")
Back to Journals » Vascular Health and Risk Management » Volume 20
Sildenafil Use and Cigarette Smoking Associated with Intracerebral Hemorrhage: A Rare Case Report
Authors Hassan MA , Mohamed IA , Omar AA , Adan ZM , Garba B, Badawi OH
Received 17 October 2023
Accepted for publication 5 January 2024
Published 9 January 2024 Volume 2024:20 Pages 21—26
DOI https://doi.org/10.2147/VHRM.S443995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Mohamed Abdulahi Hassan,1,2 Ibrahim Abdullahi Mohamed,1 Abdullahi Abdirahman Omar,1 Zakaria Mohamed Adan,1 Bashiru Garba,3 Omar Hassan Badawi4
1Department of Internal Medicine and Intensive Care Unit, Dr. Sumait Hospitals Affiliated of SIMAD University, Mogadishu, Somalia; 2Department of Medicine and Surgery of Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 3Department of Public Health, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 4Department of Radiology, Dr. Sumait Hospitals affiliated of SIMAD University, Mogadishu, Somalia
Correspondence: Mohamed Abdulahi Hassan, Tel +252615987780, Email [email protected]
Background: Intracerebral hemorrhage (ICH) is a serious condition characterized by bleeding within the brain tissue. Although the use of sildenafil, a vasodilator agent for erectile dysfunction, has been associated with rare cases of ICH, the combination of sildenafil usage and smoking as risk factors for ICH has not yet been reported. This case report describes the occurrence of ICH in a patient with a history of both sildenafil usage and heavy smoking.
Case Presentation: A 53-year-old male, with a history of smoking and regular sildenafil use, was brought to the emergency department due to loss of consciousness with right-side weakness, he initially experienced with nausea, vomiting and dizziness after taking sildenafil 100mg tablet once. The Glasgow Coma Score (GCS) was 10 with side hemiparesis. Non-contrast CT revealed left thalamic acute hemorrhage with ventricular extension. Furthermore, a head CT angiography ruled out any vascular anomalies after that the patient was admitted to the intensive care unit (ICU) for conservative management. After three days on clinical and neurological improvement, the patient was transferred to the inpatient ward for further management, monitoring and physiotherapy. On day 6, the patient was discharged and planned for flow up.
Conclusion: This rare case highlights the need for further research and awareness regarding the potential risks associated with the combination of sildenafil and heavy smoking. Healthcare professionals should carefully evaluate the individual risk factors of patients, educate them about potential complications, and consider alternative treatments if necessary. Additionally, patients should be encouraged to quit smoking and adopt a healthy lifestyle to minimize the risk of cerebrovascular events.
Keywords: sildenafil, cigarette smoking, stroke, intracerebral hemorrhage
Introduction
Intracerebral hemorrhage (ICH) accounts for approximately 15% of all subtypes of strokes, it is considered the most dreaded form of stroke due to its high case-fatality rate and poor functional outcome.1 Worldwide; ICH resulted in 2.9 million deaths in 2019.2 In high-income countries, hemorrhagic stroke accounts for approximately 11% of all strokes, whereas in low- and middle-income countries, it constitutes a higher proportion, around 22% of all strokes.3
Sildenafil citrate has emerged as one of the first medications to address male erectile dysfunction, as the male erection occurs when there is an increase in arterial blood flow to the muscle tissue of the penis, while venous blood flow is obstructed.4 Similarly, sildenafil affects other areas of the body and can result in side effects such as headaches, flushing, and visual disturbances due to cerebral vasodilation.5
Smoking is a known and significant risk factor for other vascular diseases, such as peripheral and cardiac vascular disease. There is abundant evidence on the role of smoking in the development of stroke. The reasons for this advance lie in the acknowledgement that stroke is a heterogeneous disease, in which its subtypes are associated with different risk factors including smoking.2
The combined effect of cigarette smoking and the use of sildenafil have the potential to increase the risk of fatal complications on cerebrovascular accidents in many folds. Here, we report a case of intracerebral hemorrhages associated with sildenafil use and cigarette smoking.
Case Presentation
A 53 years old male was brought to the emergency room due to the loss of consciousness with right-side weakness. Based on information provided by his wife, he experienced sudden dizziness, nausea, and vomiting while chatting with her approximately 2–3 hours prior to admission. Subsequently, the patient became confused and had difficulty comprehending words. Eventually, his loss of consciousness prompted his wife to bring him to the emergency room. As per information provided by his wife, the patient had taken two tablets of sildenafil (100 mg) two hours before experiencing these symptoms. He had a history of unprescribed regular sildenafil usage for one year prior. The patient had no history of hypertension, diabetes mellitus, hyperlipidemia, migraine headaches or pre-existing cardiovascular or cerebrovascular diseases. Additionally, the patient has history of intense cigarette smoking habit for the past 12 years with an approximate consumption rate of one pack per day; there was no report of drug addiction either by him or within the family history (eg, cocaine usage). The patient’s height measured at 1.79 meters and he weighed 82 kg with according to the Body mass index (BMI) 23kg/m2. He also had no familial background related to cerebral arteriovenous malformation, cerebral aneurysms or intracranial hemorrhage.
