")
Back to Journals » Journal of Blood Medicine » Volume 15
Survival and Treatment Outcomes of Childhood Acute Lymphoblastic Leukemia in a Low-Middle Income Country: A Single-Center Experience in West Java, Indonesia
Authors Ramadhan MH , Sari NM , Peryoga SU, Susanah S
Received 31 August 2023
Accepted for publication 18 January 2024
Published 19 February 2024 Volume 2024:15 Pages 77—85
DOI https://doi.org/10.2147/JBM.S438042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Monika Hasna Ramadhan, Nur Melani Sari, Stanza Uga Peryoga, Susi Susanah
Department of Child Health, Faculty of Medicine Universitas Padjadjaran/Dr. Hasan Sadikin Hospital, Bandung, Indonesia
Correspondence: Susi Susanah, Department of Child Health Faculty of Medicine Universitas Padjadjaran/Dr. Hasan Sadikin Hospital, Jalan Pasteur No. 38, Bandung, Indonesia, Tel/Fax +6222 2034953, Email [email protected]
Purpose: This study aimed to determine the survival rates and treatment outcomes of patients with childhood Acute Lymphoblastic Leukemia (ALL) in a single-center study at Indonesia.
Patients and Methods: Factors contributing to the relapse and survival of ALL in Bandung, Indonesia, were evaluated. Data were collected from the medical record and the Indonesian Pediatric Cancer Registry (IPCAR). Subsequently, univariate and multivariate analyses were evaluated using Cox proportional hazard regression and Kaplan Meier was used for survival analysis. An analytic observational study was conducted on newly diagnosed children aged 1– 18 with ALL from January 2019 to December 2022.
Results: A total of 137 children were included in the analysis, 30 (21,9%) were dropped out during treatment and 60.5% died during the study period. Most of the deaths occurred after relapse in 32 (38.5%) with a high early relapse (70.5%), occurring mainly during the maintenance phase (42.4%). At the one-year mark, the observed overall survival (OS) rate was at 36%, while event-free survival (EFS) was lower, at 19%. Univariate Cox regression analysis showed that the leucocyte counts at diagnosis (p=0.005) and response to induction phase (p < 0.008) was associated with the death of ALL. Furthermore, a response to induction phase was significant [hazard ratio 4.67 (CI 95%: 1.64– 13.29); p = 0.004] in the multivariate analysis.
Conclusion: In conclusion, this study underscored the persistent challenges of high treatment discontinuation rates and the occurrence of very early relapses in low- to middle-income countries (LMICs), which significantly impacted the OS of children diagnosed with ALL.
Keywords: acute lymphoblastic leukemia, children, low-middle income country, relapse, survival
Introduction
Childhood cancer is a global concern that showcases varying survival rates depending on geographical location. In high-income countries, the survival of childhood cancer was more than 80%, while in low- and middle-income countries (LMIC) survival rate was only about 20%.1 Acute Lymphoblastic Leukemia (ALL) is the most common childhood cancer, and its survival rate has significantly increased in the last two decades, with more than 90% in high-income countries. This has also improved in LMIC, although comprehensive data on global ALL survival in LMICs remain limited.2 Several studies in Indonesia showed a survival rate of childhood ALL between 20% and 60%.3–5
The mortality of ALL primarily occurs during or even before the induction phase. Prognostic factors play a pivotal role in treatment risk stratification, predicting treatment outcomes, the possibility of failure, and the risk of relapse. The goal of treatment risk stratification is to enhance survival by increasing the intensity of therapy. Several known prognostic factors in ALL were age at diagnosis, gender, initial leucocyte count, mediastinal mass, central nervous system (CNS) involvement, and response to initial therapy or induction phase.6–9 Minimal residual disease (MRD) using flow cytometry emerged as a strong predictor of outcome and relapse. However, MRD was not a routine examination due to limited facilities, particularly in Indonesia.10,11
Managing ALL in LMIC comes across challenges to improve outcomes and increase survival. To increase the survival of ALL, survival hinges on designed risk-based therapies rooted in prognostic factors that influence the outcome. Strategic selection of treatment intensity during the induction phase mitigates recurrence risks and minimizes treatment-related toxicity and death, while paying attention to compliance treatment to avoid treatment abandonment. This study aimed to determine the survival rates and treatment outcomes of children with ALL.
Materials and Methods
A retrospective cohort study was conducted from January 2019 to December 2022. This study involved newly diagnosed children ALL aged 1–18 years treated at the pediatric oncology division child health department, Hasan Sadikin Hospital, Bandung (provincial referral hospital in West Java, Indonesia). Patients falling under the categories of ALL L3, those above 18 years of age during the treatment period, or those who had passed away before commencing treatment were excluded. French-American-British classification was still used over the molecular/cytogenetic biomarkers of WHO classification due to unavailability of cytogenetic examination facility in our center.
