")
Back to Journals » Advances in Medical Education and Practice » Volume 14
Reflecting on Students’ Experiences of an Innovative Teaching Model During Aged Care Visit in Clinical Placements: A Qualitative Pilot Study
Authors Xu D, Feng S, Yang D, Ding S, Rosman JB, Kuang M , Xiao H
Received 14 September 2023
Accepted for publication 7 November 2023
Published 28 November 2023 Volume 2023:14 Pages 1339—1346
DOI https://doi.org/10.2147/AMEP.S436905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Dan Xu,1,2 Shaoting Feng,1 Daya Yang,1 Shuqin Ding,1 Johan B Rosman,2 Ming Kuang,1 Haipeng Xiao1
1First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Curtin Medical School, Faculty of Health Sciences, Curtin University, Perth, Australia
Correspondence: Dan Xu; Haipeng Xiao, Email [email protected]; [email protected]
Purpose: Clinical placement teaching could be challenging due to time constraints, lack of effective teaching models and consensus approaches. Learner-centred approach facilitated deeper learning by demonstrating “seeing-patients-under-supervision” being ideal during Residential-Aged-Care-Facility (RACF)-visit in GP clinical placements. The study aimed to reflect on the students’ experiences in aged-care visits by applying an innovative teaching model of “students-being-the-GP-clinician-in-charge-of-RACF-visit-ward-round-under-the-supervision-of-clinical-supervisor”. Through students’ reflections, this study identified 12 commonly managed RACF problems to be introduced into the curriculum to optimise clinical reasoning learning during RACF-visit.
Methods: This qualitative study used online surveys and interviews. All participating students reported all the encountered cases during the RACF visit through an online survey. The participating students acted as GP in charge of all clinical interactions with patients, caregivers, and nurses during RACF visits and final management plan discussions with GP supervisors to ensure clinical-service safety and teaching-and-learning quality. The interview questionnaires applied standard-and-open-ended-questions to examine the impact of this innovative teaching model on clinical-reasoning-learning, clinical-competence-improvement, Objective Structured Clinical Exam (OSCE) preparation, limitations-from-students’-patients’-and-supervisors’ perspectives, and intern readiness.
Results: An online survey summarising students’ encountered cases was returned by 30 students. The 12 most commonly-managed problems were tabulated. Falls, urinary tract infections, and behavioural and psychological symptoms of dementia were the three most commonly-managed problems. All thirty students’ reflections indicated the positive impact of the innovative-teaching-models on “Improving-Clinical-Reasoning-Learning”, “Enhancing-Clinical-Competency”, “Enriching-Salient-Learning-Points”, “Facilitating-Feedback-Discussion-with-Supervisor”, “Strengthening-OSCE-exam-preparation”, “Understanding-the-Limitation-from-students’-patients’-and-supervisors’-perspectives”, “Enabling-intern-readiness”. Twelve students’ individual reflections were demonstrated.
Conclusion: This qualitative pilot study demonstrated through students’ reflection that “Student-doctor-in-charge-of-nursing-home-round” is an innovative teaching model for clinical reasoning learning. This model extended the concepts of “cognitive-apprenticeship” in the context of modern medical education. Students’ reflections and summary of commonly managed problems indicated the need for further study to verify the feasibility of implementing this teaching model in the formal curriculum and creating a RACF-visit-specific curriculum for students.
Keywords: clinical reasoning learning, learner-centred approach, cognitive apprenticeship
Introduction
Teaching senior medical students during clinical placements can be a challenging task in terms of time constraints, lack of effective teaching model and lack of consensus teaching approach.1,2 Residential aged care facilities (RACFs) have been demonstrated to provide unique and valuable clinical learning opportunities in studies conducted in the Netherlands, the USA and Australia.3–6 A recent study shows that residential aged care facility (RACF) placements for senior medical students can provide student-valued anticipated learning outcomes with opportunities for inter-professional learning. However, these placements lack innovative teaching models, consistent learning approaches, and RACF-relevant topical curricula. To overcome the deficiencies in delivering these placements’ teaching and learning, the aim of this study is designed to reflect on the students’ experiences in aged care clinical placements by applying an innovative teaching model of “students being the consultant GP in charge of RACF ward round under the supervision of clinical supervisor”. This innovative teaching model demonstrates the learner-centred approach, which is well established in medical education to be essential in facilitating deeper learning.7 This study identifies RACF-relevant topics to be introduced into the curriculum for optimising clinical reasoning learning by interviewing students on completion of the placements.
