")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
The Effect of an Education Program on School Children Oral Health in Khartoum, Sudan
Authors Albani GFAA, Abdelgadir WI, Mohamed AAA , Yousif M, Mustafa AMA, Almkiy EAA , Mohammed KZM, Mohamed EAS, Alghamdi FAA, Ahmed RG , Hakami MSA, Dinar NA, Alsulami A , Mudawi AIA, Ahmed WAM
Received 14 November 2023
Accepted for publication 23 February 2024
Published 12 March 2024 Volume 2024:17 Pages 1065—1077
DOI https://doi.org/10.2147/JMDH.S446487
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Galal Faisal Abdulqader Abdulla Albani,1 Widad Ibrahim Abdelgadir,2,3 Amal Abdelgadir Ali Mohamed,4 Magda Yousif,5 Amna Mohammed Ali Mustafa,6 Egbal Abbashar Algmair Almkiy,7,8 Khadiga Z M Mohammed,4,9 Eman Ahmed Saad Mohamed,7 Fahad Abdullah A Alghamdi,10 Raga Gasim Ahmed,11 Manal SA Hakami,10 Niemat A Dinar,10 Amal Alsulami,2 AbdAllah Ibrahim AbdAlrahman Mudawi,12 Waled AM Ahmed10
1Department of Nursing, Faculty of Medical Sciences, Aljanad University for Science and Technology, Taiz, Yemen; 2Department of Community Health Nursing & Mental Nursing Sciences College of Nursing,Taif university, Taif, Saudi Arabia; 3Faculty of Nursing Sciences Bahri University, Sudan; 4Department of Maternal and Child Nursing Sciences College of Nursing,Taif university, Taif, Saudi Arabia; 5Nursing Department, Prince Sultan Military College of Health Sciences, Dhahran, Saudi Arabia; 6Faculty of Nursing Sciences, Jazan University, Jazan Saudi Arabia; 7Department of Nursing, Faculty of Applied Medical Sciences, Buraydah College, Buraydah, Saudi Arabia; 8Faculty of Nursing Sciences, Alneelain University, Sudan; 9Nursing Faculty, Zagazig University, Zagazig, Egypt; 10Faculty of Nursing, Al-Baha University, Al-Baha, Saudi Arabia; 11Department of Nursing, Faculty of Applied Medical Sciences, Al-Baha University, Al-Baha, Saudi Arabia; 12Oral and Dental Health Department, Faculty of Applied Medical Sciences, Al-Baha University, Al-Baha, Saudi Arabia
Correspondence: Waled AM Ahmed; Amal Abdelgadir Ali Mohamed, Tel +966508245369; +966550367392, Email [email protected]; [email protected]
Background: Oral health education programs have long been considered an essential part of oral health policies. This is important for reducing the risk of oral diseases through health enhancement and voluntary behavioral changes due to learning opportunities. This study aimed to evaluate the effects of school-based oral health education program on oral health in school children in Sudan.
Methods: A quasi-experimental study was conducted at four governmental schools in Khartoum, Sudan, between August 2018, and March 2022. A total of 423 school children were randomly allocated into the control (n = 211) and study (n = 212) groups. An adapted questionnaire was administered to students before and after the intervention to assess their knowledge and practice of oral health. The study group participated in oral health education activities. Data were analyzed using the Statistical Package for the Social Sciences (SPSS), version 21.
Results: The findings revealed that the mean knowledge at the pre-educational program was 9.3066 (SD = 3.91078) and the mean knowledge after the educational program was 21.2736 (SD = 2.13982). The scores indicated that the school children had significantly higher knowledge and practice scores after the oral health education program.
Conclusion: The study concluded that education program on oral health improved students’ oral health knowledge and practices. Imposing theoretical and practical lessons on oral and dental health in school curricula can motivate students to maintain oral health care, and this improves oral health status.
Keywords: education program, school children, oral health, knowledge, practice, Sudan
Introduction
The high cost of dental care has a direct economic impact on individuals, families, and communities. Therefore, prevention remains a more cost-effective method, with most dental diseases being avoided by upholding healthy oral hygiene habits.1
Schools are the most common place where traumatic dental injuries occur, followed by home.2 Childhood is a high-risk period in terms of vulnerability to injuries. However, certain oral-facial accidents can be avoided through self-discipline and environmental precautions, such as railings, good lighting, smooth walkways, and proper injury-prevention education. Sport-related orofacial injuries can be avoided by wearing mouthguards or helmets.
