")
Back to Journals » Vascular Health and Risk Management » Volume 19
Suboptimal Knowledge and Care of Patients with Acute Coronary Syndrome Among Nurses Working in Selected Hospitals in Addis Ababa, Ethiopia 2021
Authors Lakew BA, Bekele DM , Alemu Kassa W, Dugassa Tolera B
Received 8 June 2023
Accepted for publication 27 August 2023
Published 21 September 2023 Volume 2023:19 Pages 637—649
DOI https://doi.org/10.2147/VHRM.S422339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Bizuayehu Ashine Lakew, Daniel M Bekele, Wudma Alemu Kassa, Boka Dugassa Tolera
School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Boka Dugassa Tolera, School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University, Ethiopia, Tel +251-913-132-398, Email [email protected]
Background: Acute Coronary Syndrome is the leading cause of morbidity and mortality in developing nations including Ethiopia. As frontline healthcare providers, nurses need to be prudent in handling cases of acute coronary syndrome. However, nurses’ knowledge and practice of acute coronary syndrome are not well-known across Ethiopia. Thus, this study aimed to assess knowledge, practice, and associated factors regarding the care of acute coronary syndrome among acute care nurses working at selected hospitals in Addis Ababa, Ethiopia.
Methods: Institution-based descriptive cross-sectional study design was conducted from February to March among 252 purposively selected nurses working in tertiary hospitals of Addis Ababa, Ethiopia. A pretested and structured questionnaire was used for data collection. Data were entered into Epi-Data 4.6 and exported to SPSS version 25. Both descriptive and inferential statistics were used to describe and test the association between selected variables. P-values < 0.05 were declared as significant factors for the outcome variable.
Results: Out of 252 nurses, (52%) had good knowledge, and (44.4%) had good practice towards care of Acute Coronary Syndrome. Being a master’s degree [AOR=3.801, (95% CI:1.314– 10.996), P =0.014] and having guidelines [AOR= 10.998, (95% CI:2.478– 48.805), P =0.002] were significantly associated with nurse’s good knowledge of ACS. While having a master’s degree [AOR=4.258, (95% CI:1.676– 10.820), P=0.002] and getting in-service training [AOR= 1.902, (95% CI:1.022– 3.539), P = 0.042] were significantly associated with nurse’s good level of practice.
Conclusion: In this study, nurses had inadequate knowledge and practice regarding the care of Acute Coronary Syndrome. Nurses’ educational level, presence of clinical practice guidelines, and getting training were determinant factors associated with good knowledge and practice. Therefore, organizational and nursing educational support are needed to improve this gap by providing short- and long-term training, and updated evidence-based clinical practice guidelines should be available for all acute care nurses.
Keywords: knowledge, care, acute care nurses, acute coronary syndrome
Introduction
Acute Coronary Syndrome (ACS) is a type of cardiovascular disease that can result from a sudden drop in blood flow through the coronary arteries supplying different regions of the myocardium.1 This condition encompasses ST-elevation myocardial infarction, non-ST-elevation myocardial infarction, and unstable angina.2 It is responsible for about more than one million deaths each year across the world3 and the prevalence of ACS is rising in low- and middle-income countries including Ethiopia.4 A recent study indicates that ACS is responsible for about 22% of hospital mortality across Africa.5 Moreover, in Ethiopia, the prevalence of mortality due to ACS was 27.4%.6 This is higher when compared to the result of the study reported in Sub-Saharan Africa, which was 13.5%.7 This indicates that ACS remains a major public health problem and is responsible for significant morbidity and mortality in Ethiopia.
It has been reported in previous studies that ACS has a direct association with several clinical problems. These include chest pain, alterations in blood flow,8 limitation in physical activities, severe anxiety, and depression,9 which have a negative impact on the patient’s quality of life. With these multiple problems associated with ACS, prevention, early diagnosis, and management are essential to mitigate the detrimental consequence of ACS. The ultimate goal of ACS prevention and management is to reduce morbidity and mortality by promoting a healthy lifestyle, reducing risk factors, and improving adherence to medications.10 To achieve the goal established for patient-centered high-quality care, an organized and systematic approach of dedicated health healthcare professionals is needed.
As frontline healthcare providers, nurses are expected to have adequate knowledge and skill in the prevention and management of ACS.11 According to the World Health Organization, nurses are key personnel for improving CVD care access in neglected area,12 and they have a professional responsibility to lead CVD prevention initiatives, as they are a frontline to communicate with patients and their families. The nurses’ knowledge regarding the care of ACS includes Awareness of understanding about causes, signs and symptoms, risk factors, complications, and the overall management of ACS.1 This is essential to reduce the gap between evidence and practice. Mainly, acute care nurses work in Emergency Department (ED), ICU (Intensive Care Unit), and CCU (Cardiac Care Unit). Hence, as expert clinicians, they can play an integral role in the assessment, prevention, and care of patients with ACS and these can improve the quality of patient care and satisfaction.11,13
However, several studies have shown that the knowledge and practice of nurses regarding ACS were inadequate.14,15 It was demonstrated that nurses’ knowledge and ability to correctly identify the diagnostic finding of patients with ACS was limited.16,17 Another study conducted in Iran country revealed that nurses have poor knowledge and low critical thinking skills for managing serious conditions in emergency and critical care units.15 Some of the factors affecting nurses’ knowledge and necessary practice in caring for patients with ACS include Socio-demographic characteristics such as age, work experience, working department, and educational level,12,18 health system-related factors such as material resources, human resources, and in-service training,19 poor knowledge in utilizing clinical guidelines2 and health system-related barriers including lack of necessary diagnostic and treatment equipment.20
Inadequate knowledge and poor practice of acute care nurses have a negative impact on patient outcomes. Especially, it can impact the quality of life of patients.6 Therefore, ACS requires a life-saving intervention and standardized care from qualified and skilled health care provider.21 Mainly, nurses equipped with adequate knowledge about ACS care are critical in the control, prevention, and care of the disease.11,22 However, in Ethiopia, no study has been conducted related to nurses’ knowledge, practice, and associated factors regarding the care of ACS. Due to this, nurses’ knowledge and practice of ASC are not well-known across Ethiopia. Therefore, this study aimed to assess the level of knowledge, practice, and associated factors of acute care nurses regarding the care of ACS in tertiary hospitals of Addis Ababa, Ethiopia.