The data collection process involved sourcing information from medical records and the Indonesian Pediatric Cancer Registry (IPCAR), including the demographic of the patients, nutritional status, presenting signs and symptoms, and date of diagnosis. The nutritional status was measured during the diagnosis phase and classified based on the WHO growth chart. Additionally, specific medical criteria were used for defining splenomegaly (enlarged spleen, Schuffner stage 1 or greater) and hepatomegaly (spleen positioned more than 2 cm below the arcus costae). Essential diagnostic factors such as the initial leucocyte count, chest X-ray, presence of leukemic blast in cerebrospinal fluid, and bone marrow morphology during diagnosis and evaluation after induction therapy were obtained. The evaluation of the induction phase was presented as remission if bone marrow morphology evaluation showed blast percentages of 5% or less. However, blast percentages exceeding this threshold were classified as induction failure. The patients’ outcome was determined by relapse and remission during the evaluation after treatment. Specifically, relapse denoted the presence of leukemic blasts exceeding 20% in bone marrow morphology after patients had previously achieved complete remission. The timing of relapse was stratified into three categories: “very early relapse” if it occurred within 18 months of diagnosis, “early relapse” for relapses between 18 and 36 months, and “late relapse” for occurrences after 36 months post-diagnosis.
According to the Hematology Oncology Coordination Unit of the Indonesian Pediatric Society, the categorization of risk stratification was divided into groups, a standard risk (SR) and high risk (HR). High risk was characterized by an inadequate or poor response to prednisone defined by blast cell count ≥1000/µL found in peripheral blood at day eight after 7 days of prednisone and 1 dose of intrathecal methotrexate, absence of complete remission within six weeks with morphology examination, and meeting one or more of the subsequent criteria at the time of diagnosis: age <1 or >10 years old, leucocyte >50x103/µL, mediastinal mass more than 1/3 of the thoracic cavity, CNS involvement (presence of leukemic blast in cerebrospinal fluid), testicular involvement, mixed leukemia, T-cell as determined by immunophenotyping, while cases not meeting these conditions were classified as standard risk.
All patients were treated according to Indonesian Protocol ALL 2018 based on risk stratification (HR and SR). Patients monitoring occurred in the treatment course until the conclusion of the study period. Instances that were considered events for measuring event-free survival (EFS) encompassed relapse, treatment failure, or mortality. Patients who were selected to discontinue or withdraw from the study were accounted for until the last follow-up date. Statistical analysis for survival employed the Kaplan-Meier and was performed with SPSS IBM (Statistical Package for the Social Science Inc., Version 17). The factors affecting the survival of ALL were evaluated with univariate and multivariate analysis using Cox proportional hazard regression method with a confidence interval of 95% and p<0.05. This study was approved by the Ethics Committee of Hasan Sadikin General Hospital. All the data accessed has been authorized by Hasan Sadikin General Hospital for use in this study and kept anonymized using patient code.
Results
Study Population
This study identified 216 ALL children aged 1–18 years old with newly diagnosed ALL from January 2019 to December 2022. From all ALL patients identified in Hasan Sadikin Hospital, 31 had missing data. Only 185 patients were included, while 3 were diagnosed with bone marrow morphology of L3, 39 died before starting treatment, and 6 were transferred to another hospital. The data of the remaining 137 patients were subjected to analysis, as shown in Figure 1.
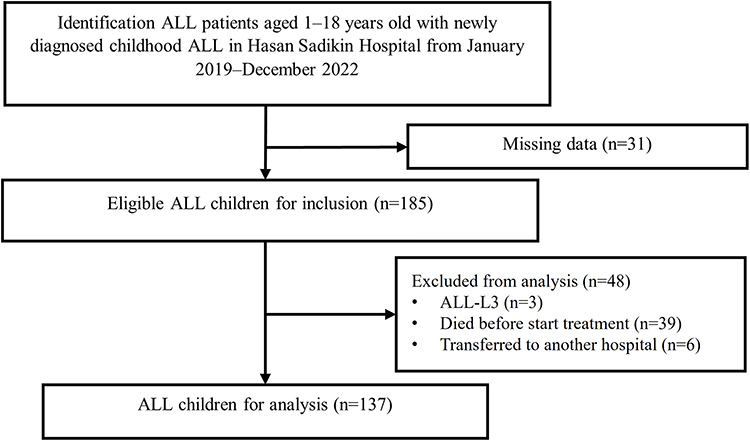 |
Figure 1 Flow chart of subject selection. Abbreviations: ALL, acute lymphoblastic leukemia; ALL-L3, acute lymphoblastic leukemia with bone marrow morphology showed L3. |
Patients Characteristics
The majority of subjects were male (52.2%), with a median age of 6 (1.0–17.7). Subsequently, nutritional status was normal (54.5%) in most subjects during diagnosis. A total of 83 (60.5%) children died until December 2022 and 32 (38.5%) of the cases occurred due to relapse. The majority of relapses transpired during the maintenance phase (42.4%), whereas occurrences during the induction and consolidation phases were observed in 4 (12.1%) and 5 (15.1%), respectively. The median time from the initial diagnosis to relapse was 15.38 months. Subsequently, most relapses occurred very early (<18 months) in 24 (70.5%) children, occurred early (18–36 months) in 7 (20.5%), and 1 (2.9%) child had late relapses. While 10 (7.3%) children completed therapy until the end of the maintenance phase and 2 children had a relapse after completing the treatment. The demographical and clinical characteristics of the subjects are shown in Table 1.