Childhood circumstances, as indicated by socioeconomic status, family structure, and parenting quality, have been shown to have a strong influence on children’s health and well-being3 have been significantly associated with poor oral health status in children.4 However, this is not always the case, with conflicting findings from a few studies in which parental socio-economic status and home environment characteristics were found to be insignificant in predicting children’s oral health status. Additionally, a study conducted in Kabul showed that Health professions students’ oral health knowledge, attitudes, and behaviors are associated with their level of education.5
Oral health education programs have long been considered integral to many oral health policies for a long time.6 Oral health education and promotion can be provided in various forums, such as hospitals, primary health centers, private dental clinics, and schools. Schools are probably the best place to improve oral health, since approximately one billion children worldwide spend much of their daily lives there.7 School-aged adolescents particularly need preventive programs to ensure positive long-term dental health and hygiene. However, owing to a lack of health education and insufficient preventive measures, there is a high prevalence of morbidity, and the health status of these students is not good always.7 Increasing levels of dental caries among children are observed in some developing countries, especially in those where community- and school-based preventive oral care programs are not established.8
Evidence has shown that an increase in knowledge about risk factors for oral diseases and strong knowledge of oral health demonstrates better oral care practices that aim to promote healthy habits.7 Moreover, school children with inadequate oral health knowledge were twice as likely to have caries as those with adequate knowledge.9 Al-Hakimi et al conducted a study in Sudan et al showed that education was significantly associated with knowledge of oral cancer and its factors.10 This study aimed to assess the effects of school-based oral health education programs on oral health promotion among school children. The following question was raised: Is a school-based oral health education program effective in improving oral health knowledge among school children in the Khartoum state?
Materials and Methods
Study Design: A quasi-experimental study (pre-post-test) was conducted in government schools in Khartoum, Sudan.
Study area: This study was conducted in Khartoum State, the capital of Sudan, which has the largest population. Khartoum State, one of the 18 states of Sudan, has the largest collection of government schools in Sudan.
Study setting: Four governmental were included as indicated in Table 1:
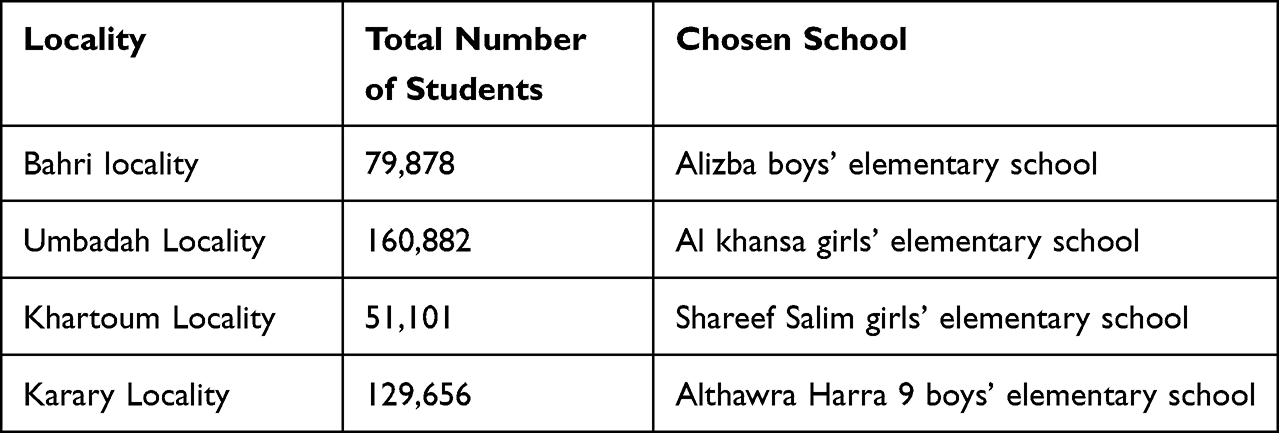 |
Table 1 Distribution of Students in Different Localities in Khartoum, Sudan |
Study population: The study included all school children in Khartoum state during the time of data collection. Students at selected schools who were willing to participate were included in this study. Students who were not selected. Students who did not agree to participate were excluded.
Sampling technique: This study used a cluster-randomized sampling technique to select, from Khartoum State, four localities: from each locality, one administrative sector was selected randomly; from each sector, one school was selected randomly within each school, and the eighth grade was selected as a cluster.
They were randomly assigned into two groups: two clusters (one girls’ school and one boys’ school) were designated as intervention group, and two clusters (one girls’ school and one boys’ school) were designated as control group. It is shown in Table 2.
