")
Back to Journals » Biologics: Targets and Therapy » Volume 18
Successful Response to Golimumab in a Case of Relapsing Polychondritis Overlapping with Ulcerative Colitis
Authors Kojima S , Matsumoto S, Koito Y, Miura T, Sekine M, Uehara T, Asano T, Yamaguchi Y, Mashima H
Received 21 August 2023
Accepted for publication 6 January 2024
Published 12 January 2024 Volume 2024:18 Pages 1—6
DOI https://doi.org/10.2147/BTT.S436301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Shein-Chung Chow
Shu Kojima,1 Satohiro Matsumoto,1 Yudai Koito,1 Takaya Miura,1 Masanari Sekine,1 Takeshi Uehara,1 Takeharu Asano,1 Yasuhiro Yamaguchi,2 Hirosato Mashima1
1Department of Gastroenterology, Jichi Medical University Saitama Medical Center, Saitama, Japan; 2Department of Respiratory Medicine, Jichi Medical University Saitama Medical Center, Saitama, Japan
Correspondence: Shu Kojima, Department of Gastroenterology, Jichi Medical University Saitama Medical Center, 1-847 Amanuma, Omiya, Saitama, 330-8503, Japan, Tel +81 48 647 2111, Fax +81 48 648 5188, Email [email protected]
Abstract: A 51-year-old Japanese man was diagnosed with left-sided ulcerative colitis (UC) at age 41. He was treated with mesalazine and azathioprine and maintained remission. At age 51, the patient developed bloody stools, abdominal pain, scleritis, arthritis, cough, bloody sputum, and pericardial effusion. Considering that pericardial effusion is an atypical extraintestinal complication of UC, and the patient met the diagnostic criteria for relapsing polychondritis (RP), a diagnosis of RP complicating a relapse of UC was made. Steroid therapy was administered, and both diseases improved. Golimumab, an anti-tumor necrosis factor-α inhibitor, was introduced as maintenance therapy for UC. All symptoms, including pericardial effusion, improved. Subsequently, no relapse of UC or RP was observed. As only a few cases of RP overlapping with UC have been reported and no treatment protocol has been established, we considered this case valuable and worthy of publication.
Keywords: ulcerative colitis, relapsing polychondritis, anti-tumor necrosis factor-α inhibitor, golimumab
Introduction
Relapsing polychondritis (RP) is a rare disease of unknown etiology that involves chronic and recurrent inflammation of cartilage tissues such as the ears, nose, eyes, joints, trachea, heart, and blood vessels, as well as collagen-rich tissues.1 Auricular chondritis and inflammation of airway, nasal, and articular cartilages are predominant, and eye inflammation also develops. The patient presents with symptoms similar to the extraintestinal manifestations of UC, such as eye inflammation and arthralgia. Approximately 30% of RP cases have concomitant other autoimmune diseases such as rheumatoid arthritis, systemic lupus erythematosus, and Sjögren’s syndrome,2 but there are few reports of RP overlapping with UC. RP is considered an autoimmune disease of the cartilage structures, and the goal of treatment is to control inflammation over a long period of time, often with prednisolone or immunosuppressants. Anti-TNF-α inhibitors have been used for rheumatoid arthritis and inflammatory bowel disease, and the indication is expanding to other inflammatory diseases. The efficacy of anti-tumor necrosis factor (TNF)-α inhibitors for RP has been reported, and a systematic review of the literature reported that anti-TNF-α inhibitors were used in 43 cases, of which infliximab was used in 31 cases and 18 cases had treatment response.3 However, no standard treatment protocols have been established for cases of RP overlapping with UC.