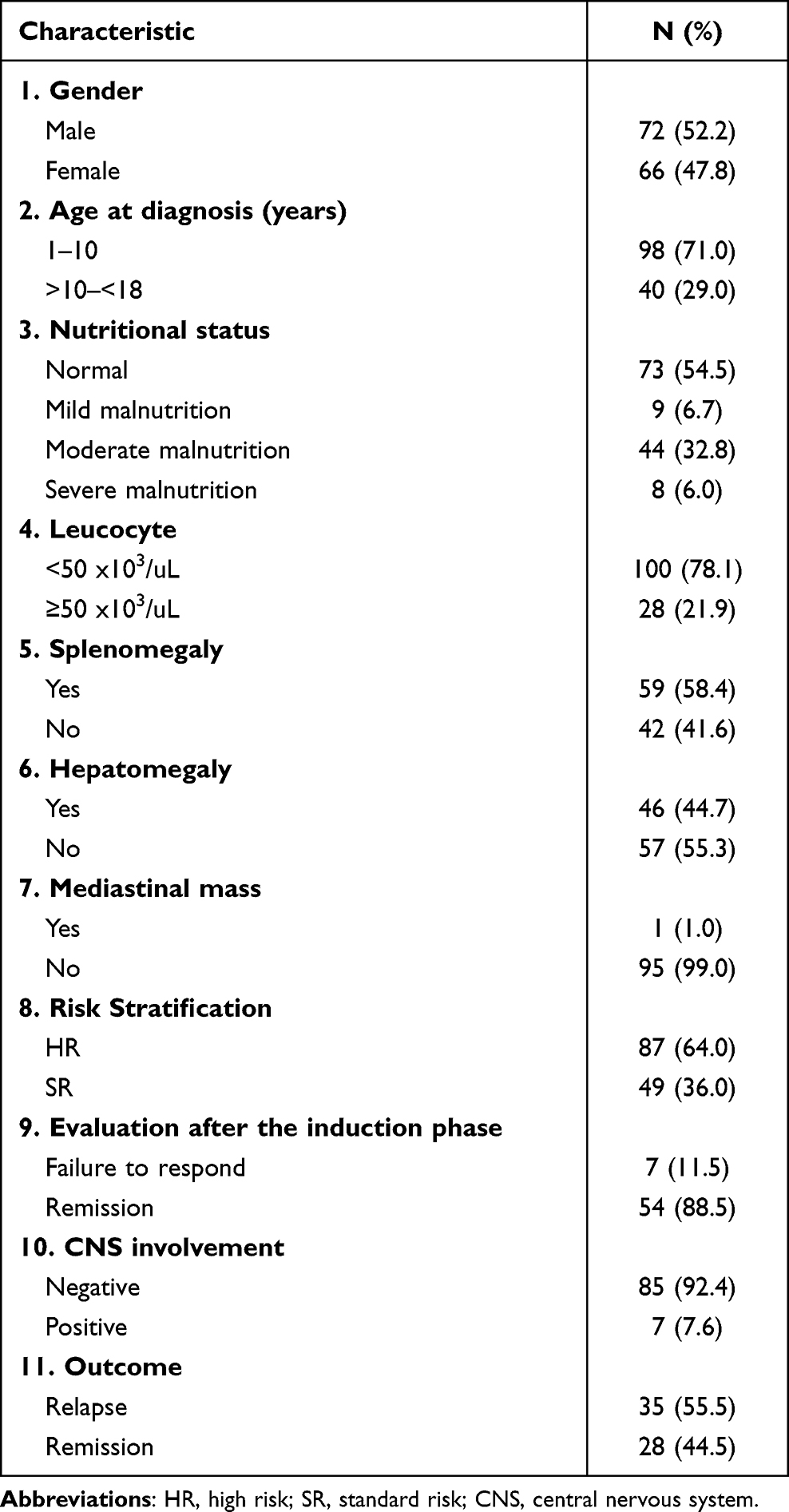 |
Table 1 Demographical and Clinical Characteristics of Subjects |
Survival Analysis
The cumulative overall survival (OS) and EFS rates at 1 year were 36% and 19%, respectively, as shown in Figure 2. In the survival curve, the inclusion of 30 children (21.9%) who dropped out during treatment was marked as censored data. The one-year OS rates for the standard risk (SR) and high-risk (HR) stratification groups were 54% and 29%, while the corresponding one-year EFS rates stood at 64% and 18% (Figure 3). Survival analysis with various demographic and clinical characteristics of subjects was carried out using the Cox regression method. Based on the results of univariate analysis, it was found that the initial leukocyte count ≥50x103/µL (p=0.005) and relapse during the induction-phase therapy evaluation (p<0.008) were associated with the death of ALL (Table 2). Moving to the multivariate analysis, the sole statistically significant variable was the absence of bone marrow remission post the induction phase, which carried a fourfold higher risk of death (Table 3).