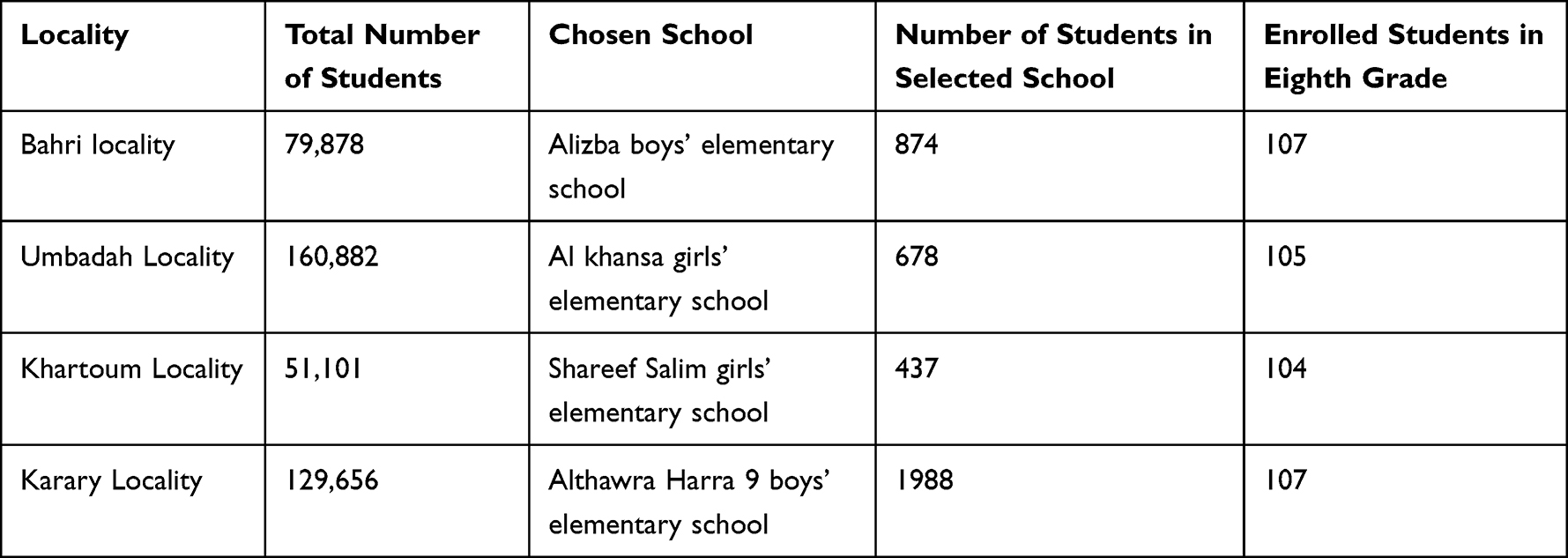 |
Table 2 Distribution of Students in the Selected Schools and in Eighth Grade |
Sample size: The sample size of 384 students was estimated using Cochran’s equation.11

where z = 1.96 for, confidence level (α) = 95%, p = proportion (expressed as a decimal), e is the margin of error.
z = 1.96, p = 0.5, e = 0.05, N = 82,320.
[(1.96)2 * 0.5 * (1–0.5)/(0.05)2]/[1 + (1.96)2 * 0.5 * (1–0.5)/((0.05)2 * 82,320)]= 384
Power analysis was conducted in this study using a power of 0.80, an alpha level of 0.05 (0.05 probability of type 1 error), and a conservative medium effect size of 0.25. The power analysis in this study indicated the need for a sample size of 440 students to avoid type II errors. To minimize factors such as refusal to participate, attrition, missing data, and incomplete data, the final sample size was increased from 382 to 440 students. Questionnaires distributed to 440 participants and returned by 423 students, for a response rate of 96%; the overall response rate was acceptable. Approximately 4% of the students did not complete the study.
Data collection process: The study was designed in three phases: assessment, implementation, and evaluation. The author started by introducing himself to school principals and teachers and giving them a brief idea of the study’s aim.
Assessment phase: This stage served to identify the baseline knowledge of the students who participated in the study and had been informed about the nature and purpose of the study before implementation of the program. Consent forms were obtained from all the participants and their parents. The author filled out the questionnaire in the students’ classrooms and took–15–20 minutes for each participant. The program was implemented to students in the classroom in terms of sessions and teaching on the spots to enhance knowledge about oral and dental health, and pre-tests were conducted.