Upon presentation, the patient’s neurological examination and vital signs were as follows: blood pressure measured 130/85, heart rate was 104 beats per minute, and temperature was 37.1 degrees Celsius. The Glasgow Coma Score (GCS) indicated a level of consciousness of 10 with Eye 2, Verbal 4 and motor 4, on neurological examination, there was only right-side hemiparesis. The Medical Research Council (MRC) Scale for motor assessment was estimated grade 2 although the patient was uncooperative. Laboratory tests did not reveal any significant findings as the platelet count, and coagulation factors appeared normal (Table 1). A brain non-contrast computed tomography (CT) scan confirmed the presence of an acute hemorrhage in the left thalamus with ventricular extension (Figure 1A). Furthermore, a head CT angiography ruled out any vascular anomalies (Figure 1B and C). The diagnosis of intracerebral hemorrhage (ICH) secondary to sildenafil use with cigarette smoking was made by excluding other potential causes based on the patient’s medical history and investigations. The patient was admitted to the intensive care unit, nasogastric tube was inserted for feeding and started treatment of mannitol (20%) 102g and Dexamethasone 8 mg for three times a day as anti-edema treatment along with intravenous fluids, antibiotics and proton pump inhibitors. After spending three days in the ICU, the patient showed signs of clinical and neurological improvement with GCS (14/15). The patient was transferred to the inpatient ward for further follow-up and physiotherapy. Eventually, after two more days at the ward, the patients became physical and neurological improved. He was discharged with a plan for further follow-up and physiotherapy. Finally, after three weeks of discharge, the right-side weakness was improved.
 |
Table 1 The Result of the Laboratory Investigations |
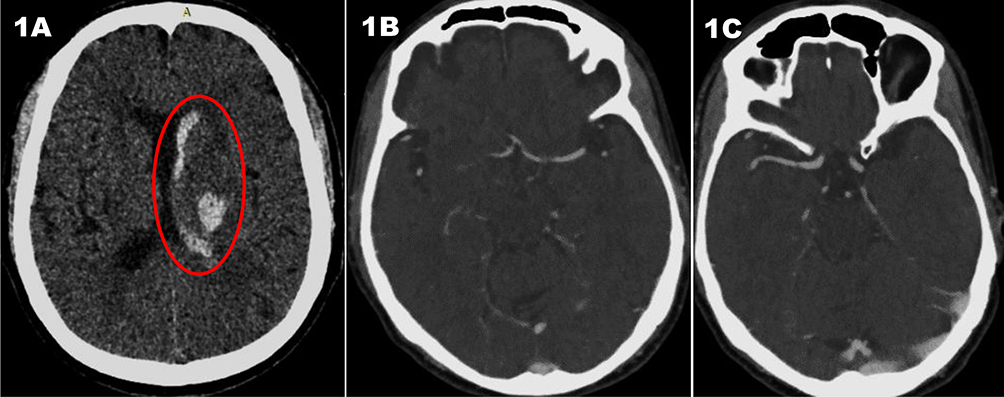 |
Figure 1 (A) Axial non-contrast-enhanced Head CT illustrates the characteristics of acute hemorrhage. The red circle indicates left thalamic high-density collection with intraventricular extension. (B) Axial Cerebral CT angiography (CTA) showing normal left middle cerebral artery (MCA) with no vascular malformation, aneurysm or stenosis. (C) Axial cerebral CTA at the level of right MCA reveals no vascular abnormalities. |
Discussion
This case study reported on the combined usage of sildenafil and smoking as risk factors for intracerebral hemorrhage while excluded other risk factors or other reasons explaining the cause of ICH.