Methods
Study Design
This was a mixed-method qualitative study that used individual interviews in conjunction with written reflections from individual students. All participating students recorded all the cases they encountered during the RACF ward round to develop a condition-specific curriculum during the interview on the completion of the placement. All participating students played the role of taking charge of the GP and interacting clinically with patients, caregivers, and nurses at the RACF ward round. The final plan for patient management was discussed with a GP supervisor to ensure the quality of care and development of learning points for students. The innovative teaching model used in the RACF ward round showcased the three-way clinical interaction, including student doctor in charge of the consultation, supervising doctor overseeing, and assisting the consultation at clinical decision-making points such as clinical assessment, investigation, diagnosis, and management, and patients receiving a consensus management plan after extensive condition-specific education through student doctors’ explanations and discussions.
Setting of Participants and Data Collection
Fifteen Australian and Chinese final-year medical students participated in RACF visits during to 4–8 weeks of general practice placements. Detailed time schedules for using these teaching models for students are presented in a table (Table 1). All 30 participating students were allocated five different supervisors but were always observed by the same allocated supervisor.
 |
Table 1 The Duration of “Students Being the GP Consultant in Charge of RACF Ward Round Under the Supervision of Clinical Supervisor” During General Practice Placements |
The interview questionnaires applied only standard and open-ended questions, including the predesigned teaching and learning themes: (1) How and what benefits has this teaching model provided in improving CR learning with its five domains? 2, In what ways has this teaching model improved clinical competence? 3, How has this teaching model broadened salient learning points? 4, In what ways has this teaching model made feedback discussion with supervisor more constructive and interactive? 5, How does this teaching model affect the OSCE exam preparation? 6) Is there any limitation from students’, patients’ and supervisors’ perspectives on this teaching model? 7, What effect of this teaching model on the readiness to become an intern?
The students were also asked to record all encountered cases at the RACF to summarise the top 12 most common conditions/problems managed by visiting the GPs in the online survey. The survey aimed to develop a condition/problem-specific curriculum for students’ aged care learning.
Data Analysis
