")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Risankizumab for the Treatment of Moderate to Severe Psoriasis: Impact on Health-Related Quality of Life and Psychological Wellbeing
Authors Gracia-Cazaña T, Bernal-Masferrer L, Morales-Callaghan AM, Almenara-Blasco M, Gilaberte Y
Received 6 October 2022
Accepted for publication 17 January 2023
Published 25 January 2023 Volume 2023:16 Pages 221—229
DOI https://doi.org/10.2147/CCID.S296544
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Tamara Gracia-Cazaña,* Laura Bernal-Masferrer,* Ana María Morales-Callaghan, Manuel Almenara-Blasco, Yolanda Gilaberte
Dermatology Service, Hospital Miguel Servet, IIS Aragon, Zaragoza University, Zaragoza, Spain
*These authors contributed equally to this work
Correspondence: Tamara Gracia-Cazaña, Dermatology Service, Hospital Miguel Servet, Zaragoza, Paseo Isabel la Católica 1-3, P.O.Box: 50009, Zaragoza, Spain, Tel +34 6657571403, Email [email protected]
Abstract: Biologic treatments are increasingly being used in the management of moderate to severe plaque psoriasis (PSO). Risankizumab (RZB) is a humanized monoclonal antibody that specifically blocks the p19 subunit of interleukin 23, which in turn regulates the activation, differentiation, and survival of Th17. RZB has proved their efficacy and their safety compared to anti-TNF. However, studies that assess and compare the improvement in other secondary PROs such as the patient’s quality of life are still scarce. Health-related quality of life (HRQoL) is the sum of physical health, well-being, and participation; it defines the functional effect of a disease or its treatment and how it is perceived by the patient. The objective of this paper is to analyze the literature on the impact of treatment with RZB on the quality of life of patients with PSO and their psychological well-being. A bibliographic search was carried out to identify all the papers published from July 2015 to June 1, 2022, on RZB treatment in psoriasis and its impact on health-related quality of life and psychological well-being, finally twenty articles have been evaluated in full text, of which 8 were excluded because they did not meet the inclusion criteria. Risankizumab has shown not only to have very relevant data on effectiveness and safety, but all of this is associated with an improvement in quality of life related to health and psychological well-being measured on generic and specific quality of life scales, both in pivotal trials, ad hoc analysis, and data in real clinical practice.
Keywords: Risankizumab, health related quality of life, psoriasis
Introduction
Psoriasis is a chronic immune-mediated inflammatory disease the predominantly affects the skin, but also encompasses a significant list of comorbidities such as an increased risk of mortality, cardiovascular disease, diabetes, hyperlipidemia, or diabetes.1,2
In addition to all of the above is its chronic nature and the feeling of therapeutic failure that often causes a sense of hopelessness and frustration, with an increased risk of suicide compared to the general population. In short, there is the effect of psoriasis at a physical level (due to the psoriasis itself, comorbidities and iatrogenesis), and also at a psychosocial level due to the limitation in social interaction and behavioural changes in daily life. Health-related quality of life (HRQoL) is the sum of physical health, well-being, and participation; it defines the functional effect of a disease or its treatment and how it is perceived by the patient.
The degree of HRQoL alteration is associated with psoriasis-dependent factors, but there are also personal factors that condition the patient’s vulnerability to the disease.3
Due to the profound systemic and emotional impact of this disease, improvements in severity scales such as PASI are not sufficient for assessing the overall effectiveness of treatment, but other scales such as quality of life indices (DLQI, HRQoL, SKINDEX-29, etc.) must be taken into account.4
With the advent of biological drugs, the psoriasis treatment paradigm has changed radically, taking into consideration PASI 90–100 therapeutic goals, and thus improvements in health-related quality of life.5 Risankizumab (RZB) is a humanized monoclonal antibody that specifically blocks the p19 subunit of interleukin 23, which in turn regulates the activation, differentiation, and survival of Th17. The IL23/Th17 pathway is activated in psoriasis, being responsible for the chronic inflammation and skin manifestations of the disease. In this sense, numerous molecules have proved their efficacy, their safety compared to anti-TNF6 however, studies that assess and compare the improvement in other secondary PROs such as the patient’s quality of life are still scarce. It has been observed that low levels of absolute PASI have been related to improvements in the quality of life related to the patient’s health and that even minimal residual disease has been related to a negative impact on the life of patients.7
The objective of this paper is to analyze the literature on the impact of treatment with risankizumab on the quality of life of patients and their psychological well-being.