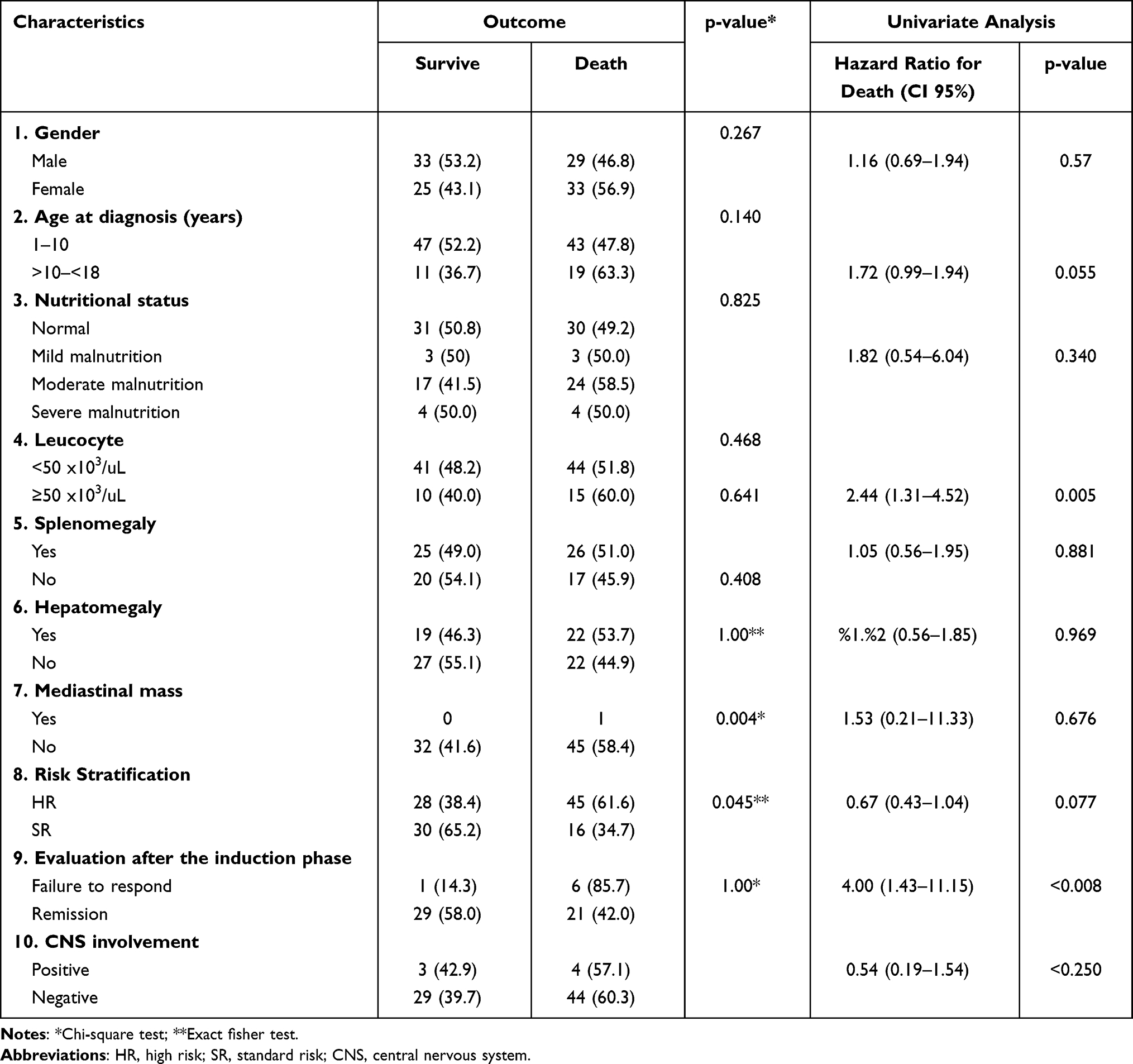 |
Table 2 Association Between Demographical and Clinical Characteristics to the Outcome and Hazard Ratio to Overall Survival (OS) |
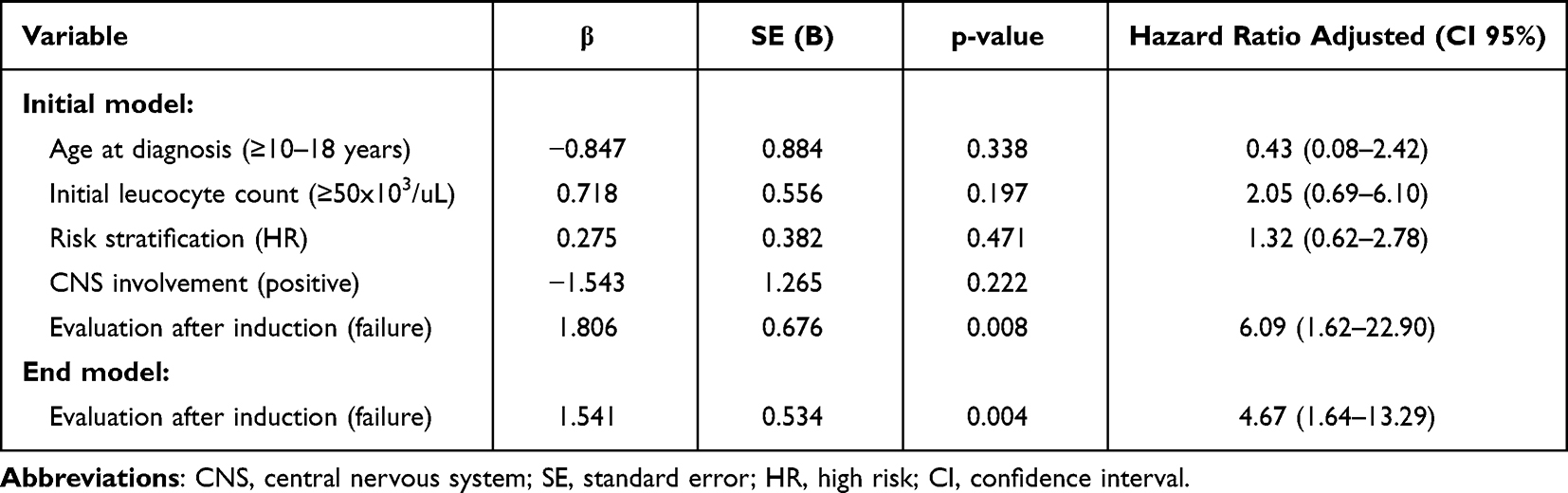 |
Table 3 Multivariate Cox Regression Analysis |
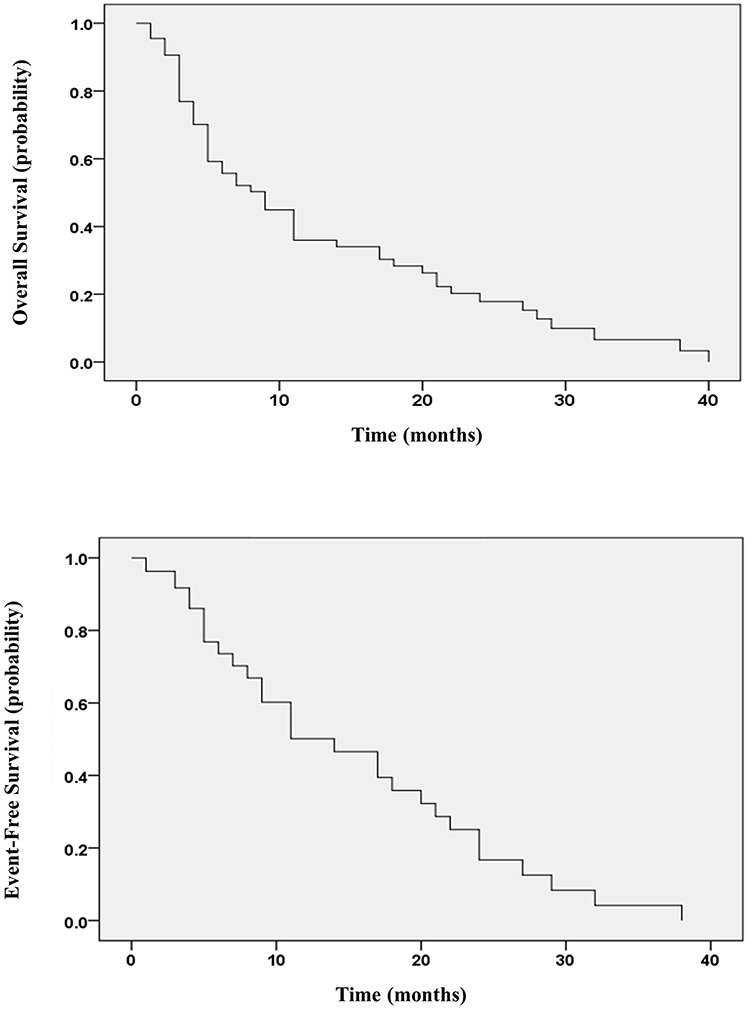 |
Figure 2 Kaplan–Meier curves of probable cumulative OS and EFS. |
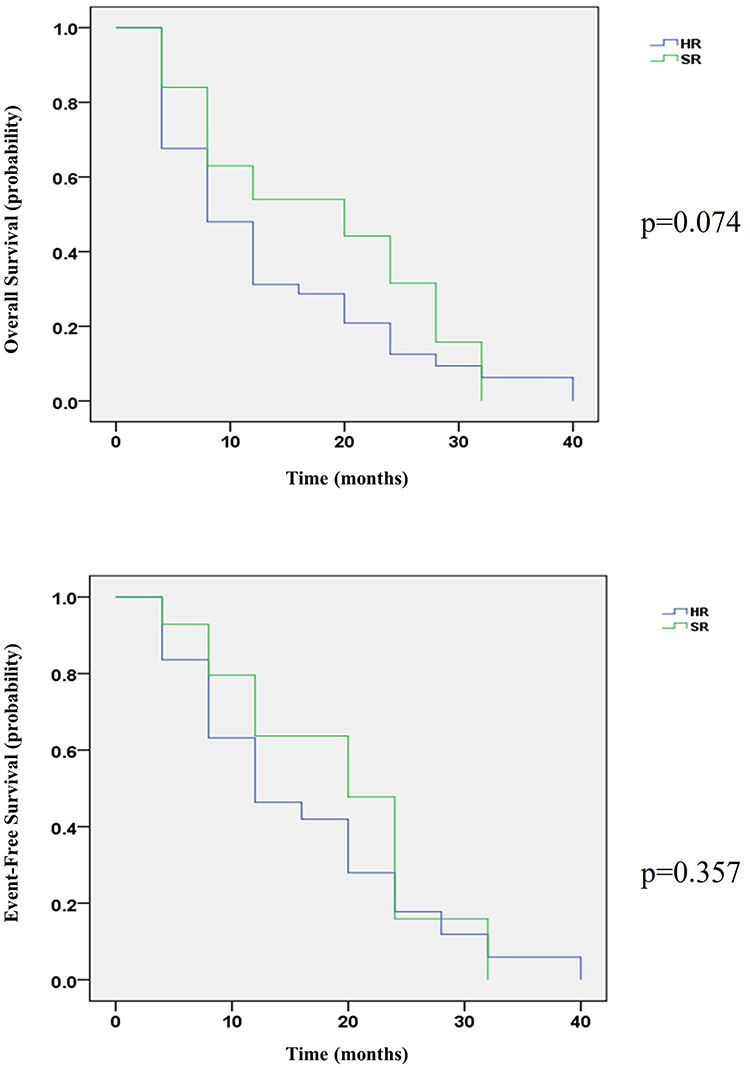 |
Figure 3 Kaplan–Meier curves of probable OS and EFS SR and HR risk stratification group. Abbreviations: SR, standard risk; HR, high risk. |
Discussion
The result of this study showed 62 (59.7%) children with ALL died during and after chemotherapy, with a low cumulative OS rate. This is consistent with the previous studies conducted in several cities in Indonesia, which showed that the survival rate of ALL in children ranges from 20% to 60%.12–14 The survival rate in low-middle-income countries based on CONCORD-2 data was 34.3–73.1%.2,15 Neutropenia was the main cause of death-related treatment enhanced by infection, leading to life-threatening conditions requiring further treatment and may contribute to the delay of therapy during the induction phase.16