Methods and Materials
Study Design, Setting, and Period
The facility-based descriptive cross-sectional study design was conducted in tertiary hospitals in Addis Ababa, Ethiopia from February – March 2021. Three tertiary-level hospitals; Tikur Anbessa Specialized Hospital, St.Paul’s Hospital, and St.Peter Specialized Hospital were selected purposively where patients with ACS are primarily treated. Tikur Anbessa specialized hospital is the largest referral hospital in the nation at the tertiary level. The hospital had 800 beds with 470 doctors and 885 nurses. An ED, CCU, and ICU was the specific setting for the study. A total of 122 nurses working in the ED (65), ICU (44), and CCU (13). St. Paul’s Hospital is the second largest tertiary-care teaching multi-facility and multi-disciplinary medical center in Ethiopia. The adult ICU is staffed by 42 nurses, CCU by 10 nurses, and ED by 40 nurses. St.Peter Specialized Hospital is one of the main cardiac centers in Ethiopia staffed by 24 nurses in ED, 8 nurses in CCU, and 25 nurses in ICU.
Population
The source populations were all nurses working in the adult ED, CCU, and ICU of selected government hospitals in Addis Ababa, Ethiopia. Whereas, the study populations were all nurses who are working in ED, ICU, and CCU of selected government Hospitals during the study period.
Inclusion and Exclusion Criteria
All acute care nurses who were available and working in the ED, ICU, and CCU at the time of data collection, those who served six months or more, and whose work was associated with the care of the cardiovascular patient. But nurses on annual leave, sick leave and not volunteered to participate in the study were excluded from the study.
Sample Size Determination and Sampling Technique
All nurses working in the ICU, CCU, and ED of the selected hospitals who fulfill the inclusion criteria were included by non-probability survey sampling. The number of acute care nurses working in Tikur Anbesa Specialized Hospital, St Paul’s Hospital, and St Peter Hospital is 122, 92, and 57 respectively. Of this, 252 of the study participants have participated in the study. Purposive sampling techniques were employed to enroll the participants.
Variables
The dependent variables were knowledge of ACS and the practice of nurses regarding the care of patients with acute coronary syndrome. The independent variables included: participants’ socio-demographics (age, gender, year of experience, working unit, and level of education), and institutional factors: (in-service training, presence of clinical practice guidelines, presence of diagnostic and treatment resources in working units).
Data Collection Tools
Data were collected by using a pretested and structured self-administered questionnaire developed after a review of literature related to the topic of interests.1,13,17,23 The data collection tool consists of three parts: The first part of this questionnaire included the socio-demographic characteristics that consist of 8 questions aimed to gather information about the study participants’ age, gender, educational level, years of work experience, working department, and attended training program on the care of ACS, presence of clinical practice guidelines, presence of diagnostic resources, and presence of treatment resource in a working unit. The second part of the questionnaire which consisted of 15- items examined nurses’ knowledge of ACS. In this part, all items were responded to by a closed-ended (ie correct and incorrect). The respondent’s correct and incorrect responses provided for the questions were given “1” or “0” points, respectively. The total score of knowledge items ranging between 0 and 15 was classified into two responses: good knowledge good knowledge (if above the mean) and poor knowledge (if equal to or below the mean value). The third part was used to examine the nurses’ practice regarding the care of a patient with ACS. This part was measured by 33- items responded with a 5-point Likert scale (never, rarely, sometimes, often, and always) and received “0” for never practice, “1” for rarely practice, “2” for sometimes practice, “3” for often practice and “4” for always practice. Then the total score of practice items ranged from 0 to 132 and was transformed into a mean for interpretation. Accordingly, nurses’ practice regarding care for patients with ACS was classified into two categories: good practice (if above the mean) and poor practice (if equal to or below the mean).
Operational Definition
Acute coronary syndrome: Is a syndrome due to decreased blood flow in the coronary arteries as a result part of the heart muscle is unable to function properly or dies.1
Acute care nurses: Refers to nursing professionals who have good knowledge and skill (or experience) in caring for patients with immediate and serious medical needs including ACS.
Nurses’ good knowledge of ACS: Respondents who scored above the mean score on knowledge items concerning ACS.
Nurses’ poor knowledge of ACS: Respondents who scored below the mean score on knowledge items concerning ACS.
Nurses’ good practice of ACS: Respondents who scored above the mean score on practice items regarding the care of patients with ACS.
Nurses’ poor practice of ACS: Respondents who scored below the mean score on practice items regarding the care of patients with ACS.
Data Collection Procedure and Data Quality Assurance
Before data collection, four data collectors and two supervisors were provided a one-day intensive training on the techniques of data collection, objectives of the study, ethical issues, procedures, tools, and ways of collecting the data. The quality of data was assured through the careful design of questionnaires. Before starting data collection, the questionnaire was checked for clarity comprehensiveness, and content validity. A pre-test was done on 5% of the sample size who worked at Alert Hospital. To test the reliability of the tool, Cronbach alpha values were calculated for questionnaires, yielding α = 0.86. Data collectors were instructed to check the completeness of each questionnaire and an ongoing checkup for completeness and consistency of responses was made by the supervisors and principal investigators on a daily basis.