Implementation phase: an educational program regarding oral and dental health among school-age children was designed by the researcher based on the available research and literature for the study group. The intervention was conducted in Arabic (the national language in Sudan) to cover the relevant theoretical and practical aspects of oral health among school children. The authors used different teaching methods such as lectures, discussions, demonstrations, and demonstrations. In addition, different assistive learning methods were used, such as pamphlets, small books, show pictures, posters, and real equipment. The intervention was implemented in small groups (typically, class-wise). The program was implemented in 2–3 sessions weekly. Each session took approximately one hour. The program was implemented in two parts, first part includes knowledge of dental care information (definition, importance of oral care, and causes of common oral diseases) and practices regarding oral care (regularity of tooth care, exact time of toothbrush, and the main equipment for toothbrush). The 2nd part includes prevention measures and oral care practices (diet and prevention, student responsibilities to prevent oral and dental problems, and how to brush, floss, and rinse teeth). The oral health education program covered all topics in the questionnaire and emphasized the following three messages (brushing teeth twice per day, healthy diet, and regular dental visits twice per year). At the end of the session, 15 min were assigned for discussion and answering the students’ questions. The total duration of the program was 30 hours.
At the end of the program, a post-test was conducted for both groups.
Control group: No intervention was performed on the control group (211 students). Only the pre-test and post-test were performed.
Evaluation phase: Post-test was carried out after the completion of the educational program for both the study and control groups, which was conducted by interviewing the students in classrooms. Each subject was evaluated using an author-administered structured questionnaire to determine the improvement in students’ knowledge and compare the groups.
Data collection tools: The tools were designed, and appropriate questions were selected and adapted to form a rough version of these tools. An interview close-ended structured questionnaire filled out by the author was used to collect data. It was designed by the author based on related literature (Figure S1). The questionnaire consists of three parts:
Part 1: consisted of six questions about the demographic data of the students (age, sex, mother’s education, father’s education, mother’s work, and father’s work), and Part 2: consisted of 11 questions with multiple options related to students’ knowledge of oral and dental health. Part 3: consisted of 12 questions with multiple options related to students’ knowledge of oral and dental-care practices.
Pilot study and Validity of the tool: Face and content validity were established by a panel of five experts who revised the tools for clarity, relevance, applicability, comprehensiveness, understanding, and ease of implementation; minor modifications were applied according to their opinions. The pilot study was conducted at Alizba Boys Elementary School. Forty students participated in a pilot study to test the questionnaire for confusion and ease of understanding. Participants were requested to make notes if there was any difficulty in understanding the meaning of the questions and the time required to complete the questionnaire. The data were entered into Statistical Package for the Social Sciences (SPSS) to conduct an appropriate analysis test to measure the tool validity and reliability. The final version of the questionnaire was used for data collection. Cronbach’s alpha was reported to be 0.79, indicating that the tool was reliable and valid.
Fieldwork: An official letter from the University of Bahri was addressed to the General Directors of governmental primary schools, and permission was obtained to conduct the study. After obtaining permission, the researchers met students in the classrooms and explained the purpose of the study to them. Parental consent was obtained before any student participated in this study. After that, the author collected pre-test information from structured questionnaires from the students of both groups (study and control groups) to assess existing knowledge regarding oral and dental health. The author then implemented an interventional program for the study group, whereas students in the other group received no oral health education programs. This was followed by a post-test to reassess students’ knowledge after implementing the program. After implementing the intervention program, post-tests were collected from the students in both groups to reassess their knowledge after implementing the program.
Data analysis: Data were collected, computed, and statistically analyzed using the Statistical Package for Social Sciences (SPSS) version 21.0.0. Descriptive and inferential statistics were used in this study. Data are presented in the form of tables of frequencies, percentages, means, and standard deviations for quantitative variables. To measure the differences between the study and control groups at pre-test and post-test, the paired sample t-test and ANOVA t-test chi-square were used to detect significant differences among participants’ demographic and behavioral variables.
