")
Back to Journals » Infection and Drug Resistance » Volume 17
Survival Rate and Predictors of Mortality Among TB-HIV Co-Infected Patients During Tuberculosis Treatment at Public Health Facilities in Bahir Dar City, Northwest Ethiopia
Authors Kegne TW, Anteneh ZA , Bayeh TL , Shiferaw BM, Tamiru DH
Received 28 December 2023
Accepted for publication 3 April 2024
Published 9 April 2024 Volume 2024:17 Pages 1385—1395
DOI https://doi.org/10.2147/IDR.S446020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Teshager Worku Kegne,1,* Zelalem Alamrew Anteneh,2,* Tadios Lidetu Bayeh,2,* Birhanu Melaku Shiferaw,3,* Desiyalew Habtamu Tamiru4,*
1Department of Health Services, Management Sciences for Health, Addis Ababa, Ethiopia; 2Department of Epidemiology and Biostatistics, School of Public Health, Bahir Dar University, Bahir Dar, Ethiopia; 3Department of Public Health, Gamby Medical and Business College, Bahir Dar, Ethiopia; 4Department of Public Health Emergency, Humedica e.V International Aid Organization, Addis Ababa, Ethiopia
*These authors contributed equally to this work
Correspondence: Desiyalew Habtamu Tamiru, Tel +251912717030, Email [email protected]
Background: Tuberculosis and human immunodeficiency virus co-infection pose a major public health concern, particularly in developing countries. The survival and predictors of mortality were not sufficiently studied among TB-HIV co-infected patients in Ethiopia.
Objective: This study aimed to investigate the survival rate and predictors of mortality among TB-HIV co-infected patients during TB treatment at public health facilities in Bahir Dar, Northwest Ethiopia.
Methods: A retrospective follow-up study was conducted among 401 TB-HIV co-infected patients who were treated for tuberculosis between July 2018 and June 2022 at public health facilities in Bahir Dar city, Ethiopia. Data were collected using a structured checklist from patient charts. Data entry and analysis were done using EpiData 3.1 and Stata version 15, respectively. A Cox proportional Hazard regression model was used to identify predictors of mortality. Predictors with P < 0.05 in the multivariable regression were considered statistically significant.
Results: Among the 401 TB-HIV co-infected patients, 59 (14.7%) died during the follow-up period. Predictors like lower BMI (AHR = 3.00, 95% CI = 1.44, 6.28), extrapulmonary TB infection (AHR = 3.30, 95% CI = 1.50, 7.29), presence of opportunistic infection (AHR = 5.07, 95% CI = 2.55, 10.08), functional status (bedridden: AHR = 4.49, 95% CI = 1.63, 12.33), and adherence to TB treatment (fair = AHR = 2.74, 95% CI = 1.41, 7.20, and poor = AHR = 3.75, 95% CI = 1.52, 9.23) were associated with mortality.
Conclusion: Mortality among TB and HIV coinfected people was high at public health facilities in Bahir Dar city. This result suggested that in order to increase patient survival, it would be necessary to enhance nutritional status, increase adherence to TB treatment, and prevent opportunistic infections.
Keywords: TB, HIV, mortality, predictors, retrospective, survival, Ethiopia
Introduction
Tuberculosis (TB) and the Human Immunodeficiency Virus (HIV) are among the leading public health problems globally. Tuberculosis is one of the most common illnesses and causes of death among people living with HIV (PLWHIV). HIV positive individuals have a 20–30 times greater risk of contracting TB than HIV negative individuals due to lowered immunity. Reports also indicated that PLWHIV are more likely to develop active TB than HIV negative.1,2 The global TB report 2021 stated that out of ten million people infected with TB, 8% were PLHIV. The proportion of TB episodes coinfected with HIV was highest in the African region, exceeding 50% in parts of Southern Africa.2
TB and HIV form a lethal combination, each speeding the other’s progress. As a result, individuals with co-infections of TB and HIV have a significant risk of increased mortality. Without proper treatment, 60% of HIV-negative people with TB on average and nearly all HIV-positive people with TB will die.3 Globally, 1.6 million people died from TB and 1 million from HIV in 2017 and accounting for one in every 300,000 deaths from both diseases.1 Most recently, about one-third of all AIDS-related deaths worldwide are caused by TB, which is the leading cause of death among HIV-positive individuals. An estimated 167,000 people died from TB-HIV coinfection in 2022.3 The syndromic interaction between TB and HIV has played a ruinous role, with Africans bearing a disproportionate share of the burden. In 2019, people in Africa accounted for 73% of TB-HIV co-infection cases and 81% of all TB-HIV deaths. At the country level, South Africa and Nigeria rank among the worst affected in sub-Saharan Africa and globally for both diseases.4,5 In addition to TB disease, PLHIV bears a high burden of drug-resistant TB strains; thus, if diagnosis is delayed, there is an increased risk of mortality from multidrug-resistant and extensively drug-resistant TB in this population.6
With an estimated TB incidence rate of 164 per 100,000 people and 112 cases per 100,000 TB cases among PLWHIV, Ethiopia is one of the twenty nations in the world with the highest burdens of TB and TB-HIV.7,8 According to a nationwide retrospective cohort study, 9% of HIV patients receiving treatment also had TB.9 About 13% of all new TB cases are also HIV coinfected. Moreover, Ethiopia is one of the high TB-HIV and multidrug resistant TB (MDR TB) burden countries. Among TB patients with known HIV status, about 11% were HIV co-infected.10 According to the global report, 3600 people in Ethiopia who had TB and HIV co-infections died while receiving TB treatment in 2017 alone.11 Despite the availability of free ART and anti-TB medications in the country, the survival rate for those with TB and HIV co-infection has not increased.12,13