Most of the deaths occurred after children had relapsed (<18 months from diagnosis). This is consistent with previous studies in Indonesia and Latin America, showing that most deaths occur after relapse and most relapses occur very early.17,18 Furthermore, a high rate of very early relapse indicated that the therapy given was inadequate to maintain remission and clearance of leukemic cells due to the contributions of several factors, such as delay of diagnosis and treatment, abandonment of therapy, and longer duration of the induction phase. Factors that contributed to the longer duration of the induction phase included infection during the induction phase, waiting for the chemotherapy room to be available, or side effects of previously administered chemotherapy. Inadequate clearance of leukemic cells during the induction phase might increase the risk of induction failure, as well as lead to a higher risk of relapse and severe complication.19
The result showed a high dropout rate of 21.9% due to treatment abandonment, which was still the main problem in developing countries, causing inadequate therapy and reducing the survival rate of ALL. Economic difficulties and lack of parental education might be barriers to therapy compliance despite the provision of national health insurance to cover all examination and treatment costs. Parents or guardians still needed to pay for daily living and the long duration of ALL treatment makes it difficult for parents to work and earn an income. Some were also hesitant to give chemotherapy to their children due to its severe side effects, long-term complications, and incurability beliefs.6,7,17,20 Treatment abandonment should be fixed up in LMIC as one of the preventable factors of treatment failure in ALL.
Initial leucocyte count showed a significant result related to the outcome of ALL. The higher number of leucocyte counts at diagnosis showed the high proliferation of malignancy cells. Hyperleukocytosis leads to circulatory stasis due to the increased blood viscosity with blasts. This is related to the inflammatory process and the release of cytokines that cause ischemic tissue injury and damage by the entry of leukemic cells into the microcirculation.21,22 A high initial leucocyte count was considered in the therapy risk stratification as one of the factors that worsened the prognosis. High-risk patients had lower OS and EFS as mentioned in many previous studies due to poorer prognosis and more intensive therapy.18,23 Most of the patients were in the high-risk stratification group. In addition to the high rate of relapse, the delay in patients getting diagnosed and receiving treatment may lead to further progressivity of leukemic cells requiring the administration of more intensive therapy.