Statistics
Data were initially coded, verified, and entered into Epi-Data software version 4.6 then exported to SPSS software version 25.0 for statistical analysis. A descriptive statistics such as frequency, percentages, means, standard deviation, and ranges were used to describe the outcome variables. Binary logistic regression and multivariable logistic regression were used to determine the association between dependent and independent variables. Chi‐square (χ2) assumptions were checked for categorical variables before identifying candidate variables on bi‐variate binary logistics regression and multicollinearity was checked using the variance inflation factor. The variable in bivariate analysis with p-value <0.25 was entered into multivariate logistic regression. Besides, model fitness was checked with Hosmer‐Lemeshow goodness‐of‐fit test (p > 0.05). A statistically significant association was declared at a P-value less than 0.05 in multivariable logistic regression analysis. The strength of the association of factors with knowledge and practice was demonstrated by computing the Odds Ratio (OR) and the Adjusted Odds Ratio (AOR) with a 95% Confidence Interval (CI).
Results
Socio-Demographic Characteristics of the Respondents
As presented in Table 1, Out of 271 nurses employed in selected hospitals’ working units, 252 nurses gave complete responses yielding a response rate of 93%. Of these, almost 57.1% were females. The mean age was 29.3+3.7, range (24–50 years). The majority of (84.5%) study participants were Bachelor’s degree holders. Nearly 48% of study participants work in CCU. Half of the participants had an intermediate level of work experience and a significant number (76.2%) of the participants did not get in-service training. The majority of the study participants have no access to clinical practice guidelines (87.7%), diagnostic resources (72.6), and treatment resources (69.0%).
 |
Table 1 Socio-Demographic Characteristics of Study Participants (N = 252) |
Nureses’ Knowledge Regarding the Care of ACS
The mean score of the respondent’s knowledge regarding the care of ACS was 54.0%. The percentage of correct responses to individual questions ranged from 22 to 77%. The rate of correct response was higher in knowledge items which is asked about the position recommended for a patient with ACS (76.6%) and lower (22.2%) in items asked concerning the timing of recommended invasive strategy in patients with heart failure-related non-ST-elevation ACS (Table 2).
 |
Table 2 Nurses’ Knowledge of Acute Coronary Syndrome (N = 252) |
Further, our study findings showed the level of nurses’ knowledge regarding ACS. As Presented in Figure 1, out of 252 study participants 121 (48%) of the study participants had poor knowledge and 131 (52%) of participants had good knowledge regarding the care of ACS.
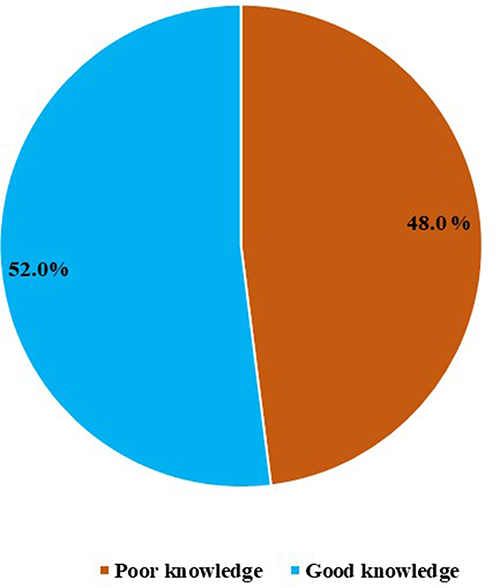 |
Figure 1 Overall knowledge of nurses regarding the care of Acute Coronary Syndrome (n=252). |
Nurses’ Practice Regarding the Care of ACS
The finding of this study revealed that the mean score for nurse’s practice regarding care of acute coronary syndrome was 3.07 with a 5-a-point Likert scale (Table 3). Further, the overall analysis of our study findings showed that only 112 (44.4%) of the study participants had good practice and the remaining 140 (55.6%) had poor practice (Figure 2).
