")
Back to Journals » Clinical Interventions in Aging » Volume 19
Risk Factors for Postoperative Cognitive Decline After Orthopedic Surgery in Elderly Chinese Patients: A Retrospective Cohort Study
Authors Li X , Lai H, Wang P, Feng S, Feng X , Kong C, Wu D, Yin C, Shen J, Yan S , Han R, Liu J, Ren X, Li Y, Tang L, Xue D, Zhao Y, Huang H, Li X, Zhang Y, Wang X, Wang C, Jin P, Lu S, Wang T, Zhao G, Wang C
Received 21 October 2023
Accepted for publication 25 February 2024
Published 19 March 2024 Volume 2024:19 Pages 491—502
DOI https://doi.org/10.2147/CIA.S436349
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Xian Li,1,* Hong Lai,2,* Peng Wang,3 Shuai Feng,4 Xuexin Feng,4 Chao Kong,3 Dewei Wu,5 Chunlin Yin,5 Jianghua Shen,6 Suying Yan,6 Rui Han,7 Jia Liu,7 Xiaoyi Ren,8 Ying Li,8 Lu Tang,9 Dong Xue,9 Ying Zhao,9 Hao Huang,10 Xiaoying Li,10 Yanhong Zhang,10 Xue Wang,11 Chunxiu Wang,12 Ping Jin,13 Shibao Lu,3 Tianlong Wang,4 Guoguang Zhao,14 Chaodong Wang1 On behalf of the APPLE-MDT Research Team, Xuanwu Hospital, Capital Medical University and National Clinical Research Center for Geriatric Diseases
1Department of Neurology & Neurobiology, Xuanwu Hospital, Capital Medical University, National Clinical Research Center for Geriatric Diseases, Beijing, 100053, People’s Republic of China; 2Department of Neurology, The First Affiliated Hospital of Gannan Medical University, Ganzhou, 341000, People’s Republic of China; 3Department of Orthopedic Surgery, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 4Department of Anesthesiology, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 5Department of Cardiology, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 6Department of Pharmacy, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 7Department of Gerontology, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 8Department of Nutrition, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 9Department of Oral Medicine, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 10Department of Medical Administration, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 11Department of Medical Library, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 12Center for Evidence-Based Medicine, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 13Center for Medical Information, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 14Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, National Clinical Research Center for Geriatric Diseases, Beijing, 100053, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chaodong Wang, Department of Neurology, Xuanwu Hospital of Capital Medical University, National Clinical Research Center for Geriatric Diseases, No. 45 Changchun Street, Beijing, 100053, People’s Republic of China, Tel/Fax +86-10-8319-8677, Email [email protected]
Purpose: We aimed to identify the risk factors for postoperative cognitive decline (POCD) by evaluating the outcomes from preoperative comprehensive geriatric assessment (CGA) and intraoperative anesthetic interventions.
Patients and Methods: Data used in the study were obtained from the Aged Patient Perioperative Longitudinal Evaluation–Multidisciplinary Trial (APPLE-MDT) cohort recruited from the Department of Orthopedics in Xuanwu Hospital, Capital Medical University between March, 2019 and June, 2022. All patients accepted preoperative CGA by the multidisciplinary team using 13 common scales across 15 domains reflecting the multi-organ functions. The variables included demographic data, scales in CGA, comorbidities, laboratory tests and intraoperative anesthetic data. Cognitive function was assessed by Montreal Cognitive Assessment scale within 48 hours after admission and after surgery. Dropping of ≥ 1 point between the preoperative and postoperative scale was defined as POCD.
Results: We enrolled 119 patients. The median age was 80.00 years [IQR, 77.00, 82.00] and 68 patients (57.1%) were female. Forty-two patients (35.3%) developed POCD. Three cognitive domains including calculation (P = 0.046), recall (P = 0.047) and attention (P = 0.007) were significantly worsened after surgery. Univariate analysis showed that disability of instrumental activity of daily living, incidence rate of postoperative respiratory failure (PRF) ≥ 4.2%, STOP-Bang scale score, Caprini risk scale score and Sufentanil for maintenance of anesthesia were different between the POCD and non-POCD patients. In the multivariable logistic regression analysis, PRF ≥ 4.2% (odds ratio [OR] = 2.343; 95% confidence interval [CI]: 1.028– 5.551; P = 0.046) and Sufentanil for maintenance of anesthesia (OR = 0.260; 95% CI: 0.057– 0.859; P = 0.044) was independently associated with POCD as risk and protective factors, respectively.
Conclusion: Our study suggests that POCD is frequent among older patients undergoing elective orthopedic surgery, in which decline of calculation, recall and attention was predominant. Preoperative comprehensive geriatric assessments are important to identify the high-risk individuals of POCD.
Keywords: cognitive dysfunction, postoperative cognitive complications, orthopedic surgery, comprehensive geriatric assessment, risk factors
Introduction
As the population ages, surgery is being performed frequently in older patients, which was accompanied by high frequency of complications. Postoperative cognitive dysfunction (POCD), a common postoperative complication, is defined as an objective cognitive decline after surgery.1 Studies have shown that 26% of patients over the age of 65 years had POCD within a few weeks of non-cardiac surgeries.2 Moreover, previous studies demonstrated that patients with POCD experienced a much higher risk for new disability after surgery, such as impairment of independence in activities of daily living.3 Due to the increasing incidence of POCD, it is important to identify the risk factors and interventions for POCD. In contrast to POCD, postoperative delirium (POD) occurs in the first few days following surgery which develops no earlier than the end of the first postoperative week. However, POD is considered a strong predictor of POCD development and a harbinger of POCD which has far more significant repercussions on patient health and the healthcare system.4
The pathogenesis of POCD is complex and remains poorly understood. Glumac et al reported that preoperative administration of corticosteroids ameliorates the inflammatory response induced by surgery and, thereby, reduce the incidence and severity of POCD, suggesting that inflammatory response has a key role in POCD development.5 In addition, embolism,6 hypoperfusion7 and other factors during the surgery have also been proposed as the potential mechanisms for POCD.