Materials and Methods
A bibliographic search was carried out to identify all the papers published from July 2015 to June 1, 2022, on risankizumab treatment in psoriasis and its impact on health-related quality of life and psychological well-being. The results have been limited to studies conducted in humans and published in Spanish or English.
The studies were identified by searching the following databases: MEDLINE via PubMed, EMBASE, Centre of Review and Dissemination via University of York, Cochrane Library via Cochrane Database of Systematic Reviews, Cochrane Skin Group, Centre of Evidence Based Dermatology at the University of Nottingham, and the TESEO database of doctoral theses.
Additionally, the search has been expanded with the following websites: ClinicalTrials.gov, reec.aemps.es, Clinicaltrialsregister.eu.
Finally, with the aim of identifying the systematic reviews on quality of life related to health and psychological well-being in psoriasis, and more specifically on treatment with risankizumab, which are currently being carried out, an electronic search was conducted in PROSPERO, the International Prospective Register of Systematic Reviews.
The search terms that have been entered to conduct the definitive search for articles, according to the MeSH and DeSC dictionaries, have been: psoriasis, risankizumab, Health-Related Quality Of Life, quality of life.
Inclusion Criteria for the Studies
- Types of studies: Randomized controlled clinical trials; systematic reviews; observational studies with n greater than or equal to 20.
- Population: Psoriasis patients of legal age, regardless of gender, ethnicity, comorbidity, and prior treatment.
- For studies to be considered, they had to include psoriasis patients treated with risankizumab, at any dose for psoriasis.
- They were restricted to the following languages: Spanish and English.
Exclusion Criteria for the Studies
- Studies published outside the established time range.
- Studies that did not use accepted and validated assessment measures to evaluate health-related quality of life and psychological well-being.
- Case series with less than 20 patients.
- Studies in which risankizumab treatment was for psoriatic arthritis.
- Editorials and narrative reviews.
Management, Data Extraction, Data Synthesis, and Analysis of Methodological Quality
The results obtained by the searches were downloaded to a bibliographic reference manager (Mendeley®), where the papers were filtered based on the title and abstract. During this process, all the duplicate, discarded, and selected references have been recorded in a flow chart (Figure 1). The search was not blind in terms of authors, journal, or institution.
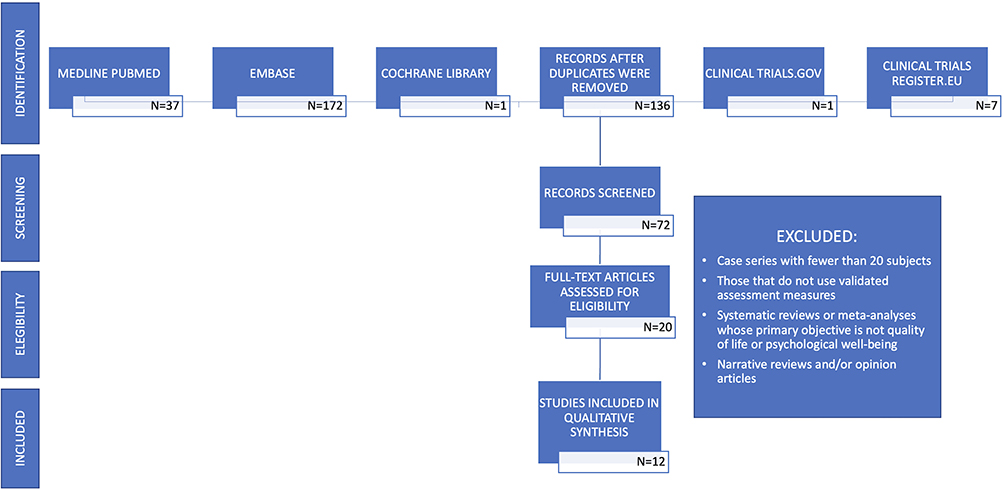 |
Figure 1 Flowchart of the bibliographic search carried out in the systematic review. |
The Jadad scale for randomized trials8 has been consulted, and the critical analysis has been based on the CONSORT guide.9 To synthesize the data, the OSTEBA tool has been used, since it allows the quality of the evidence from the various types of studies to be assessed, in addition to preparing summary tables of results.10
Results
Included and Excluded Studies