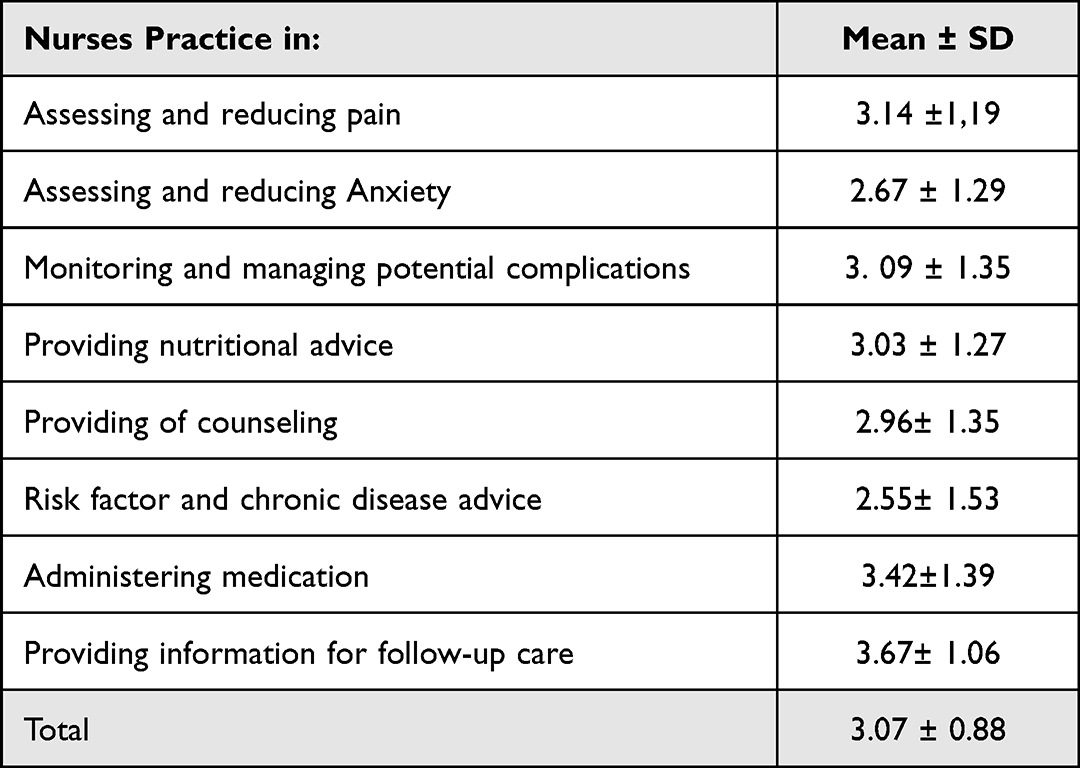 |
Table 3 The Mean of Practice Sub-Scale Responses by Study Participants (N = 252) |
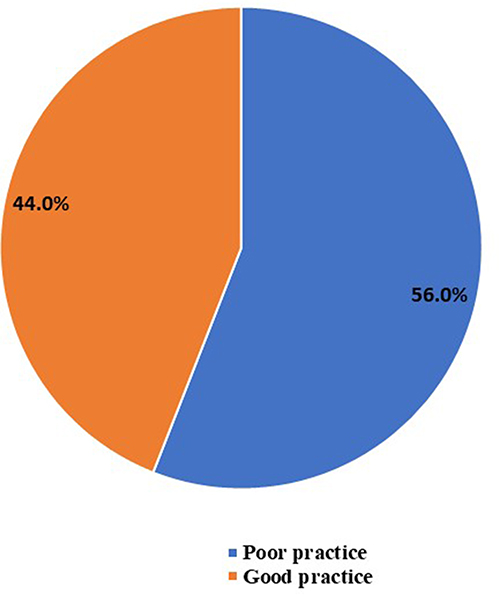 |
Figure 2 Overall practice of nurses regarding the care of Acute Coronary Syndrome (N=252). |
Factors Associated with Nurses’ Knowledge and Practice Regarding Care of ACS
To determine the association of selected variables, we used both bivariate and multivariable logistic regression analysis. In bivariate logistic regression, all variables with a p-value of less than 0.25 were considered as a candidate variable and entered together into a multivariate logistic regression, and a P-value less than 0.05 was taken as a cut point value to be statistically significant. Accordingly, bivariate logistic regression analysis revealed, having a master’s degree [COR=6.454,(95% CI:2.596–16.044), P<0.001], presence of clinical practice guidelines in a working unit [COR=16.917,(95% CI:3.940–72.631), P<0.001] and presence of diagnostic resources [COR= 1.942,(95% CI:1.098–3.435), P= 0.023] were found more likely to have good knowledge of ACS compared to those who were Bachelor degree holder, did not a have clinical practice guideline and diagnostic resource in their working unit respectively. However, working in the emergency department [COR=0.241, (95% CI:0.099–0.590), P= 0.002] and CCU [COR= 0.394, (95% CI:0.164–0.947), P=0.037] were found less likely to have good knowledge regarding ACS compared to those who were working in ICU. Further, the multivariate logistic regression analysis revealed that having master’s degree [AOR=3.801, 95% CI (1.314–10.996), P =0.014] and having clinical practice guidelines in their working unit [AOR= 10.998, 95% CI (2.478–48.805), P =0.002] were found more likely to have good knowledge regarding ACS compared to those who were Bachelor degree holder and those who did not have clinical practice guideline in their working unit respectively (Table 4).
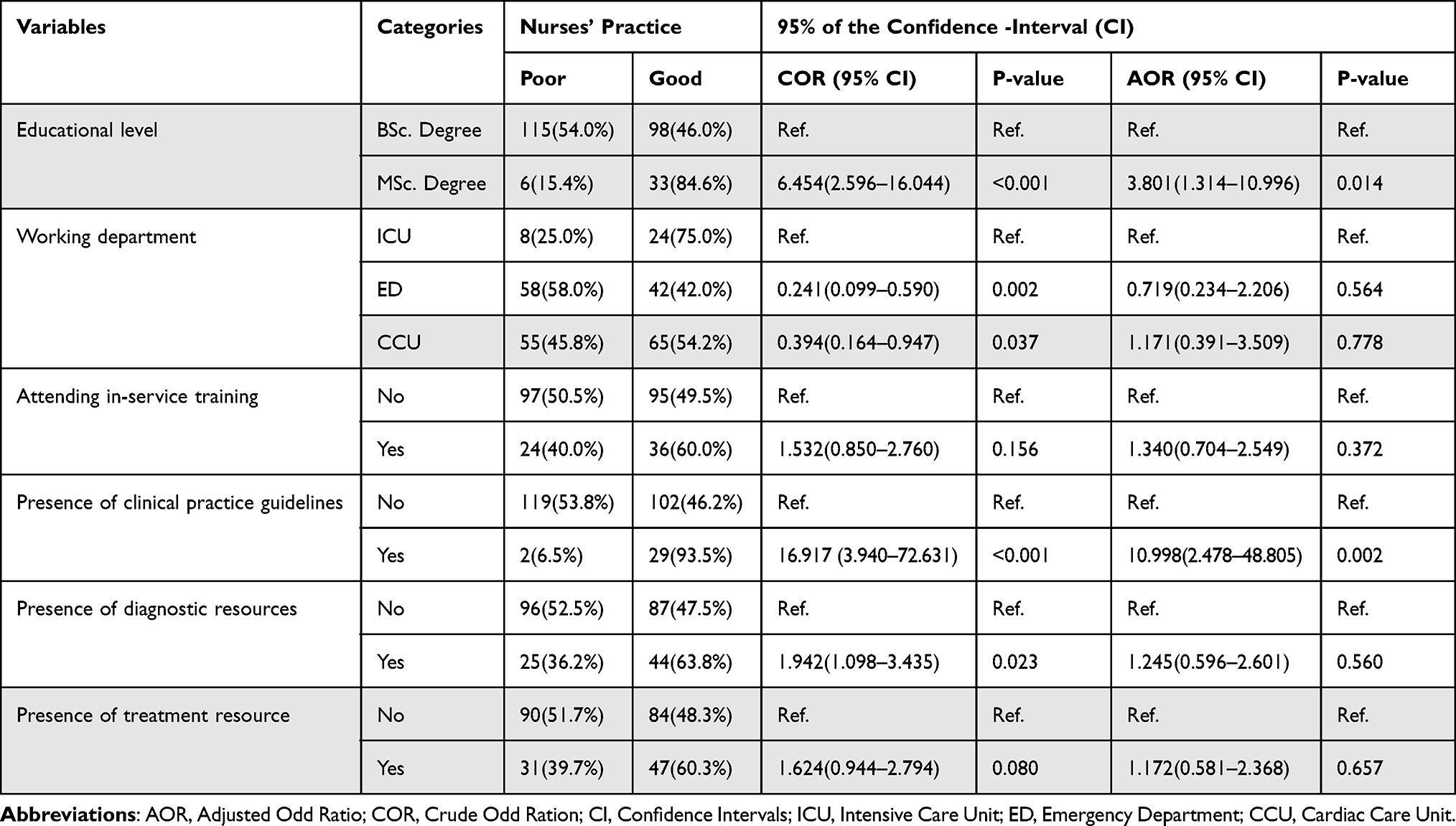 |
Table 4 Knowledge of Nurses and Associated Factors Regarding the Care of ACS (N=252) |
Regarding nurses’ practice towards care ACS, bivariate logistic regression analysis revealed, having a master’s degree (COR=4.633, (95% CI:2.633–10.005), P<0.001) attending in service- training (COR= 2.137, (95% CI:1.186–3.857), P= 0.012) were found more likely to have good practice towards care of the patient with ACS compared to those who were Bachelor degree holder, did not attend in-service training respectively. However, working in the emergency department (COR=0.434(0.192–0.985), P= 0.046) and CCU (COR= 0.41, (95% CI: 0.186–0.924), P=0.031) were found less likely to have good practice towards care of the patient with ACS compared to those who were working in ICU. Then the multivariate logistic regression analysis revealed that the odds of nurses having master’s degrees were found about almost four times higher than those having good practice regarding care of ACS (AOR=4.258, (95% CI:1.676–10.820), P=0.002) than nurses having a bachelor degree. Further, the odds of nurses who attended in-service training were also found about almost two times higher than good practice regarding care of acute coronary syndrome. [AOR= 1.902, (95% CI:1.022–3.539), P = 0.042] than those who did not attend in-service training (Table 5).