Case Report
In a 51-year-old Japanese man, diarrhea and bloody stools developed at age 41. A blood test revealed an increased inflammatory reaction with white blood cell (WBC) count of 11,400/μL and C-reactive protein (CRP) of 125.0 mg/L, and a colonoscopy was performed. Based on the clinical symptoms, endoscopic findings and the results of the biopsy, the patient was diagnosed with left-sided UC. Remission was maintained with mesalazine (3600 mg/day) and azathioprine (75 mg/day) for UC. At the age of 51, the patient developed bloody stools, abdominal pain, hyperemia of the bulbar conjunctiva of the left eye without discharge, and arthralgia. One month later, he developed cough and bloody sputum, and made an outpatient visit. He had 5–6 bloody bowel movements per day, and the blood test results showed a high inflammatory reaction of WBC count of 14,330/μL and CRP of 334.1 mg/L, suggesting a relapse of UC and extraintestinal complications of UC. Chest computed tomography (CT) revealed thickening of the tracheal wall, lumen stenosis, and pericardial effusion (Figure 1). There was no chest pain, and chest auscultation and electrocardiogram showed no abnormalities. Redness was found on the left bulbar conjunctiva, and arthralgia with tenderness was observed on the right shoulder, left knee, and right foot. The redness of the left ocular conjunctiva had already been diagnosed as scleritis by an ophthalmologist, and the asymmetric joint pain in multiple locations was considered to be polyarthritis because it was also accompanied by tenderness. Regarding the joints, there were no symptoms, such as morning stiffness. Various autoantibodies submitted for differential diagnosis including rheumatic diseases were negative (Table 1). Bronchoscopy revealed stenosis of the trachea 2–3 cm from the glottis to before the tracheal bifurcation, edematous mucosa with redness of the anterior wall and no specific findings in the membranous portion (Figure 2). Biopsy pathology results from the edematous mucosa with erythema of the anterior tracheal wall showed the formation of granulation tissue under the epithelium, which was considered to be a secondary change associated with inflammation of the ventrally located airway cartilage, suggesting tracheochondritis. Since UC is rarely associated with airway involvement and pericardial effusion, other disease than extraintestinal complication of UC was suspected. The diagnosis of RP complicating a relapse of UC was made because the patient met the diagnostic criteria proposed by McAdam et al4 and revised by Damiani et al5 for nonerosive polyarthritis, scleritis, and tracheochondritis. Mesalazine and azathioprine were continued at the original doses, and prednisolone was initiated at a dose of 20 mg (0.25 mg/kg), and bloody stools, arthralgia, cough, and bloody sputum all markedly improved. Prednisolone was tapered by 5 mg at weekly intervals and completed after 6 weeks. Subsequently, the interval and route of administration of an anti-TNF-α inhibitor were discussed with the patient, and golimumab was introduced as maintenance therapy for UC, which can be injected subcutaneously with relatively long intervals. Echocardiography performed one-month post-administration of golimumab revealed no significant findings of valvular heart disease or pericardial effusion. Two months after golimumab administration, chest CT showed improvement of tracheal wall thickening and tracheal lumen narrowing, disappearance of pericardial effusion (Figure 3), and improvement of inflammatory response to WBC 4710/µL and CRP 6.6 mg/L on blood test. The 4-weekly administration of golimumab is currently being continued. Three years to date, the patient remains free of relapse of UC or RP.