Previous studies have suggested the patient-, operation- anesthesia-specific risk factors. The patient-specific factors include age, educational level, preoperative mental health and chronic pain.8–10 The operation- and anesthesia-specific factors include duration and complexity of surgery, duration of anesthesia and anesthetic drugs used.8,11 Although all the studies focused on elderly over 65 years old, the features in even older (≥75 years) patients, who may have more frequent and severe complications, have not been delineated. Moreover, although comprehensive geriatric assessment (CGA) was advocated increasingly for elderly,12 it has not been specifically applied to screen risk factors for POCD.
The Aged Patient Perioperative Longitudinal Evaluation–Multidisciplinary Trial (APPLE-MDT) cohort recruited the elderly patients over 75 years undergoing elective orthopedic surgery. All enrolled patients accepted CGA before and after surgery, and the cognitive status was assessed using the Montreal Cognitive Assessment (MoCA) scale, which was sensitive and specific to screen cognitive impairment.13 We hypothesized that preoperative CGA is likely to have a positive impact on identifying the risk factors for POCD in older patients to improve decision-making for the elective surgery and plan for perioperative interventions.
Materials and Methods
The Establishment of the APPLE-MDT Cohort
The protocol of the APPLE-MDT study has been published previously.14 In brief, this study is a single-center, parallel and randomized study developed to: (1) evaluate the comprehensive risk for surgery based on preoperative multidisciplinary assessments; (2) assist doctors and patients in decision-making for orthopedic surgery with general anesthesia; and (3) formulate managements and interventions to these risk factors. Upon understanding the assessment results and the informed consent, the patients were scheduled for elective orthopedic surgery. Patients were recruited from Department of Orthopedics in Xuanwu hospital, Capital Medical University between March, 2019 and June, 2022. This study was approved by the ethics review board of Xuanwu Hospital of Capital Medical University (2018–086) and registered in Chinese Clinical Trial Registry (ChiCTR1800020363). All patients accepted CGA by multidisciplinary specialists including orthopedists, anesthetists, neurologists, geriatricians, nutritionists, pharmacists and nurses within 48 hours of admission and 48 hours after surgery.
Perioperative CGA Assessment
Data used in this study were obtained from the APPLE-MDT study, and patients with complete data including CGA evaluation, intraoperative data and postoperative MoCA assessment were enrolled. Variables with missing values ≥20% were not included in the study. Definitions of relevant variables were shown in Supplementary Table 1. Briefly, basic personal demographics, comorbidities and laboratory tests were collected from electronic medical record (EMR) which was recorded by orthopedic residents. Preoperative CGA used 13 common scales to assess their state of health across 15 domains covering blood pressure, fasting glucose, fall risk, pain, daily activities, frailty, nutritional status, risk for postoperative respiratory failure (PRF), obstructive sleep apnea (OSA), thrombosis, risk for stroke, scales for anxiety and depression, and the American Society of Anesthesiologists class (ASA) and medications (Supplementary Table 1).
Intraoperative Surgery and Anesthesia
Intraoperative surgical and anesthetic data were collected from the electronic surgical and anesthesia records for the orthopedic operation. All patients underwent spinal fusion surgery with general anesthesia. Spinal localization included cervical, lumbar, cervical and lumbar, and thoracolumbar vertebra. All included patients were prepared for routing general anesthesia by inserting an intravenous line, and electrocardiogram, noninvasive blood pressure, pulse oximetry, and PET CO2 were monitored. Following consideration of perioperative risks, the anesthetist group will implement individualized anesthesia schemes for each patient including full sedation, analgesia, antistress management, accurate monitoring indicator management, objectives-oriented liquid management, and circulation ventilation management, as appropriate. Drugs used in surgery are listed in Supplementary Table 1.
Cognitive Assessment and Definition of POCD
Patients with history of dementia (diagnosed in medical records) who were unable to cooperate with the evaluation were excluded from APPLE-MDT cohort. Pre- and postoperative cognitive assessments were conducted using the MoCA scale by the neurologists. MoCA is a highly sensitive and specific brief cognitive screening tool for detecting cognitive impairment, and < 24 points was defined as cognitive impairment. It evaluates orientation to time and place, executive functions, calculation, naming, repetition, visuospatial function short-term and delayed recall and attention.15 For correcting the education effects, one point was added for participants with 12 years of education or less on their total MoCA scores (if <30). Drop of ≥1 point between preoperative and postoperative MoCA assessments was defined as the POCD.
Statistical Analysis
The distribution normality of numerical variables was assessed with the two-tailed Shapiro–Wilk and Lilliefors tests. For univariate analysis, we used Mann–Whitney U-test for non-normal distributions (data reported as median [interquartile range, IQR]) or the independent samples t-test for normally distributed continuous variables (data reported as mean ± standard deviation [SD]), and Chi-Square test for categorical variables (reported as count[%]) to compare differences between POCD and non-POCD groups. For all statistical tests, we chose 0.05 as the significance level. A multivariable logistic regression model was established to screen independent risk factors for predicting POCD. Variables with significant differences in the univariate analysis and risk factors identified in previous studies were included in the stepwise logistic regression analysis model by both forward and backward steps. The algorithm can both add and remove variables in an iterative manner based on the Akaike Information Criterion (AIC). We did not calculate the sample size, but we referred to previous literature9,16–18 in which sample sizes ranged from 60 to 130, close to our sample size. All analyses were performed using R statistical software version 4.1.1 (R Project for Statistical Computing).
Results
Characteristics of Patients and POCD
We enrolled 119 patients with complete data, including preoperative baseline information and multidisciplinary assessments for surgery and anesthesia and postoperative MoCA score. The characteristics of patients were shown in Table 1. Of these patients, the median age was 80.00 [IQR, 77.00, 82.00] years, 68 (57.1%) were female, and 90 (75.6%) had junior middle school education or above. The highest prevalent comorbidity was hypertension (64.7%), followed by diabetes (27.7%), ischemic heart diseases (23.5%) and anemia (20.2%). Patients with history of anesthesia accounted for 79.8%, and 46.2% patients had general anesthesia before. No significant differences in demographic information, comorbidities and laboratory testing results were observed between patients with POCD and without POCD (Table 1 and Supplementary Table 2).
