")
Back to Journals » Advances in Medical Education and Practice » Volume 14
Sociodemographic Factors Associated with Knowledge About Management of Cleft Lip and Palate Patients in Peruvian Dental Students: A Logistic Regression Analysis
Authors Luyo-Peñafiel BR, Briceño-Vergel G, Ladera-Castañeda MI, Córdova-Limaylla N, Huamaní-Echaccaya JL, Romero-Velásquez L, Hernández-Huamaní E, Castro-Rojas M, Cervantes-Ganoza L, Cayo-Rojas C
Received 21 September 2023
Accepted for publication 10 November 2023
Published 16 November 2023 Volume 2023:14 Pages 1287—1298
DOI https://doi.org/10.2147/AMEP.S437637
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Brigith R Luyo-Peñafiel,1 Gissela Briceño-Vergel,1 Marysela Irene Ladera-Castañeda,2 Nancy Córdova-Limaylla,1 Jose Luis Huamaní-Echaccaya,1 Leysi Romero-Velásquez,1 Emily Hernández-Huamaní,1 Miriam Castro-Rojas,2 Luis Cervantes-Ganoza,3 César Cayo-Rojas1
1School of Stomatology, Universidad Privada San Juan Bautista, Ica, Peru; 2Faculty of Dentistry and Postgraduate School, Research Team “salud Pública – Salud Integral”, Universidad Nacional Federico Villarreal, Lima, Peru; 3Faculty of Stomatology, Universidad Inca Garcilaso de la Vega, Lima, Peru
Correspondence: César Cayo-Rojas, School of Stomatology, Universidad Privada San Juan Bautista, Carretera Panamericana Sur Km. 300, La Angostura, Subtanjalla, Ica, Peru, Email [email protected]
Background: Cleft lip and palate are relatively frequent craniofacial alterations caused by the lack of union of the frontonasal processes with the maxillary processes during the first weeks of intrauterine life. This study evaluated the sociodemographic factors associated with the level of knowledge about management of cleft lip and palate (CLP) patients in Peruvian dental students.
Methods: This analytical, observational, cross-sectional and prospective study evaluated 191 dental students belonging to two branches of a private Peruvian university (one branch in the capital city and the other in a province), from September to November 2022. A validated questionnaire of 14 closed multiple-choice questions was used. A logit model was used to evaluate the influence of the variables: sex, age, academic year of study, marital status, relationship with CLP persons, place of origin and area of residence, on the level of knowledge of the students considering a significance level of p< 0.05.
Results: Of the total, 77%, 22.5% and 0.5% presented a poor, fair and good level of knowledge, respectively, on the dental management of the patient with cleft lip and palate. In addition, those who lived in urban areas were 2.8 times more likely to have poor knowledge about the dental management of patients with CLP, compared to those who lived in non-urban areas (OR = 2.83; 95% CI: 1.26– 6.33). Finally, sex, age, marital status, place of origin, academic year of studies and relationship with CLP persons were not considered influential factors (p> 0.05).
Conclusion: Most of the students showed a poor level of knowledge about the dental management of patients with cleft lip and palate, a risk factor being that the students live in an urban area. It is recommended that educational authorities include selected topics on CLP in subjects related to infant, child and adolescent care.
Keywords: cleft lip, cleft palate, associated factors, dentistry, level of knowledge, Peru
Introduction
Cleft lip and/or cleft palate (CLP) are relatively frequent craniofacial alterations caused by an embryological defect in the lack of union of the frontonasal processes with the maxillary processes during the first weeks of intrauterine life.1–3 According to a report by the World Health Organization (WHO), this malformation affected more than 1 in every 1000 neonates in the world, both in isolation and in association with syndromes. In Peru the incidence is 1 per 700 neonates and in the high Andean areas the incidence is 1 per 600 neonates with 25% females with cleft palate, 25% males with cleft lip and 50% with both pathologies.4–6
Several factors can contribute to this congenital malformation, including genetics. Inherited from one parent, there is a 5% chance of the first child being affected. If not inherited, the second child would have a 15% risk of developing the condition.7,8 In this regard, the disease may emerge randomly as a result of certain gene abnormalities. The most prominent of these is the alteration of IRF6 (Interferon regulatory factor 6), which, according to prior research, contributes significantly to facial growth. IRF6 participates in the proliferation and differentiation of keratinocytes in oral periderm formation, and its regulation is critical for maintaining proper palatal adhesion.9,10 Furthermore, the FOXE1 gene (forkhead box protein E1) may also be altered, affecting the transportation of PVRL1 (poliovirus-related receptor 1) from the thyroid. This plays a crucial role in cell adhesion and could result in the failure of palatal ridges fusion during intrauterine life between the 5th and 12th week.8,11 It is also important to consider other genes involved in this malformation such as MSX1, GLI2, JAG2, SATB2, LHX8, SKI, ERBB2, TGFA, TGFβ2, TGFβ3, FGF, SPRY2, TBX10 and MSX2.7,8,12,13 Other possible factors include physical, chemical or environmental factors (drugs, smoking, alcohol) (Paradowska), diseases during the first trimester of pregnancy, eg rubella, influenza, gestational diabetes, radiation according to its intensity, duration and frequency of exposure, maternal age, use of teratogenic agents such as cortisone, carbamazepine, phenytoin, valproate, diazepam, diets low in riboflavin and folic acid, organic solvents, and stress. The latter can lead to increased adrenocortical activity with consequent release of cortisone, and if this event occurs during any stage of organogenesis, it can lead to various types of malformations and incidence of miscarriages.14,15
General problems in neonates and infants with cleft lip and palate include feeding reflux, sucking and swallowing disorders, mouth breathing and phonation problems.8 They may also present with dental problems such as delayed tooth eruption, enamel hypoplasia, dental caries, dilacerations, anodontia, crowding, supernumerary teeth, ectopic teeth, hypodontia and severe G4 and G5 malocclusions according to the Goslon index (Great Ormond Street, London and Oslo) caused mainly by maxillary hypoplasia, among others.11,14,16,17 To mitigate the consequences of this malformation, a series of protocols have been recommended for the feeding and maintenance of oral hygiene of these patients, especially in the early stages of development, as they are usually surgically intervened in the first months after birth.1,6,15 However, it is important that the dentist and the dental student about to graduate know how to identify, classify and timely diagnose this malformation in order to carry out activities that may allow the development of an orientation plan, consultation with the head and neck surgeon, and orthodontic treatment that will contribute to improve the health of these patients and allow them to have a better quality of life.8,15–17
Because of the aforementioned, the present study aimed to determine the sociodemographic factors associated with the level of knowledge about the management of cleft lip and palate patients in Peruvian dental students.