Of the 218 records obtained, 198 were excluded after evaluating the title and abstract, and due to duplication in the search databases. Twenty articles have been evaluated in full text, of which 8 were excluded because they did not meet the inclusion criteria or had a small number of patients, as well as the systematic reviews whose primary objective was to evaluate only efficacy and safety, (Figure 1).11–18
Given the small number of clinical trials and systematic reviews, case series have been included, despite the fact that the evaluation of efficacy and effectiveness in them is very limited.19–30 The studies that have been evaluated are: 8 clinical trials with high evidence,19,20,23–26,28,29 3 case series, one prospective,21 and 2 retrospective,22,27 of which the evidence is of low quality, and a cohort study of medium evidence quality.30
The studies have been carried out in Europe, the United States, and Japan. The follow-up period, the number of patients, the characteristics of the study population, and the applied intervention in the included studies are summarized in Table 1.
 |
Table 1 Summary of the Articles Included in the Review, Number of Patients, Intervention, Type of Study, Results, and Level of Evidence |
Sample Size
The number of participants in the included studies varied considerably, with a maximum of 127625 and a minimum of 2021,30 with a total of 5035 patients analyzed. The mean number of participants was 419.5.
Participants
All studies included adults over 18 years old with moderate to severe chronic plaque psoriasis, both men and women.19–29 One study only included patients with genital psoriasis.30
Design
Eight of the twelve included studies are clinical trials,2,19,20,23–26,28 and the rest are case series,21,22,27 and a cohort study.30
Of the studies included, five of them analyze data from the pivotal trials31 UltIMMa-1, UltIMMa-2, which include active comparator with ustekinumab (UST) and placebo (PBO).19,20,23,25,29
In addition, Papp et al20 and Lebwohl et al23,25 use data from the IMMvent and IMMhance clinical trials, with active comparator with PBO and adalimumab (ADA).32,33 Two studies analyze data from the LIMMitless extension clinical trial.24,29 Ohtsuki et al26 evaluated data from the SustaIMM trial comparing RZB 75 mg, 150 mg, and placebo. All these trials have a high level of evidence.
Of the studies with a case series design, one of them is based on the BIOREP registry,27 and analyses patients with moderate-severe psoriasis in the Czech cohort treated with RZB; another article from a real clinical practice carried out in Spain analyses the effectiveness and safety of RZB.21 Mastorino et al22 studied whether there are differences in response to risankizumab in patients with bio-naive psoriasis versus bio-experience.
Finally, a cohort of patients with genital psoriasis has been included in which the efficacy and safety of risankizumab versus ixekizumab in genital psoriasis has been evaluated.30
Outcome Measures
The results, as well as the methodology and the quality of the evidence, are represented in Table 1. In the included studies, there was some variation in the method of evaluating the outcomes.