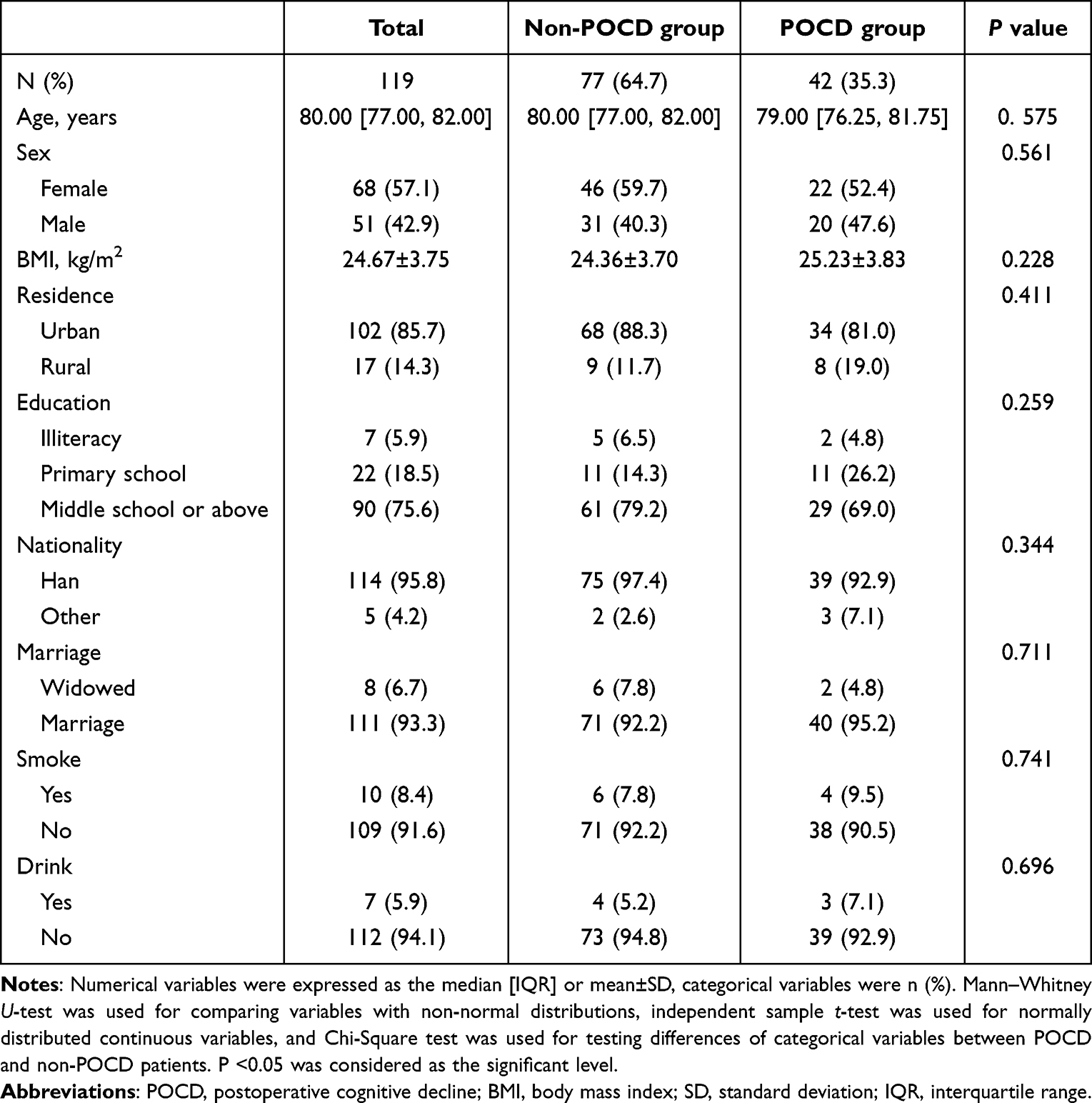 |
Table 1 Demographic of Patients with or Without POCD |
Two days after surgery, we found MoCA scores declined in 42 (35.3%) patients and about half (n = 20, 47.6%) declined 1 point (Figure 1A). In the eight cognitive domains of MoCA scale, three cognitive domains including calculation (P = 0.046), recall (P = 0.047) and attention (P = 0.007) were significantly decreased after surgery (Figure 1B).