Methods
Study Design
This analytical, observational, cross-sectional and prospective study was written in accordance with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines for observational studies,18 and was conducted from September to November 2022 at two locations of the School of Stomatology of the San Juan Bautista Private University (UPSJB): the main site located in the Peruvian capital (Lima) and a branch located in a Peruvian province (Ica). The present study respected the bioethical principles of the Declaration of Helsinki related to confidentiality, freedom, respect, and nonmaleficence.19 It had the approval of an institutional ethics committee of the San Juan Bautista Private University with resolution No. 43–2022-CIEI-UPSJB dated January 17, 2022. In addition, voluntary informed consent was requested on the first page of the questionnaire.
Population and Selection of Participants
The population consisted of 353 students from the 3rd to the 5th academic year of study of the professional career of Stomatology of the UPSJB. Of these, 124 students belonged to the 3rd year, 133 students to the 4th year and 96 students to the 5th year. The sample size was 191 students (67 3rd year, 72 4th year and 52 5th year) and was calculated based on a formula to estimate a proportion with finite population using the statistical software Epidat 4.2. The values were p=0.5 and q=0.5 considering an absolute precision of 5%. The selection method was stratified random.
Inclusion Criteria
- Students enrolled between the third and fifth year in the professional career of Dentistry at the UPSJB.
- Dental students enrolled in semester 2022–2.
- Dental students who have voluntarily given informed consent.
Exclusion Criteria
- Students who did not complete the entire questionnaire.
Variables
The dependent variable considered was knowledge about the management of patients with cleft lip and palate. The independent variables were sex (X1)10–23 and age (X2).24 The possible confounding variables were academic year of study (X3),25 marital status (X4),18 place of origin (X5),23 area of residence (X6) and relationship with CLP persons (X7).23,26
Elaboration of the Instrument
A questionnaire of 14 closed-ended questions27 was used and improved to evaluate knowledge about dental management of cleft lip and palate patients in four aspects: general knowledge with 5 questions (Q1 to Q5), treatment protocol with 4 questions (Q6 to Q9), feeding with 3 questions (Q10 to Q12) and oral hygiene with 2 questions (Q13 and Q14) [Table 1]. Overall knowledge levels were defined according to Stanones’ rule [mean ( ) ± 0.75 (Standard deviation)]: poor (0 to 7 points), fair (8 to 11 points) and good (12 to 14 points). One point was awarded for each correct answer. Furthermore, these levels of knowledge about the dental management of the CLP patient were dichotomized as poor = 1 and fair/good = 0. The cutoff point (7.5 points) was validated by Livingston’s K2 coefficient, with an acceptable value of 0.832.
) ± 0.75 (Standard deviation)]: poor (0 to 7 points), fair (8 to 11 points) and good (12 to 14 points). One point was awarded for each correct answer. Furthermore, these levels of knowledge about the dental management of the CLP patient were dichotomized as poor = 1 and fair/good = 0. The cutoff point (7.5 points) was validated by Livingston’s K2 coefficient, with an acceptable value of 0.832.
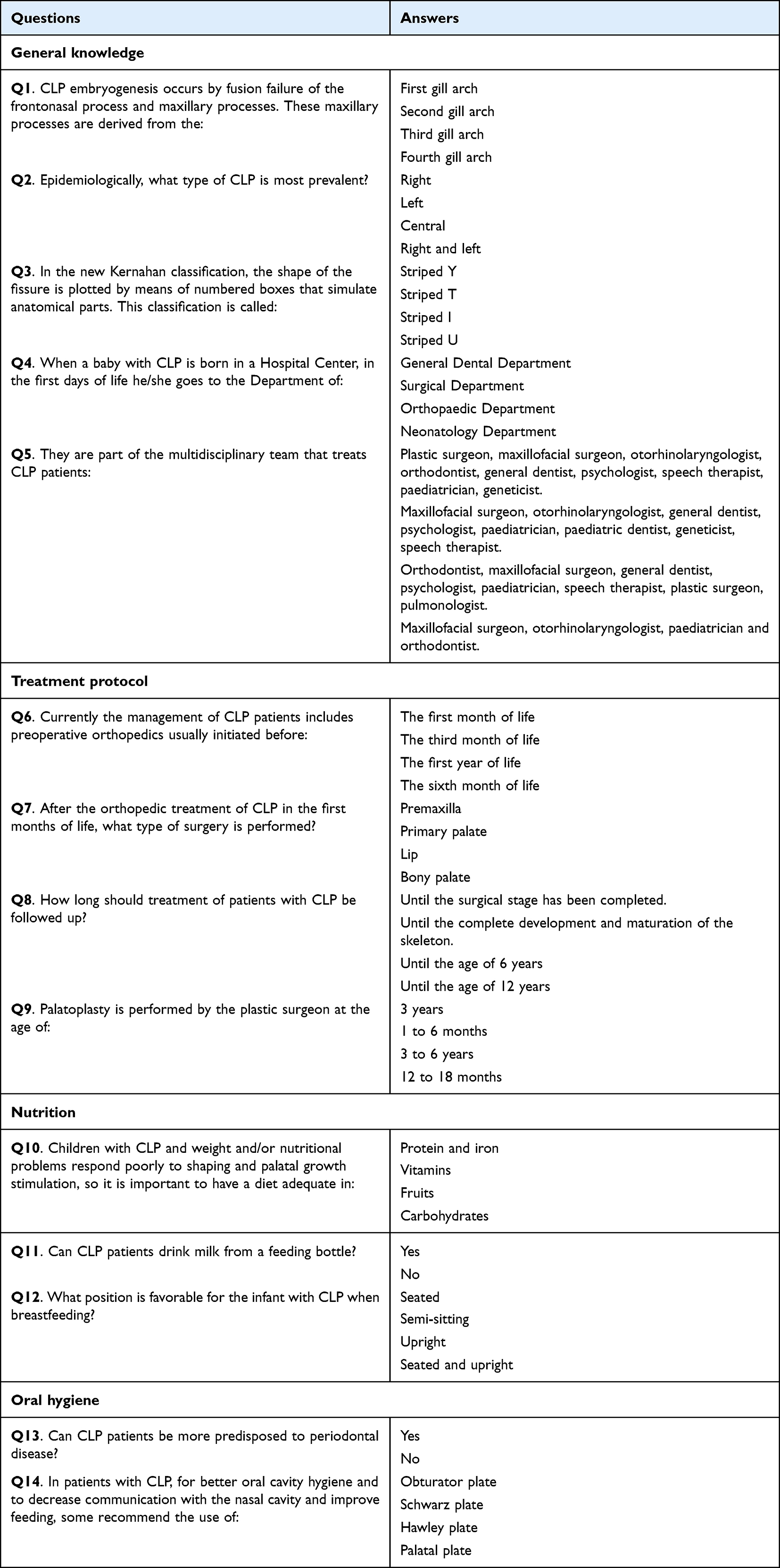 |
Table 1 Questionnaire |
Procedure
The questionnaire was distributed to each student in person by the principal researcher (B.R.L.P.). The informed consent of the students to participate in the study was at the beginning of the questionnaire, followed by the indications for its development. The questionnaire also contained the e-mail address, telephone number and full name of the principal researcher. It also contained the researcher’s home university and the institutional e-mail address of the ethics committee. Students were free to refuse the evaluation if they did not wish to complete it during its completion. Only the principal researcher had access to the students’ personal data such as their name, e-mail address and telephone number. No incentives were given for participation. The study was conducted from September to November 2022. Finally, the results of the study were sent to all those who requested the information by e-mail addressed to the principal researcher.