Early response to induction-phase therapy was a significant predictive factor in the outcome of children with ALL. Patients who have induction failure often experience disease progression to become more severe and even cause death. Steroid response, morphological assessment, and MRD evaluation strongly predict therapy outcomes guide the adjustment of treatment intensity and estimate the likelihood of relapse. Response to steroids, morphological assessment, and MRD assessment are strong predictors for predicting therapy outcomes, adjusting the intensity of therapy given, and estimating the likelihood of relapse. In several developing countries with limited MRD facilities, morphological examination at the end of the induction phase still plays an important role in the assessment of ALL therapy.24,25 The longer duration of the induction phase could worsen the prognosis and the outcome of therapy, as well as increase the risk of failure. Induction phase therapy was the most important because it eliminated all leukemic cells, while other phases prevented the risk of relapse and maintained EFS.8
The limitations of this study were in its retrospective design and conducted at a single center, potentially resulting in low external validity. In addition, the high dropout rate means that children cannot be followed until the end of therapy or until relapse occurs. Early death before starting treatment was caused by late of diagnosis and some had refused to referred to tertiary hospital. Many variables showed insignificant results in terms of ALL therapy in this study, as it might be influenced by the small number of subjects investigated. Future studies are expected to assess characteristics that may influence the survival of ALL in LMIC, such as socio-economic factors, parental education, family perception of the disease, and distance between home and health facilities. This assessment should be incorporated into the prospective cohort design of the study.
In conclusion, the evaluation conducted after the induction phase by bone marrow morphology remained a remarkable predictor for the outcome of ALL therapy, specifically in limited resources settings. Treatment delay and abandonment also played an important role in the outcome of ALL in LMIC. Furthermore, improving the survival of ALL remained a challenge in LMIC to determine optimal treatment intensity with less treatment-related toxicity and maintain compliance, as well as reduce delay of diagnosis and treatment.
Acknowledgment
The authors are grateful to the IPCAR and medical staff of the department for the care of patients.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization. WHO Global Initiative for Childhood Cancer: An Overview. WHO Publication; 2020.
2. Bonaventure A, Harewood R, Stiller CA, et al. Worldwide comparison of survival from childhood leukaemia for 1995–2009, by subtype, age, and sex (Concord-2): a population-based study of individual data for 89 828 children from 198 registries in 53 countries. Lancet Haematol. 2017;4(5):e202–e217. doi:10.1016/S2352-3026(17)30052-2
3. Garniasih D, Susanah S, Sribudiani Y, Hilmanto D, Yassin MA. The incidence and mortality of childhood acute lymphoblastic leukemia in Indonesia: a systematic review and meta-analysis. PLoS One. 2022;17(6):e0269706. doi:10.1371/journal.pone.0269706
4. Mostert S, Sitaresmi MN, Gundy CM, Veerman AJP, Veerman AJP. Influence of socioeconomic status on childhood acute lymphoblastic leukemia treatment in Indonesia. Pediatrics. 2006;118(6):e1600–e1606. doi:10.1542/peds.2005-3015
5. Martín-Trejo JA, Núñez-Enríquez JC, Fajardo-Gutiérrez A, et al. Early mortality in children with acute lymphoblastic leukemia in a developing country: the role of malnutrition at diagnosis. A multicenter cohort MIGICCL study. Leuk Lymphoma. 2017;58(4):898–908. doi:10.1080/10428194.2016.1219904
6. Abdelmabood S, Fouda AE, Boujettif F, Mansour A. Treatment outcomes of children with acute lymphoblastic leukemia in a middle-income developing country: high mortalities, early relapses, and poor survival. J Pediatr. 2020;96(1):108–116. doi:10.1016/j.jped.2018.07.013
7. Hafez HA, Soliaman RM, Bilal D, Hashem M, Shalaby LM. Early deaths in pediatric acute leukemia: a major challenge in developing countries. J Pediatr Hematol Oncol. 2019;41(4):261–266. doi:10.1097/MPH.0000000000001408