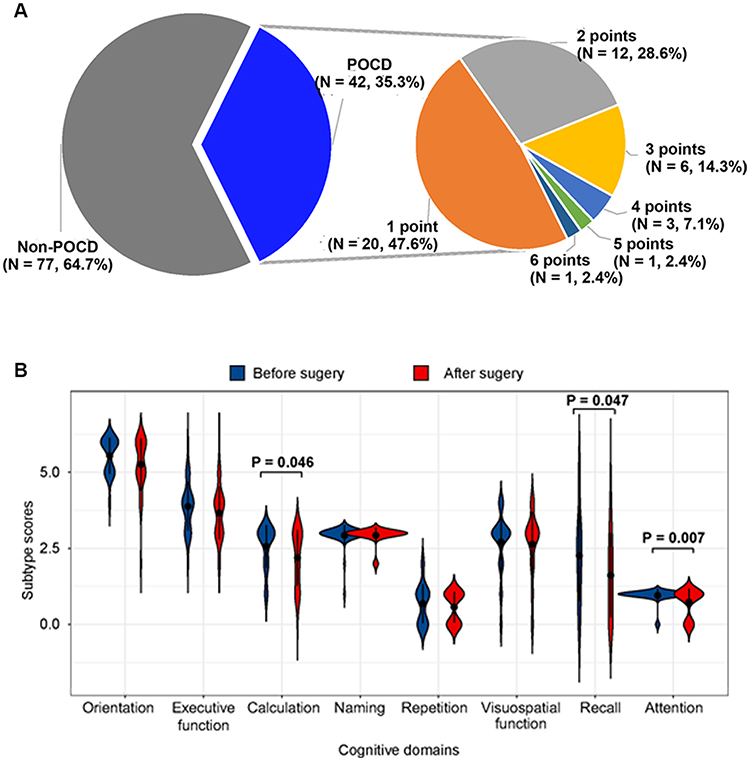 |
Figure 1 Description of POCD in our cohort. (A) Description of POCD in this study. Left pie described the ratio of POCD among all patients (n=119), and right pie described ratio of decreased MoCA points after surgery among POCD group (n=42). (B) Comparison of eight cognitive domains before (blue) and after (red) surgery among POCD group (n=42). Black dots and lines inside violin were mean and standard deviation. Abbreviations: POCD, postoperative cognitive decline. |
Preoperative CGA and POCD
In the preoperative CGAs, we found a significant difference in the assessments of Instrumental Activity of Daily Living (IADL), risk for PRF, OSA and thrombosis between patients with and without POCD (Table 2). Compared to patients without POCD, those with POCD had higher proportion of disability for IADL before surgery (88.1% vs 70.1%; P = 0.048), although the score of IADL scale showed no significant differences between these cases. Moreover, patients with POCD had higher score of PRF risk scale (23.00 points; IQR, 16.00–23.00) than those without (16.00 points; IQR, 16.00–23.00; P = 0.049), and had increased proportion for PRF > 4.2% (P = 0.033). Furthermore, the median score of STOP-Bang scale was 3.00 points [IQR, 2.00–4.00] in patients with POCD which was higher than those without POCD (2.00 points; IQR, 2.00–3.00; P = 0.026). Although there was no statistical difference, the proportion of high-risk for OSA was higher in POCD patients than non-POCD cases (59.5% vs 44.2%). All patients in the two groups had very high risk for thrombosis, however, patients with POCD had higher score of Caprini risk scale than those without POCD (P = 0.018). Although there was no statistical difference, the proportion of patients with preoperative blood pressure exceeding the surgical criteria was higher in POCD patients than the non-POCD ones (35.7% vs 18.2%, P = 0.057).
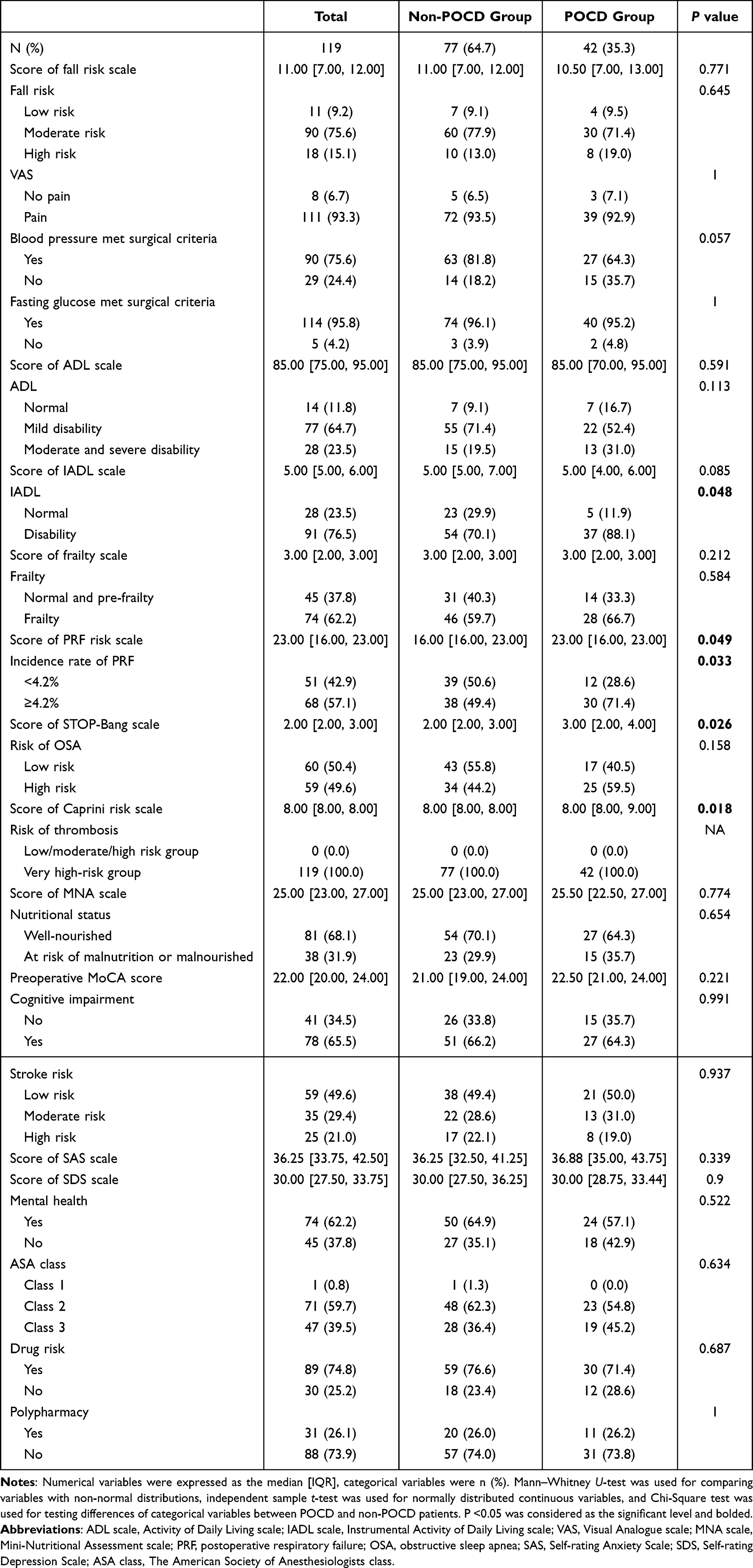 |
Table 2 Preoperative Comprehensive Geriatric Assessments Results of Patients with or Without Cognitive Decline |
Surgical and Anesthetic Variables Associated with POCD
No significant difference in surgical information was observed between the two groups (Table 3). As for anaesthetic delivery, we found only 7.1% patients in POCD group used Sufentanil for maintenance of anesthesia, which was significantly less than the 24.7% of non-POCD group (P = 0.025). Moreover, none of the patients with POCD used Urapidil during surgery, while 9.1% of non-POCD patients used it (P = 0.051).