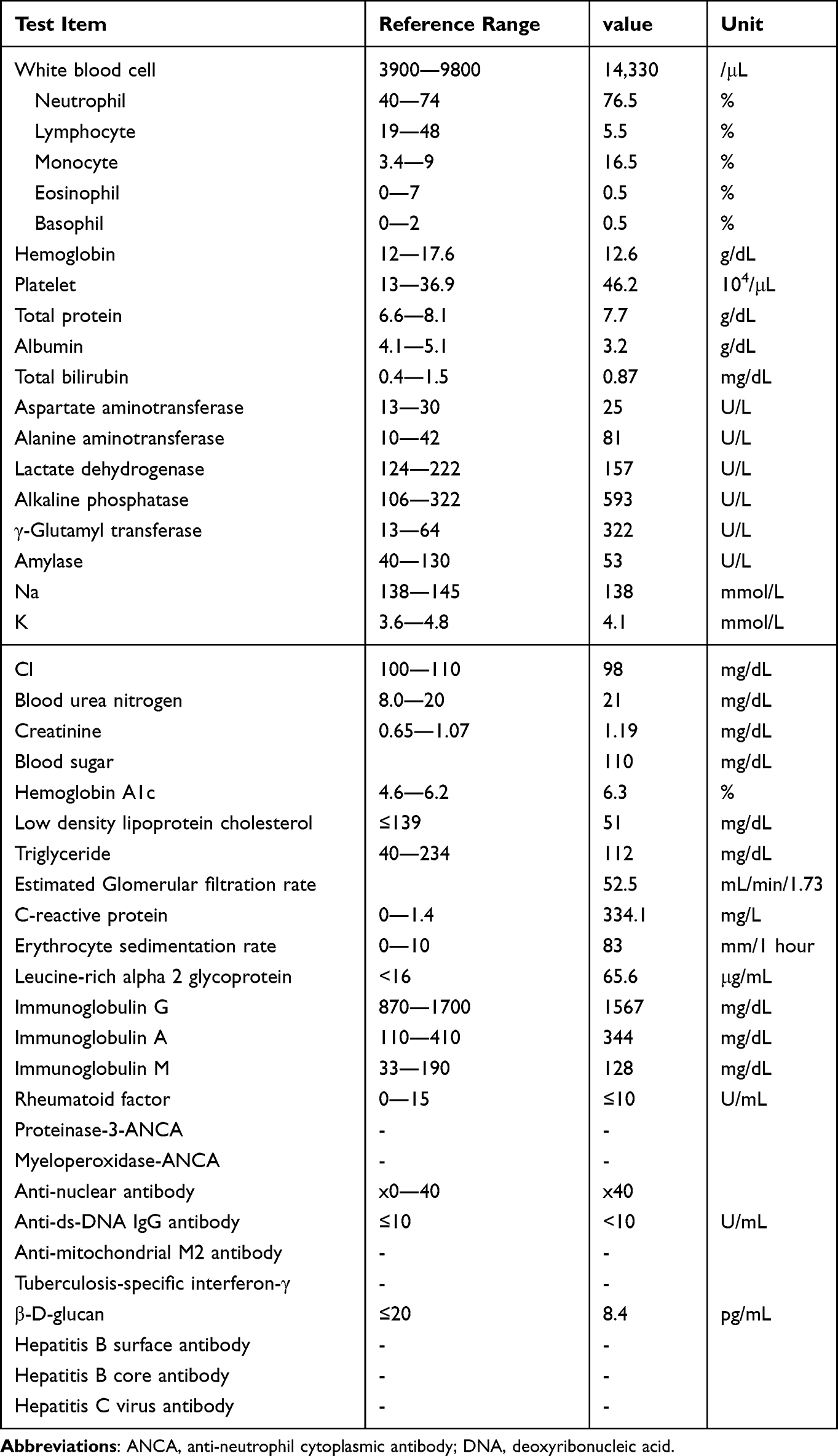 |
Table 1 Laboratory Findings |
 |
Figure 1 Pre-treatment contrast chest CT image. Tracheal wall thickening and narrowing of the tracheal lumen (a and b) and pericardial effusion (c) were observed. |
 |
Figure 2 Bronchoscopic image. Mucosa before the tracheal bifurcation was edematous and erythematous. |
 |
Figure 3 Post-treatment contrast chest CT image. Tracheal wall thickening and tracheal lumen narrowing improved (a and b) and pericardial effusion disappeared (c). |
Discussion
Clinical manifestations of RP involve six areas: bilateral auricular chondritis, non-erosive seronegative polyarthritis, nasal chondritis, eye inflammation, airway chondritis, and vestibulocochlear dysfunction. According to the diagnostic criteria of McAdam et al, diagnosis of RP is made when three or more of them are met, or when other causes such as infectious chondritis are excluded even if three of them are not met.4 Damiani et al reported that a definitive diagnosis of RP can be made based on a single symptom and histological diagnosis or when two sites of chondritis respond to prednisolone or diaphenylsulfone even if three of the criteria are not met.5 The patient had scleritis, respiratory tract chondritis, and nonerosive sero-negative inflammatory polyarthritis, and then we diagnosed RP with UC relapse.
