")
Back to Journals » Open Access Journal of Sports Medicine » Volume 15
Tendinopathic Plantaris but Normal Achilles Tendon Found in About One-Fifth of Patients Not Responding to Conservative Achilles Tendon Management – Results from a Prospective WALANT Surgical Case Series on 105 Tendons
Authors Alfredson H, Waldén M , Roberts D, Spang C
Received 23 December 2023
Accepted for publication 28 March 2024
Published 10 April 2024 Volume 2024:15 Pages 41—45
DOI https://doi.org/10.2147/OAJSM.S456389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Håkan Alfredson,1,2 Markus Waldén,3,4 David Roberts,3 Christoph Spang5– 7
1Department of Community Medicine and Rehabilitation, Sports Medicine, Umeå University, Umeå, Sweden; 2Alfredson Tendon Clinic, Capio Ortho Center Skåne, Malmö, Sweden; 3Capio Ortho Center Skåne, Malmö, Sweden; 4Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden; 5Department of Integrative Medical Biology, Anatomy Section, Umeå University, Umeå, Sweden; 6Private Orthopaedic Spine Center, Würzburg, Germany; 7Institute for Sports Science, Würzburg University, Würzburg, Germany
Correspondence: Håkan Alfredson, Department of Community Medicine and Rehabilitation, Sports Medicine, Umeå University, Umeå, 90187, Sweden, Tel +46 (0) 702288441, Email [email protected]
Purpose: Midportion Achilles tendinopathy is a relatively common condition. This study aimed to investigate the presence of a normal Achilles tendon, but a tendinopathic plantaris tendon, in a large and consecutive prospective sample of patients referred to a specialised tendon clinic for midportion Achilles tendon pain not responding to non-surgical treatment.
Patients and Methods: A total of 105 consecutive tendons were operated on in 81 patients (62 males) suffering from painful midportion Achilles tendon pain. Clinical examination, ultrasound (US) and colour Doppler (CD) examination, and wide awake local anaesthetic no tourniquet (WALANT) surgery were performed in all patients.
Results: For 19/105 (18%) tendons from 14 patients, clinical examination suspected plantaris tendinopathy alone as there was a distinct tenderness on the medial side, but no thickening of the Achilles tendon. US examination followed by surgery confirmed the diagnosis.
Conclusion: Midportion Achilles tendon pain is not always related to Achilles tendinopathy since pain related to the plantaris tendon alone was found in almost every fifth patient. Consequently, there is an obvious need for proper examination to identify the pain source and establish a correct diagnosis before treatment.
Keywords: Achilles tendinopathy, surgery, plantaris, consecutive, ultrasound
Introduction
Painful midportion Achilles tendinopathy is a relatively common condition, affecting both professional/elite athletes, amateur/recreational athletes and sedentary/non-active individuals.1,2 A high proportion of these patients are cured or have sufficient symptom relief with different loading regimens,3,4 but surgical treatment can be needed for a sub-group of patients.
The role of plantaris tendinopathy, co-existing with midportion Achilles tendinopathy, has recently been highlighted.5–7 Tendinopathic plantaris tendons have been shown to exhibit similar histological changes as tendinopathic Achilles tendons.8,9 It has been hypothesized that in a subgroup of patients with Achilles tendon pain, where the anatomical location is very close, the two tendons interact with each other in the form of compressive or shearing forces.10,11 The richly innervated peritendinous connective tissue in between the two tendons where the interactions take place is thought to be the main pain driver.9 These patients suffer from pain and tenderness located on the medial side of the Achilles.12 Conservative management is challenging, and surgery is relatively often needed. Excellent short- and longer-term results from surgical removal of the plantaris tendon, together with a scraping procedure on the medial (peritendinous connective tissues) and ventral side of the Achilles tendon, have been shown in several studies.13–16
Recently, it has been discovered that plantaris tendinopathy alone, without co-existence of midportion Achilles tendinopathy, occurs in a subgroup of patients and can be related to loading-related pain often referred to the region of the Achilles midportion.17 Furthermore, histological studies have found that the plantaris tendon contains relatively frequent sensory innervation.9 These findings show that the plantaris tendon itself can be a pain driver in the Achilles tendon region.
The aim of the present study was to evaluate the frequency of plantaris tendinopathy alone in consecutive patients referred to a specialised tendon clinic for midportion Achilles tendon pain not responding to non-surgical treatment.