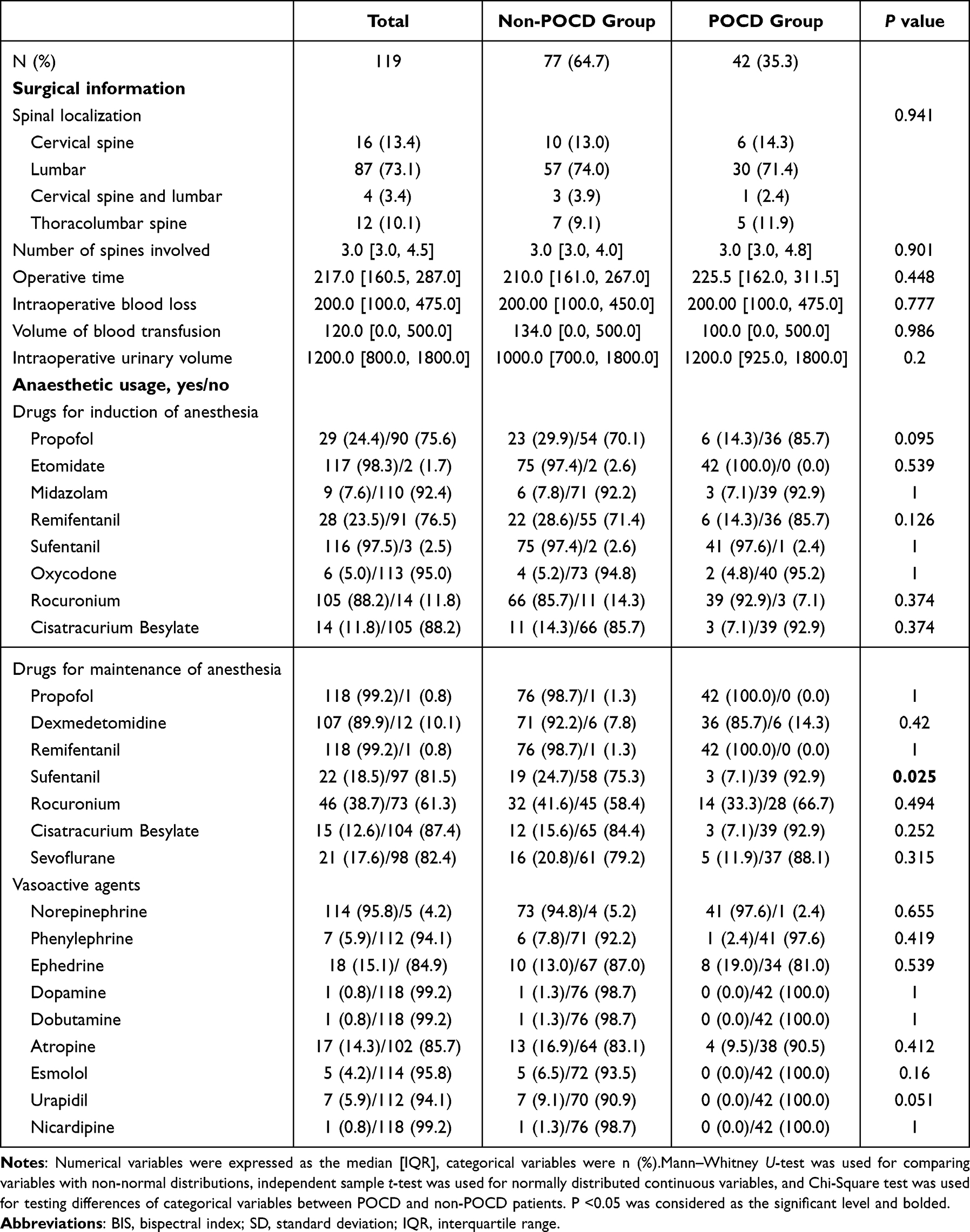 |
Table 3 Surgery and Intraoperative Anesthesia of Patients with or Without Cognitive Decline |
Multivariable Logistic Regression Analysis
A multivariable logistic regression model was constructed for predicting POCD using age, education, mental health, preoperative cognitive impairment, IADL, incidence rate of PRF, Sufentanil for maintenance of anesthesia and risk for OSA and thrombosis as the covariables. As shown in Table 4, after both selection processes, age, education, mental health, preoperative cognitive impairment and risk for OSA and thrombosis were removed from the model. The incidence rate of PRF ≥4.2% was revealed to be independently associated with the POCD (odd ratio [OR] = 2.343; 95% confidence interval [CI]: 1.028–5.551; P = 0.046). In contrast, usage of Sufentanil for maintenance of anesthesia (OR = 0.260; 95% CI: 0.057–0.859; P = 0.044) was identified as a protective factor for POCD.