Studies conducted worldwide indicated that the survival of TB-HIV infected patients was determined by different predictors. Socio-demographic and personal factors like age, sex, residency, education, occupation and body mass index play a key role in predicting the mortality of people co-infected with HIV and TB in countries around the world.14–18 Studies showed that patients with TB-HIV without ART tend to have poorer TB outcomes compared to those who are on ART, and TB infection with late presentation and HIV diagnosis are further risk factors for unsuccessful TB treatment outcomes among patients with TB-HIV.19,20 Previous research has also shown a significant correlation between TB-HIV-related mortalities and baseline CD4 cell count, WHO clinical stage, use of co-trimoxazole preventive therapy, the presence of opportunistic infections and baseline functional level.9,21,22 Although, co-infection with TB and HIV is bidirectional and a dual public health burden worldwide, TB-HIV co-infected patients have not received enough attention.23,24
A few studies conducted in Ethiopia found that factors such as ART status, baseline CD4 cell count, baseline functional level, WHO clinical stage, cotrimoxazole preventive therapy, type of TB diagnosis, and coexistence of other opportunistic infections (OIs) were predictive of survival among TB-HIV co-infected patients.21,25 However, previous studies are not sufficient to estimate the survival status of the patients. In addition, the results of earlier studies may no longer be applicable to use as an intervention tool to improve patient survival because there are recurring or ongoing changes in the characteristics of the diseases, in the ART and TB treatment regimens, in population migration, and in the drug resistance of the disease. As a result, up-to-date studies are required that take all these changes into consideration. Therefore, this study was conducted to identify the survival status and predictors of mortality among TB-HIV-coinfected patients who were on TB treatment between 2018 and 2022 at public health facilities in Bahir Dar City.
Methods and Materials
Study Setting and Period
This study was conducted at public health facilities located in Bahir Dar City by reviewing medical records of patients recorded from July 2018 to June 2022. Bahir Dar is the capital city of Amhara Regional State, which is located 560 km northwest of Addis Ababa, the capital of Ethiopia. There are eleven HCs and three public hospitals administered by the Bahir Dar city health department. These facilities are expected to serve about 422,580 people around Bahir Dar and other nearby areas.
Study Design: An institution-based retrospective follow-up study was conducted among TB-HIV co-infected patients treated at public health facilities in Bahir Dar city.
Source and Study Populations
The source population was all TB-HIV-coinfected patients being treated for TB at public health facilities in Bahir Dar city, while the study population was all TB-HIV-coinfected patients being treated for TB at public health facilities in Bahir Dar city from July 2018 to June 2022.
Inclusion and Exclusion Criteria
All TB-HIV co-infected patients who were treated for TB at public health facilities in Bahir Dar city from July 2018 to June 2022 were included. And those patient charts that lacked complete disease documentation, an incomplete base line, and follow-up data were excluded from the study.
Study Variables
Dependent Variable
The dependent variable for this study was survival time to death of TB-HIV co-infected patients from the time of initiation of TB treatment to end of follow-up period.
Independent Variables
Socio demographic factors: age, sex, marital status, educational status, occupation, residence.
Clinical characteristics: WHO clinical stage, CD4 count/mm3, hemoglobin level, nutritional status (Weight, Height), site of TB, functional status, comorbidities (DM, HTN, Asthma) and opportunistic infection (OI).
Treatment-related factors: TB regimen, ART regimen, adherence to TB and HIV, and CPT.
Operational Definition
Survival time: The time in days between diagnosis of TB-HIV co-infection and occurrence of outcome (event or censored).
Time to death: The time from TB-HIV co-infection to the occurrence of the event (death) during the follow-up period.
Events: The event of this study is death of a TB-HIV co-infected patients.
Censored: Represents patients lost to follow-up, treatment completed, recovered and treatment failure.
Loss to follow-up: A TB-HIV co-infected patient whose treatment was interrupted for 2 consecutive months or more.
Transferred out: Those TB-HIV patients who were transferred-out to another health facilities for TB treatment.
Adherence: A patient was following the recommended course of treatment by taking all prescribed medications and coming for scheduled exams and tests.
Sampling Techniques and Procedures
All patients co-infected with TB and HIV who were registered and receiving follow-up care from July 2018 to June 2022 were included in the current study. During the study period, a total of 2675 HIV-positive clients and 3192 TB patients were notified. Among these patients, 472 were TB-HIV co-infected. Each TB-HIV co-infection patient in the cohort was retrospectively studied, starting from the initiation of TB treatment to the occurrence of the outcome (event or censored) or the end of the follow-up period. Seventy-one charts were rejected due to incompleteness, and 401 TB-HIV-coinfected patients who were treated during the study period were included in the study.