Materials and Methods
Patients and Inclusion Criteria
Swedish and international patients seeking help for persistent painful midportion Achilles tendon pain between August 2020 and November 2023 were consecutively included. All patients had tried non-surgical treatment including various loading regimens without effect.
Clinical Examination
All patients were evaluated and operated at the Alfredson Tendon Clinic, Capio Ortho Center Skåne, in Malmö, Sweden. Clinical examination and ultrasound (US) and colour doppler (CD) examination with high resolution greyscale (S-500, Siemens AG, Germany) using a linear multifrequency (8–13 MHz) probe was done pre-operatively (Figure 1A and B). During clinical examination the Achilles tendon was carefully palpated, a local thickening of the Achilles and local tenderness in relation to the Achilles or surrounding tissues was of special interest. Immediately prior to surgery, US + CD scanning was carried out to identify tendon changes, to apply skin markers to map the region with maximum palpation tenderness and to mark where the plantaris tendon was positioned in relation to the Achilles tendon.
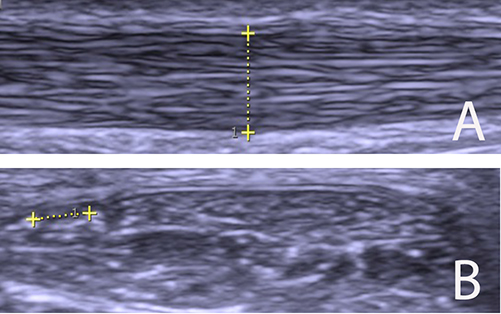 |
Figure 1 (A and B) Grey scale ultrasound pictures. (A) Longitudinal view showing a normal 4.5 mm thick Achilles tendon midportion. (B) Cross view showing a plantaris tendon (marked) localised close to the medial side of a normal Achilles tendon midportion. |
Surgical Procedure
This outpatient surgical treatment was performed exclusively under local anaesthesia, the so-called wide awake local anaesthetic no tourniquet (WALANT) surgery. After disinfecting the skin with wet cloths of chlorhexidine cutaneous solution (Klorhexidinsprit 5 mg/mL, Fresenius Kabi AB, Sweden), 4–5 mL of a local anaesthetic (Xylocain + adrenalin 10 mg/mL+5 μg/mL, Aspen, South Africa) was injected in the skin and subcutaneous tissues on the medial side (the mapped region) of the Achilles midportion. The skin was then carefully scrubbed and draped with a sterile paper-cover exposing only the midportion of the Achilles tendon.
A longitudinal skin incision (1.5–2 cm) was placed on the medial side of the Achilles midportion. Following blunt dissection, the plantaris tendon was carefully identified, released, and followed distally and proximally from the skin incision. The plantaris was cut in both ends, and 5–8 centimetres of the tendon was resected (Figure 2). Any vascularised fat tissue inter-positioned between the Achilles and the plantaris tendons was scraped away. The Achilles tendon was evaluated visually and by palpation. Following careful haemostasis using bipolar diathermy, the skin was closed by single non-resorbable sutures which were removed after 3 weeks. A sterile wound dressing was applied with elastic bandages from the toes to below the knee.
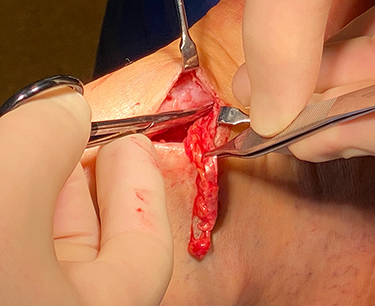 |
Figure 2 Picture from a patient with Plantaris tendinopathy alone, where 5–6 cm of a thickened plantaris tendon embedded in fat tissue is excised and removed from the medial side of a normal Achilles tendon midportion. |
Post-Operative Care and Rehabilitation
No post-operative thrombosis prophylaxis was used. Patients were supplied with a pain-killer bag consisting of Paracetamol (500 mg, 8 tablets), Diclofenac (50 mg, 2 tablets) and Oxycodone (5 mg, 1 tablet). After resting with an elevated foot for the first 12 hours after surgery, the patients were immediately mobilised with full weight-bearing as tolerated without crutches. All patients followed the same principal rehabilitation programme consisting of free range of motion exercises and gradually increased walking and light biking in week 1, followed by free walking and biking in weeks 2 and 3. Sutures were removed after 3 weeks, and then more sport-specific loadings, such as running, were gradually introduced.