As a relapse of UC was initially observed, respiratory symptoms, scleritis, and joint symptoms were considered extraintestinal complications of UC. However, cardiovascular disease is rare as an extraintestinal complication of inflammatory bowel disease (IBD), and pericardial effusion was considered an atypical extraintestinal complication. Conversely, RP can be complicated by cardiovascular lesions, in addition to auricular chondritis, arthritis, and tracheochondritis, and these complications can exist in 24–52% of patients with RP.6 Cardiovascular lesions associated with RP include valvular heart disease, aortic aneurysm, aortic dissection, myocarditis, pericarditis, atrioventricular block, and systemic vasculitis.1 In this case, there was no chest pain or electrocardiographic abnormalities, and acute pericarditis was unlikely. Although the cause of the pericardial effusion was not clear, various autoantibodies and microbiological antibodies submitted for differential diagnosis were all negative. Then, we believe that microbiological etiologies and other autoimmune diseases including ANCA associated vasculitis were ruled out. The patient was also taking sitagliptin and allopurinol, rosuvastatin, and esomeprazole, all of which, including mesalazine, had been continued for a long period, so pharmacological etiologies, including drug-induced lupus erythematosus, were unlikely. Steroid treatment improved the patient’s pericardial effusion. This may be due to the improvement of systemic inflammation with steroid therapy rather than cardiovascular involvement of RP.
The present patient started treatment with prednisolone for UC relapse and RP. Considering that anti-TNF-α inhibitors would be introduced after tapering of prednisolone, golimumab was selected. Treatment with prednisolone improved bloody stools, joint symptoms, and cough, and remission was achieved for UC and RP. Remission for both UC and RP was maintained with golimumab even after the completion of treatment with prednisolone.
There have been several reported cases of RP complicating UC7–13 (Table 2), and all of them had been treated with prednisolone. However, prevention of further relapse of RP and maintenance therapy for UC have not been mentioned except in the report by Kawano et al.12 Anti-TNF-α inhibitors may be useful for the prevention of further relapse of RP.14 According to the report, when the effects of biological agents were compared for each organ lesion of RP, anti-TNF-α inhibitors were effective for joint lesions and tocilizumab or anti-TNF-α inhibitors were effective for airway lesions.15 Both UC and RP, which are autoimmune diseases, may share common pathological conditions. TNF-α increases in the inflammatory phase of both UC and RP.16 In UC, the mechanism by which TNF-α induces inflammation in the intestinal tract is being identified, while in RP, the autoimmune response of the Th1 phenotype has been suggested to generate a TNF-α-driven inflammatory cascade.17 These results suggest the efficacy of anti-TNF-α inhibitors in both UC and RP.