Results
Table 3 shows the distributions of participants according to demographic variables (n=423) clarified that 50.5% of school’s children of the study group were male. On the other hand, male gender of the control group was 50.7%. Most participants were 13 years old, 55.2% in the study group, while in the control group the majority were 14 years old 42.2%. It highlights that most of student’s fathers are employed in both groups (study group n=212 and control group n=211) with 66.5%, 67.3% respectfully. In addition to distribution of student’s mothers according to work status. It highlights that most of student’s mothers are housewives in both groups (study and control group) with 65.6%, 78.7%, respectively, it shows distribution of participants according to Father’s education level, majority of fathers are graduated in both group (study and control group) with 62.3%, 51.3%, respectively. The table illustrates that half of mothers of students in study group (n=212) graduated 50%. While the graduated mothers of students in the control group (n=211) were 44.1%.
 |
Table 3 Distributions of Participants According to Demographic Variables (n = 423) |
Table 4 points out the distribution of participants according to having artificial teeth or undergoing orthodontic treatment, and the reasons for previous visits to the dentist (n=423). Most students did not go for orthodontic treatment in both groups (study and control group) with 98.1%, 91.5%, respectively).
 |
Table 4 Distributions of Participants According to Having Artificial Teeth or Going for Orthodontic Treatment and the Reasons for Previous Visit to the Dentist (n = 423) |
Table 5 reflects knowledge and practice of school children regarding oral health for study group (n=212) and control group (n=211). The result showed that the mean of knowledge at pre-educational program level was 9.3066 (SD = 3.91078), and the mean of knowledge at post-educational program was 21.2736 (SD = 2.13982). Scores indicated school children had a significant score knowledge and practice post-oral health educational program. The result showed that the mean of practice at pre-test level was 4.3460 (SD = 1.58057), and the mean of practice at post-test level was 4.3602 (SD = 1.58057). Scores indicated school children did not have a significant score of knowledge and practice within control group. The results showed that the school children who participate in study group have highly significant score of knowledge than school children who participate in control group at pre-test and post-test level (p = 0 0.013), (p = 0.000), respectively. The result showed that the school children’s who participate in the study group have highly significant score of practice than school children’s who participate in control group at post-test level (p = 0.000).
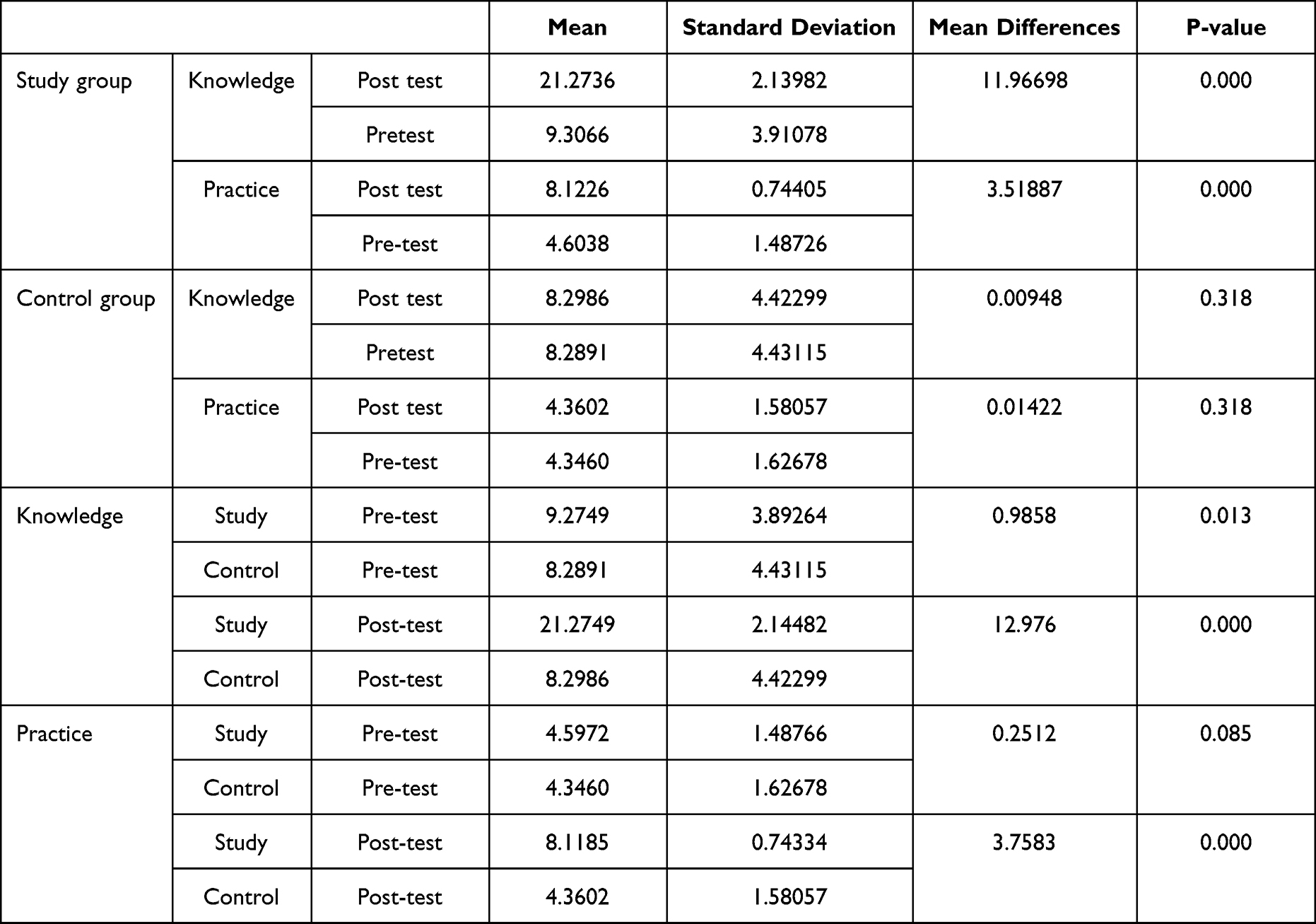 |
Table 5 Knowledge and Practice of School Children Regarding Oral Health for Study Group (n = 212) and Control Group (n = 211) |
Table 6 presents the levels of knowledge and practice of school children regarding oral health according to demographic variables for study group (n = 212) The female gander had higher score of Knowledge at post-test level (M = 23.0762, P = 0.000). The thirteen years old school children’s had higher scores of Knowledges at pre-test level (M = 10.0342, P = 0.004) while no significance was observed according to school children’s age at post-test. The school children of Khartoum locality had higher score of Practice at post-test level (M = 8.3810, P = 0.000). The school children of retired father had higher score of Practice at pre-test level (M = 5.2083, P = 0.014). The Employee mother had higher score of Practice at pre-test (M = 4.9041, P = 0.033) and post-test level (M = 8.3014, P = 0.011). No significant difference observed for practice at pre- and post-test father’s statues of education. The mother who had Khalwa educations had higher score of Practice at pre-test (M = 5.7500, P = 0.011) and post-test (M = 8.9167, P = 0.000).