Data Collection Methods and Procedures
The data were collected using a structured checklist prepared in English. The data extraction tool was adapted from existing studies and adopted from patients’ charts, registrations, and ART and TB intake forms. The tool consisted of predictors related to socio-demographic characteristics, clinical characteristics of the patient, laboratory investigations, treatment, and adherence to treatment. Four nurses who have training in ART and TB participated in the data collection process.
Data Quality Assurance
Prior to actual work, data collectors and supervisors were given a one-day orientation on data collection tools. During orientation, emphasis was given on the purpose of the study, how to use data extraction tools and their content, and how to address possible problems. In each facility, a card room porter was recruited for card delivery from the card room. The principal investigator and the supervisors closely monitored the whole data collection process on a regular basis. The collected data were cleaned before the analysis.
Data Processing and Analysis
Data were entered using EpiData version 3.1 and analyzed using STATA version 15. Before analysis, the data were cleaned and checked for consistency by using simple frequencies and cross tabulation; re-categorization of categorical variables and categorization of continuous variables was done to make it suitable for analysis. Descriptive statistics were used to present the demographic and background clinical characteristics of the patients. The Kaplan–Meier survival curve was used to estimate the median survival time and cumulative probability of survival, while the Log rank test was used to assess overall survival differences between group predictors. Cox proportional hazard regression analysis was used to identify the potential predictors of mortality. Multicollinearity between predictors was checked. A bivariable Cox-proportional hazard regression model was fitted for each explanatory variable, and those variables having a p-value ≤0.25 were selected for multivariable analysis. The adjusted hazard ratio (AHR) with 95% confidence intervals was computed, and statistical significance was declared at p < 0.05. Finally, results were presented using tables, graphs, and text.
Results
Socio-Demographic Characteristics
The data used for this study was obtained from the medical records of 401 TB-HIV-coinfected patients. The median age of the patient was 35, with an interquartile range of 13 years (28 to 41). Slightly more than half, 227 (56.6%) were male in sex, and most, 340 (84.79%) of them were urban regarding their residency. A total of 164 (40.9%) individuals were married, and nearly one-third (30.43%) of participants had no formal education (Table 1).
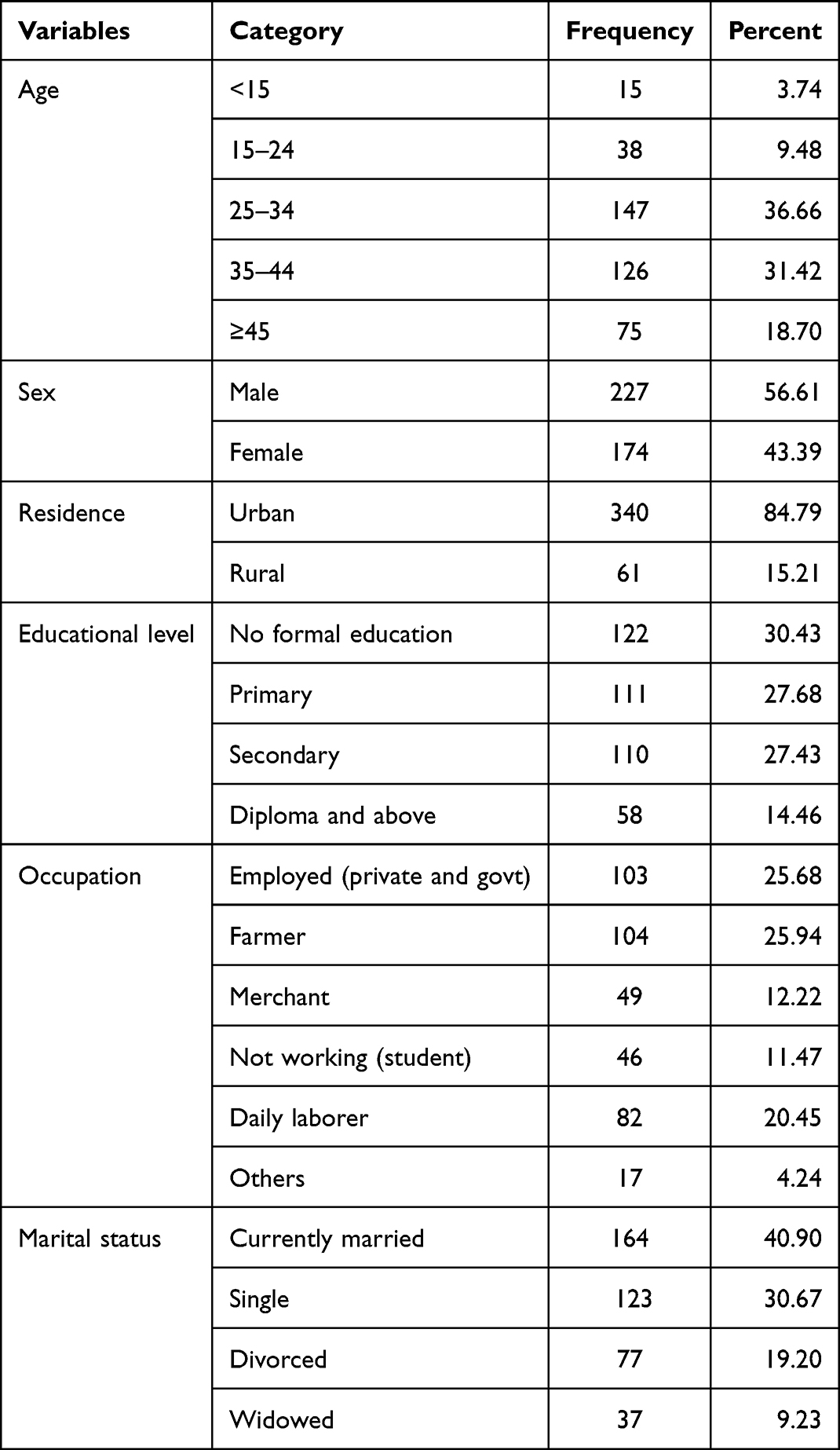 |
Table 1 Socio-Demographic Characteristics of TB-HIV Co-Infected Patients at PHFs in Bahir Dar City, Northwest Ethiopia, August 2023 (n = 401) |
Background Clinical Characteristics
The findings of this study showed that among participants majority, 358 (89.28%) were in advanced WHO stages (stage III and IV). In addition, 20 (4.99%), 10 (2.49%) and 24 (5.99%) had asthma, diabetic mellitus, and hypertension, respectively. Among individuals who have one or more comorbidities 23 (42.59%) died during the follow-up period. Regarding the functional status of participants, 291 (72.57%), 96 (23.94%), and 14 (3.49%) were working, ambulatory, and bedridden, respectively. More than half (55.86%) of patients were diagnosed with pulmonary TB, while the rest, 177 (44.14%), were extra-pulmonary. Among 83 (20.7%) patients who had opportunistic infections, 38 (45.78%) died during