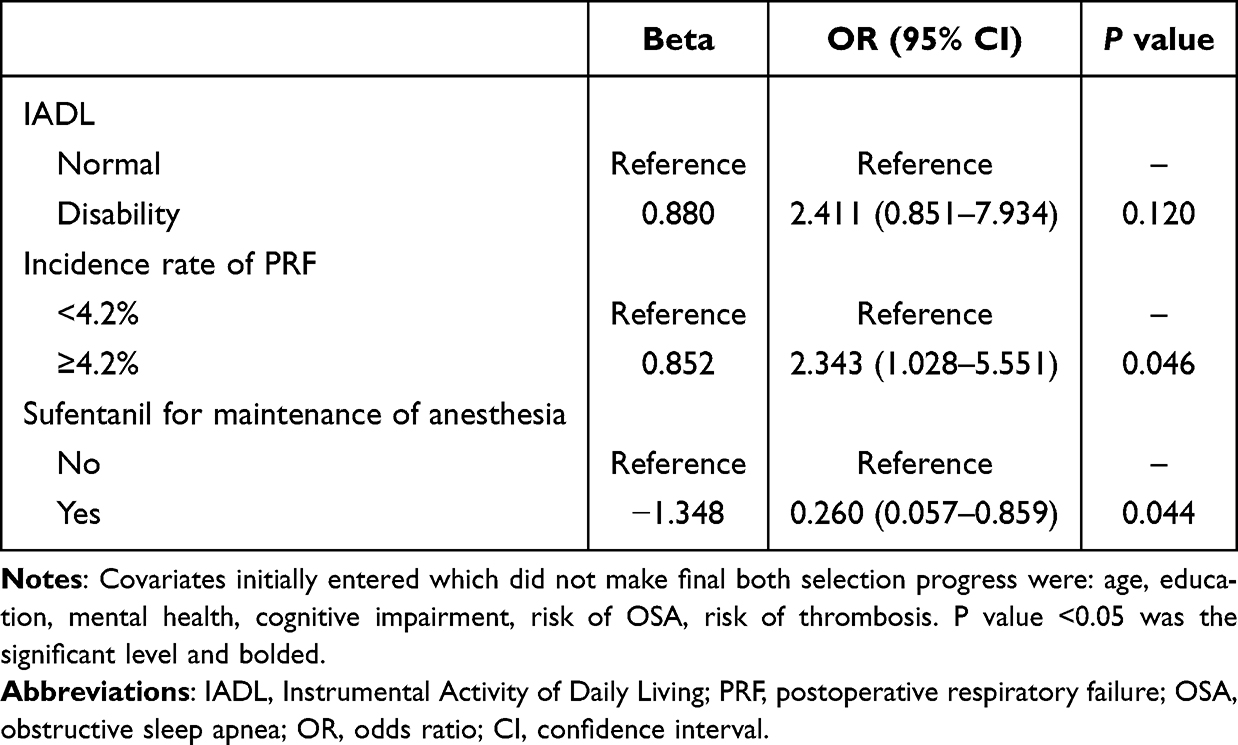 |
Table 4 Multivariable Logistic Regression Analysis for POCD |
Discussion
In our study, we found that 35.3% of the super-elderly patients (over 75 years old) receiving orthopedic surgeries had POCD, which mainly influenced the ability of recall, calculation and attention. The results also demonstrated that the preoperative risk for PRF ≥4.2% was an independent risk factor and Sufentanil for maintenance of anesthesia was a protective factor for POCD. Unlike most previous studies, we focused on patients over 75 years old who accepted the management by the same orthopedic and anesthesia team and reduced the heterogeneity in the study.
The advantage of this study is that all patients enrolled accepted preoperative CGAs by multidisciplinary specialists. Prior study which used the same APPLE-MDT cohort demonstrated that the CGAs process reduced mortality and increases safety in older orthopedic surgery patients.19 However, it did not uncover whether CGAs process can estimate the risk of cognitive decline after orthopedic surgery in older patients. In this study, we first explored the relationship between preoperative CGAs and POCD. We showed that preoperative estimated incidence rate of PRF ≥4.2% increased the risk of POCD by 2.3 times. PRF is the most serious postoperative pulmonary complications, which is usually evaluated in all types of surgeries (including aortic aneurysm repair and surgeries for thoracic, neurological, abdominal, vascular and neck), albumin < 30 g/L, blood urea nitrogen <30 mg/dL, dependent functional status, chronic obstructive pulmonary disease (COPD) and age.20 This index reflects dysfunctions in nutrition status, perioperative fluid management, activity and pulmonary function, which are likely to be associated with POCD. Surgical stress and anesthesia lead to changes in respiratory physiology, altering lung volumes, respiratory drive and muscle function.21 Patients with high PRF risk may suffer from hypoxemia that commonly develops after general anesthesia and can be aggravated by factors such as hypoventilation due to the residual effects of anesthetics, lung edema, laryngospasm and bronchospasm.22 Previous studies found that lower PCO2 was associated with better cognitive performance on measures of executive functioning and attention and verbal memory, whereas higher PO2 values were associated with better performance on the executive functioning and attention measure.23 Thus, postoperative recall and attention dysfunction may be caused by intraoperative hypoxemia, and risks for POCD can be reduced by correcting the preoperative risk factors and intraoperative preventive strategies for PRF.
The anesthetics have an important influence on postoperative cognitive function. Sufentanil is agonists of opioid receptors with a strong analgesic effect.24 Although opioid analgesics have been shown to be risk factors for cognitive decline, we found that Sufentanil for maintenance of anesthesia reduced the incidence of POCD. It may have beneficial roles in recovery and analgesic effect. Compared with patients used fentanyl, the MoCA scores were significantly higher and the incidence of POCD was significantly lower among patients used Sufentanil at 1-day post-surgery.25 The effects of remifentanil and Sufentanil were controversial. A study revealed that patients receiving Sufentanil have reduced analgesic requirements and better cognitive function postoperatively than those who received remifentanil.26 On the other hand, there was also a study showed that propofol-remifentanil resulted earlier cognitive recovery than Propofol-Sufentanil in patients undergoing supratentorial craniotomy.27 However, another study found no difference in POCD between Sufentanil and remifentanil.28 These controversial results may be caused by heterogeneity of each study such as type of surgery, definition of POCD and time of postoperative cognitive assessment. Our finding suggested the protective roles of Sufentanil in POCD, but, due to the relatively small sample size, it is necessary to be verified in random clinical trials.