Validation of the Instrument
Three judges from dental research and public health fields with more than 20 years of experience evaluated and validated the content of the questionnaire. They reviewed the constructs and corresponding items, adapting the instrument to the research context. Aiken’s V validity coefficient was acceptable with a value of 0.89 (95% CI: 0.85–0.92). According to the principal component analysis with varimax rotation and Kaiser normalization, four dimensions were identified: D1 (General knowledge) (Q1 to Q5), D2 (Treatment protocol) (Q6 to Q9), D3 (Nutrition) (Q10 to Q12) and D4 (Oral hygiene) (Q13 and Q14). Bartlett’s test of sphericity and the Kaiser-Meyer-Olkin (KMO) measure indicated acceptable values of p = 0.004 and 0.505 respectively.28 Subsequently, the internal consistency reliability of the instrument was evaluated using Cronbach’s alpha obtaining an acceptable result of 0.75 (95% CI: 0.70–0.80). To assess the repeatability of the instrument, 30 randomly selected participants were surveyed at two different times (within 10 days), altering the order of the questions to avoid recall bias (test-retest).29 A Spearman’s Rho of both scores was obtained with a very good value (Rho = 0.92; 95% CI:0.84–0.96).
Statistical Analysis
Data analysis, construct validation and reliability and repeatability analysis of the instrument were carried out with the Statistical Package for the Social Sciences (SPSS) version 28.0 (SPSS Inc., Chicago, IL, United States). Descriptive statistics were applied to obtain a table of absolute and relative frequencies and bar graphs. Pearson’s chi-square test was used for bivariate analysis to test whether the distribution of the observed response is random or significantly associated with an independent variable. For the multivariate analysis, a logistic regression model with Odds Ratio (OR) was used, adjusting the model with the stepwise technique and considering the statistical prerequisites such as independent observations, sufficient sample size according to the number of independent variables, absence of multicollinearity, and goodness of fit of the model. The level of significance in all the analyses performed was p<0.05.
Results
The average age of the 191 dental students surveyed was 24.3 ± 4.2 years. The majority were women with 58.1% of the total. Of the participants, 54.5% were under 24 years of age. The 4th year students were the most numerous with 37.7% of the total. 90.1% of the participants were single. More than half of the participants (56.0%) were from the capital city and the great majority (83.2%) were urban residents. Likewise, more than half of the students did not have any type of relationship with people with cleft lip and palate (67.0%) [Table 2]. On the other hand, it was observed that 77% (95% CI: 71.0% - 82.9%), 22.5% (95% CI: 16.6% - 28.4%) and 0.5% (95% CI: 0.0% - 1.5%) presented poor, fair and good levels of knowledge, respectively, about the dental management of patients with cleft lip and palate [Figure 1].
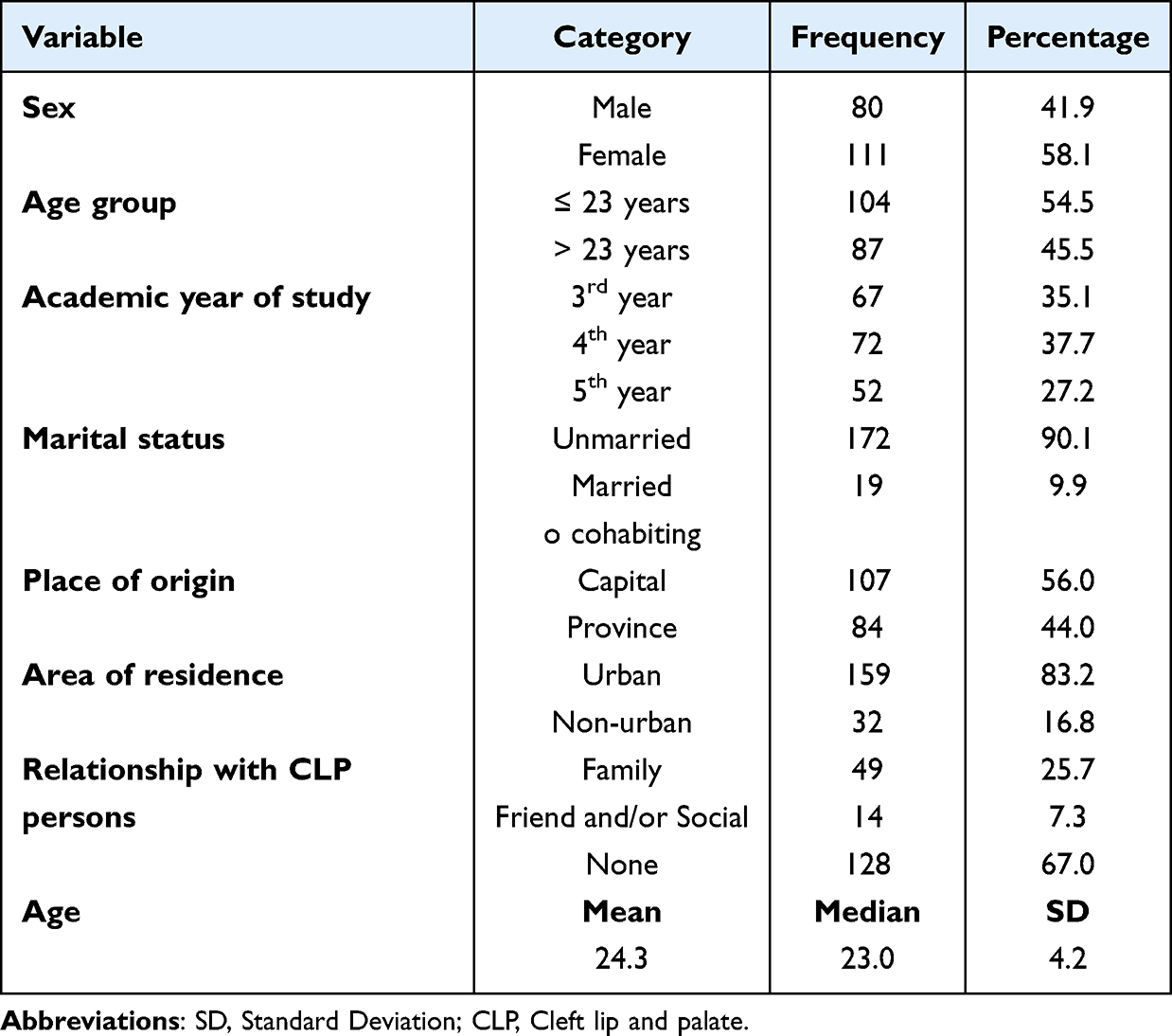 |
Table 2 Sociodemographic Characteristics of Dental Students |
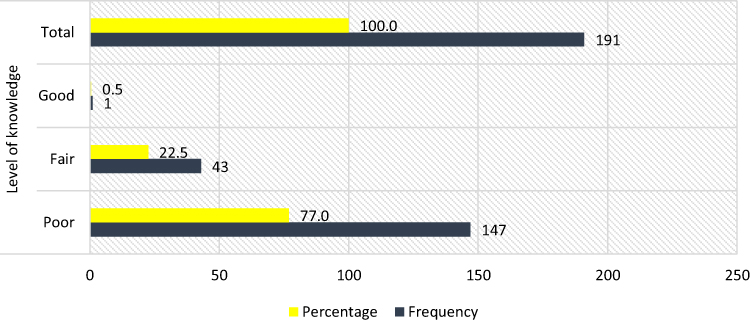 |
Figure 1 Frequency of the level of knowledge about dental management of patients with CLP in dental students. |
The bivariate analysis showed that there was a significant association of the level of knowledge about dental management of patients with CLP with the place of origin and area of residence (p = 0.021 and p = 0.010, respectively). Sex, age group, academic year of study, marital status and relationship with CLP persons were not significantly associated with this level of knowledge (p> 0.05) [Table 3].