Ethics
Informed consent was obtained from all patients. The study was conducted in accordance with the Declaration of Helsinki and approved by the Umeå University Ethical Board (ref. no. 2011/83-32M).
Statistics
Only descriptive statistics was used reporting absolute numbers and percentages.
Results
There were 81 patients (62 males and 19 females) with a long duration (>6 months) of pain in altogether 105 Achilles midportions. The median age for males was 47 (range 22–70) years and for females was 46 (range 23–64) years. In total, 21 patients were elite athletes, 42 were recreationally actives and 18 patients were non-active individuals. The elite athletes were active in different sports: football (n=9), marathon running (n=3), triathlon (n=2), orienteering (n=2) hurling (n=2), handball (n=1) cross-country skiing (n=1), middle distance running (n=1).
For the patients having plantaris tendinopathy alone, 10/14 were elite athletes, 3/14 were recreational athletes and 1/14 was a non-active individual.
Clinical examination: In these 14 patients (19/105 tendons), there was distinct tenderness on the medial side of the Achilles midportion, but no thickening of the Achilles tendon.
US and CD examination: In the same 14 patients (19/105 tendons), there was a plantaris tendon localised close to the medial side of a normal (regular fiber structure and thickness < 6 mm) Achilles tendon.
Surgery: In 14 patients (19/105 tendons) a plantaris tendon of varying size (width and thickness) was found in close relation to the medial side of a macroscopically normal Achilles midportion (Figure 2.).
Discussion
The principal finding of this study on 81 consecutive patients (105 tendons), referred to a tendon clinic for midportion Achilles tendon pain not responding to traditional non-surgical treatment, was that there was plantaris tendinopathy alone and a normal Achilles tendon in almost one-fifth of tendons.
Recent research has shown that all patients have a plantaris tendon, but there are many different positions for the plantaris tendon in relation to the Achilles tendon.6,18 Furthermore, the histology and innervation patterns for the plantaris tendon have recently been clarified; these studies show that the plantaris tendon can be tendinopathic, and both the tendon itself and the surrounding fat tissue can have a rich sensory innervation.8,9 This new information is clinically relevant when managing patients with pain in the Achilles tendon region.
The relatively high proportion of plantaris tendinopathy alone in the current study was a surprising finding, and clearly demonstrates the importance of using appropriate diagnostic tools, such as careful palpation and US + CD scanning, to identify the pain source and establish a correct diagnosis before treatment is initiated. We see two major reasons for not using a casual approach without imaging support. First, for patients with painful Achilles midportion, but having a normal Achilles on clinical examination and US + CD scanning, it is important to know that the pain likely is caused by the plantaris tendon, and this pain can be treated successfully via surgical removal of the plantaris tendon. Unfortunately, it is our experience that many of the patients with plantaris tendinopathy alone have been dismissed and told that because the Achilles was found normal the pain was likely a sign of central non-structural pain or mental weakness. Second, the pain from plantaris tendinopathy seems to respond poorly to classical treatment with various loading regimens. This is supported by findings from studies on midportion Achilles tendinopathy with plantaris tendon involvement, where treatment with eccentric training has been indicated to cause a worsening with localised sharp pain on the medial side of the Achilles midportion.5,7 Altogether, we would like to push for the use of US examination in skilled hands, and not only patient history and a casual clinical examination, for proper diagnostics;13 US is often considered as the first-line imaging modality for tendon pain.
For both the clinician and the researcher, it is important to know that the plantaris tendon can be involved in two separate clinical entities of the Achilles tendon region, the midportion and the insertion. In the latter, there are often multiple tissues and pathologies involved with subcutaneous and retrocalcaneal bursitis, Achilles and plantaris tendinopathy,19 and bony spurs/calcifications (insert ref), whereas the novel finding in the present study is that plantaris tendon can be the sole contributor to midportion pain.
