412
11. Habib MS. ILUVIEN((R)) technology in the treatment of center-involving diabetic macular edema: a review of the literature. Ther Deliv. 2018;9(8):547–556. doi:10.4155/tde-2018-0006
12. Messenger WB, Beardsley RM, Flaxel CJ. Fluocinolone acetonide intravitreal implant for the treatment of diabetic macular edema. Drug Des Devel Ther. 2013;7:425–434. doi:10.2147/DDDT.S44427
13. Alimera Sciences Limited. Iluvien summary of product characteristics. Available from: https://www.medicines.org.uk/emc/product/3061/smpc.
14. Campochiaro PA, Hafiz G, Shah SM, et al. Sustained ocular delivery of fluocinolone acetonide by an intravitreal insert. Ophthalmology. 2010;117(7):1393–1399 e1393. doi:10.1016/j.ophtha.2009.11.024
15. Campochiaro PA, Nguyen QD, Hafiz G, et al. Aqueous levels of fluocinolone acetonide after administration of fluocinolone acetonide inserts or fluocinolone acetonide implants. Ophthalmology. 2013;120(3):583–587. doi:10.1016/j.ophtha.2012.09.014
16. Alfaqawi F, Lip PL, Elsherbiny S, Chavan R, Mitra A, Mushtaq B. Report of 12-months efficacy and safety of intravitreal fluocinolone acetonide implant for the treatment of chronic diabetic macular oedema: a real-world result in the United Kingdom. Eye (Lond). 2017;31(4):650–656. doi:10.1038/eye.2016.301
17. Bertelmann T, Schulze S. Long-term follow-up of patient with diabetic macular edema receiving fluocinolone acetonide intravitreal implant. Ophthalmol Ther. 2015;4(1):51–58. doi:10.1007/s40123-015-0028-0
18. Fusi-Rubiano W, Mukherjee C, Lane M, et al. Treating diabetic macular oedema (DMO): real world UK clinical outcomes for the 0.19mg Fluocinolone Acetonide intravitreal implant (Iluvien) at 2 years. BMC Ophthalmol. 2018;18(1):62. doi:10.1186/s12886-018-0726-1
19. Meireles A, Goldsmith C, El-Ghrably I, et al. Efficacy of 0.2 mug/day fluocinolone acetonide implant (ILUVIEN) in eyes with diabetic macular edema and prior vitrectomy. Eye (Lond). 2017;31(5):684–690. doi:10.1038/eye.2016.303
20. Pessoa B, Coelho J, Correia N, Ferreira N, Beirao M, Meireles A. Fluocinolone acetonide intravitreal implant 190 mug (ILUVIEN(R)) in vitrectomized versus nonvitrectomized eyes for the treatment of chronic diabetic macular edema. Ophthalmic Res. 2018;59(2):68–75. doi:10.1159/000484091
21. Bailey C, Chakravarthy U, Lotery A, Menon G, Talks J, Medisoft Audit G. Real-world experience with 0.2 mug/day fluocinolone acetonide intravitreal implant (ILUVIEN) in the United Kingdom. Eye (Lond). 2017;31(12):1707–1715. doi:10.1038/eye.2017.125
22. Rehak M, Busch C, Unterlauft JD, Jochmann C, Wiedemann P. Outcomes in diabetic macular edema switched directly or after a dexamethasone implant to a fluocinolone acetonide intravitreal implant following anti-VEGF treatment. Acta Diabetol. 2020;57(4):469–478. doi:10.1007/s00592-019-01439-x
23. Carneiro A, Meireles A, Castro Sousa JP, Teixeira C. Clinical impact of the 0.2 µg/day fluocinolone acetonide intravitreal implant: outcomes from the ILUVIEN(®) clinical evidence study in Portugal. Ther Adv Ophthalmol. 2020;12:2515841420917768. doi:10.1177/2515841420917768
24. Campochiaro PA, Brown DM, Pearson A, et al. Long-term benefit of sustained-delivery fluocinolone acetonide vitreous inserts for diabetic macular edema. Ophthalmology. 2011;118(4):626–635 e622. doi:10.1016/j.ophtha.2010.12.028
25. Singer MA, Sheth V, Mansour SE, Coughlin B, Gonzalez VH. Three-year safety and efficacy of the 0.19-mg fluocinolone acetonide intravitreal implant for diabetic macular edema: the PALADIN study. Ophthalmology. 2022;129(6):605–613. doi:10.1016/j.ophtha.2022.01.015
26. Bailey C, Chakravarthy U, Lotery A, Menon G, Talks J. Extended real-world experience with the ILUVIEN® (fluocinolone acetonide) implant in the United Kingdom: 3-year results from the Medisoft® audit study. Eye (Lond). 2022;36(5):1012–1018. doi:10.1038/s41433-021-01542-w
27. Quhill H, Quhill F. Real-Life ILUVIEN (Fluocinolone Acetonide) case study: rapid drying of the macula and improved vision within 2 years after therapy initiation. Case Rep Ophthalmol. 2016;7(3):301–307. doi:10.1159/000452883
28. Pessoa B, Castro C, Ferreira A, et al. Changes in Ganglion Cell Layer Thickness after Treatment with the 0.2 microg/day fluocinolone acetonide implant in vitrectomized and nonvitrectomized eyes with diabetic macular edema. Ophthalmic Res. 2022;65(3):310–320. doi:10.1159/000520411
29. Amoaku WM, Saker S, Stewart EA. A review of therapies for diabetic macular oedema and rationale for combination therapy. Eye (Lond). 2015;29(9):1115–1130. doi:10.1038/eye.2015.110
30. Chakravarthy U, Taylor SR, Koch FHJ, Castro de Sousa JP, Bailey C; Group IRSSI. Changes in intraocular pressure after intravitreal fluocinolone acetonide (ILUVIEN): real-world experience in three European countries. Br J Ophthalmol. 2019;103(8):1072–1077. doi:10.1136/bjophthalmol-2018-312284
31. Khoramnia R, Peto T, Koch F, et al. Safety and effectiveness of the fluocinolone acetonide intravitreal implant (ILUVIEN): 3-year results from the European IRISS registry study. Br J Ophthalmol. 2022;15(321415):2022–321415.
32. Nurozler Tabakci B, Unlu N. Corticosteroid Treatment in Diabetic Macular Edema. Turk J Ophthalmol. 2017;47(3):156–160. doi:10.4274/tjo.56338
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.