The survey data were descriptively analysed by the authors due to the nature of the data gathered.8 Participating participants were interviewed with pre-designed questions by the main author to collect students’ reflections for semantic analysis. The reflection data were transcribed and summarised into learning and teaching themes by the main author. Qualitative content analysis was conducted based on the interview questionnaire, and the outcomes were summarised as teaching and learning themes in the results section of students’ reflective samples based on the most common problems or conditions they encountered during the placement.
Ethics
Ethical approval was granted by the ethics committees of Curtin University and First Affiliated Hospital of Sun Yat-sen University.
Consent for Participation
Informed written consent was obtained from all participants via electronic invitation including informed consent with publication of participants’ anonymized responses.
Results
An online survey regarding a summary of the students’ encountered cases was completed and returned by 30 students. The top 12 most commonly-managed conditions/problems are presented in Table 2.
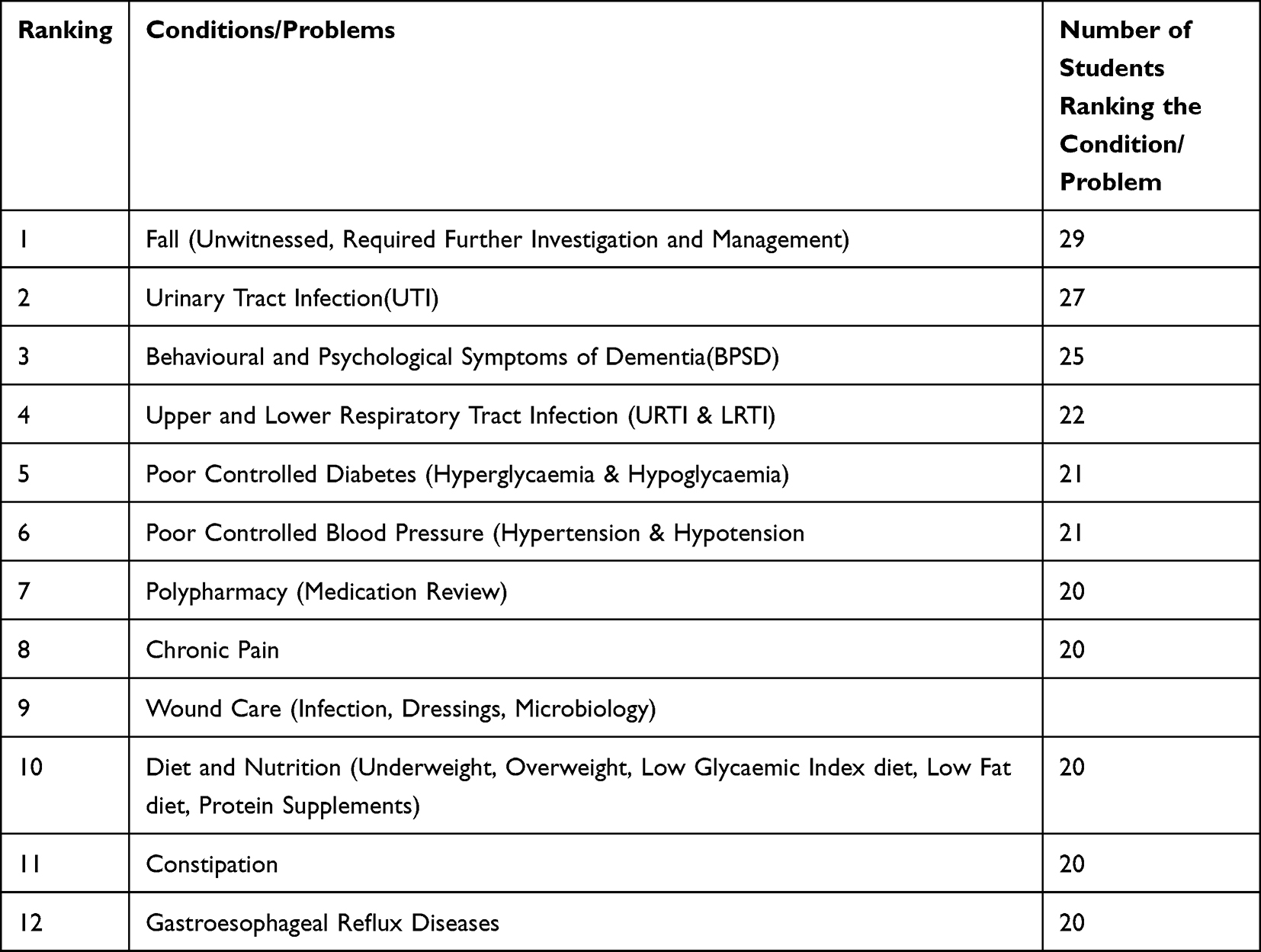 |
Table 2 Ten Most Common Conditions/Problems Managed by Visiting GPs at RACF |
Falls (unwitnessed, requiring further investigation, and management) were the most common problems managed by the student doctor in charge, which included fall clinical assessment, risk factor screening, cause identification, non-pharmacological and pharmacological management, and fall prevention using a multidisciplinary approach. Urinary tract infection was the second most common condition managed by the student doctor in charge, and included clinical assessment, relevant physical examination, laboratory investigation, diagnosis confirmation, comprehensive management, and appropriate further investigation and management for the prevention of recurrent infection. Behavioural and Psychological Symptoms of Dementia (BPSD) were the third most common conditions managed by the student doctor in charge, which was challenging for the student doctor in charge because history taking is difficult and unreliable and physical examination is not interpretable due to uncooperative behaviours of the patients.
All 30 students were interviewed for reflection, which was summarised in the pre-designed learning and teaching themes. The main theme of this stage is clinical reasoning learning based on the five domains of clinical reasoning learning.9 The remaining six themes included “Clinical Competency”, “salient learning points”, “Feedback discussion with supervisors”, “Impact on OSCE exam preparation”, “Limitation from students’, patients’, and supervisors’ perspectives’, and Impact on your readiness to become an intern”. All reflections described their clinical placement experiences with the student being doctor-in-charge during the RACF ward round.
A few individual students’ reflections on the seven themes based on the most commonly-encountered problems or conditions are illustrated below.
Student one (Fall): In contrast to traditional observer-style learning, I am the doctor in charge and able to form my own clinical reasoning under supervision instead of attempting to remember someone else’s, thus increasing my knowledge and clinical skill retention.