the follow-up period. In addition, from 97 (24.19%) patients with a CD4 count <200 cells/mm3, 17 (17.5%) died during the TB treatment period. Of the study’s participants, 168 (41.90%) had their ART treatment regimen changed after enrolling, and 25 (14.88%) of them passed away while receiving TB treatment. Among those patients who were co-infected, 19 (4.74%) and 20 (4.99%) exhibited poor adherence to ART and TB treatment, respectively. There were 283 (70.57%) patients who received cotrimoxazole preventive therapy, of whom 7.77% died during TB treatment and the follow-up period (Table 2).
 |
Table 2 Base Line Clinical Characteristics of TB and HIV Co-Infected Patients During TB Treatment at PHFs in Bahir Dar City, Northwest Ethiopia, August 2023 (n = 401) |
Mortality and Survival Status of TB-HIV Co‑infected Patients
Among the 401 patients who were included in this study, there were 310 (73.3%) treatment successes, 59 (14.7%) deaths, 18 (4.5%) did not get evaluated, 8 (2.0%) lost follow-ups, and 6 (1.5%) treatment failures. High mortality in TB and HIV co-infected patients was observed in the earlier months of the treatment period. Twelve (27%), twenty-two (64%), and fifty-four (95%) of deaths among co-infected patients occurred in the second, third, and sixth-months following anti-TB treatment initiation, respectively. The incidence rate of mortality among TB-HIV coinfected patients was 7.47 per 10,000-person day (95%: CI = 5.79, 9.64) or 242 per 10,000-person month. The survival rates were also 96%, 90%, and 85% at 2, 3, and 6 months, respectively, after the initiation of TB treatment.
Overall Survival and Survival Comparison Between Group Predictors
The Kaplan–Meier technique was employed to plot the survival graph. Even though there was no abrupt decline, the Kaplan–Meier survival curve showed that overall survival was gradually declining until about three months (the 200 days) of the follow-up period. However, in the subsequent follow-up period, the graph flattened out, showing nearly constant survival time until the end of the follow-up period (Figure 1). The Log rank test and the KM graphical curve were used to evaluate survival differences for categorical predictors. Therefore, a separate Kaplan–Meier graph was drawn for each predictor. Accordingly, there were differences in the survival times for predictors such as the site of the TB, the presence of OI, the body mass index, the patient’s functional level, TB adherence, status of DM, CD4 count, and CPT. For other group predictors such as sex, residency, or age, there were, however, no clear differences in survival time.
 |
Figure 1 Overall Kaplan-Meier survival probability curve among TB-HIV coinfected patients, during TB treatment at PHFs in Bahir Dar City, Northwest Ethiopia, August 2023 (n = 401). |
Predictors of Mortality Among TB-HIV Coinfected Patients
In this study, the Cox proportional hazard analysis was used to identify significant predictors of mortality. Variables that meet the basic requirements of the Cox proportional hazard assumptions and that had a p-value of ≤0.25 in the bi-variable Cox proportional analysis were included in the final model. Accordingly, marital status, the presence of asthma, the presence of DM, BMI, WHO clinical stages, sites of TB, the presence of OI, the functional status of the patients, adherence to the ART treatment, adherence to TB treatment, and cotrimoxazole preventive therapy were variables fitted into the final model. In multi-variable Cox-Proportional Hazard model, BMI, the site of TB infection, the presence of OI, functional status of the patient, and adherence to TB treatment were remain significant predictors of mortality.