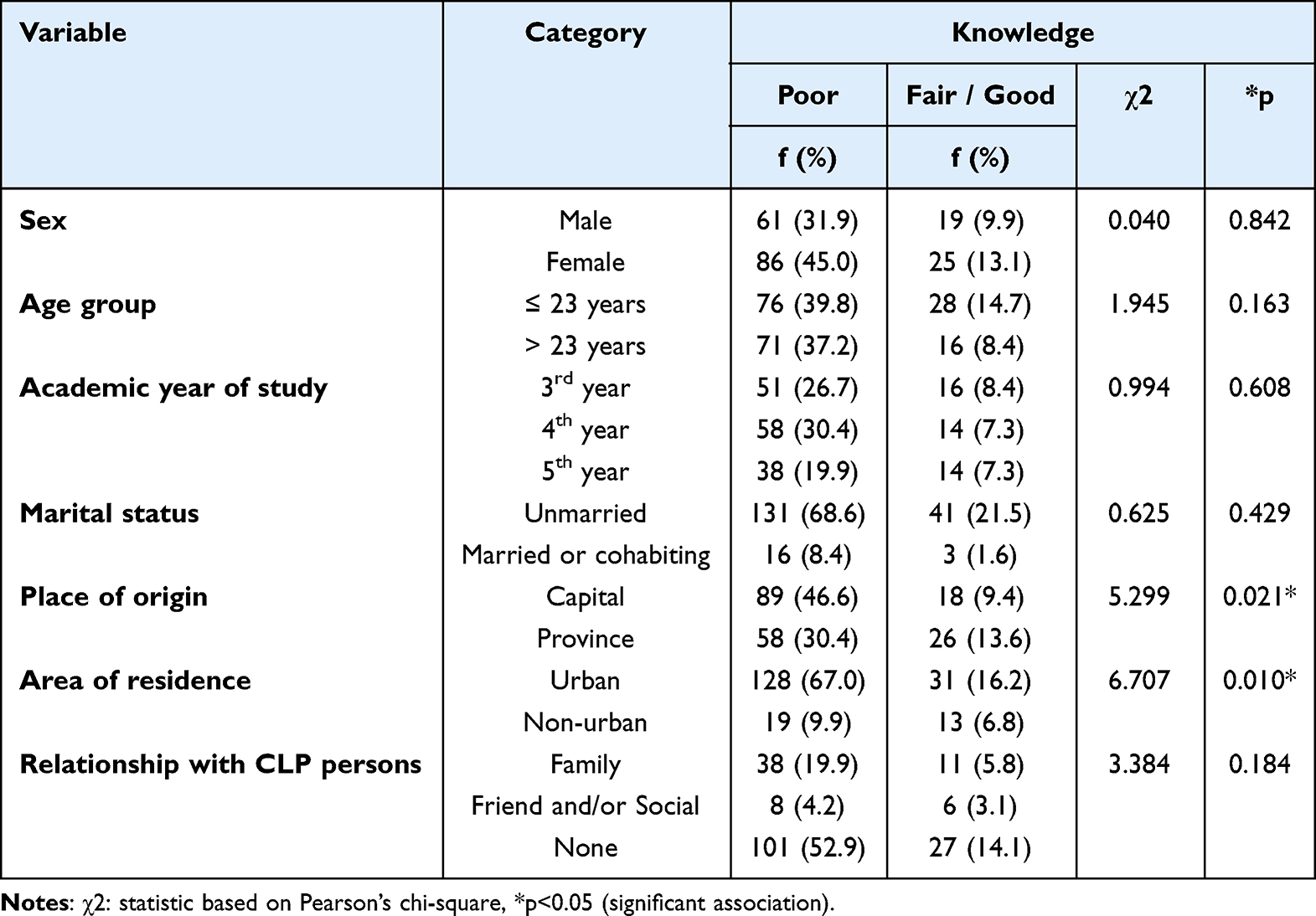 |
Table 3 Sociodemographic Factors Associated with the Level of Knowledge About Dental Management of CLP Patients |
Regarding knowledge about the dental management of the patient with CLP, there was a significant association of sex with Q3 (In the new Kernahan classification, the shape of the fissure is plotted by means of numbered boxes that simulate anatomical parts. This classification is called) and Q9 (Palatoplasty is performed by the plastic surgeon at the age of) (p = 0.011 and p = 0.025; respectively). Age group was only significantly associated with Q12 (What position is favorable for the infant with CLP when breastfeeding?) (p = 0.030). The students’ place of origin was only significantly associated with Q7 (After the orthopedic treatment of CLP in the first months of life, what type of surgery is performed?) (p = 0.013). Area of residence was significantly associated with Q6 (Currently the management of CLP patients includes preoperative orthopedics usually initiated before) and Q7 (p = 0.013 and p = 0.004; respectively). Finally, the relationship with CLP persons was significantly associated with Q4 (When a baby with CLP is born in a Hospital Center, in the first days of life he/she goes to the Department of) (p = 0.033) [Table 4].