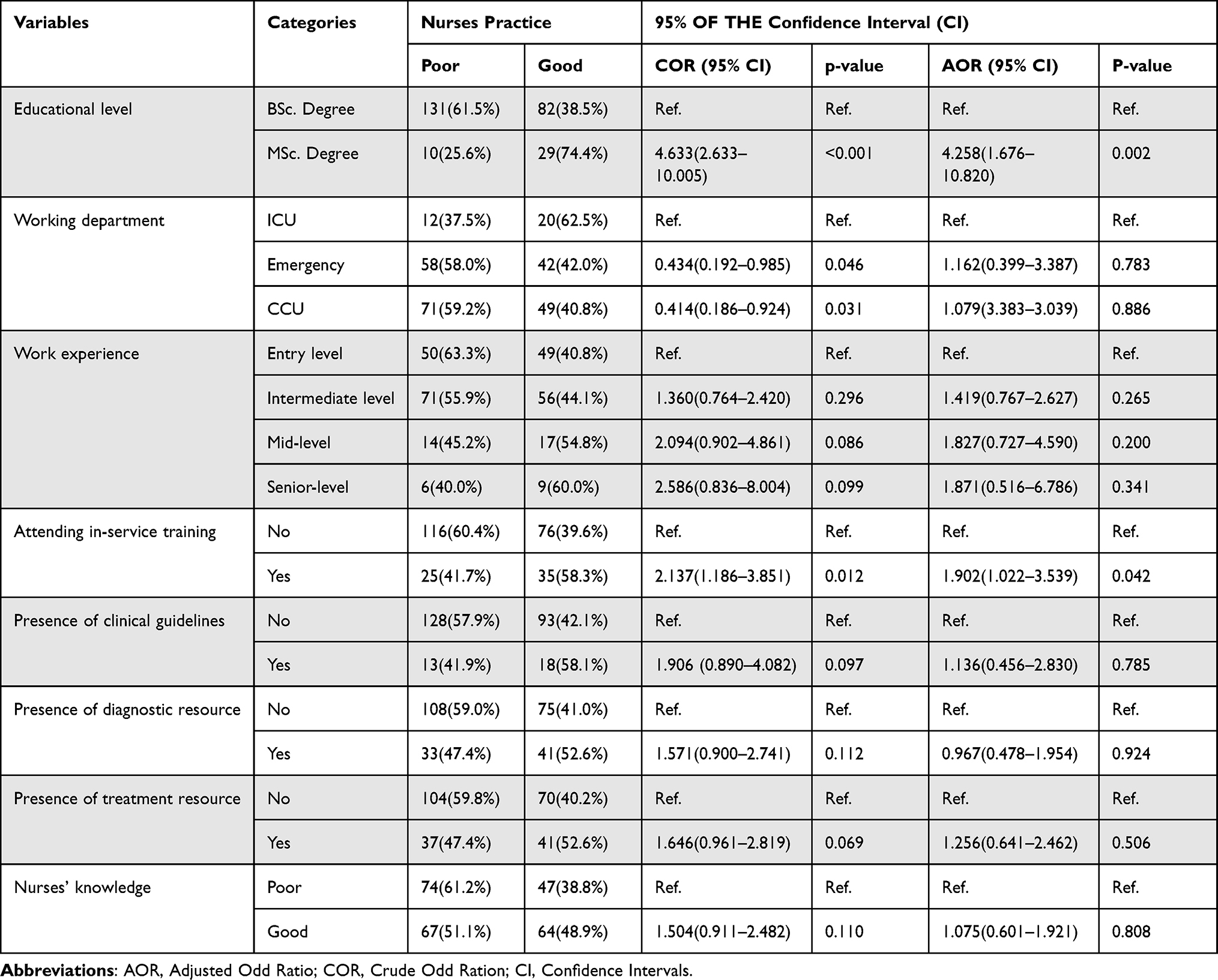 |
Table 5 The Practice of Nurses and Associated Factors Regarding the Care of ACS (N= 252) |
Discussion
Knowledge and practice of acute care nurses towards care of ACS are critical concerns. The main purpose of this research was to examine the overall knowledge and practice of nurses and its associated factors regarding the care of ACS. In both the national and international contexts, studies that specifically aim to address the problems are limited. In the current study, the level of knowledge and practice towards ACS among the study participants is low. The low level of nurses’ knowledge and practice regarding the care of ACS may impact the patient outcome negatively.
The study revealed that (52%) of acute care nurses had a good level of knowledge regarding care for ACS. This was lower than the study done in a developing country, China14 in which (75%) of nurses had a good level of knowledge towards cardiovascular disease risk prevention. But, this finding was higher than a study conducted by Angkachand, Sarosario, and Funk (2011), in which only 38% of cardiac ICU nurses had adequate knowledge regarding ACS.17 The gap in knowledge among acute care nurses may hinder the outcome of patients. Ideally, an acute care nurse should have high-level critical thinking skills and a knowledge base that is vital for independent judgments and timely decision-making skills. Studies suggest that acute care nurses must be expert clinicians who have adequate knowledge to recognize signs, symptoms, and complications of ACS at the earliest stages to improve patient outcome.23,24
In the current study, educational level was an important factor in the level of knowledge. Nurses having a master’s degree were about four times more likely to have adequate knowledge when compared with Bachelor’s degree holders. This finding is supporting that increased educational level had a significant effect on the acquisition of knowledge regarding ACS among acute care nurses.18 Another positive effect of educational level on the promotion of nurses’ knowledge regarding disease management was investigated in a previous study.12 The findings indicate that having a good educational background and participating in continuous professional development, play important roles in helping acute care nurses to provide quality care for patients with ACS. This could be due to the fact that nurses who have more educational status can get more knowledge through the learning process.
It was well established that nursing activities in caring for a patient with ACS should include prevention and objective risk assessment based on evidence-based clinical practice guidelines.11 This study found that acute care nurses who have a guideline in their working department were about eleven times more likely to have adequate knowledge of ACS when compared with nurses who did not have clinical guidelines. This finding was supported by a cross-sectional study done in Northern Ethiopia25 and a mixed study conducted in Nigeria.24 This may be due to study participants reading the clinical guideline by using the opportunity of the presence of the guide in the