")
Back to Journals » Open Access Journal of Sports Medicine » Volume 14
Stress Fractures of the First Rib Related to Soft Tennis, Associated with the Tennis Ground Stroke
Authors Sakamoto A, Okudaira S, Onishi Y, Noguchi T, Matsuda S
Received 2 November 2023
Accepted for publication 21 December 2023
Published 27 December 2023 Volume 2023:14 Pages 99—102
DOI https://doi.org/10.2147/OAJSM.S447674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Akio Sakamoto, Shuzo Okudaira, Yuta Onishi, Takashi Noguchi, Shuichi Matsuda
The Department of Orthopaedic Surgery, Graduate School of Medicine, Kyoto University, Kyoto, Japan
Correspondence: Akio Sakamoto, The Department of Orthopaedic Surgery, Graduate School of Medicine, Kyoto University, Shogoin, Kawahara-cho 54, Sakyo-ku, Kyoto, 606-8507, Japan, Tel +8175-751-3366, Fax +81-75-751-8409, Email [email protected]
Abstract: Stress fractures of the first rib are uncommon and thought to be associated with overhead-throwing athletes. Soft tennis is similar to regular tennis but uses a much softer rubber ball. In the current report, a 14-year-old girl suffered from shoulder girdle pain, especially at the end of her tennis ground stroke. Plain radiographs showed overgrowth of bone with a fracture line on the first rib, and a diagnosis of stress fracture was made. She was advised to amend her stroke form to reduce force to the shoulder and was able to continue sports activity without pain 10 months after the appearance of her symptoms and before confirmation of bone healing. The current case is not associated with overhead-throwing, but possibly with repetitive exercises of her tennis ground strokes. Conservative medical follow-up with proper sport-specific professional advice allows continuation of the sport.
Plain Language Summary: Stress fractures of the first rib are rare, mainly linked to overhead-throwing athletes. Soft tennis resembles regular tennis but uses a softer rubber ball. In this case, a 14-year-old girl with shoulder girdle pain, especially during tennis strokes, was diagnosed with a first rib stress fracture via plain radiographs. She improved by adjusting her stroke and resumed sports pain-free within 10 months, even before full bone healing. This case was not linked to overhead-throwing but potentially resulted from repetitive ground strokes. Proper medical guidance supports sport continuation.
Keywords: first rib, stress fracture, tennis, tennis stroke
Introduction
Stress fractures of the first rib are uncommon but have been reported in various sports such as baseball,1,2 rugby,3 and gymnastics.4 An association of first rib stress fractures with overhead-throwing in baseball has been reported.1,2 However, first rib stress fractures are also reported on the non-throwing side.5–8 First rib stress fractures on the non-throwing side may be related to swinging a baseball bat.7
Soft tennis was developed in Japan based on regular tennis. The main difference between soft tennis and regular tennis is that the ball in soft tennis is a much softer rubber ball, from which the name “soft tennis” comes. The rubber balls are hollow and filled with air, 6.6 cm in the diameter and 30–31 g in weight. They bounce 70 to 80 cm when dropped from a height of 150 cm.9
This case reports a first rib stress fracture in a girl playing soft tennis as a school club activity. The current case is not associated with overhead-throwing, but possibly with repetitive exercises of her tennis ground strokes.
Case Presentation
A 14-year-old right-handed female suddenly suffered from right shoulder and scapular regional pain at the end of her tennis ground stroke. She was one of the representative junior high school players in the prefecture, and Japan had 47 prefectures in total. She practiced for 2 hr daily, 6 days a week at school. Her practice menu was mainly ground strokes and practice of the overhead service every practice day, but only for a short time. She did not engage in muscle training and participated in matches only 1 or 2 days a month. She noticed no shoulder pain during activities of daily living but felt pain when she carried her backpack on her right side. She visited a nearby hospital and was introduced to our institute with a working diagnosis of a bone tumor 4 weeks after the appearance of symptoms. Initially, her doctor advised her to refrain from joining tennis club activities.
On physical examination, the range of motion in her right shoulder was 180° in flexion, 180° in abduction, and 60° in both internal and external rotation. The motion of the extremity caused no pain during the examination. Tenderness of the right scalene muscle area was recognized. Radiculopathy was negative based on Jackson compression and Spurling tests. There was no sensory disturbance. Plain radiographs of the cervical spine depicted bone overgrowth with an osteolytic fracture line in the first rib (Figure 1). Because a specific history of an accident was absent, the diagnosis was made of a stress fracture associated with playing soft tennis.