Since there are many tools for measuring the quality of life of people with psoriasis and other skin disorders, studies that have used psoriasis-specific measures have been taken into account. These measures can be categorized as psoriasis-specific (Psoriasis Symptoms Scale [PSS];19,28 skin-specific (Dermatology Life Quality Index [DLQI];19–24,26–30 and generic quality of life measures (SF‐36),28 (EQ-5D-5L),19,28 Hospital Anxiety and Depression Scale (HADS),19,28 Work Productivity and Activity Impairment Questionnaire (WPAI),25 Patient Global Assessment of Disease Activity (PtGA),28 and Patient Benefit Index (PBI).28
Discussion
Through the analyzed studies, RZB has shown to achieve a very significant improvement in the quality of life of patients compared to other drugs analyzed, especially in those who have not previously received any biological treatment.22 Compared to UST, at week 16, 66.2% of patients achieved a DLQI 0/1 versus 44.7% with UST.19 In the IMMvent and LIMMitless studies, these improvements were shown to increase to 77% and 78% at weeks 57 and 172, respectively.24 Similar improvements were found when evaluating other scales related to quality of life, such as EQ-5D-5L or HADS.19
In addition, psoriasis-specific PROs (patient reported outcomes) such as PSS 0, indicating that there are no symptoms of psoriasis, is obtained in 30.3% of patients treated with RZB, compared to 15.1% with UST and 1% with PBO.19
When compared with fumaric acid esters (FAEs),28 the most frequently prescribed first-line systemic treatment in Germany, patients treated with RZB had a lower PSS score compared to those treated with AEDs, which translates into less redness, itching, and burning associated with psoriasis.
On the other hand, patients randomized to RZB showed significant improvements in SF-36, HADS, PtGA, and EQ-5D-5L (<0.002); the benefit of treatment was even assessed from the patient’s perspective based on the PBI questionnaire on the patient’s therapeutic needs and another on the benefit achieved by the treatment. In this last questionnaire, RZB presented a better score than the FAEs.28
In real clinical practice, similar results have been observed; Ruiz-Villaverde et al21 analyzed the effectiveness and safety of risankizumab in an observational and retrospective study, where they showed that the mean DLQI score at the start of treatment was 13.64 ± 4.80 and at week 16 the mean DLQI was less than 1, correlating with both improvements in PASI, BSA, and the visual analogue scale of pruritus.
Another very important piece of information is job productivity and the indirect costs associated with this disease. Lebwohl et al25 through the Work Productivity and Activity Impairment Questionnaire (WPAI). The total work productivity impairment (TWPI) in the RZB trials (N.2046), incremental TWPI relative to RZB was 3.4%/week for UST/ADA, and 17.1%/week for placebo; incremental indirect cost savings for risankizumab were $2179/year vs adalimumab, $2321/year vs ustekinumab, and $11,284/year vs placebo.
Due to the systemic and psychological implications of psoriasis, it is necessary to analyse various PROs, both psoriasis-specific and general, in a combined manner, relating them to efficacy data, which allows us to obtain a global vision of the patient’s situation. Thus, absolute PASI<1 and DLQI 0/1 were compared, showing adjusted differences of 22.1% [15.2, 29.1 (95% CI)] in patients treated with RZB versus those treated with UST at week 16, and 30.3% [23.1, 37.6 (95% CI)] at week 52.29 Similarly, the LiMMItless study showed that more than half of patients achieved both PASI 90 and DLQI 0/1 at 16 weeks of treatment (56.9%), and this percentage increased to 70% at week 172.24
Lebwohl et al23 in a Post Hoc Analysis of Four Phase 3 Clinical Trials (UltIMMa-1, UltIMMa-2, IMMvent, and IMMhance) agreed with the LiMMItless study; patients treated with risankizumab during the study period experienced the longest duration of DLQI 0/1: 215.7 days (59% over one year) followed by patients receiving adalimumab, adalimumab/risankizumab, 159.1 days (44% over one year) and ustekinumab, 144.3 days (40% over one year). The patients who received PBO/risankizumab maintained the DLQI 0/1 for less time, 90.5 days (25% over one year).