unit. However, utilizing existing clinical practice guidelines depends on providers’ knowledge and skill. According to a study conducted by Uchmanowicz et al, a few nurses (14%) had a good knowledge of utilizing clinical practice guidelines developed for the management of ACS.2 The lack of knowledge and skill in the utilization of evidence-based clinical guidelines could cause poorer quality of life among patients with ACS.2 Thus, nurses should ensure that patients receive guidelines-based care. Moreover, acute care nurses must utilize up to dated clinical practice guidelines developed for the management of ACS and promote evidence-based practice in the acute care unit.
It has previously been reported that nursing practice could improve patients’ self-care practice attitudes, and beliefs in control of ACS symptoms.13 However, the finding of this study showed only (44%) of study participants had good practice regarding care of the patient with ACS. This finding was significantly lower when compared to a study reported from USA,23 in which the majority of a nurse (75%) had higher accuracy in recommending appropriate actions for patients with ACS symptoms. Another study from the USA revealed that 87% and 52% of acute care nurses frequently ask about chest pain and give analgesics respectively.26 Similarly, in the UK, a study focused on triage nurses to identify better management of high-risk patients with ACS reported a significant improvement in patient outcomes in various aspects of nursing care.22 The difference could be due to the fact that variations in the educational level of the study population, the socioeconomic status of participants, and the policy of the healthcare system. Therefore, nurses must possess a broad range of cognitive and communication skills that will help them function effectively in a critical care department.
The need for better education and in-service- training of nursing staff regarding the care of patients with cardiovascular disease was suggested in prior studies.18,19 The finding of this study revealed that nurses who had master’s degrees were four times higher to have good practice regarding the care of ACS than nurses having bachelor’s degrees. This finding was in line with the study conducted by La Sala et al.19 In fact, it is well-established that the level of knowledge and scope of nursing practice increases with an increment of educational level.12,18 More educated people are usually more willing to improve their skills in providing appropriate care for a patient with chronic diseases like ACS. The current study has also revealed that nurses who attended in-service training about ACS had a significantly higher level of practice than those who did not. This result was supported by studies done in Italy19 and Iran27 suggesting that in-service training significantly improves nurses’ knowledge and practice in outcomes of patients with cardiovascular disease including ACS. This could be the fact that attending in-service training play a vital role in increasing the tendency to learn more knowledge and skill about the management of the disease. Moreover, updating the knowledge of acute care nurses through training could improve the older understanding and help to develop new knowledge and skill in disease management.