Patients who had a BMI of lower than normal were 3.00 times higher risks of dying as a compared to those who had normal BMI (AHR = 3.00, 95% CI = 1.44, 6.28). Patients with Extrapulmonary TB had 3.30 times more risk of death than patients with pulmonary TB (AHR = 3.30, 95% CI = 1.49, 7.29). The risk of dying was 5.07 times higher for those patients with OIs as compared to their counterparts (AHR = 5.07; 95% CI = 2.55, 10.09). Bedridden patients had a mortality risk that was 4.49 times higher than those with working functional status (AHR = 4.49; 95% CI = 1.63, 12.33). Furthermore, this study found that patients who had fair and poor adherence to their TB treatment had 2.74 times (AHR = 2.74, 95% CI = 1.41, 7.20) and 3.75 times (AHR = 3.75, 95% CI, 1.52, 9.23) a higher risk of dying during TB treatment compared to patients who had good adherence to their treatment, respectively (Table 3).
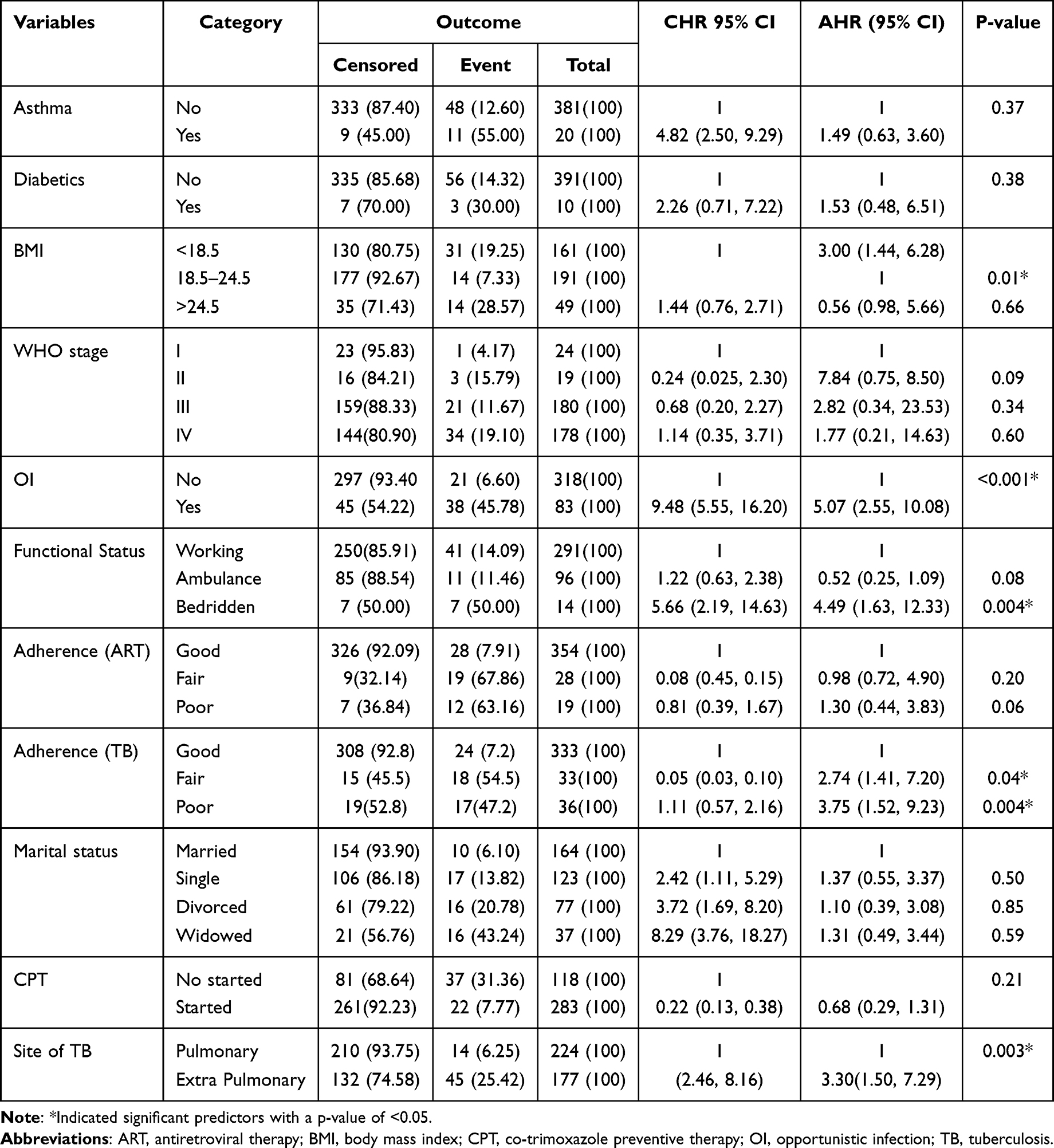 |
Table 3 Multivariable Cox Regression Analysis Among TB-HIV Co-Infected Patients Being Treated for TB at PHFs in Bahir Dar City, Northwest Ethiopia, August 2023 (n = 401) |
Discussion
This study was conducted to determine the survival time and predictors of mortality among TB-HIV co-infected patients during tuberculosis treatment at public health facilities in Bahir Dar. The finding indicated that the median follow-up period was 212 days with a minimum and maximum days of 34 and 355 days.