 |
Table 6 Association Between Knowledge and Practice of School Children Regarding Oral Health According with Demographic Variables for Study Group (n = 212) |
Table 7 shows the distributions of participants according to having artificial teeth or going for orthodontic treatment (n = 423). The table shows the distribution of participants according to having artificial teeth or going for orthodontic treatment. It illustrated that most students did not go for orthodontic treatment in both groups (study and control group) with 98.1%, 91.5%, respectively.
 |
Table 7 Distributions of Participants According to Having Artificial Teeth or Going for Orthodontic Treatment (n = 423) |
Table 8 reflects knowledge and practice of school children regarding oral health according to mother’s work for study group (n=212). The table reflects the differences in total score of knowledge and practice of school children regarding oral health according to their mother’s statues of employment for Study group. The Employee mother had higher score of Practice at pre-test (M = 4.9041, P = 0.033) and post-test level (M = 8.3014, P = 0.011).
 |
Table 8 Knowledge and Practice of School Children Regarding Oral Health According to Mother’s Work for Study Group (n = 212) |
Table 9 presents the levels of knowledge and practice of school children regarding oral health according to father education for study group (n = 212). The table reflects the differences in total score of Knowledge and practice of school children’s regarding oral health according to their father’s statues of education for Study group. No significant difference was observed for practice at pre- and post-test father’s statues of education.
 |
Table 9 Knowledge and Practice of School Children Regarding Oral Health According to Father Education for Study Group (n = 212) |
Discussion
The school years covered the period from childhood to adolescence. These are influential stages in people’s lives when lifelong sustainable oral health-related behaviors, beliefs, and attitudes are being developed.12 As children are particularly receptive during the school years, and the earlier the habits are established, the longer the impact lasts. The present study aimed to evaluate the impact of school-based oral health education programs on the level of knowledge and practice of school children regarding oral health in Khartoum state.
The findings of the sociodemographic profile of the participants indicated that 50.5% of school’s school children in the study group were male, while female was 49.5%. On the other hand, male gender of the control group and 50.7%, the female was 49.3%. The age range of all participants was 13–16 years with a mean age of 14.5 ± 1.5. Participants age was 13 years old in 55.2% of the study group and 34% of the sample were 14 years old, while control group the majority were 14 years old 42.2%), and 35.5% of the sample were 13 years old. It is normal for students in the same grade to be an approximate age. However, no statistically significant differences were found between the two groups of subjects with respect to sex.