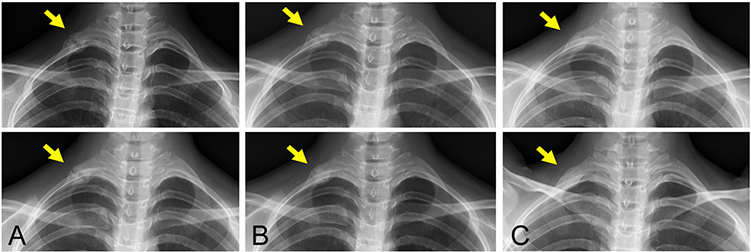 |
Figure 1 A fracture line are seen at one month (A-top), three months (A-bottom), five months (B-top) and six months (B-bottom) after the appearance of shoulder pain. Bone union is observed at 10 months after the initial symptoms (C). Fracture lines are indicated by the yellow arrows. |
At our institute, the form of the stroke was checked. We observed that, in her efforts to enhance swing speed, she concentrated on her upper extremities rather than the trunk. Specifically, she emphasized increasing the angular velocity of the elbow joint, resulting in a shorter swing with the hitting point closer to the body. The patient had a form in which the elbow was bent and rotated around the shoulder during the fore stroke. We recommend incorporating the trunk into her swing and introducing muscle exercises, such as push-ups and sit-ups, to enhance trunk strength. With the corrected swing, the arch widened, and she began hitting the ball slightly away from her body. To reduce stress to the shoulder, the form was amended so that the elbow was extended during the follow-through. She was allowed to join the club activity minding her corrected form and was able to continue the sport activity without pain. Bone healing was confirmed 10 months after the appearance of the symptoms (Figure 1).
Discussion
Symptoms of a rib stress fracture are nonspecific, but include pain in the periscapular region, posterior shoulder, upper chest, or base of the neck.2,8 The absence of specific characteristics during physical examination makes the diagnosis difficult.6,8 Evoked pain in shoulder motion can lead to a differential diagnosis of shoulder injuries such as rotator cuff impingement.2 Therefore, rib stress fractures can be overlooked as a cause of shoulder pain in athletes.10
Stress fractures typically occur in the subclavian groove of the first rib.2 The fracture lines in the subclavian groove can often overlap with the clavicle in an anteroposterior plain radiograph of the ribs, therefore first rib fractures are easily overlooked.11 It has been reported that the sensitivity of radiography for stress fractures is about 10%.12 Although it has been reported that only 1 of 6 first rib stress fractures is diagnosed on plain radiographs of the shoulder, plain radiography of the cervical spine nevertheless is useful for the diagnosis of first rib fractures.6
The subclavian groove of the first rib is located between the anterior and middle scalene muscle attachments.2 The shape of the first rib is broad and flat, and the subclavian groove where the subclavian artery and vein are located on its cephalad surface is its thinnest portion. This part of the first rib is vulnerable to stress fractures because tensile forces occur from the downward forces of the serratus anterior muscle and upward forces of the scalene muscles.5,7,13,14
Stress fractures of the first rib are possibly associated with overhead-throwing in athletes.2,6,7 However, they may occur on either the dominant or non-dominant sides.15 First rib stress fractures on the non-dominant side in baseball players are also reported in association with intensive bat swinging.7 In the current case, the patient played a tennis club activity after school, mainly exercising her tennis ground stroke, and the injury was not associated with overhead-throwing. She was advised to amend her stroke form to reduce the force to the shoulder. She was able to continue tennis activity without pain, before confirmation of bone healing.
Previous reports of sports-related first rib fractures indicate a relatively good prognosis.7,13,16,17 Reports have shown that rest and avoiding sports activities are usually sufficient to treat these stress fractures.6,13,16 Most of these injuries heal spontaneously without any intervention after 4 to 6 weeks of rest, with return to competitive sports between 2 and 3 months.4,6,11 However, fractures with delayed union and nonunion of the first rib have been described.4,6,11 In one report, 29% of 24 patients with first rib stress fractures led to a nonunion in spite of the conservative treatment of avoiding sports activities.6 Even in cases of a delayed union or nonunion, most athletes can return to sports activities without symptoms.1,5
Conclusions
The current case of a first rib fracture was not associated with overthrowing but rather with the practice of tennis ground strokes. Suspecting rib stress fractures is necessary in athletes experiencing shoulder pain, particularly those engaged in throwing and racket sports. In the current case, amendment of the form allowed the patient to continue the sports activity without pain before bone union. Conservative medical follow-up with proper sport-specific advice leads to the continuation of the sport.