8. Kato M, Manabe A. Treatment and biology of pediatric acute lymphoblastic leukemia. Pediatr Int. 2018;60(1):4–12. doi:10.1111/ped.13457
9. Capria S, Molica M, Mohamed S, et al. A review of current induction strategies and emerging prognostic factors in the management of children and adolescents with acute lymphoblastic leukemia. Expert Rev Hematol. 2020;13(7):755–769. doi:10.1080/17474086.2020.1770591
10. Shen S, Cai J, Chen J, et al. Long‐term results of the risk‐stratified treatment of childhood acute lymphoblastic leukemia in China. Hematol Oncol. 2018;36(4):679–688. doi:10.1002/hon.2541
11. Widiaskara IM, Permono B, Ugrasena IDG, Ratwita M. Luaran Pengobatan Fase Induksi Pasien Leukemia Limfoblastik Akut pada Anak di Rumah Sakit Umum Dr. Soetomo Surabaya [Induction Phase Treatment Outcomes of Acute Lymphoblastic Leukemia Patients in Children at Dr. Soetomo General Hospital Surabaya]. Sari Pediatr. 2016;12(2):128–134. doi:10.14238/sp12.2.2010.128-34
12. Wijayanti LP, Supriyadi E. Faktor Prognostik dan Kesintasan Pasien Leukemia Limfoblastik Akut Anak di RSUP Dr. Sardjito, Yogyakarta, 2010–2015 [Prognostic Factors and Survival of Pediatric Acute Lymphoblastic Leukemia Patients at Dr. Sardjito Hospital, Yogyakarta, 2010–2015]. Indones J Cancer. 2018;11(4):145–150. doi:10.33371/ijoc.v11i4.532
13. Simanjorang C, Kodim N, Tehuteru E. Perbedaan kesintasan 5 tahun pasien leukemia limfoblastik akut dan leukemia mieloblastik akut pada Anak di Rumah Sakit Kanker “Dharmais”, Jakarta, 1997–2008. Indones J Cancer. 2013;7(1):15–21 doi:10.14414/ijoc.v7i1.274.
14. Meirizkia A, Ayu DR, Indra RM, Sari DP. 3-year survival rate in acute lymphoblastic leukemia: comparison of ALL-2006 and ALL-2013 Protocols. Paediatr Indones. 2021;61(3):155–164. doi:10.14238/pi61.3.2021.155-64
15. Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000–14 (Concord-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018;391(10125):1023–1075. doi:10.1016/S0140-6736(17)33326-3
16. Widjajanto PH, Sumadiono S, Cloos J, Purwanto I, Sutaryo S, Veerman AJP. Randomized double blind trial of ciprofloxacin prophylaxis during induction treatment in childhood acute lymphoblastic leukemia in the WK-ALL protocol in Indonesia. J Blood Med. 2013;1–9. doi:10.2147/JBM.S33906
17. Sari NM, Nurazizah NA, Lesmana R, Suryawan N, Susanah S. Retrospective study on very early relapse of childhood acute lymphoblastic leukemia at a reference centre in Indonesia. Bali Med J. 2022;11(1):44–49. doi:10.15562/bmj.v11i1.2495
18. Jaime-Pérez JC, Pinzón-Uresti MA, Jiménez-Castillo RA, Colunga-Pedraza JE, González-Llano Ó, Gómez-Almaguer D. Relapse of childhood acute lymphoblastic leukemia and outcomes at a reference center in Latin America: organomegaly at diagnosis is a significant clinical predictor. Hematology. 2018;23(1):1–9. doi:10.1080/10245332.2017.1333294
19. Schrappe M, Hunger SP, Pui C-H, et al. Outcomes after induction failure in childhood acute lymphoblastic leukemia. N Engl J Med. 2012;366(15):1371–1381. doi:10.1056/NEJMoa1110169
20. Cai J, Yu J, Zhu X, et al. Treatment abandonment in childhood acute lymphoblastic leukaemia in China: a retrospective cohort study of the Chinese Children’s Cancer Group. Arch Dis Child. 2019;104(6):522–529. doi:10.1136/archdischild-2018-316181
21. Park KM, Yang EJ, Lee JM, et al. Treatment outcome in pediatric acute lymphoblastic leukemia with hyperleukocytosis in the yeungnam region of Korea: a multicenter retrospective study. J Pediatr Hematol Oncol. 2020;42(4):275–280. doi:10.1097/MPH.0000000000001771
22. Alfina D, Widjajanto PH, Patria SY. The outcomes of childhood acute lymphoblastic leukemia with hyperleukocytosis. Paediatr Indones. 2018;58(4):186–191. doi:10.14238/pi58.4.2018.186-91
23. Sutaryo S, Widjajanto PH, Mulatsih S, et al. Childhood acute lymphoblastic leukemia: four years evaluation of protocols 2013 and 2016 in a single center in Indonesia, a lower‐middle‐income country. Pediatr Blood Cancer. 2022;69(11):e29875. doi:10.1002/pbc.29875
24. Wei W, Chen X, Zou Y, et al. Prediction of outcomes by early treatment responses in childhood T-cell acute lymphoblastic leukemia: a retrospective study in China. BMC Pediatr. 2015;15(1):1–11. doi:10.1186/s12887-015-0390-z
25. Möricke A, Lauten M, Beier R, et al. Prediction of outcome by early response in childhood acute lymphoblastic leukemia. Klin Pädiatrie. 2013;225(1):S50–S56 doi:10.1055/s-0033-1337964.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.