Even small differences in PASI can be significant when assessing the implications for patients’ quality of life. In a Czech cohort of patients with moderate-severe psoriasis treated with RZB at week 16, patients with a PASI 100 response achieved greater reductions in DLQI compared with those who achieved a PASI 90 response (15.9 points vs 11.8 p<0.033).27,34
In addition, the DLQI deteriorates more rapidly than the PASI when treatment is discontinued (49.7% versus 36.4%) based on predictive models.20
Regarding the RZB dose, the DLQI 0/1 response rate is very good with both RZB 75 mg and 150 mg, both being much higher than the placebo (62.1% and 58.2% versus 5.2%, respectively). However, when the placebo group of patients was re-randomized to receive risankizumab 75 mg and 150 mg, the DLQI 0/1 response rates increased from week 16 to week 52 to 66.7% and 81.5%, respectively.26
On the other hand, the impact of RZB on special areas, such as the genitals, has also been studied. Sotiriou et al30 compared the efficacy and safety of risankizumab vs ixekizumab in this area, demonstrating a reduction in DLQI from baseline to week 24 of 91.8% and 92.1%, respectively, obtaining similar rates for PGA-G, falling to 0.3 and 0.4, respectively.
Limitations
The lack of SCOPUS database search and practical limitations when assessing the risk of bias in non-randomized studies.
In conclusion, risankizumab has shown not only to have very relevant data on effectiveness and safety, but all of this is associated with an improvement in quality of life related to health and psychological well-being measured on generic and specific quality of life scales, both in pivotal trials, ad hoc analysis, and data in real clinical practice.
Funding
There are no sources of funding.
Disclosure
Tamara Gracia-Cazaña and Laura Bernal-Masferrer are co-first authors for this study. Dr Tamara Gracia-Cazaña provided advisory service for Abbvie. The authors report no other conflicts of interest in this work.
References
1. Goff KL, Karimkhani C, Boyers LN, et al. The global burden of psoriatic skin disease. Br J Dermatol. 2015;172(6):1665–1668. doi:10.1111/BJD.13715
2. Vanaclocha F, Crespo-Erchiga V, Jiménez-Puya R, et al. Immune-mediated inflammatory diseases and other comorbidities in patients with psoriasis: baseline characteristics of patients in the AQUILES study. Actas Dermosifiliogr. 2015;106(1):35–43. doi:10.1016/J.AD.2014.06.003
3. Hilhorst N, Deprez E, Pauwels N, Grine L, Lambert J, Hoorens I. Patient-relevant outcomes in psoriasis: a systematic review. JAMA Dermatol. 2022;158(7):806. doi:10.1001/JAMADERMATOL.2022.1756
4. Katugampola RP, Lewis VJ, Finlay AY. The dermatology life quality index: assessing the efficacy of biological therapies for psoriasis. Br J Dermatol. 2007;156(5):945–950. doi:10.1111/J.1365-2133.2007.07817.X
5. Chan TC, Hawkes JE, Krueger JG. Interleukin 23 in the skin: role in psoriasis pathogenesis and selective interleukin 23 blockade as treatment. Ther Adv Chronic Dis. 2018;9(5):111–119. doi:10.1177/2040622318759282
6. Ataseven A, Temiz SA, Eren G, Özer İ, Dursun R. Comparison of anti-TNF and IL-inhibitors treatments in patients with psoriasis in terms of response to routine laboratory parameter dynamics. J Dermatolog Treat. 2022;33(2):1091–1096. doi:10.1080/09546634.2020.1801975
7. Gerdes S, Körber A, Biermann M, Karnthaler C, Reinhardt M. Absolute and relative psoriasis area and severity index (PASI) treatment goals and their association with health-related quality of life. J Dermatolog Treat. 2020;31(5):470–475. doi:10.1080/09546634.2020.1746734
8. Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1–12. doi:10.1016/0197-2456(95)00134-4
9. Schulz KF, Altman DG, Moher D; CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. Int J Surg. 2011;9(8):672–677. doi:10.1016/j.ijsu.2011.09.004
10. López de Argumedo M, Reviriego E, Andrío E, et al. Revisión externa y validación de instrumentos metodológicos para la lectura crítica y la síntesis de la evidencia científica INFORMES, ESTUDIOS E INVESTIGACIÓN MINISTERIO DE SANIDAD Y CONSUMO.Servicio de Evaluación de Tecnologías Sani- tarias del País Vasco (Osteba) [External review and validation of methodological instruments for critical reading and synthesis of scientific evidence REPORTS, STUDIES AND RESEARCH MINISTRY OF HEALTH AND CONSUMPTION. Health Technology Assessment Service of the Basque Country (Osteba)]; Informes de Evaluación de Tecnologías Sanitarias: OSTEBA No 2006/02; 2006. Available from: http://www.euskadi.net/ejgvbiblioteka.