This study revealed that the cumulative incidence of mortality was 14.7% (95% CI = 11.4%, 18.6%) among TB-HIV co-infected patients during TB treatment and follow-up period. The finding was consistent with a study in Myanmar, 13.7%26 and Ethiopian studies reported from, Somali, 11.1%27 and Bahir Dar, 18%.28 But it was lower than studies in Almaty, Kazakhstan 27.4%,29 Metu Karl Hospital 20.9%,30 Mizan Tepi University Hospital 21.8%,31 and Mekelle, 23.0%.24 However, this finding significantly higher than the study conducted in Harar town 7.7%.32 The overall incidence rate was 2.42 per 100 person months (95% CI = 1.88, 3.12), which was higher than studies conducted in Metu Karl Referral Hospital and Mizan Tepi teaching Hospital which reported 1.21 per 100 person month and 0.52 per 100 person month, respectively.4,30 However, the finding was lower than a study conducted in Bahir Dar28 which reported 4.1 per 100 Person-Month. The differences might be having been due to differences in the study’s design and period, differences in the quality of care in the treatment center and changes in the treatment protocol.
TB-HIV co-infected patients whose BMI was lower than normal (BMI < 18.5 kg/m2) had more than three times higher risk of death as compared to those with normal BMI. The finding was in line with a study in Lesotho18 and an Ethiopian study conducted in Mekelle.33 The possible justification might be that those with a lower BMI are supposed to suffer from malnutrition, which is one of the causes of immunocompromising diseases that result in death.
Site of TB was also a predictor of mortality, and hence, Extra Pulmonary TB (EPTB) had 3.3 times more risk of mortality than pulmonary TB. The finding was consistent with studies conducted in Ethiopia, Mekelle24 and Bahir Dar.28 Possible justification for the similarities might be that EPTB cases have a greater chance of being disseminated to different body organs, which may result in treatment failure, and, finally lead to multi-drug resistance and mortality.24 Unlikely, the result of this study were different from a study conducted in Ambo Referral Hospital, Ethiopia, indicated PTB patients were 2.3 times more likely to die than EPTB.21 The differences might be due to differences in study period, setting and design of the study.
Those patients with opportunistic infections had 5.07 times higher risk of dying compared with those without opportunistic infections. The finding was consistent with other studies conducted in Botswana34 and Cameron35 and at teaching hospitals in Harar Ethiopia.32 The possible reason could be that those patients with opportunistic infection less likely to resist TB and recover from their illness.
The functional status of the patient was another predictor of mortality among TB-HIV coinfected patients. Those bed ridden patients were 4.49 times more at risk of death compared to those with working status. The finding was in line with studies conducted at Mizan Tepi, Bahir Dar, Metu Karl and Jimma Referral hospitals.4,28,30,36 This might be because bedridden patients have a worse prognosis for health because of a relentless immunity-lowering cycle, which can result in patients contracting opportunistic infections and dying.30
According to this study, participants with poor adherence to TB treatment had 3.75 times an increased risk of mortality as compared to good adherence. This agreed with a study done in Mizan-Tepi southwest Ethiopia.31 The similarities could be those people who were unable to take TB drugs adherently had come up with many problems such as treatment failure, a resistant strain which resulted in death of their outcome.
Limitations of the Study
The data were extracted from secondary sources, and as a result, some important variables related to behavioral factors like smoking, drug use, and others like income were missed, which might be potential predictors of mortality in TB-HIV co-infected patients.
Conclusion
The findings of this study indicated that there was high mortality among TB-HIV coinfected patients during the follow-up period, and specifically, low survival was observed in the earlier months of initiation of TB treatment. Since the number of deaths was significantly high, efforts must be made to reduce it. Low BMI (<18 gm/m2) at baseline, presence of OI, EPTB, bedridden functional status, and inability to adhere to anti-TB treatment were independent predictors affecting the survival of TB-HIV co-infected patients. Therefore, to increase the survival of the patient, health care providers in the study area should work to improve the nutrition status of the patient, improve their adherence, and prevent and treat opportunistic infections.
Abbreviations
AIDS, acquired immune deficiency syndrome; ART, antiretroviral therapy; BMI, body mass index; CD4, cluster differentiation-4; EPTB, extra pulmonary TB; HIV, human immunodeficiency virus; OI, opportunistic infection; PHFs, public health facilities; TB, tuberculosis; WHO, World Health Organization.