The most memorable case was an unwitnessed fall in a 92 years old lady with left periorbital bruise injury. I was able to learn about the circumstances of the fall with a subsequent plan to organise a 24-hour Holter monitor, which gave out the eventual diagnosis of many pauses within the 24-hour ECG. Consequently, the patient was referred for a successful pacemaker insertion. I appreciate my supervisor for letting me go through the entire consultation during the ward round. It really dawned me that falls can harbour many causes; however, my clinical assessment focused only on pathological causes of differentiating cardiovascular causes from neurological causes. My supervisor provided me with salient learning points as the framework of the clinical approach for fall cause screening, including physiological causes due to aging (poor vision with cataract/macular degeneration and poor hearing), pathological causes (I did well in this case), environmental causes (floor without anti-slippery mat may easily trigger falls), and medication causes (antihypertensive may cause postural hypotension leading to the fall). Upon reflection, I probably would have missed the clinical assessment of three other causes of falls. Thus, I can almost confidently conclude that I am progressing towards a competent intern when I have been the student doctor in charge during the nursing home-ward rounds.
The limitation of this teaching model was that it balanced the time management of our supervisor and that of the care staff, including clinical nurse managers, duty nurses, and caregivers accompanying the round.
Student two (Urinary Tract Infection): This teaching model of student-doctor in charge of nursing home ward rounds required a focused history and examination, as opposed to in medical school, where you learn to do a full history and examination of each system. One of the cases I managed during the ward round was a new case of 83 an old lady with a recurrent UTI. My management was to confirm UTI with MSU collection, then commence empirical antibiotics and review after the MSU result returned. The clinical reasoning discussion with my supervisor allowed me to have in-depth learning about the risk factors of recurrent UTI, including constipation, peri-genital hygiene, and urinary tract structural abnormalities. I returned to obtain more history from the patient and care staff after the ward round with the final management plan of urinary tract ultrasound to identify reflux inside the urinary tract and potential obstructions. Ultrasound identified a staghorn renal stone, which was referred to a urologist for further management. My supervisor also used the opportunity to revise the urinary tract anatomy, especially the three narrowing along the urinary tract, where stones are commonly lodged. After this case, my role as a student doctor in charge allowed me to extend the simple and common problem to different disciplines of learning. This case also taught me about the different bacterial species responsible for recurrent UTI. I am certain that my OSCE exam preparation will benefit daily cases treated at an OSCE exam station.
Student three (Behavioural and Psychological Symptoms of Dementia): I initially thought that nursing home visits in GP placement would be limited in terms of learning clinical reasoning with unreliable history and difficult physical examination due to poor cooperation, especially in patients with dementia. When I became the doctor in charge of the ward round, the collateral history from the care staff and a specific clinical approach made the consultation efficient in developing a tailored management plan. Learning how to realistically plan an investigation, not just agreeing with what a supervisor has already mentioned. Exactly what tests you want – not just using generic phrases like “blood test” or “imaging” but more specifically oriented to differential diagnosis and management eg FBP, U&Es, LFTs, ANAs, ASO titre or CT angiogram with contrast.
Student four (Upper and lower respiratory tract infections): Before I joined my aged care visits during GP placement, my expectation for any case of respiratory tract infection would be management with supportive measures, symptomatic treatment, and antibiotics on infrequent occasions. Clinical reasoning teaching using student-doctor-in-charge has opened up diverse discussions of many learning points regarding the topic during our nursing home rounds. Many cases of pneumonia have increased our scope to study the bacteriology of pneumonia with rare conditions or differential diagnosis of pneumonia-associated conditions, including PCP and immunocompromised diseases such as HIV. The red-flag diagnosis provided us with the opportunity to learn about tonsillar abscesses, sinusitis, and severe reflux disease. The rewarding learning points in terms of clinical skills included the interpretation of various crepitation and CXR findings, which provided immense benefits for my OSCE exam preparation and my intern year.
Student five (Poor controlled diabetes): During the nursing home rounds by the student doctor in charge, we managed many hyperglycaemia cases. I initially instructed the nursing staff and patients to increase the dose of insulin and diabetes medications. My discussion with my supervisor always brought about two extra points of management: spot urine for ketones and bedtime BGL checks. I did not realise the importance of these extra points until we had a case of DKA and another case of nocturnal hypoglycaemia leading to fall and fracture of the femoral neck. I really appreciate my student-doctor in-charge role with the large learning resources and the clinical reasoning discussion with our supervisor at our nursing home round, which provided both confidence and clinical skill training to prepare me as a competent clinician.