Unlike the study conducted in South Korea28 and USA23, this study found no statistically significant association between work experience and nursing practice in the care of patients with ACS. A possible justification for this variation might be due to the small sample size, study population, and study design. In general, this study showed that the majority of acute care nurses had poor knowledge and practice regarding the care of ACS. This might be due to lower educational levels, lack of getting training, and absence of clinical guidelines in their working unit. In our study, a significant number (84.5%) of study participants were bachelor’s degree holders, 76.2% did not get in-service training about the care of ACS and 50.4% had an intermediate duration of work experience. In addition, it might also be due to poor health infrastructure (such as the absence of clinical practice guidelines, and diagnostic and treatment resources) of the health institutions in the study areas.
Conclusion and Recommendations
The study concluded a significant number of the study participants have suboptimal knowledge and practice regarding the care of ACS. This finding is bothersome, in the presence of a high prevalence of cardiac patient mortality in the country. Further; the study found, nurses’ educational level, presence of clinical practice guidelines in working units, and getting in-service training were determinant factors associated with nurses’ good knowledge and practice regarding the care of ACS. Therefore, there should be an intervention that mediates the factors affecting the knowledge and practice level of nurses regarding the care of ACS. Organizational and nursing educational support was needed to improve this gap by providing continuous training, creating awareness, and enhancing nurses’ abilities for the utilization of evidence-based clinical practice guidelines. Nurses should update their knowledge regarding the care of ACS through reading and learning from various resources like textbooks and internet-based online resources. Researchers should carry out further studies by using observational study designs to identify actual practices.
Limitations of the Study
This study has some limitations. First, this study used a self-administered questionnaire, so there could be social desirability and recall bias. Second, no adequate literature was found on a similar topic, especially in the Ethiopian context making it difficult to compare. Third, since we used a cross-sectional study design, the direction of the relationship between variables cannot always be determined.
Abbreviations
ACS, Acute Coronary Syndrome; AOR, Adjusted Odds Ratio; CCU, Cardiac Care Unit; COR, Crude Odds Ratio; CVD, Cardiovascular Disease; ED, Emergency Department; ICU, Intensive Care Unit; MI, Myocardial Infarction; SPSS, Statistical Package for Social Science; UK, United Kingdom; USA, United State of America.
Data Sharing Statement
The data of this study can be available for reasonable request from the corresponding author.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Research Ethical Review Board (IRERB), College of Health Science, Addis Ababa University, with meeting number: 01/2013 E.C and protocol number: 12/21/SNM. Before the commencement of the study, both written and verbal consent were obtained from each respondent based on their educational level. All data collection activities were carried out in accordance with the declaration of Helsinki. The study’s objectives and significance were explained to the participants. All study participants were informed that their participation in the study was voluntary and they had the right to withdraw from the study at any time they wanted. To ensure participants’ confidentiality and anonymity, codes, and identification numbers were used in survey questionnaires. The collected data were stored and kept on a password-protected computer. Only the principal investigator had access to the computerized data.
Acknowledgments
We would also like to express our gratitude to the medical directors and managers of each hospital for their unreserved support. We also thank the study participants for their valuable time. Last but not least we would like to express our gratitude to the reviewer of this manuscript for their valuable comment and suggestion that helped us improve the paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Disclosure
This paper is based on the thesis of Bizuayehu Ashine Lakew. It has been recorded on the Addis Ababa University Institutional Repository (http://etd.aau.edu.et/handle/123456789/28423). The authors report no conflicts of interest in this work.
References
1. D’Souza E. An overview and awareness of acute coronary syndrome based on risk factors, early clinical assessment tools, and improving clinical outcomes. J Dr Nurs Pract. 2019;12(1):125–131. doi:10.1891/2380-9418.12.1.125
2. Uchmanowicz I, Wleklik M, Hill L, et al. BeGuideWell: a prospective cross-sectional study analyzing the awareness and opinions of nursing students in Poland on the usefulness of European Society of Cardiology guidelines in the post-graduate education program. Eur J Cardiovasc Nurs. 2019;18(7):601–610. doi:10.1177/1474515119851615
3. Yuan L, Yuan L. Effectiveness of nursing intervention on anxiety, psychology, and self-efficacy among elderly patients with acute coronary syndrome after percutaneous coronary intervention: an observational cohort study. Medicine. 2021;100(33):e26899. doi:10.1097/MD.0000000000026899
4. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