Other possible risk factors of POCD we found in the univariate analysis included disability of IADL, risk for OSA and thrombosis. Patients with orthopedic disorders had poor IADL because of pain or disability. Previous study demonstrated that poor IADL was associated with postoperative delirium29 and higher risk of cardiac and respiration complications.19 Although not reaching the statistical significance, the relationship between preoperative poor IADL and POCD is still worth investigating. Prevalence of OSA was progressively increased with age, which occurs in ≥20% of people over 60 years old.30 Our study focused on patients over 75 years old and 49.6% of them had high risk for moderate to severe OSA. Furthermore, previous studies found that untreated OSA often leads to decline of cognitive functions including attention, working memory, episodic memory and executive functions, or even leads to permanent brain damage.31 The possible contribution of thrombosis to POCD was also found in this study. Since the incidence of thrombosis increases greatly with age, patients with high risk of thrombosis may exist immobility, malignant disease, comorbidities and increased levels of coagulation factors, it is highly possible that POCD could be caused by thrombosis.32
The association between cognitive reserve and POCD has been widely reported. We included education level as an indicator of cognitive reserve in multivariable logistic regression, although it had no association with POCD in univariate analysis. However, we did not find the association between education levels and POCD (p=0.259), as shown in Table 1. However, we did not find the association between education levels and POCD (p=0.259, Table 1). The explanations for the lack of such association might be multifold. One might be related to the relatively small sample size we analyzed. Although the rate of patients in POCD group had more primary school education, the difference did not reach statistical significance. The second might be that we did not specifically analyze the difference between POCD and non-POCD patients with high school and higher education, which was reported to affect the risk for POCD.33 Further studies are warranted using expanded sample sizes and focusing on patients with higher education level.
There are some limitations in our study. Our sample size was relatively small and we only detected factors associated with POCD within 48 hours after surgery, which may not reflect the dynamic cognitive changes within the whole postoperative period. Moreover, although our patients underwent unified general anesthesia, the anesthetist implement individualized anesthesia schemes for each patient according to the results of preoperative CGA and other factors. Thus, cautions must be taken for using these results in clinical practice. With increased sample size and prolonged follow-up of the patients in the APPLE-MDT cohort, the outcomes will be validated for preventing and targeted interventions for POCD in the advanced elderly patients.
Conclusion
In conclusion, our findings showed that 35.3% of patients over 75 years undergoing elective orthopedic surgery aggravate early cognitive function after surgery, mainly including calculation, recall and attention. Preoperative risk of PRF ≥4.2% increases the POCD, while Sufentanil for maintenance of anesthesia protects patients from POCD.
Abbreviations
POCD, postoperative cognitive dysfunction; CGA, comprehensive geriatric assessment; APPLE-MDT, The Aged Patient Perioperative Longitudinal Evaluation-Multidisciplinary Trial; MoCA, Montreal Cognitive Assessment scale; EMR, electronic medical record; PRF, postoperative respiratory failure; OSA, obstructive sleep apnea; ASA, the American Society of Anesthesiologists class; IQR, interquartile range; SD, standard deviation; IADL, Instrumental Activity of Daily Living; OR, odd ratio; CI, confidence interval; COPD, chronic obstructive pulmonary disease.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the ethics review board of Xuanwu Hospital of Capital Medical University (2018–086) and registered in Chinese Clinical Trial Registry (ChiCTR1800020363). All participants provided written informed consent. All methods were carried out in accordance with relevant guidelines and regulations complied with the Helsinki declaration.
Acknowledgments
All members of the APPLE-MDT Research Team included Ping Jin, Chunxiu Wang, Yingmei Deng, Hao Huang, Jing Li, Jia Liu, Rui Han, Suying Yan, Jianghua Shen, Ying Li, Xiaoyi Ren, Hongjuan Qian, Chunlin Yin, Jing Tan, Dewei Wu, Jun Yu, Yanyan Chu, Ying Zhao, Lu Tang, Dong Xue, Meng Wang, Chunsong Jia, Lianrui Guo, Xixiang Gao, Liqiang Li, Wujian Liu, Qi Sun, Shikun Du, Xue Wang, Guoguang Zhao. All of them were from Xuanwu Hospital including department of Anesthesiology, Nutrition, Pharmacy, Cardiology, and Pulmonology for collaboration in MDT assessments. We thank Tang L, Xue D, Zhao Y for their expertise and guidance, Wang X and Wang C for their assistance in literature review and statistical analyses, and Jin P for assistance for the construction and maintenance of the electronic evaluation system. We also thank all the participants and their guardians.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Beijing Municipal Medical Science Institute Public Welfare Development Reform Pilot Project (Capital Medical Research No. 2019–2) to Prof. Guoguang Zhao; grants from the National Natural Science Foundation of China (NSFC) (82171412) to Prof. Chaodong Wang and National Key Research and Development Program of China (No.2020YFC2004900) to Prof. Shibao Lu.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Evered LA, Silbert BS. Postoperative cognitive dysfunction and noncardiac surgery. Anesthesia Analg. 2018;127(2):496–505. doi:10.1213/ANE.0000000000003514
2. Kotekar N, Shenkar A, Nagaraj R. Postoperative cognitive dysfunction - current preventive strategies. Clin Interventions Aging. 2018;13:2267–2273. doi:10.2147/CIA.S133896
3. Deiner S, Liu X, Lin HM, et al. Does postoperative cognitive decline result in new disability after surgery? Ann Surg. 2021;274(6):e1108–e1114. doi:10.1097/SLA.0000000000003764
4. Glumac S, Kardum G, Karanovic N. Postoperative cognitive decline after Cardiac Surgery: a narrative review of current knowledge in 2019. Int J Exp Clin Res. 2019;25:3262–3270 doi:10.12659/MSM.914435
5. Glumac S, Kardum G, Sodic L, Supe-Domic D, Karanovic N. Effects of dexamethasone on early cognitive decline after cardiac surgery: a randomised controlled trial. Eur J Anaesthesiol. 2017;34(11):776–784. doi:10.1097/EJA.0000000000000647
6. Sulek CA, Davies LK, Enneking FK, Gearen PA, Lobato EB. Cerebral microembolism diagnosed by transcranial Doppler during total knee arthroplasty: correlation with transesophageal echocardiography. Anesthesiology. 1999;91(3):672–676. doi:10.1097/00000542-199909000-00018
7. Zhu J, Wang W, Shi H. The association between postoperative cognitive dysfunction and cerebral oximetry during geriatric Orthopedic Surgery: a randomized controlled study. Biomed Res Int. 2021;2021:5733139. doi:10.1155/2021/5733139
8. Moller JT, Cluitmans P, Rasmussen LS, et al. Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study. Lancet. 1998;351(9106):857–861. doi:10.1016/S0140-6736(97)07382-0
9. Ren S, Yuan F, Yuan S, Zang C, Zhang Y, Lang B. Early cognitive dysfunction in elderly patients after total knee arthroplasty: an analysis of risk factors and cognitive functional levels. Biomed Res Int. 2022;2022:5372603. doi:10.1155/2022/5372603
10. Huai X, Jiao Y, Gu X, et al. Preoperative chronic pain as a risk factor for early postoperative cognitive dysfunction in elderly patients undergoing hip joint replacement surgery: a prospective observational cohort study. Front Neurosci. 2021;15:747362. doi:10.3389/fnins.2021.747362
11. Li WX, Luo RY, Chen C, et al. Effects of propofol, dexmedetomidine, and midazolam on postoperative cognitive dysfunction in elderly patients: a randomized controlled preliminary trial. Chinese Med J. 2019;132(4):437–445. doi:10.1097/CM9.0000000000000098
12. Eamer G, Taheri A, Chen SS, et al. Comprehensive geriatric assessment for older people admitted to a surgical service. Cochrane Database Syst Rev. 2018;1(1):Cd012485 doi:10.1002/14651858.CD012485.pub2.