The results showed that the oral health education program was effective in improving participants’ oral health knowledge and practice in the group enrolled in the educational program. Overall, the baseline mean knowledge score was 9.30 ± 3.91 and after the intervention, the mean knowledge increased to 21.27 ± 2.14. After the intervention, the mean practice score was 4.60 ± 1.49 and after the intervention, the mean practice increased to 8.12 ± 0.74. There was a statistically significant increase in oral health knowledge and practice after the program implementation (P<0.000). There was a statistically significant improvement in the knowledge and practice of the study group, whereas there was no change in the knowledge and practice of the control group. The same finding was reported by Haque et al that an education program led to increasing school-aged knowledge and practices scores toward oral health, with a statistically significant difference (p < 0.001).7
In the comparison between the study group and control group, the results of the current study showed that the school children who participate in the study group had a significantly higher knowledge score than those who participate in the control group at the post-test level (p = 0.000). This finding is supported by a previous study by De Farias et al. They reported that there was a statistically significant difference (P < 0.001) between the number of correct answers in the questionnaire after the educational intervention and that the control group had a 10-fold greater likelihood of obtaining wrong answers.13 This clearly reveals that students’ oral health-related knowledge improved through oral health education.
Regarding oral health care practice, there was no significant practice score between the study and control group in the pre-test in the current study (p=0.085), which could be due to the similarity of sources of information. In comparison to the post-test level, the school children who participate in the study group had a significantly higher practice score than those who participate in the control group (p = 0.000). The results obtained by Haleem et al proved that oral health education programs are effective in enhancing oral health behavior and oral hygiene status of students in the study group when compared with students in the control group.14 Knowledge of oral health is considered an essential prerequisite for health-related practices and studies have shown an association between increased knowledge and improved oral health. Knowledge is derived from information that when accepted and believed is translated into action, which in turn becomes a habit. A good knowledge of oral health is essential for oral health behavior.15,16
The association between gender and the total knowledge and practice score for the study group in the current study showed that males had a higher knowledge score at the pre-test level (M = 9.8692, P = 0.034), while females had a higher knowledge score at the post-test level (M = 23.0762, P = 0.000). In addition, female gander had a higher score of Practice at the post-test level (M = 8.3810, P = 0.000). This may have been due to the motivation of these girls due to the educational resources used in the school. However, the educational resources used in schools may not be exciting for male students in these classrooms.
The current study examined the relationship between the total knowledge and practice score of school children regarding oral health according to their parents’ employment status in the study group. The school children of retired fathers had higher Practice scores at the pre-test level (M = 5.2083, P = 0.014), while no significant differences were observed at the post-test level. This may be because retired fathers tend to spend more time with their children, which gives them more opportunities to provide advice, instruction, and guidance to their children. The students of employee mothers had higher knowledge scores at the post-test level (M = 21.7260, P = 0.025). In addition, the students of the employee mother had higher scores on the Practice at the pre-test (M = 4.9041, P = 0.033) and post-test levels (M = 8.3014, P = 0.011). Being in paid employment allows them to invest more in health care and afford a healthier lifestyle, and employees may receive benefits such as health insurance and housing. On the other hand, students with fathers who had Khalwa education had higher score of knowledge at pre-test level (M = 15.0000, P = 0.000).
However, no significant difference was observed in practice at pre- and post-test fathers’ education (Khalwas is an Islamic educational institution in Sudan. Most such schools are for boys who wish to study and memorize the Quran, read, and write Arabic and study Fiqh (Islamic jurisprudence). There are some Khalawi for girls in some areas of the country. The teacher of the Khalwa is usually referred to as a Shaykh). Furthermore, students of mothers with secondary education had higher score of knowledge at pre-test level (M = 10.8393, P = 0.008). The students of mothers who had Khalwa education had higher scores on the Practice pre-test (M = 5.7500, P = 0.011) and post-test (M = 8.9167, P = 0.000). Parents’ knowledge and attitudes about the importance of oral health care and their fear of dental treatment have influenced their children’s dental care.17 Moreover, the social environments in which children live (relatives, friends, classmates, teachers, etc.) are mainly responsible for their encouragement to perform any behavior.
Conclusion
Based on these results, the study concluded that education programs on oral health had positive effects on students’ oral health knowledge and practice. The improvement in school children’s oral health knowledge and practice can motivate them to maintain oral health care, which improves their oral health status.