5. Adem F, Abdi S, Amare F, Mohammed MA. In-hospital mortality from acute coronary syndrome in Africa: a systematic review and meta-analysis. SAGE Open Med. 2023;11:20503121221143646. doi:10.1177/20503121221143646
6. Bogale K, Mekonnen D, Nedi T, Woldu MA. Treatment outcomes of patients with acute coronary syndrome admitted to Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. Clin Med Insights Cardiol. 2019;13:1179546819839417. doi:10.1177/1179546819839417
7. N’Guetta R, Yao H, Ekou A, et al. Prevalence and characteristics of acute coronary syndromes in a sub-Saharan Africa population. Ann Cardiol Angeiol. 2016;65(2):59–63. doi:10.1016/j.ancard.2016.01.001
8. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139–e228. doi:10.1016/j.jacc.2014.09.017
9. Serrano-Rosa M, León-Zarceño E, Giglio C, et al. Psychological state after an acute coronary syndrome: impact of physical limitations. Int J Environ Res Public Health. 2021;18(12):6473. doi:10.3390/ijerph18126473
10. Paoli G, Notarangelo MF, Mattioli M, et al. Alliance for sEcondary PREvention after an acute coronary syndrome. The ALLEPRE trial: a multicenter fully nurse-coordinated intensive intervention program. Am Heart J. 2018;203:12–16. doi:10.1016/j.ahj.2018.06.001
11. Tierney S, Cook G, Mamas M, Fath-Ordoubadi F, Iles-Smith H, Deaton C. Nurses’ role in the acute management of patients with non-ST-segment elevation acute coronary syndromes: an integrative review. Eur J Cardiovasc Nurs. 2013;12(3):293–301. doi:10.1177/1474515112451555
12. Schultz WM, Kelli HM, Lisko JC, et al. Socioeconomic status and cardiovascular outcomes: challenges and interventions. Circulation. 2018;137(20):2166–2178. doi:10.1161/CIRCULATIONAHA.117.029652
13. Darsin Singh SK, Ahmad A, Rahmat N, Hmwe NTT. Nurse-led intervention on knowledge, attitude, and beliefs towards acute coronary syndrome. Nurs Crit Care. 2018;23(4):186–191. doi:10.1111/nicc.12240
14. Ding S, Deng Y, Lu S, Lamb KV, Zhang Y, Wu Y. Knowledge and practice in cardiovascular disease prevention among hospital registered nurses: a cross-sectional study. J Clin Nurs. 2017;26(21–22):3318–3327. doi:10.1111/jocn.13678
15. Hosseinzadeh T, Tabrizi KN, Fallahi-Khoshknab M, Khankeh H, Shokooh F. Barriers to the development of clinical reasoning skills among coronary care nurses: a Qualitative Study. Iran J Nurs Midwifery Res. 2022;27(6):567–574. doi:10.4103/ijnmr.ijnmr_164_21
16. Pelter MM, Carey MG, Stephens KE, Anderson H, Yang W. Improving nurses’ ability to identify the anatomic location and leads on 12-lead electrocardiograms with ST-elevation myocardial infarction. Eur J Cardiovasc Nurs. 2010;9(4):218–225. doi:10.1016/j.ejcnurse.2010.01.005
17. Sangkachand P, Sarosario B, Funk M. Continuous ST-segment monitoring: nurses’ attitudes, practices, and quality of patient care. Am J Crit Care. 2011;20(3):226–237; quiz 238. doi:10.4037/ajcc2011129
18. Fitzsimons D, Carson MA, Hansen TB, Neubeck L, Tanash MI, Hill L. The varied role, scope of practice, and education of cardiovascular nurses in ESC-affiliated countries: an ACNAP survey. Eur J Cardiovasc Nurs. 2021;20(6):572–579. doi:10.1093/eurjcn/zvab027
19. La Sala R, Dicembrino RB, Dall’Argine S, et al. Nurse training in self-management of patients with cardiovascular diseases: a multicentre observational study. Acta Biomed. 2017;88(5S):22–30. doi:10.23750/abm.v88i5-S.6882
20. Bahiru E, Temu T, Mwanga J, et al. Facilitators, the context of and barriers to acute coronary syndrome care at Kenyatta National Hospital, Nairobi, Kenya: a qualitative analysis. Cardiovasc J Afr. 2018;29(3):177–182. doi:10.5830/CVJA-2018-013
21. Jarvis SS. Diagnosis, management and nursing care in acute coronary syndrome. Nurs Times. 2017;113:31–35.
22. O’Neill L, Smith K, Currie P, Elder D, Wei L, Lang C. Nurse-led Early Triage (NET) study of chest pain patients: a long-term evaluation study of a service development aimed at improving the management of patients with non-ST-elevation acute coronary syndromes. Eur J Cardiovasc Nurs. 2014;13(3):253–260. doi:10.1177/1474515113488026
23. Davis LL, Maness JJ. Nurse practitioner knowledge of symptoms of acute coronary syndrome. J Nurse Pract. 2019;15(1):e9–e12. doi:10.1016/j.nurpra.2018.09.017
24. Odunaiya NA, Akinpelu AO, Ogwu S, Aje A. Healthcare professionals’ perception of quality of care of patients with cardiac disease in Nigeria: implication for a clinical guideline, inter-professional education, and teamwork. Malawi Med J. 2019;31(1):31–38. doi:10.4314/mmj.v31i1.6
25. Biset G, Habte T, Dugasa B, Bizuwork K. Nurses’ and midwives’ knowledge regarding neonatal resuscitation in public hospitals of south Wollo zone of Amhara Region, Northern Ethiopia. Int J Afr Nurs Sci. 2023;18:100527. doi:10.1016/j.ijans.2023.100527
26. Arslanian-Engoren C, Eagle KA, Hagerty B, Reits S. Emergency department triage nurses’ self-reported adherence with American College of Cardiology/American Heart Association myocardial infarction guidelines. J Cardiovasc Nurs. 2011;26(5):408–413. doi:10.1097/JCN.0b013e3182076a98
27. Gholami M, Fayazi M, Hosseinabadi R, Anbari K, Saki M. Effect of triage training on nurses’ practice and triage outcomes of patients with acute coronary syndrome. Int Emerg Nurs. 2023;68(68):101288. doi:10.1016/j.ienj.2023.101288
28. Kim MS, Kim HJ, Choi JE, Kim SJ, Chang SO. Nursing home nurses conceptualize how to care for residents with cardiac vulnerability. Nurs Crit Care. 2017;22(6):329–338. doi:10.1111/nicc.12132
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.