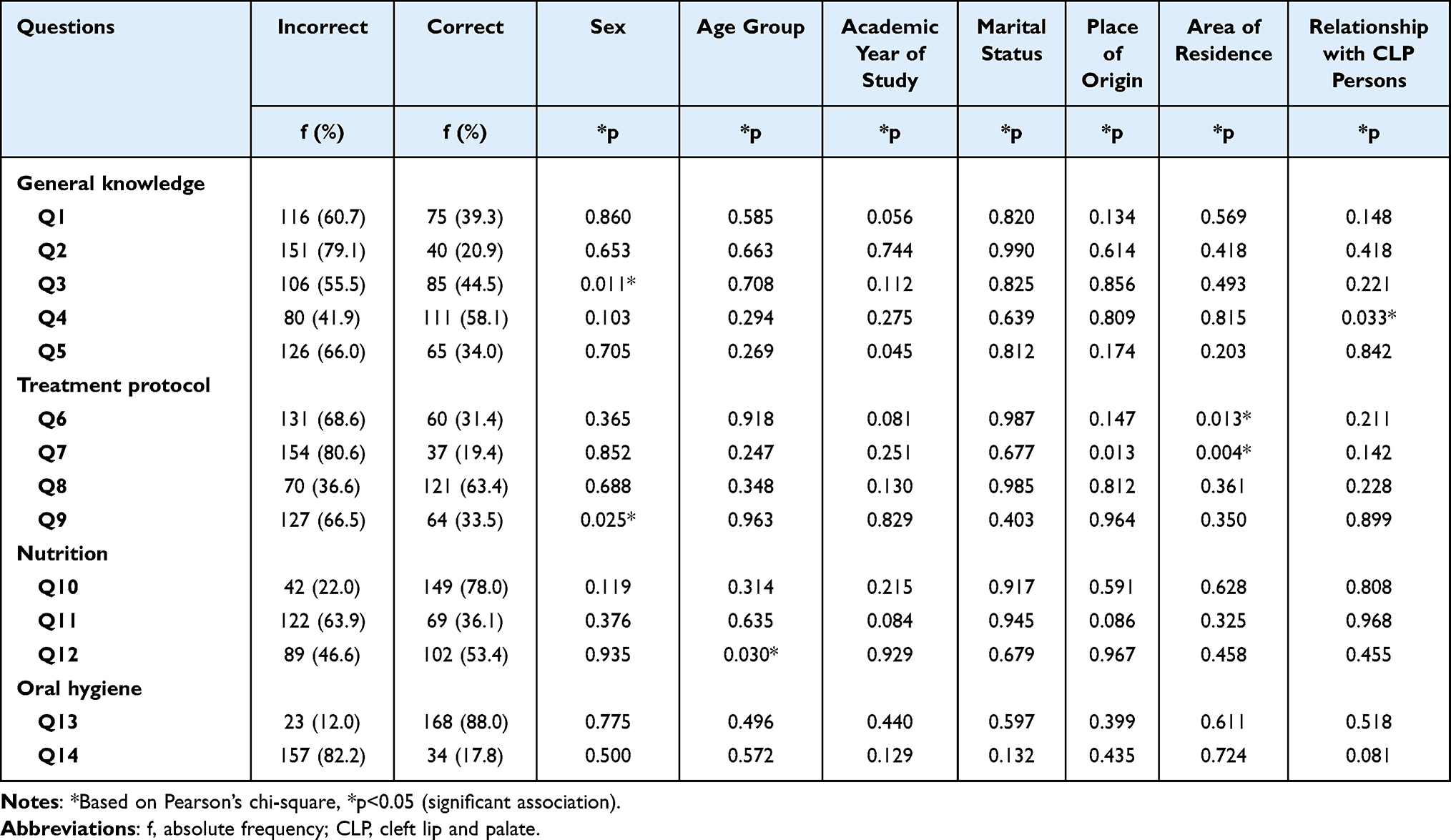 |
Table 4 Knowledge by Dimensions About Dental Management of CLP Patients Associated with Sociodemographic Factors |
Under a logit model adjusted with the stepwise technique, it could be observed that the students’ area of residence was a significant influential factor (p = 0.012) in the knowledge about the dental management of patients with CLP (categorized as poor = 1 and fair/good = 0). Those living in urban areas were 2.8 times more likely to have poor knowledge about the dental management of such patients compared to those living in non-urban areas (OR = 2.83; 95% CI: 1.26–6.33). Sex, age group, academic year of study, marital status, place of origin and relationship with CLP persons were not considered influential factors in the level of knowledge about this topic (p> 0.05) [Table 5].
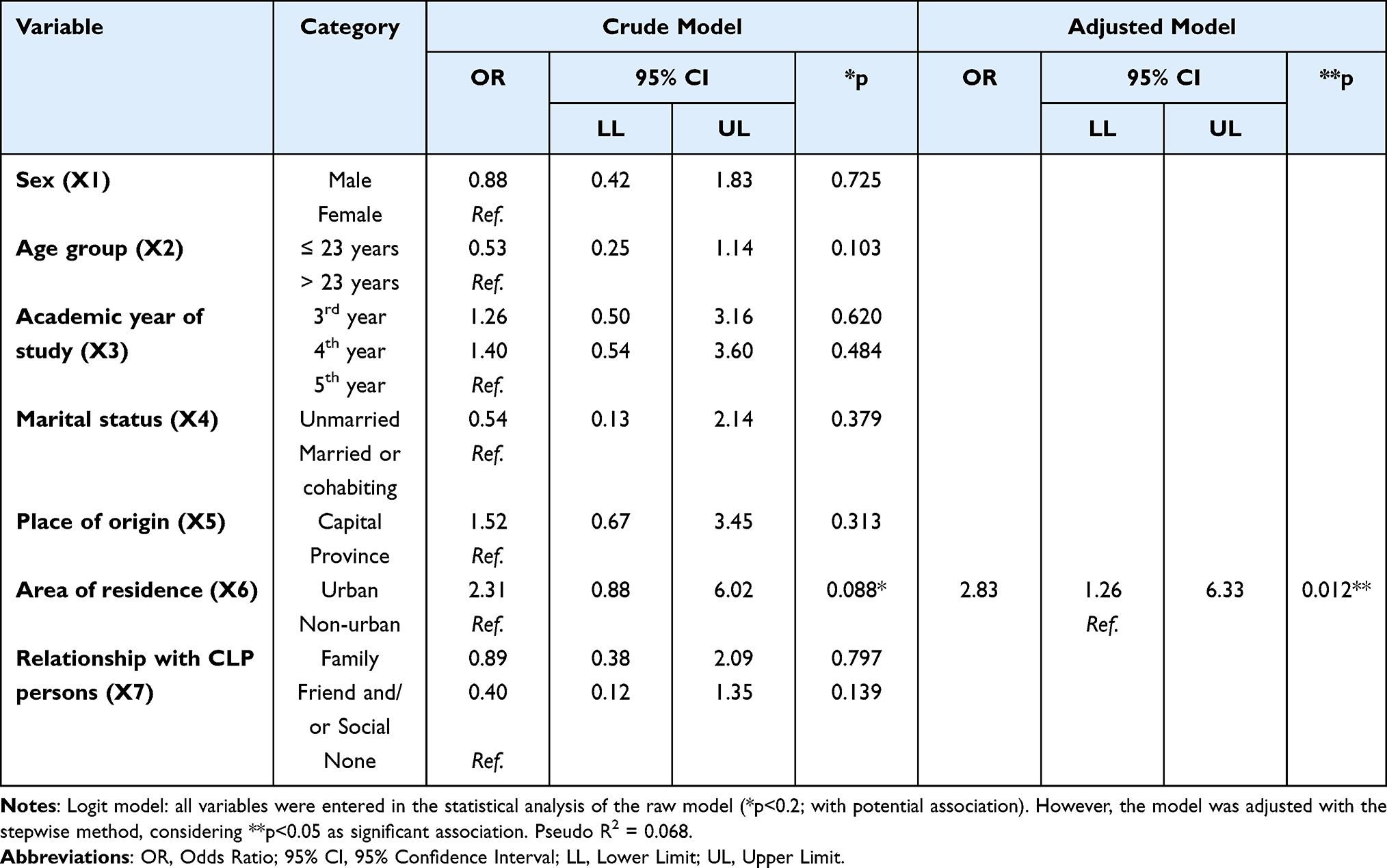 |
Table 5 Logistic Regression Model for Knowledge About Dental Management of CLP Patients |
Discussion
Cleft lip and cleft palate are the most common congenital malformations of the head and neck.30 Children born with these conditions have severe difficulties in breastfeeding, eating, speaking, hearing, smiling, breathing and may have moderate to severe malocclusion. All this generates physical and psychosocial alterations that affect their quality of life.30 Services and treatment for these conditions vary according to the severity of the cleft, the age, the needs of the child, and the presence of associated syndromes or other birth defects. Therefore, a multidisciplinary approach is important, with dentists playing an essential role.31,32 It is therefore essential for students to acquire knowledge of etiopathogenesis, diagnosis, care protocols, oral hygiene and nutritional counseling of these patients during their academic training.33 The present study aimed to determine the sociodemographic factors associated with the level of knowledge about the management of cleft lip and palate patients in Peruvian dental students. The results obtained indicate that 77% of the respondents had a poor level of knowledge about the dental management of patients with CLP. This differs from that reported by Agha et al31 who found that 73% of dental students had moderate knowledge about the management of these patients. This could be due to the fact that the students included in the present study were in their third to fifth year of study and did not take subjects with specific topics about the dental management of the CLP patient. In addition, the students surveyed received virtual theoretical education and most of their clinical practices were carried out in a semi presential manner, which could make it difficult to observe clinical cases of patients with this disorder. On the contrary, the study by Agha et al34 only included dental interns who probably had a greater possibility of developing diverse practices, clinical experiences and training on patients with CLP since their rotations are commonly performed in hospital centers. This last argument is in agreement with Moore et al35 who indicated that clinical experiences help to reinforce academic knowledge in students, thus favoring their learning.
The present study showed that the highest number of incorrect answers was in the questions about the most prevalent type of CLP, the continuity of orthopedic treatment after the first months of life, recommendations to improve oral hygiene, feeding, as well as the decrease in communication with the nasal cavity. This could be due to the fact that the respondents did not have the possibility to experience in situ the management of this type of patients. The learning of these students was based on discussion of clinical cases rather than clinical assessment, as the mode of teaching in 2022 was virtual, as due to the COVID-19 pandemic the students had been under compulsory social isolation for two years mandated by the central government.36,37 This may have had a negative impact on their level of knowledge about CLP35 since the methods available for learning did not allow them to reinforce their clinical management and link it with the theoretical learning.38