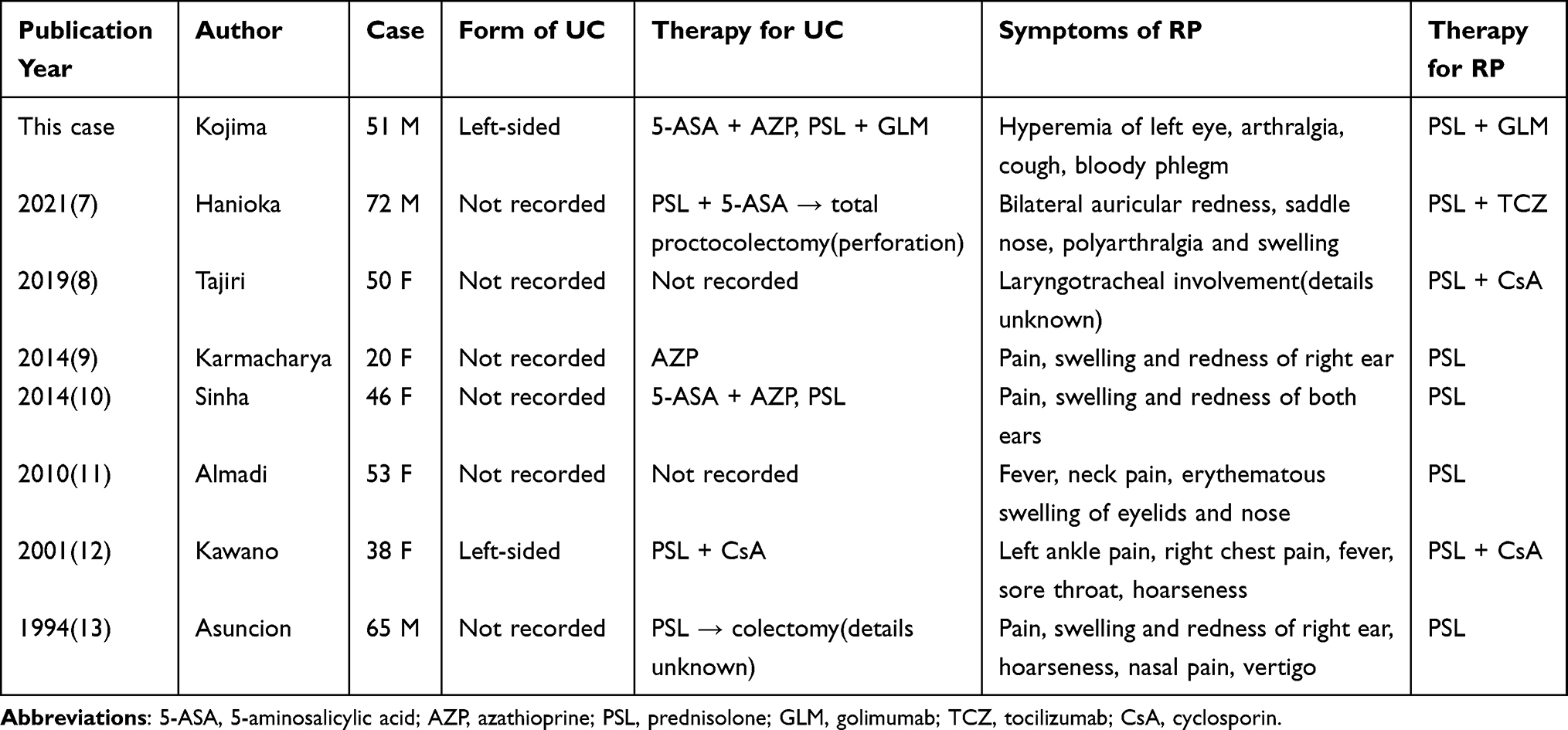 |
Table 2 Cases of Relapsing Polychondritis Associated with Ulcerative Colitis |
Conclusion
As some of the symptoms of extraintestinal complications of UC are similar to those of RP, it is often difficult to make the diagnosis of RP. Autoimmune diseases such as UC may coexist with other autoimmune diseases; thus, meticulous attention should be paid to the existence of similar symptoms. Anti-TNF-α inhibitors can be a therapeutic option for patients with RP overlapping with UC.
Institutional Approval
No institutional approval was required for the publication of this manuscript.
Ethical Considerations
Written informed consent was obtained from the patient for publication of this Case Report and the accompanying images.
Funding
This article has no funding source.
Disclosure
The authors have no conflicts of interest in this work.