Student six (Poor controlled blood pressure): Being the doctor in charge is a good revision for the student; it reinforces what we know and highlights the gaps in our knowledge. By observing many cases of hypertension and hypotension, I managed to address many gaps in my clinical approach, assessment, diagnosis, and management. In terms of hypertension, I previously knew only to confirm the clinical diagnosis through lifestyle modifications and pharmacological interventions. After the experience of the student doctor in charge, I now know to broaden my clinical approach by investigating secondary causes and minimising target organ damage, including the heart, brain, kidneys, and eyes. Managing hypotension cases helped develop a thorough framework of clinical approach, including immediate nonpharmacological management if symptomatic, checking various causes (physiological, pathological, environmental, and medication), and applying management (nonpharmacological and pharmacological interventions). The teaching approach provided me with many opportunities to practice the above-mentioned clinical approaches to fill my learning gaps, thus fulfilling my goal of clinical competency for future career practice.
Student seven (Polypharmacy): Assuming the in-charge doctor’s role is an excellent way for student doctors to practice their communication skills, including discussions with patients and next of kin regarding medication review for deprescribing, motivational interviewing, and navigating a wide range of emotions from patients. The case taught me that most was a case of medication review in light of polypharmacy. I was the student doctor in charge of discussing with next of kin an 80-year-old woman for deprescribing five medications out of her list of ten medications. Clinical reasoning learning was used to manage the adverse consequences of polypharmacy and the effective application of deprescribing guidelines, in which nursing home patients were perfect candidates for students to learn about the topic.
Student eight (Chronic Pain): The feedback discussion section with the supervisor after each patient during the round allowed for reflection on the positives and negatives of student-doctor consultation. During round I was the student doctor in charge; I thought managing chronic pain would be simply pain assessment, analgesia, and monitoring the side effects of pain medications. The student doctor in the charge nursing home round expanded my clinical reasoning learning into frequently somatising and complex chronic mental health patients at the nursing home. I have grown my confidence in managing patients with complex chronic pain and will benefit my future role as a junior doctor.
Student nine (Wound Care): I always thought wound care was a nursing issue when I helped the nurses change a few wound dressings at the beginning of my nursing home visits. During this round, my supervisor taught me what to discuss with the staff from the perspective of being an in-charge doctor. I learned about wound infection and the importance of the locations (potential osteomyelitis at certain locations) as well as various dressings to apply and antibiotic stewardship to minimise the risks of resistant bacterial development. Wound care in nursing homes provides a great opportunity for students to learn practical and clinical skills in managing chronic wounds from multidisciplinary perspectives (duty nurses, wound care nurse specialists, and general practitioners).
Student ten (Diet and Nutrition): The student doctor in charge of the nursing home round came across many cases requesting the management of weight loss and weight gain. I, being the in-charge doctor, initiate investigations and relevant management, however my supervisor invited me into a few family meetings to meet the multidisciplinary team including speech pathologists, dieticians, carers and nurses. I used my medical knowledge to work closely with speech pathologists for post-stroke patients, and dieticians for patients with depression. It was rewarding to see the patient’s weight improvement after our multidisciplinary intervention after the third round and family meetings.
Student eleven (Constipation): Constipation is so common in the nursing home setting, I initially managed with regular toileting and aperients. During one of our routine rounds, I was in charge of an 85 years old patient with constipation for 4 days, despite giving many aperients. On day 5, the patient experienced multiple watery movements, and I was requested to reduce the number of aperients. My supervisor requested that I examine the patient’s abdomen and find signs of faecal loading, which were subsequently confirmed by plain abdominal radiography. The student doctor in charge during the nursing home round required supervision to minimise the risks of an adverse outcome, which would be bowel obstruction if we simply followed the request from the staff without further clinical assessment. I appreciate the supervision of this role and further understand the importance of clinical reassessment on every encounter in the nursing home setting.
Student twelve (Gastroesophageal Reflux Diseases): Gastroesophageal reflux disease is a common condition encountered by nursing home patients. I learned how to manage the guideline-based use of proton pump inhibitors (PPI), PPI deprescribing to over-the-counter (OTC) antacids, and management of the PEG feeding tube. The case of a patient with PEG tube feeding who developed recurrent aspiration pneumonia made me learn about the literature search for evidence-based management. Before I was assigned the student-doctor role during the nursing home round, I always thought that PEG tube insertion for feeding would prevent aspiration pneumonia. When my supervisor questioned me and requested that I search the literature, I learned that PEG did not prevent aspiration pneumonia. The doctor-in-charge role taught me that evidence-based practice requires ongoing learning and questioning.