Likewise, the results obtained showed that the area of residence of the students was an influential factor in the knowledge about the dental management of the patient with CLP. Those who lived in urban areas were 2.8 times more likely to have poor knowledge compared to those who lived in non-urban areas. This may be due to the fact that students living in rural areas are generally more sensitive to people with diseases or disabilities and because of their culture or lifestyle are accustomed to performing socially responsible activities to help their community.24
The results also showed that gender, age group, academic year of study, marital status, place of origin and relationship with CLP persons were not considered influential factors in the level of knowledge. These results are consistent with studies in other areas of knowledge where age,20,24 marital status,20,21,24 sex,20–23 academic year of study,25 place of origin21,23 and relationship with vulnerable persons23 were not considered influential factors. This could be because the students surveyed from the third to the fifth year of study had little or no clinical experience in the evaluation and/or care of patients with CLP because the audiovisual resources used in virtual and blended learning were learning complements that do not replace the actual clinical experience. This situation probably limited or hindered the predisposition (attitude) towards the search for knowledge about the care of patients with CLP since it has been reported that clinical experiences generate in the student greater motivation to acquire more knowledge about situations that are considered important in their professional training.35,39
We can mention as a strength of the design of this study, a cross-sectional study was conducted that evaluated the factors associated with knowledge of the management of patients with CLP, so these findings are of utmost importance, as dental students should acquire basic knowledge for the management of these patients in clinical practice. Furthermore, it should be noted that to date (June 2023) very few studies have been found in the literature assessing the level of knowledge about the management of CLP in dental students.40,41 These studies did not consider questions on prevention strategies in relation to nutrition and oral hygiene in these patients, did not specify the general knowledge obtained by the students and did not evaluate the factors influencing knowledge on the management of CLP, as they reported knowledge on the frequency, diagnosis, distribution, aetiology, form of presentation and sequence of treatment of patients with CLP.40,41 The oral and dental problems that occur in these patients are characterized by dental anomalies in addition to scarring results of orthopedic and early maxillary surgery that interfere with proper oral hygiene maneuvers and consequently increase the risk of dental caries and periodontal disease. In view of the above, it is important that students about to graduate and dental professionals have knowledge of preventive strategies (dietary patterns, oral hygiene, use of sealants and varnishes, among others)42–45 as well as criteria for the proper diagnosis and treatment of patients with CLP in order to avoid oral problems that compromise their general health. The evaluation of knowledge in this regard is an essential tool to improve the performance of students as it evidences their preparation for the clinical field in this topic.33
This study had some limitations such as not including the entire student population since at the time the survey was conducted the students surveyed were developing some virtual and blended learning classes in the framework of the health emergency. For this reason, some did not agree to participate.23,46 Despite this, it was possible to complete the minimum sample requirement with stratified probability sampling. Likewise, the decision to carry out this study in a private university with one campus in the capital and another in the province was due to the control of the variable “curricular plan” since the dental schools in Peru do not have the same curricular design. Finally, the cross-sectional design of this study did not allow us to evaluate the dynamism of knowledge and its sustainability over time.