Ethics Approval and Informed Consent
Patients and their parents were informed that data from the cases would be submitted for publication, and their parents gave consent. The study has been approved by the institutional review board Kyoto University (R2499).
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Edwards TB, Murphy C. Nonunion of a dominant side first rib stress fracture in a baseball pitcher. Orthopedics. 2001;24(6):599–600. doi:10.3928/0147-7447-20010601-20
2. Mithöfer K, Giza E. Pseudarthrosis of the first rib in the overhead athlete. Br J Sports Med. 2004;38(2):221–222. doi:10.1136/bjsm.2002.002998
3. Kemp SP, Targett SG. Injury to the first rib synchondrosis in a rugby footballer. Br J Sports Med. 1999;33(2):131–132. doi:10.1136/bjsm.33.2.131
4. Proffer DS, Patton JJ, Jackson DW. Nonunion of a first rib fracture in a gymnast. Am J Sports Med. 1991;19(2):198–201. doi:10.1177/036354659101900218
5. Curran JP, Kelly DA. Stress fracture of the first rib. Am J Orthop. 1966;8(1):16–18.
6. Funakoshi T, Furushima K, Kusano H, et al. First-rib stress fracture in overhead throwing athletes. J Bone Joint Surg Am. 2019;101(10):896–903. doi:10.2106/JBJS.18.01375
7. Kawashima K, Terabayashi N, Miyagawa T, et al. Stress fractures of the first rib related to swinging of a baseball bat: two case reports. Clin J Sport Med. 2016;26(6):e108–e110. doi:10.1097/JSM.0000000000000278
8. Ozawa S, Lee SY, Fujimaki Y, Kawasaki K, Inagaki K. Delayed union of stress fracture of the first rib in a Yoga instructor: a case report. JBJS Case Connect. 2021;11(2). doi:10.2106/JBJS.CC.20.00893
9. Japan-Soft-Tennis-Association. Available from: https://www.jsta.or.jp/wp-content/uploads/international/en/whats.html.
10. Barrett GR, Shelton WR, Miles JW. First rib fractures in football players. A case report and literature review. Am J Sports Med. 1988;16(6):674–676. doi:10.1177/036354658801600622
11. Gamble JG, Comstock C, Rinsky LA. Erroneous interpretation of magnetic resonance images of a fracture of the first rib with non-union. Two case reports. J Bone Joint Surg Am. 1995;77(12):1883–1887. doi:10.2106/00004623-199512000-00013
12. Wild AT, Begly JP, Garzon-Muvdi J, Desai P, McFarland EG. First-rib stress fracture in a high-school lacrosse player: a case report and short clinical review. Sports Health. 2011;3(6):547–549. doi:10.1177/1941738111416189
13. Mintz AC, Albano A, Reisdorff EJ, Choe KA, Lillegard W. Stress fracture of the first rib from serratus anterior tension: an unusual mechanism of injury. Ann Emerg Med. 1990;19(4):411–414. doi:10.1016/S0196-0644(05)82349-2
14. Chimenti PC, Elfar JC, Giordano BD. Dominant-sided first-rib stress fracture in a collegiate baseball pitcher: a case report. JBJS Case Connect. 2013;3(4 Suppl 2):e108. doi:10.2106/JBJS.CC.M.00019
15. Young EJ, Curtis RJ. First-rib stress fractures related to hitting in two baseball teammates. Clin J Sport Med. 2008;18(3):300–301. doi:10.1097/JSM.0b013e31816ffbd4
16. Coris EE, Higgins HW. First rib stress fractures in throwing athletes. Am J Sports Med. 2005;33(9):1400–1404. doi:10.1177/0363546505275349
17. Chaudhury S, Hobart SJ, Rodeo SA. Bilateral first rib stress fractures in a female swimmer: a case report. J Shoulder Elbow Surg. 2012;21(3):e6–e10. doi:10.1016/j.jse.2011.08.048
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.