Data Sharing Statement
Data for this study are available upon request. Interested individuals can contact the corresponding author (Galal Faisal Abdulqader Abdulla Albani) to obtain access to data.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the Ethics Committee of the International University of Africa in Sudan (reference number IUA/FM/18/08/18-28). This study was conducted in compliance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants, who were informed of their right to decline participation or withdraw from the study at any time. Written informed consent indicated that the participants had the right to decline or withdraw at any point during the study, which was obtained from all participants and from the parents or legal guardians of all participants under the age of 18 years. Furthermore, confidentiality was ensured for each participant.
Acknowledgments
The authors express their appreciation to the study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the authors.
Disclosure
The authors declare no competing interests to be addressed.
References
1. Singh H, Singhal S. Evidence Brief: Behavioural Impacts of School-Based Oral Health Education Among Children. Ontario Agency for Health Protection and Promotion (Public Health Ontario); 2017.
2. Ogordi PU, Ize-Iyamu IN, Adeniyi EO. Prevalence of traumatic dental injury to the anterior teeth in children attending paramilitary and nonparamilitary schools in Nigeria. Ann Afr Med. 2019;18(2):80. doi:10.4103/aam.aam_27_18
3. Hosokawa R, Katsura T, Wasserman D. Association between mobile technology use and child adjustment in early elementary school age. PLoS One. 2018;13(7):e0199959. doi:10.1371/journal.pone.0199959
4. Kumar G, Tripathi RM, Dileep CL, et al. Assessment of oral health status and treatment needs of Santhal tribes of Dhanbad District, Jharkhand. J Int Soc Prev Community Dent. 2016;6(4):1.
5. Ehsan H, Ahmadzai N, Orfani Z, Rezayee BM, Wally M, Daftani S. Oral health knowledge, attitude, and behavior among health professions’ students at Kabul University of medical sciences. Clin Cosmetic Invest Dentistry. 2023;349–358. doi:10.2147/CCIDE.S444093
6. Chandrapooja JaJ G. Effectiveness of good behavior game on oral health among children-A randomized trial. Drug Invention Today. 2018;10(8):1.
7. Haque SE, Rahman M, Itsuko K, et al. Effect of a school-based oral health education in preventing untreated dental caries and increasing knowledge, attitude, and practices among adolescents in Bangladesh. BMC Oral Health. 2016;16(1):44. doi:10.1186/s12903-016-0202-3
8. Alrmaly B, Assery MK. Need of oral health promotion through schools among developing countries. J Int Oral Health. 2018;10(1):1.
9. Ghazali N, Mohamad Jan AS, Shukran AS. Assessment between oral health knowledge, attitude and practice with dental caries among 6-years-old private pre-school children. Int J Stud Child Women Elder Disabl. 2018;3:184–190.
10. Al-Hakimi HA, Othman AE, Mohamed OG, Saied AM, Ahmed WA. Public knowledge of oral cancer and modelling of demographic background factors affecting this knowledge in Khartoum State, Sudan. Sultan Qaboos Univ Med J. 2016;16(3):e335–e340. doi:10.18295/squmj.2016.16.03.012
11. Cochran WG. The combination of estimates from different experiments. Int Biom Soc. 1954;10(1):101–129. doi:10.2307/3001666
12. Prabhu SaJ J. Oral health education for improving oral health status of school children—a systematic review. J Dent Med Sci. 2015;14(2):101–106.
13. de Farias IA, De Araújo Souza GC, Ferreira MÂF, et al. A health education program for Brazilian public schoolchildren: the effects on dental health practice and oral health awareness. J Public Health Dent. 2009;69(4):225–230. doi:10.1111/j.1752-7325.2009.00127.x
14. Haleem A, Siddiqui MI, Khan AA. School-based strategies for oral health education of adolescents--a cluster randomized controlled trial. BMC Oral Health. 2012;18:54.
15. Al-Qahtani SM, Razak PA, Khan SD. Knowledge and practice of preventive measures for oral health care among male intermediate school children in Abha, Saudi Arabia. Int J Environ Res Public Health. 2020;17(3):703. doi:10.3390/ijerph17030703
16. Togoo RA, Yaseen SM, Zakirulla M, et al. Oral hygiene knowledge and practices among school children in a rural area of southern Saudi Arabia. Int J Contemp Dentistry. 2012;3(1):1.
17. Priya MM, Kumar P, Saraswathi S. Assessment of parental oral health knowledge, attitude, and behavior. J Pharm Res. 2018;12(1):47–50.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.