13. Jia X, Wang Z, Huang F, et al. A comparison of the mini-mental state examination (MMSE) with the Montreal cognitive assessment (MoCA) for mild cognitive impairment screening in Chinese middle-aged and older population: a cross-sectional study. BMC Psychiatry. 2021;21(1):485. doi:10.1186/s12888-021-03495-6
14. Zhang Y, Ma L, Wang T, et al. Protocol for evaluation of perioperative risk in patients aged over 75 years: aged patient perioperative longitudinal evaluation-multidisciplinary trial (APPLE-MDT study). BMC Geriatr. 2021;21(1):14. doi:10.1186/s12877-020-01956-3
15. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
16. Wu WQ, Zheng WB, Wang HB, Han JH, Huang Y, Wang CY. Influence of obstructive sleep apnea on postoperative cognitive dysfunction in elderly patients undergoing joint replacement. Am J Transl Res. 2022;14(6):4050–4057.
17. Oyeyemi DM, Cooter M, Chung S, et al. Relationship between depression/anxiety and cognitive function before and 6 weeks after major non-Cardiac Surgery in older adults. J Geriatric Psychiatry Neurol. 2022;35(1):145–154. doi:10.1177/0891988720978791
18. Cartailler J, Loyer C, Vanderlynden E, et al. Determinants of post-operative cognitive decline in elderly people. J Prev Alzheimers Dis. 2021;8(3):322–328. doi:10.14283/jpad.2021.13
19. Kong C, Zhang Y, Wang C, et al. Comprehensive geriatric assessment for older orthopedic patients and analysis of risk factors for postoperative complications. BMC Geriatr. 2022;22(1):644. doi:10.1186/s12877-022-03328-5
20. Arozullah AM, Daley J, Henderson WG, Khuri SF. Multifactorial risk index for predicting postoperative respiratory failure in men after major noncardiac surgery the national veterans administration surgical quality improvement program. Ann Surg. 2000;232(2):242–253. doi:10.1097/00000658-200008000-00015
21. Sameed M, Choi H, Auron M, Mireles-Cabodevila E. Preoperative pulmonary risk assessment. Respiratory Care. 2021;66(7):1150–1166. doi:10.4187/respcare.09154
22. Canet J, Gallart L. Postoperative respiratory failure. Curr Opin Crit Care. 2014;20(1):56–62. doi:10.1097/MCC.0000000000000045
23. Parekh PI, Blumenthal JA, Babyak MA, et al. Gas exchange and exercise capacity affect neurocognitive performance in patients with lung disease. Psychosomatic Med. 2005;67(3):425–432. doi:10.1097/01.psy.0000160479.99765.18
24. Scholz J, Steinfath M, Schulz M. Clinical pharmacokinetics of alfentanil, fentanyl and sufentanil. An Update Clin Pharmacokinet. 1996;31(4):275–292. doi:10.2165/00003088-199631040-00004
25. Zhang J, Chen L, Sun Y, He W. Comparative effects of fentanyl versus sufentanil on cerebral oxygen saturation and postoperative cognitive function in elderly patients undergoing open surgery. Aging Clin Exp Res. 2019;31(12):1791–1800. doi:10.1007/s40520-019-01123-8
26. Martorano PP, Aloj F, Baietta S, et al. Sufentanil-propofol vs remifentanil-propofol during total intravenous anesthesia for neurosurgery. A multicentre study. Minerva Anestesiol. 2008;74(6):233–243.
27. Bilotta F, Caramia R, Paoloni FP, et al. Early postoperative cognitive recovery after remifentanil-propofol or sufentanil-propofol anaesthesia for supratentorial craniotomy: a randomized trial. Eur J Anaesthesiol. 2007;24(2):122–127. doi:10.1017/S0265021506001244
28. Rasmussen LA, Ryhammer PK, Greisen J, Bhavsar RR, Lorentzen AG, Jakobsen CJ. Ultrashort acting remifentanil is not superior to long-acting sufentanil in preserving cognitive function-A randomized study. J Clin Anesth. 2016;33:127–134. doi:10.1016/j.jclinane.2016.03.023
29. Dogrul RT, Dogrul AB, Konan A, et al. Does preoperative comprehensive geriatric assessment and frailty predict postoperative complications? World J Surg. 2020;44(11):3729–3736. doi:10.1007/s00268-020-05715-8
30. Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):136–143. doi:10.1513/pats.200709-155MG
31. Vanek J, Prasko J, Genzor S, et al. Obstructive sleep apnea, depression and cognitive impairment. Sleep Med. 2020;72:50–58. doi:10.1016/j.sleep.2020.03.017
32. Engbers MJ, van Hylckama Vlieg A, Rosendaal FR. Venous thrombosis in the elderly: incidence, risk factors and risk groups. J Thromb Haemost. 2010;8(10):2105–2112. doi:10.1111/j.1538-7836.2010.03986.x
33. Feinkohl I, Winterer G, Spies CD, Pischon T. Cognitive reserve and the risk of postoperative cognitive dysfunction. Dtsch Arztebl Int. 2017. doi:10.3238/arztebl.2017.0110
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.