The first successful oral medication for the treatment of erectile dysfunction (ED) is sildenafil citrate; by increasing blood flow to the penis as a natural response to sexual excitement, it improves erectile dysfunction.6 Nitric oxide (NO), which is released from the corpus cavernosum during sexual stimulation, is necessary for the physiological process that causes the penis to enlarge, the isolated human corpus cavernosum is not directly relaxed by sildenafil; however, sildenafil may enhance the relaxing effects of nitric oxide in this tissue. Similar to how sexual stimulation activates the NO/cGMP pathway, sildenafil blocks PDE5 and raises cGMP levels in the corpus cavernosum, with this function, sildenafil raises the cGMP concentration in corporeal smooth muscles and strengthens the nitric oxide’s relaxing effects through comparable mechanisms, the NO-cGMP pathway may also be in charge of vasodilation in the brain.6 Cerebral vascularity is influenced by PDE-1 and PDE-2 enzymes, and sildenafil may also have an impact on these enzymes. The literature has documented numerous adverse effects of sildenafil. The most frequent side effects of vasodilation include headaches, flushing, and nasal congestion. Other adverse effects include dyspepsia, respiratory infection, lightheadedness, and abnormalities of the vision and retina. Changes in pulmonary blood flow indicate that the medication has caused a systemic vasodilation.4
The causes of non-traumatic intracerebral haemorrhage can be divided into hypertension and non-hypertensive gross structural vascular anomalies (AVM, aneurysm, Moya-Moya diseases such as amyloid angiopathy and others), intracranial tumours, thrombosis of the veins in the brain, infection, and dysfunctional coagulopathy. Drug-induced intracerebral haemorrhages are related to sympathomimetics, anticoagulant thrombolytics, cocaine or methamphetamines. Hemorrhages in relation to sildenafil use are being increasingly reported.7 Numerous studies have reported the occurrence of intracerebral hemorrhages following the use of sildenafil.5,8 While the link between sexual intercourse and subarachnoid hemorrhage is well established, the studies believe that spontaneous sildenafil-induced intraparenchymal hematoma may be a separate entity due to the vasodilation effects of nitric oxide on the cerebrovascular system.6,9
In previous literatures, we could not find any linear relationship between drug dosage (25 mg, 50 mg, and 100 mg) and occurrence of stroke but all cases were associated with utilizing more than 50 mg once or twice in a short period.
An unknown process of sensitization may be involved however, the mode of drug action in large part, may not be cumulative but idiosyncratic.10
In this case, the patient has been using non-prescribed sildenafil previously for the past year and in this case, he ingested two sildenafil 50 mg tablet once 2 hours prior to admission, while previously he used to take 50mg per need. He had no any history of chronic illness. He also denied taking any other medications. So, we hypothesize that the use of this drug for long time and overdose he took may have altered the cerebral autoregulation with resultant abnormal cerebral arterial vasodilatation followed by subsequent hemorrhage.
Smoking has been considered as independent modifiable risk factor for stroke, with 12.4% of accidental stroke cases being attributable to current smoking behavior.11
Cigarette smoking is an independent risk factor for ICH, and several epidemiological studies have confirmed that it is a significant risk factor for stroke. In the past, this connection was primarily observed through studies, and it was believed that the effects of smoking combined with hypertension, diabetes, age, high cholesterol, and existing cardiovascular issues had significant contribution of stroke, on the other hand there is a correlation between daily cigarette smoking and intracerebral hemorrhagic volumes in ICH but the underlying mechanisms are not well understood.12 Nicotine, one of the main harmful substances in the complex toxic mixture of over 9000 chemicals in cigarette smoke, raises the risk of cardiovascular and cerebrovascular illnesses.13
According to a meta-analysis of published studies on smoking and intracerebral hemorrhage (ICH), the overall relative risk of ICH associated with smoking was found to be 0.74 (95% CI, 0.56–0.98).14 It is important to note, however, that this result was influenced by a single study conducted in neurological hospitals.14 There have been conflicting reports on the role of smoking in the development of ICH, with some studies suggesting a link between heavy smoking and ICH, while others find no association.2 The Physicians’ Health Study has been conducted on smoking and intracerebral hemorrhage for 108 cases of ICH two decades prior and found that the relative risk (RR) for ICH among current smokers was 1.98 (95% CI 1.07–3.65) when compared to never smokers.15 A study conducted in the UK revealed that the combination of smoking and aspirin use on the previous night resulted in a 40% higher risk of sICH (spontaneous intracerebral hemorrhage).16
The patient of this case has been smoking since the last 12 years with an average consumption of 15–20 pieces of cigarette per days, he has been passive smoking since 15 years, and he had no any other modified risk factors for intracerebral hemorrhage except smoking.
The combination of sildenafil use and cigarette smoking has contributed to the development of ICH in this case. The synergistic effects of these two potential factors may have led to the occurrence of ICH in this patient.
The limitations of our case, digital subtraction angiography (DSA) is not available in our country instead of that we use CT head angiography to exclude the aneurysm, and information about the patient was provided by his wife which is prone to recall bias.
This case study emphasizes the need for further research to fully understand the relationship and underlying mechanism between sildenafil use, cigarette smoking, and the occurrence of intracerebral hemorrhage.