Data Sharing Statement
The corresponding author will provide the datasets used and/or analyzed for this study upon reasonable request.
Ethics Approval
The study was conducted after getting ethical clearance from the Amhara Public Health Institute research directorate ethical review committee. The study utilized the five-year secondary data collected retrospectively from individual patient medical records. Therefore, the ethical committee approved that there was no patient consent as there was no direct patient contact during data collection, provided that the data would be used only for the sole purpose of the study. The letter of cooperation written by the ethical committee on January 27, 2023, with a reference number of 1888/APHI, was presented to each health facility in Bahir Dar city. The research committee in each health facility gave a grant to conduct the research in their respective facilities. Confidentiality of the information was secured throughout the study by excluding names and patient medical record numbers on the data extraction form, and the data were used only for the proposed study. This study adhered to the Declaration of Helsinki’s ethical standards.
Acknowledgments
We would like to express our heartfelt gratitude to health care providers and administrators of public health facilities in Bahir Dar city. We also want to pass our dedication to the Amhara public health institute for their cooperation during the process of the ethical approval.
Author Contributions
All authors made a significant contribution to this work, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded.
Disclosure
The authors declare no competing interests in this work.
References
1. World Health Organization. TB-HIV Co-Infection Myanmar Factsheet Special. World Health Organization; 2019.
2. Dean GL, Edwards SG, Ives NJ, et al. Treatment of tuberculosis in HIV-infected persons in the era of highly active antiretroviral therapy. Aids. 2002;16(1):75–83. doi:10.1097/00002030-200201040-00010
3. World Health Organization. Tuberculosis fact sheet. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis.
4. Wondimu W, Dube L, Kabeta T. Factors affecting survival rates among adult TB/hiv co-infected patients in Mizan Tepi University teaching hospital, South West Ethiopia. HIV/AIDS. 2020;12:157.
5. Nachega JB, Kapata N, Sam-Agudu NA, et al. Minimizing the impact of the triple burden of COVID-19, tuberculosis and HIV on health services in sub-Saharan Africa. Inter J Infect Dis. 2021;113:S16–S21. doi:10.1016/j.ijid.2021.03.038
6. Abdool Karim Q, Abdool Karim SS. COVID-19 affects HIV and tuberculosis care. Science. 2020;369(6502):6502):366–8. doi:10.1126/science.abd1072
7. Alem Y, Gebre-Selassie S. Treatment outcome of tuberculosis patients in selected health centres in Addis Ababa: a Five Year Retrospective Study. J Lung Health Dis. 2017;1(1):5–12. doi:10.29245/2689-999X/2017/1.1106
8. World Health Organization. World Health Organization global tuberculosis report 2021; 2021. Available from: https://wwwwhoint/teams/global-tuberculosis-programme/tbreports/global-tuberculosis-report-2021.
9. Teklu AM, Nega A, Mamuye AT, et al. Factors associated with mortality of TB/HIV co-infected patients in Ethiopia. Ethiop J Health Sci. 2017;27(1):29–38. doi:10.4314/ejhs.v27i1.4S
10. World Health Organization. Global tuberculosis report 2022 factsheet; 2022.
11. Mugusi FM, Mehta S, Villamor E, et al. Factors associated with mortality in HIV-infected and uninfected patients with pulmonary tuberculosis. BMC Public Health. 2009;9(1):1–8. doi:10.1186/1471-2458-9-409
12. Smith JP, Gandhi NR, Shah NS, et al. The impact of concurrent antiretroviral therapy and MDR-TB treatment on adverse events. J Acquir Immune Defic Syndr. 2020;83(1):47.
13. Gebremariam G, Asmamaw G, Hussen M, et al. Impact of HIV status on treatment outcome of tuberculosis patients registered at Arsi Negele Health Center, Southern Ethiopia: a six year retrospective study. PLoS One. 2016;11(4):e0153239. doi:10.1371/journal.pone.0153239
14. ArunMohan M, Tejaswi H, Ranganath T. Socio-demographic profile of TB-HIV co-infected adults and it’s association with tuberculosis treatment outcome, in a South Indian city. Int J Community Med Public Health. 2016;3:3498–3503.
15. Domingos MP, Caiaffa WT, Colosimo EA. Mortality, TB/HIV co-infection, and treatment dropout: predictors of tuberculosis prognosis in Recife, Pernambuco State, Brazil. Cad Saude Publica. 2008;24:887–896. doi:10.1590/S0102-311X2008000400020
16. Kosgei RJ, Callens S, Gichangi P, et al. Gender difference in mortality among pulmonary tuberculosis HIV co-infected adults aged 15–49 years in Kenya. PLoS One. 2020;15(12):e0243977. doi:10.1371/journal.pone.0243977
17. Roshanaei G, Ghannad MS, Poorolajal J, Mohraz M, Molaeipoor L. Survival rates among co-infected patients with human immunodeficiency virus/tuberculosis in Tehran, Iran. Iran J Public Health. 2017;46(8):1123.