11. Sbidian E, Chaimani A, Afach S, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev. 2020;1(1). doi:10.1002/14651858.CD011535.PUB3
12. Lin PH, Tsai TF. Effects of risankizumab in patients with psoriasis previously treated with guselkumab: a case series. Eur J Dermatol. 2021;31(2):251–252. doi:10.1684/EJD.2021.4001
13. Al-Janabi A, Jabbar-Lopez ZK, Griffiths CEM, Yiu ZZN. Risankizumab vs. ustekinumab for plaque psoriasis: a critical appraisal. Br J Dermatol. 2019;180(6):1348–1351. doi:10.1111/BJD.17624
14. Warren RB, Blauvelt A, Poulin Y, et al. Efficacy and safety of risankizumab vs. secukinumab in patients with moderate-to-severe plaque psoriasis (IMMerge): results from a Phase III, randomized, open-label, efficacy-assessor-blinded clinical trial. Br J Dermatol. 2021;184(1):50–59. doi:10.1111/BJD.19341
15. van der Schoot LS, van den Reek JMPA, Grine L, et al. Dose reduction of the new generation biologics (IL-17 and IL-23 inhibitors) in psoriasis: study protocol for an international, pragmatic, multicenter, randomized, controlled, non-inferiority study-The BeNeBio study. Trials. 2021;22:1. doi:10.1186/S13063-021-05681-Z
16. Leonardi CL, See K, Burge R, et al. Number needed to treat network meta-analysis to compare biologic drugs for moderate-to-severe psoriasis. Adv Ther. 2022;39(5):2256–2269. doi:10.1007/S12325-022-02065-W
17. Singh S, Singh S, Thangaswamy A, Thangaraju P, Varthya SB. Efficacy and safety of Risankizumab in moderate to severe psoriasis: a systematic review and meta-analysis. Dermatol Ther. 2021;34:1. doi:10.1111/DTH.14487
18. Rentz AM, Skalicky AM, Esser D, et al. Reliability, validity, and the ability to detect change of the Psoriasis Symptom Scale (PSS) in patients with plaque psoriasis. J Dermatolog Treat. 2020;31(5):460–469. doi:10.1080/09546634.2019.1709612
19. Augustin M, Lambert J, Zema C, et al. Effect of Risankizumab on patient-reported outcomes in moderate to severe psoriasis: the UltIMMa-1 and UltIMMa-2 randomized clinical trials. JAMA Dermatol. 2020;156(12):1344–1353. doi:10.1001/JAMADERMATOL.2020.3617
20. Papp KA, Soliman AM, Done N, Carley C, Lemus Wirtz E, Puig L. Deterioration of health-related quality of life after withdrawal of Risankizumab treatment in patients with moderate-to-severe plaque psoriasis: a machine learning predictive model. Dermatol Ther (Heidelb). 2021;11(4):1291–1304. doi:10.1007/S13555-021-00550-8
21. Ruiz-Villaverde R, Ruiz-Carrascosa JC, Galán-Gutierrez M, Armario-Hita JC. Risankizumab: a pilot study of short-term effectiveness and safety in real clinical practice. Dermatol Ther. 2021;34(1). doi:10.1111/DTH.14711
22. Mastorino L, Castelli F, Stroppiana E, et al. Risankizumab shows faster response in bio naïve than in bio-experienced psoriatic patients. J Eur Acad Dermatol Venereol. 2022;36(10). doi:10.1111/JDV.18314
23. Lebwohl MG, Soliman AM, Yang H, et al. Impact of Risankizumab on PASI90 and DLQI0/1 duration in moderate-to-severe psoriasis: a post hoc analysis of four phase 3 clinical trials. Dermatol Ther. 2022;12(2):407–418. doi:10.1007/S13555-021-00660-3