Conclusion
The case report highlights a potential association between sildenafil use, cigarette smoking, and intracerebral hemorrhage particularly in developing countries. Our finding preliminarily suggests that the combined use of sildenafil and smoking may significantly increase the risk of hemorrhagic stroke. However, it is important to note this is a single case report, and further research is needed to establish a definitive causal relationship. Nonetheless, these findings underscore the importance of raising awareness about the potential risks of sildenafil use and smoking in developing countries. Implementing preventive measures and promoting healthier lifestyle choices are crucial in reducing the incidence of intracerebral hemorrhage in the low-income countries.
Abbreviations
ICH; intra-cerebral hemorrhage, GCS; Glasgow coma score, ICU; intensive care unit, DSA; digital subtraction angiography.
Ethics and Consent
Informed consent: A Written consent form was attained from the patient for publication of this case report and the attaching images. In our institution, ethical approval is not required for case reports.
Acknowledgments
We would like to express our sincere gratitude and deep appreciation of Center of Research and Development, SIMAD University for their guidance and recommendations and also Dr. Omar Hassan for interpreted of images in this case report.
Disclosure
As authors, we declare that there are no financial or conflicts of interest in this case report.
References
1. Donnan GA, Hankey GJ, Davis SM. Intracerebral haemorrhage: a need for more data and new research directions. Lancet Neurol. 2010;9(2):133–134. doi:10.1016/s1474-4422(10)70001-6
2. Paul SL, Thrift AG, Donnan GA. Smoking as a crucial independent determinant of stroke. Tob Induc Dis. 2004;2(2):67. doi:10.1186/1617-9625-2-2-67
3. Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8(4):355–369. doi:10.1016/s1474-4422(09)70025-0
4. Guntel M, Can H, Gok F, Tangulec G, Balikel U, Usta Busra N. Intracranial hemorrhage associated with sildenafil use: a very rare complication. Internat J Neurol Neuroth. 2020;7(1):
5. Buxton N, Flannery T, Wild D, Bassi S. Sildenafil (Viagra)-induced spontaneous intracerebral haemorrhage. Br J Neurosurg. 2001;15(4):347–349. doi:10.1080/02688690120072513
6. McHugh JM, Cheek D. Nitric oxide and regulation of vascular tone: pharmacological and physiological considerations. Am J Crit Care. 1998;7(2):131–140. doi:10.4037/ajcc1998.7.2.131
7. Antar V, Koksal Sutpideler NH, Baran O, Bitirak G. Subarachnoid and intracerebral hemorrhage after alcohol ingestion and illicit use of sildenafil. Turk Neurosurg. 2014. doi:10.5137/1019-5149.jtn.9995-13.1
8. Alpsan MH, Bebek N, Ciftci FD, Coban O, Bahar S, Tuncay R. Intracerebral hemorrhage associated with sildenafil use: a case report. J Neurol. 2008;255(6):932–933. doi:10.1007/s00415-008-0618-z
9. Pelligrino D. Cyclic nucleotide crosstalk and the regulation of cerebral vasodilation. Progress Neurobiol. 1998;56(1):1–18. doi:10.1016/s0301-0082(98)00009-4
10. Egan RA, Pomeranz H. Transient ischemic attack and stroke associated with sildenafil (Viagra) use. Neurology. 2002;59(2):
11. O’Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761–775. doi:10.1016/S0140-6736(16)30506-2
12. Aldoori MI, Rahman SH. Smoking and stroke: a causative role. BMJ. 1998;317:962–963. doi:10.1136/bmj.317.7164.962
13. Benowitz NL, Burbank AD. Cardiovascular toxicity of nicotine: implications for electronic cigarette use. Trend Cardiovasc Med. 2016;26(6):515–523. doi:10.1016/j.tcm.2016.03.001
14. Jamrozik K, Broadhurst RJ, Anderson CS, Stewart-Wynne EG. The role of lifestyle factors in the etiology of stroke. A population-based case-control study in Perth, Western Australia. Stroke. 1994;25(1):51–59. doi:10.1161/01.str.25.1.51
15. Kurth T, Kase CS, Berger K, Schaeffner ES, Buring JE, Gaziano JM. Smoking and the risk of hemorrhagic stroke in men. Stroke. 2003;34(5):1151–1155. doi:10.1161/01.STR.0000065200.93070.32
16. Thrift AG, McNeil JJ, Forbes A, Donnan GA. Risk of primary intracerebral haemorrhage associated with aspirin and non-steroidal anti-inflammatory drugs: case-control study. BMJ. 1999;318:759–764. doi:10.1136/bmj.318.7186.759
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.