References
1. Borgia F, Giuffrida R, Guarneri F, Cannavò SP. Relapsing polychondritis: an updated review. Biomedicines. 2018;6(3):84. doi:10.3390/biomedicines6030084
2. Rednic S, Damian L, Talarico R, et al. Relapsing polychondritis: state of the art on clinical practice guidelines. RMD Open. 2018;4(Suppl 1):e000788. doi:10.1136/rmdopen-2018-000788
3. Kemta Lekpa F, Kraus VB, Chevalier X. Biologics in relapsing polychondritis: a literature review. Semin Arthritis Rheum. 2012;41(5):712–719. doi:10.1016/j.semarthrit.2011.08.006
4. McAdam LP, O’Hanlan MA, Bluestone R, Pearson CM. Relapsing polychondritis: prospective study of 23 patients and a review of the literature. Medicine. 1976;55(3):193–215. doi:10.1097/00005792-197605000-00001
5. Damiani JM, Levine HL. Relapsing polychondritis--report of ten cases. Laryngoscope. 1979;89(6 Pt 1):929–946. doi:10.1288/00005537-197906000-00009
6. Del Rosso A, Petix NR, Pratesi M, Bini A. Cardiovascular involvement in relapsing polychondritis. Semin Arthritis Rheum. 1997;26(6):840–844. doi:10.1016/s0049-0172(97)80028-5
7. Hanioka Y, Shimizu K, Yamagami K, et al. Exacerbation of ulcerative colitis with tocilizumab: a report of two cases, one with takayasu arteritis and the other with relapsing polychondritis. Intern Med. 2021;60(10):1615–1620. doi:10.2169/internalmedicine.5215-20
8. Tajiri M, Tominaga M, Kinoshita T, et al. Clinical characteristics of relapsing polychondritis: a report of 8 cases in Japan. Kurume Med J. 2019;65(2):47–53. doi:10.2739/kurumemedj.MS652006
9. Karmacharya P, Pathak R, Shrestha P, Alweis R. The red hearing: swollen ear in a patient with ulcerative colitis. J Community Hosp Intern Med Perspect. 2014;4(3):1. doi:10.3402/jchimp.v4.24659
10. Sinha N, Gallant C, Walsh NM. A case of red ears. Relapsing polychondritis. Am J Dermatopathol. 2014;36(2):158–185. doi:10.1097/DAD.0b013e3182a4153a
11. Almadi MA, Alenizi AT, Menard HA, Hilzenrat N. Relapsing polychondritis and ulcerative colitis. Saudi J Gastroenterol. 2010;16(1):49. doi:10.4103/1319-3767.58770
12. Kawano Y, Okamoto T, Okubo S, et al. Nihon. Naika Gakkai Zasshi. 2001;90(11):2279–2281. doi:10.2169/naika.90.2279
13. Asuncion AM, Federman DG, Kirsner RS. Swelling of the ear in a patient with ulcerative colitis. Arthritis Rheum. 1994;37(3):432–434. doi:10.1002/art.1780370319
14. Kingdon J, Roscamp J, Sangle S, D’Cruz D. Relapsing polychondritis: a clinical review for rheumatologists. Rheumatology. 2018;57(9):1525–1532. doi:10.1093/rheumatology/kex406
15. Moulis G, Pugnet G, Costedoat-Chalumeau N, et al. Efficacy and safety of biologics in relapsing polychondritis: a French national multicentre study. Ann Rheum Dis. 2018;77(8):1172–1178. doi:10.1136/annrheumdis-2017-212705
16. Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med. 2011;365(18):1713–1725. doi:10.1056/NEJMra1102942
17. Buckner JH, Van Landeghen M, Kwok WW, Tsarknaridis L. Identification of type II collagen peptide 261-273-specific T cell clones in a patient with relapsing polychondritis. Arthritis Rheum. 2002;46(1):238–244. doi:10.1002/1529-0131(200201)46:1<238::AID-ART10030>3.0.CO;2-M
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.