According to the results obtained, it is recommended that educational authorities include selected topics on CLP in subjects related to infant, child and adolescent care. It is also recommended that the health authorities develop modules and guides for general dentists as well as the development of continuing education programs for the care of patients with CLP. Centers or networks of multidisciplinary health professionals should be established for the care of these patients that include general dentists, pediatric dentists, orthodontists, plastic surgeons, oral and maxillofacial surgeons, otolaryngologists, geneticists, prosthodontists, nutritionists, psychologists, speech therapists, among others, as well as education and counseling for children with this disorder and their families.30 Finally, longitudinal studies should be performed to evaluate the effects of an educational intervention in students about the management of patients with CLP.
Conclusions
It can be concluded that the majority of students showed a poor level of knowledge about the dental management of patients with CLP, being a risk factor that the students live in urban areas. It is recommended that educational authorities include selected topics on CLP in subjects related to infant, child and adolescent care. It is also recommended that the health authorities develop modules and guides for general dentists as well as the development of continuing education programs for the care of these vulnerable patients.
Abbreviations
CI, Confidence interval; CLP, Cleft lip and/or cleft palate; OR, odds ratio; STROBE, Strengthening the Reporting of OBservational studies in Epidemiology; SPSS, Statistical Package for the Social Sciences; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethic Approval and Consent to Participate
The present study respected the bioethical principles for medical research on human beings of the Declaration of Helsinki, related to confidentiality, freedom, respect and non-maleficence. It was also approved by the Institutional Research Ethics Committee of the Universidad Privada San Juan Bautista with resolution No. 43-2022-CIEI-UPSJB dated January 17, 2022. All participants understood and gave informed consent.
Acknowledgments
We thank the Social Responsibility team of the San Juan Bautista Private University, School of Stomatology, Ica, Peru, for their constant support in the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Self-financed.
Disclosure
The authors declare that they have no conflict of interest with the development and publication of this research.
References
1. Castillo-Torres TI, Peralta-Pedrero ML, Pérez-Dosal MR, Dominguez-Martínez NM, Apodaca-García O, Cruz-Sandoval A. Educational intervention for the evaluation of nasal symmetry in cleft lip and palate operated patients. Bol Med Hosp Infant Mex. 2021;77:68–75.
2. Guerrero-Abello P, Ariza-Araujo Y, Caycedo-García DJ, Pachajoa H. Necesidad de guías clínicas para el manejo integral de pacientes con labio paladar hendido. Rev Salud Publica. 2016;18(1):82–94. doi:10.15446/rsap.v18n1.41884
3. Díaz-Casado GH, Diaz-Grávalos GJ. Orofacial closure defects: cleft lip and palate. A literature review. Semergen. 2019;267–271. doi:10.1016/j.semerg.2012.08.003
4. Peres MA, Macpherson LMD, Weyant RJ. Oral diseases: a global public health challenge. Lancet. 2019;394(10194):249–260. doi:10.1016/S0140-6736(19)31146-8
5. Instituto Nacional de Salud del Niño San Borja-INSN SB Niños con labio y paladar fisurado son intervenidos por médicos del INSN SB y operación sonrisa; 2019. Available from: https://www.insnsb.gob.pe/blog/2019/03/16/ninos-con-labio-y-paladar-fisurado-son-intervenidos-por-medicos-del-insn-sb-y-operacion-sonrisa/.
6. Lombardo-Aburto E. The intervention of the pediatrician in the child with cleft lip and palate. Acta Pediatr Mex. 2017;38:267–273. doi:10.18233/APM38No4pp267-2731435
7. Rahimov F, Jugessur A, Murray JC. Genetics of nonsyndromic orofacial clefts. Cleft Palate Craniofac J. 2012;49(1):73–91. doi:10.1597/10-178
8. Serrano CA, Ruiz JM, Quiceno LF, Rodríguez MJ. Cleft lip and/or palate: a review. Int J Med. 2009;8:44–52. doi:10.15332/us.v8i1.1180
9. Nasroen SL, Maskoen AM, Soedjana H, Hilmanto D, Gani BA. IRF6 rs2235371 as a risk factor for non-syndromic cleft palate only among the Deutero-Malay race in Indonesia and its effect on the IRF6 mRNA expression level. Dent Med Probl. 2022;59(1):59–65. doi:10.17219/dmp/142760
10. Bezerra JF, Silva HPVD, Bortolin RH, Luchessi AD, Ururahy MAG, Loureiro MB. IRF6 polymorphisms in Brazilian patients with non-syndromic cleft lip with or without palate. Braz J Otorhinolaryngol. 2020;6(6):696–702. doi:10.1016/j.bjorl.2019.04.011
11. Paradowska-Stolarz A, Kawala B. Incisors and Canines among Patients with Total Cleft Lip and Palate. Applied Sciences. 2023;13(11):1–14. doi:10.3390/app13116635
12. Letra A, Menezes R, Fonseca RF, et al. Novel cleft susceptibility genes in chromosome 6q. J Dent Res. 2010;89(9):927–932. doi:10.1177/0022034510370004
13. Tirado LR, Madera MV, González FD. Genetic and epigenetic interactions related to non-syndromic cleft lip and palate. Av Odontoestomatol. 2016;32:21–34. doi:10.4321/S0213-12852016000100003
14. Ortega-Miller JG, Yezioro-Rubinsky S, Benavides-Pinto BC, Báez-Quintero LC. Efectos teratogénicos de insecticidas organofosforados en la etiología de labio y paladar hendido: revisión de literatura. Rev nac odontol. 2017;13(24). doi:10.16925/od.v12i24.1658
15. Mejía AC, Suárez DE. Factores de riesgo materno predominantes asociados con labio leporino y paladar hendido en los recién nacidos. Medigraphic. 2012;4:55–62.
16. Navas-Aparicio M. Prevalence of supernumerary teeth in cleft lip and palate patients by analysing orthopantomographies. Rev Esp Cir Oral Maxilofac. 2017;39(3):171–178. doi:10.1016/j.maxilo.2016.03.004
17. Lehtonen V, Anttonen V, Ylikontiola LP, Koskinen S, Pesonen P, Sándor GK. Dental anomalies associated with cleft lip and palate in Northern Finland. Eur J Paediatr Dent. 2015;16(4):327–332.
18. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Re-porting of Observational Studies in Epidemiology [STROBE] statement: guidelines for reporting observational studies. Gac Sanit. 2008;22:144–150. doi:10.1157/13119325
19. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
20. Cayo-Rojas CF, Soto-Castro L, Castro-Mena M, et al. Level of knowledge about metalloproteinases in dental students close to graduate from three universities in Peruvian capital city. Eur J Dent Educ. 2022;26(4):692–699. doi:10.1111/eje.12748
21. Flores-Montalvo E, Córdova-Limaylla N, Ladera-Castañeda M. Factors associated with knowledge about pharmacological management of pregnant women in Peruvian dental students: a logistic regression analysis. BMC Med Educ. 2023;23(1):89. doi:10.1186/s12909-023-04068-9
22. Alamoudi NM, Almushayt AS, El Derwi DA, Mirdad LH, El-Ashiry EA. Dentists’ Perception of the Care of Patients with Special Health Care Needs in Jeddah, Saudi Arabia. J Oral Hyg Health. 2017;5:1–7. doi:10.4172/2332-0702.1000226
23. Santome-Pariona J, Briceño-Vergel G, Córdova-Limaylla N. Factors Associated with the Level of Knowledge about Biosafety against COVID-19 in Peruvian Dental Students: a Cross-Sectional Study under a Multivariable Regression Model. Int J Environ Res Public Health. 2023;20 11 :5938. doi:10.3390/ijerph20115938
24. Lurita-Córdova P, Ladera-Castañeda M, Santander-Rengifo F, et al. Sociodemographic factors associated with the level of knowledge about management of epileptic patients in Peruvian dental students: a cross-sectional study under a multivariable analysis. BMC Oral Health. 2023;23(1):51. doi:10.1186/s12903-023-02745-1
25. Saquib S, Ibrahim W, Othman A, Assiri M, Al-Shari H, Al-Qarni A. Exploring the Knowledge, Attitude and Practice Regarding Hepatitis B Infection Among Dental Students in Saudi Arabia: a Cross-Sectional Study. Open Access Maced J Med Sci. 2019;7(5):805–809. doi:10.3889/oamjms.2019.111
26. Cayo-Rojas C, Córdova-Limaylla N, Ladera-Castañeda M, et al. Psychological distress facing the COVID-19 pandemic in dental interns from the Peruvian capital: a cross-sectional study under a multivariable regression model. Front Public Health. 2022;10:996921. doi:10.3389/fpubh.2022.996921
27. Morales-Jiraldo JA. Nivel de conocimiento del manejo odontológico de pacientes con fisura labio palatina de los internos de odontología de tres universidades de lima metropolitana en el año 2014 [DDS Thesis]. Lima, Peru: Universidad Nacional Mayor de San Marcos; 2014. Available from: https://cybertesis.unmsm.edu.pe/handle/20.500.12672/4486.
28. Cayo-Rojas CF, Córdova-Limaylla N, Briceño-Vergel G, et al. Psychometric evidence of a perception scale about covid-19 vaccination process in Peruvian dentists: a preliminary validation. BMC Health Serv Res. 2022;22(1):1296. doi:10.1186/s12913-022-08677-w
29. Cayo-Rojas CF, Medrano-Colmenares SM, Escurra-Estrada CI, Ladera-Castañeda MI, Agramonte-Rosell RC, Cervantes-Ganoza LA. Epidemiological, preventive and healthcare knowledge about COVID-19, in dental students from three Peruvian universities. Rev Cuba De Educ Med Super. 2021;35:e2604.
30. World Dental Federation. Management of Cleft Lip and Cleft Palate Statement. 2021 Available from: https://www.fdiworlddental.org/management-cleft-lip-and-cleft-palate-statement.
31. Sabbagh HJ, Alamoudi RA, Zeinalddin M. COVID-19 related risk factors and their association with non-syndromic orofacial clefts in five Arab countries: a case-control study. BMC Oral Health. 2023;23(1):1–10. doi:10.1186/s12903-023-02934-y
32. Centers for Disease Control and Prevention. Cleft lip and cleft palate information; 2022. Available from: https://www.cdc.gov/ncbddd/spanish/birthdefects/cleftlip.html.
33. Kaul R, Jain P, Saha S, Sarkar S. Cleft lip and cleft palate: role of a pediatric dentist in its management. Int J Pedod Rehabil. 2017;2(1):1–6. doi:10.4103/ijpr.ijpr_3_17
34. Agha B, Helal NMS, Al-Khafaji TJ, Farie GA, Basri O, Fleming PS. Knowledge Assessment on Cleft Lip and Palate among Recently Qualified Dentists: a Cross-sectional Study. BMC Oral Health. 2023;23(1). doi:10.21203/rs.3.rs-2833311/v1
35. Moore R, Molsing S, Meyer N, Schepler M. Early Clinical Experience and Mentoring of Young Dental Students—A Qualitative Study. Dent J. 2021;9:1–16. doi:10.3390/dj9080091
36. Delgado-Castillo SM, Miguel-Soto S, Atoche-Socola KJ, Arriola-Guillén LE. Revolution in modern teaching in dentistry since the appearance of the COVID-19 pandemic: a review. Dent Med Probl. 2022;59(1):137–141. doi:10.17219/dmp/141522
37. Cayo-Rojas CF, Agramonte-Rosell R. Social Isolation and Virtual Proximity in the Face of the COVID-19 Pandemic. Rev cuba med gen integral. 2021;37(Sup):e1510.
38. Mansfield KJ, Peoples GE, Parker-Newlyn L, Skropeta D. Approaches to Learning: does Medical School Attract Students with the Motivation to Go Deeper? Educ Sci. 2020;10(11):302. doi:10.3390/educsci10110302
39. Jain M, Jain V, Yadav NR, et al. Dental students’ tooth shade selection ability in relation to years of dental education. Fam Med Prim. 2019;8(12):4010–4014. doi:10.4103/jfmpc.jfmpc_803_19
40. Sruthi S, Sivakumar A, Pandian KS, Navaneethan R. Knowledge, awareness, and attitude on cleft lip and palate management among dental students. Drug Invent Today. 2018;10:2608–2613.
41. Arthanari A. Knowledge and Awareness about Cleft Lip Among Undergraduate Students - A Survey. DCTH. 2021;10:451–462.
42. Rodrigues R, Fernandes MH, Bessa Monteiro A, et al. Are there any solutions for improving the cleft area hygiene in patients with cleft lip and palate? A systematic review. Int J Dent Hyg. 2019;17(2):130–141. doi:10.1111/idh.12385
43. Peña-Soto C, Arriola-Guillén L, Díaz-Suyo A, Flores-Fraile J. Clinical and epidemiological profile of cleft lip and palate patients in Peru, 2006-2019. J Clin Exp Dent. 2021;13:1118–1123. doi:10.4317/jced.58976
44. Luzzi V, Zumbo G, Guaragna M, et al. The Role of the Pediatric Dentist in the Multidisciplinary Management of the Cleft Lip Palate Patient. Int J Environ Res Public Health. 2021;19(1):1–9. doi:10.3390/ijerph18189487
45. Mendes M, Silveira MM, Costa FS, Schardosim LR. Evaluation of perception and experience of dentists in the municipal network of Pelotas/RS in attendance of cleft lip and palate patients. RFO UPF. 2012;17:196–200.
46. Morales-Montoya M, Córdova-Limaylla N, Briceño-Vergel G, et al. Psychological impact on dental students and professionals in a Lima population during COVID-19s wave: a study with predictive models. Sci Rep. 2022;12(1):14752. doi:10.1038/s41598-022-18899-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.