24. Papp KA, Lebwohl MG, Puig L, et al. Long-term efficacy and safety of risankizumab for the treatment of moderate-to-severe plaque psoriasis: interim analysis of the LIMMitless open-label extension trial beyond 3 years of follow-up. Br J Dermatol. 2021;185(6):1135–1145. doi:10.1111/BJD.20595
25. Lebwohl M, Soliman AM, Yang H, Wang J, Freimark J, Puig L. Impact of PASI response on work productivity and the effect of risankizumab on indirect costs using machine learning in patients with moderate-to-severe psoriasis. J Dermatolog Treat. 2022;33(4):2094–2101. doi:10.1080/09546634.2021.1919287
26. Ohtsuki M, Fujita H, Watanabe M, et al. Efficacy and safety of risankizumab in Japanese patients with moderate to severe plaque psoriasis: results from the SustaIMM Phase 2/3 trial. J Dermatol. 2019;46(8):686–694. doi:10.1111/1346-8138.14941
27. Gkalpakiotis S, Cetkovska P, Arenberger P, et al. Risankizumab for the treatment of moderate-to-severe psoriasis: real-life multicenter experience from the Czech Republic. Dermatol Ther. 2021;11(4):1345–1355. doi:10.1007/S13555-021-00556-2
28. Thaçi D, Soliman AM, Eyerich K, et al. Patient-reported outcomes with risankizumab versus fumaric acid esters in systemic therapy-naïve patients with moderate to severe plaque psoriasis: a phase 3 clinical trial. J Eur Acad Dermatol Venereol. 2021;35(8):1686–1691. doi:10.1111/JDV.17109
29. Gooderham M, Pinter A, Ferris LK, et al. Long-term, durable, absolute psoriasis area and severity index and health-related quality of life improvements with risankizumab treatment: a post hoc integrated analysis of patients with moderate-to-severe plaque psoriasis. J Eur Acad Dermatol Venereol. 2022;36(6):855–865. doi:10.1111/JDV.18010
30. Sotiriou E, Bakirtzi K, Papadimitriou I, et al. A head-to-head comparison of risankizumab and ixekizumab for genital psoriasis: a real-life, 24-week, prospective study. J Eur Acad Dermatol Venereol. 2022;36(5):e359–e361. doi:10.1111/JDV.17880
31. Gordon KB, Strober B, Lebwohl M, et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled phase 3 trials. Lancet. 2018;392(10148):650–661. doi:10.1016/S0140-6736(18)31713-6
32. Blauvelt A, Leonardi CL, Gooderham M, et al. Efficacy and safety of continuous Risankizumab therapy vs treatment withdrawal in patients with moderate to severe plaque psoriasis: a phase 3 randomized clinical trial. JAMA Dermatol. 2020;156(6):649–658. doi:10.1001/JAMADERMATOL.2020.0723
33. Reich K, Gooderham M, Thaçi D, et al. Risankizumab compared with Adalimumab in patients with moderate-to-severe plaque psoriasis (IMMvent): a randomised, double-blind, active-comparator-controlled phase 3 trial. Lancet. 2019;394(10198):576–586. doi:10.1016/S0140-6736(19)30952-3
34. Armstrong AW, Villanueva Quintero DG, Echeverría CM, Gu Y, Karunaratne M, Reyes Servín O. Body region involvement and quality of life in psoriasis: analysis of a randomized controlled trial of Adalimumab. Am J Clin Dermatol. 2016;17(6):691–699. doi:10.1007/S40257-016-0229-X
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.