Discussion
The students’ reflection on the main theme of CR learning valued the teaching model as the best in terms of the five domains of clinical reasoning learning,9 as well as the rest of the themes being well valued by all the participating students. At the students’ request, we believe it is paramount to discuss the feasibility of the practical and quantitative implementation of this teaching model in the RACF round during clinical placement.
The teaching model of “Student doctor in charge of RACF round” has mirrored an educational term “Cognitive Apprenticeship”. Cognitive apprenticeship is defined as learning-through-guided-experience on cognitive and metacognitive, rather than physical, skills, and processes,10 and is on developing cognitive skills in authentic learning experiences.11 Teaching and learning through cognitive apprenticeship requires a learning process that is understandable to learners for their career practice. The methods and frameworks to support cognitive apprenticeship include modelling, explanation, coaching, scaffolding, reflection, articulation, and exploration.12 Central to cognitive apprenticeship as a method of learning are concepts of situatedness and legitimate peripheral participation.13 Situatedness in medical educational term corresponded to cognitive apprenticeship as a method of learning. In terms of legitimate peripheral participation in our study, the teaching model of “Student doctor in charge of RACF round” has demonstrated the use of modelling, coaching and scaffolding by the supervisor, while the students have engaged in observation, supervised practice and reflection and exploration for their clinical reasoning learning, also provided a well-evidenced learner-centre approach14 and a clinically safe and positive learning environment, which was proved to be valuable to students’ CR learning.15 With students’ reflections, this teaching model ensured the clinical safety of the patient when student doctors were in charge of the full clinical assessment, differential diagnosis and management under supervision.
The cognitive-apprenticeship framework was initially introduced into the undergraduate medical education teaching by Stalmeijer and others15 and was found to be beneficial in undergraduate clinical training, however the framework was subsequently used more often in postgraduate education for junior doctor’s training into their individual specialty.16 The overarching framework of cognitive apprenticeship is to provide scaffolding – just enough structural support that junior doctors may begin to build their own clinical reasoning skills and strategies to enable independent practice. However, with our senior medical students in this study, the teaching model of “Student doctor in charge of RACF round” acted as the scaffolding for cognitive apprenticeship. Consequently, their reflections showed that this scaffolding improved their clinical reasoning skills and thus clinical competence, preparing them well for their OSCE exam and intern year. As we delved into their reflections, our students were constantly using “Reflection”, “Articulation” and “Exploration” to self-analyse upon feedback from supervisor, discuss reflection and learning points and empowering self to the next level of clinical competency. Scaffolding removal for medical students is debatable because of clinical safety, which was reflected in the students’ feedback that they were constantly concerned about clinical decisions when they consulted the patient independently.
All participating students claimed a more in-depth understanding and learning of the five domains of clinical reasoning, especially in the domain of shared decision-making, with enhanced understanding of patient communication and interprofessional communication at multidisciplinary team meetings during nursing home visits. Shared decision-making also allowed students to appreciate the importance of shared decision-making from clinical-safety, medico-legal, professional, and cultural perspectives.
Limitations
This pilot study had some limitations regarding the setting and design of the study. The students’ reflections were from one main supervisor and two associate supervisors at a particular GP clinic associated with the RACFs. Recent research has demonstrated that universities should purposefully design clinical placements in not just university teaching clinics but also multiple community clinics including RACFs with many well-trained supervisors interested in teaching pre-registration students.17 An extension study will be needed to increase the number of participating students to make better interpretation of our current results.
Another emerging limitation of this teaching model for all participating students is the inefficiency of time management, which potentially compromises service quality. A recent narrative review concluded that inefficiency of time management can be a barrier to senior students’ clinical education, suggesting a designated teaching clinic.18 In contrast, most of the students in our study reflected positively that this limitation could potentially turn into a better quality consultation with the benefit of patient management because of the extra time spent during the round to ensure the patients’ and care staff’s understanding of the plan.