Conclusion
In conclusion, pain in the Achilles midportion is not always related to Achilles tendinopathy. In this study, pain related to the plantaris tendon alone was found in almost one-fifth of patients in this large consecutive sample from a specialised tendon clinic. It is of high clinical value to know that the plantaris tendon alone can cause pain, and there is, therefore, an obvious need for proper examination to establish a correct diagnosis before treatment.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. De Jonge S, Van den Berg C, De Vos RJ, et al. Incidence of midportion Achilles tendinopathy in the general population. Br J Sports Med. 2011;45:1026–1028. doi:10.1136/bjsports-2011-090342
2. Fahlström M, Jonsson P, Lorenzon R, Alfredson H. Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg Sports Traumatol Arthrosc. 2003;11:327–333. doi:10.1007/s00167-003-0418-z
3. Murtaugh B, Ihm J. Eccentric training for the treatment of tendinopathies. Curr Sports Med Reports. 2013;12(175):182. doi:10.1249/JSR.0b013e3182933761
4. Alfredson H, Pietilä T, Lorentzon R, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998;26:360–366. doi:10.1177/03635465980260030301
5. Alfredson H. Midportion Achilles tendinosis and the plantaris tendon. Br J Sports Med. 2011;45:1023–1025. doi:10.1136/bjsports-2011-090217
6. Spang C, Alfredson H, Docking SI, Masci L, Andersson G. The plantaris tendon: a narrative review focusing on anatomical features and clinical importance. Bone Joint J. 2016;98-B:1312–1319. doi:10.1302/0301-620X.98B10.37939
7. Alfredson H. Persistent pain in the Achilles mid-portion? Consider the plantaris tendon as a possible culprit! Br J Sports Med. 2017;51:833–834. doi:10.1136/bjsports-2016-097360
8. Spang C, Alfredson H, Ferguson M, Roos B, Bagge J, Forsgren S. The plantaris tendon in association with mid-portion Achilles tendinosis: tendinosis-like morphological features and presence of a non-neuronal cholinergic system. Histol Histopathol. 2013;28:623–632. doi:10.14670/HH-28.623
9. Spang C, Harandi VM, Alfredson H, Forsgren S. Marked innervation but also signs of nerve degeneration between the Achilles and plantaris tendons and presence of innervation within the plantaris tendon in midportion Achilles tendinopathy. J Muculoskeletal Neuronal Interact. 2015;15:197–206.
10. Smith J, Alfredson H, Masci L, Sellon JL, Woods CD. Differential plantaris-achilles tendon motion: a sonographic and cadaveric investigation. PM R. 2017;9(7):691–698. doi:10.1016/j.pmrj.2016.10.013
11. Cook JL, Purdam C. Is compressive load a factor in the development of tendinopathy? Br J Sports Med. 2012;46(3):163–168. doi:10.1136/bjsports-2011-090414
12. Masci L, Spang C, van Schie H, Alfredson H. How to diagnose plantaris tendon involvement in midportion Achilles tendinopathy - clinical and imaging findings. BMC Musculoskeletal Disord. 2016;17:97. doi:10.1186/s12891-016-0955-5
13. Masci L, Spang C, van Schie HT, Alfredson H. Achilles tendinopathy-do plantaris tendon removal and Achilles tendon scraping improve tendon structure? A prospective study using ultrasound tissue characterisation. BMJ Open Sport Exerc Med. 2015;1(1):e000005. doi:10.1136/bmjsem-2015-000005
14. Masci L, Neal BS, Wynter Bee W, Spang C, Alfredson H. Achilles scraping and plantaris tendon removal improves pain and tendon structure in patients with mid-portion Achilles tendinopathy-A two-year follow-up case series. J Clin Med. 2021;10:2695. doi:10.3390/jcm10122695
15. Calder JD, Freeman R, Pollock N. Plantaris excision in the treatment of non-insertional Achilles tendinopathy in elite athletes. Br J Sports Med. 2015;49(23):1532–1534. doi:10.1136/bjsports-2014-093827
16. Bedi HS, Jowett C, Ristanis S, Docking S, Cook J. Plantaris excision and ventral paratendinous scraping for achilles tendinopathy in an athletic population. Foot Ankle Int. 2016;37(4):386–393. doi:10.1177/1071100715619989
17. Alfredson H, Masci L, Spang C. Surgical plantaris removal for patients with plantaris tendon related pain only and a normal Achilles tendon: a case series. BMJ Open Sp Exerc Med. 2018;4:000462.
18. van Stekenburg MN, Kerkhoffs GM, Kleipool RP, van Dijk NC. The plantaris tendon and a potential role in mid-portion Achilles tendinopathy: an observational anatomical study. J Anatomy. 2011;218:336–341. doi:10.1111/j.1469-7580.2011.01335.x
19. Alfredson H, Masci L, Spang C. Ultrasound and surgical inspection of plantaris tendon involvement in chronic painful insertional Achilles tendinopathy: a case series. BMJ Open Sport Exerc Med. 2021;7(1):e000979. doi:10.1136/bmjsem-2020-000979
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.