18. Satti H, McLaughlin MM, Hedt-Gauthier B, et al. Outcomes of multidrug-resistant tuberculosis treatment with early initiation of antiretroviral therapy for HIV co-infected patients in Lesotho. PLoS One. 2012;7(10):e46943. doi:10.1371/journal.pone.0046943
19. Tesfaye B, Alebel A, Gebrie A, Zegeye A, Tesema C, Kassie B. The twin epidemics: prevalence of TB/HIV co-infection and its associated factors in Ethiopia; A systematic review and meta-analysis. PLoS One. 2018;13(10):e0203986. doi:10.1371/journal.pone.0203986
20. Alemu A, Wubie Aycheh M, Dilnessa T. Tuberculosis and human immunodeficiency virus co-infection and associated factors at Debre Markos Comprehensive Specialized Hospital, Northwest Ethiopia: a Four-Year Retrospective Study. HIV/AIDS-Res Palliative Care. 2021;293–299. doi:10.2147/HIV.S284034
21. Refera H, Wencheko E. Survival of HIV-TB co-infected adult patients under ART in Ambo Referral Hospital, Ethiopia. Ethiop J Health Dev. 2013;27(2):88–93.
22. Beyene Y, Geresu B, Mulu A. Mortality among tuberculosis patients under DOTS programme: a historical cohort study. BMC Public Health. 2016;16(1):1–6. doi:10.1186/s12889-016-3557-0
23. Raviglione M, Director G. Global Strategy and Targets for Tuberculosis Prevention, Care and Control After 2015. Geneva: World Health Organization; 2013.
24. Gezae K, Abebe H, Gebretsadik L, Gebremeskel A. Predictors of time to death among TB/HIV co-infected adults on ART at two governmental hospitals in Mekelle, Ethiopia, 2009–2016: a retrospective cohort study. Ann Infect Dis Epidemiol. 2020;5(1):1049.
25. Health FMo. National Guidelines for Comprehensive HIV Prevention, Care and Treatment. Addis Ababa, Ethiopia: Federal Ministry of Health; 2017.
26. Aung ZZ, Saw YM, Saw TN, et al. Survival rate and mortality risk factors among TB–HIV co-infected patients at an HIV-specialist hospital in Myanmar: a 12-year retrospective follow-up study. Inter J Infect Dis. 2019;80:10–15. doi:10.1016/j.ijid.2018.12.008
27. Damtew B, Mengistie B, Alemayehu T. Survival and determinants of mortality in adult HIV/Aids patients initiating antiretroviral therapy in Somali Region, Eastern Ethiopia. Pan Afr Med J. 2015;22(1). doi:10.11604/pamj.2015.22.138.4352
28. Sileshi B, Deyessa N, Girma B, Melese M, Suarez P. Predictors of mortality among TB-HIV Co-infected patients being treated for tuberculosis in Northwest Ethiopia: a retrospective cohort study. BMC Infect Dis. 2013;13:1–10. doi:10.1186/1471-2334-13-297
29. Zhandybayeva A, Truzyan N, Shahumyan E, et al. The survival rate of tuberculosis patients in HIV-treated cohort of 2008–2018 in Almaty, Kazakhstan. J Infect Developing Countries. 2020;14(11.1):116S–21S. doi:10.3855/jidc.11955
30. Lelisho ME, Wotale TW, Tareke SA, et al. Survival rate and predictors of mortality among TB/HIV co-infected adult patients: retrospective cohort study. Sci Rep. 2022;12(1):18360. doi:10.1038/s41598-022-23316-4
31. Lelisho ME, Teshale BM, Tareke SA, et al. Modeling survival time to death among TB and HIV co-infected adult patients: an institution-based retrospective cohort study. J Racial Ethn Health Disparities. 2022;2022;1–13.
32. Tola A, Mishore KM, Ayele Y, Mekuria AN, Legese N. Treatment outcome of tuberculosis and associated factors among TB-HIV Co-infected patients at public hospitals of Harar town, eastern Ethiopia. A five-year retrospective study. BMC Public Health. 2019;19:1–12. doi:10.1186/s12889-019-7980-x
33. Gezae KE, editor. Predictors of accelerated mortality of Tb/Hiv Co- infected patients on art in Mekelle, Ethiopia: an 8 Years Retrospective Follow- Up Study; 2019.
34. Muyaya LM, Young T, Loveday M. Predictors of mortality in adults on treatment for human immunodeficiency virus-associated tuberculosis in Botswana: a retrospective cohort study. Medicine. 2018;97(16):e0486. doi:10.1097/MD.0000000000010486
35. Agbor AA, Bigna JJR, Billong SC, et al. Factors associated with death during tuberculosis treatment of patients co-infected with HIV at the Yaoundé Central Hospital, Cameroon: an 8-year hospital-based retrospective cohort study (2006–2013). PLoS One. 2014;9(12):e115211. doi:10.1371/journal.pone.0115211
36. Gesesew H, Tsehaineh B, Massa D, Tesfay A, Kahsay H, Mwanri L. The role of social determinants on tuberculosis/HIV co-infection mortality in southwest Ethiopia: a retrospective cohort study. BMC Res Notes. 2016;9(1):1–8. doi:10.1186/s13104-016-1905-x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.