Conclusion
This qualitative pilot study clearly demonstrates that “Student doctor in charge of the RACF round” is an effective teaching model in clinical placement for senior-year medical students at RACF visits. This innovative teaching model embraces and extends all features of cognitive apprenticeships with better educational outcomes through active learning. Through this model, students feel confident in applying their own clinical reasoning with a greater degree of assurance in clinical practice. An extension of the current pilot study was planned with more senior-year students to verify the positive outcomes of this teaching model on clinical reasoning, learning, clinical competence, and academic performance in an elderly care setting. Ultimately, this extension study may provide evidence to medical educators and curriculum designers on whether this teaching model should be introduced quantitatively into the curriculum of senior-year clinical placement at RACFs.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request. All data for this study, which were not publicly available, were securely stored in the research drive with encrypted and password-protected files at Curtin University.
Acknowledgments
We acknowledge the staff at Curtin Medical School, Curtin University, Australia, and First Affiliated Hospital, Sun Yat-sen University, China.
Funding
There is no external funding for the study to be declared.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Best J. 2012 teaching medical students; tips from the frontline. Aus Fam Phys. 2012;41(1/2):22.
2. Almoallim H, k A, Minguet J, Alotaibi M. Advantages and perspectives of teaching in outpatient clinics: a systematic review creative education. Sci Res. 2015;6:1782–1789.
3. Huls M, de Rooij SE, Diepstraten A, Koopmans R, Helmich E. Learning to care for older patients: hospitals and nursing homes as learning environments. Med Educ. 2015;49(3):332–339. doi:10.1111/medu.12646
4. Saunders R, Miller K, Dugmore H, Etherton-Beer C. Demystifying aged care for medical students. Clin Teach. 2017;14(2):100–103. doi:10.1111/tct.12484
5. Dent J. Learning in ambulatory care. In: Walsh K, editor. Oxford Textbook of Medical Education. New York: Oxford University Press; 2013:221–231.
6. Kanter SL. The nursing home as a core site for educating residents and medical students. Acad Med. 2012;87(5):547–548. doi:10.1097/ACM.0b013e3182557445
7. Radford J, Dallas A, Ramsay R, Robin E, Todd A. Medical students in residential aged care: a guide. Clin Teach. 2020;17(6):617–623. doi:10.1111/tct.13168
8. Creswell J, Clark V. Designing and Conducting Mixed Method Research.
9. Cooper N, Bartlett M, Gay S, et al., On behalf of the UK Clinical Reasoning in Medical Education (CReME) consensus statement group. Consensus statement on the content of clinical reasoning curricula in undergraduate medical education. Med Teach. 2021;43(2):152–159. doi:10.1080/0142159X.2020.1842343
10. Collins A, Brown JS, Newman SE. Cognitive apprenticeship: teaching the crafts of reading, writing, and mathematics. In: Resnick L, editor. Knowing, Learning, and Instruction: Essays in Honor of Robert Glaser. Hillsdale, NJ: Lawrence Erlbaum Associates, Inc; 1989.
11. Collins A, Brown JS, Holum A. Cognitive apprenticeship: making things visible. Am Educ. 1991;15(3):38–46.
12. Enkenberg J. Instructional design and emerging models in higher education. Comput Human Behav. 2001;17(5–6):495–506. doi:10.1016/S0747-5632(01)00021-8
13. Lave J. Wenger E Situated Learning: Legitimate Peripheral Participation. Cambridge: Cambridge university press; 1991.
14. Spencer JA, Jordan RK. Learner centred approaches in medical education. BMJ. 1999;318(7193):1280–1283. doi:10.1136/bmj.318.7193.1280
15. Stalmeijer RE, Dolmans DHJM, Wolfhagen IHAP, Scherpbier AJJA. Cognitive apprenticeship in clinical practice: can it stimulate learning in the opinion of students? Adv in Health Sci Educ. 2009;14(4):535–546. doi:10.1007/s10459-008-9136-0
16. Merritt C, Daniel M, Munzer BW, Nocera M, Ross JC, Santen S. A cognitive apprenticeship-based faculty development intervention for emergency medicine educators. West J Emerg Med. 2018;19(1):198–204. doi:10.5811/westjem.2017.11.36429
17. Moore K, Bacon R, Bevitt T, et al. Wells C Student-led clinical services within the university health clinic: definition, educational practices and outcome. Focus Health Prof Edu. 2018;19(2):1–13. doi:10.11157/fohpe.v19i2.213
18. Franco RLO, Machado JLM, Grinbaum RS, Martiniano Porfírio GJ. Barriers to outpatient education for medical students: a narrative review. Int J Med Edu. 2019;10:180–190. ISSN: 2042–6372. doi:10.5116/ijme.5d76.32c5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.