")
Back to Journals » Journal of Pain Research » Volume 17
The Effect of Singular Nonverbal Behaviours of Experimenters on Pain Reports
Authors Daniali H , Ruben MA, Aslaksen PM , Fiskum C, Kaptchuk TJ, Flaten MA
Received 17 November 2023
Accepted for publication 2 March 2024
Published 3 April 2024 Volume 2024:17 Pages 1345—1360
DOI https://doi.org/10.2147/JPR.S449150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Hojjat Daniali,1 Mollie A Ruben,2 Per M Aslaksen,3 Charlotte Fiskum,1 Ted J Kaptchuk,4 Magne A Flaten1
1Department of Psychology, Norwegian University of Science and Technology, Trondheim, Norway; 2Department of Psychology, University of Rhode Island, Kingston, RI, USA; 3Department of Psychology, UiT The Arctic University of Norway, Tromsø, Norway; 4Program in Placebo Studies, Beth Israel Deaconess Medical Center/ Harvard Medical School, Boston, MA, USA
Correspondence: Hojjat Daniali, Department of Psychology, Norwegian University of Science and Technology, Trondheim, NO-7491, Norway, Email [email protected]
Introduction: Studies suggest facial expressions of caregivers may be important in placebo effects; however, this has not been systematically tested. This experiment investigated the effects of caregivers’ singular positive nonverbal behaviours (NBs) on pain reports.
Methods: Fifty-one males and 53 females (total of 104) participants were randomized to four groups that were displayed positive facial expressions, tone of voice, body movement, or neutral NBs of videotaped experimenters. Subjective reports of pain, stress, arousal, and cardiac activity were obtained in a pre-test, a conditioning phase, and at a post-test. Four minutes of heat pain was induced in each test, and a placebo cream was administered before the conditioning and post-test in all groups.
Results: There were no differences between the NB groups in the reduced pain. Males had larger reduction in pain in the post-test, and females had lower arousal than the opposite sex. During the conditioning, females had larger reduction in pain ie, unconditioned pain response (UPR). In females, the UPR predicted the reinforced expectation ie, increase in expectations from conditioning to post-test, and fear of minor pain negatively predicted both the UPR and reinforced expectation.
Discussion: Singular NBs of caregiver were weak to enhance placebo effects. Females had lower pain during conditioning, and the UPR amplitude in females was associated with positive expectations. Moreover, for females, fear of minor pain weakened the UPR and expectations of cream.
Conclusion: No NB of caregivers is more effective in reducing pain. Caregivers’ NBs are less effective when displayed individually. Males and females may be different in underlying mechanisms of placebo effects.
Keywords: placebo effects, subtle factors, nonverbal behaviours, heat pain, experimenter effects, pain report
Introduction
The present experiment investigated the effects of singular positive nonverbal behaviours (NBs) on subjective pain, stress, arousal, and heart rate variability.
The context in which medical or psychological treatment is administrated can increase or decrease the effect of that treatment,1–4 and caregivers are an important component of that context.1,5 Caregiver features such as sex or gender,6 expectations,7 and nonverbal behaviours8 can have profound impacts on treatment outcome.
A review by Daniali and Flaten9 showed that caregivers’ positive NBs (eg, smiling, enhanced eye contact, positive tone of voice) led to lower pain reports, and conversely, negative NBs (eg, lack of smiling, minimal eye contact, flat tone of voice, etc.) led to higher pain report. Ruben et al10 showed that the high nonverbal support of videotaped caregivers led participants to increased pain tolerance.
NBs are expressed through micro- and macro-behaviours, in positive and negative valences.11 Micro-NBs such as facial expressions (eye contact, smiling, etc.), tone of voice (calm, friendly, etc.), body and limb movement and gestures (eg, hand and finger movements, etc.),12 generate impression of macro-NBs of for example warmth or being friendly.13
Previous studies have shown that caregivers' expectations about treatment,7,14 and their emotions15,16 can transmit to the care seeker, mostly through caregivers’ facial expressions.17 For instance, Czerniak et al18 showed that altering the doctors’ style, from a typical to a positive style both verbally and nonverbally, made the patients withstand a cold pain stimulation longer and report less pain. Chen et al17 investigated how caregivers’ expectations transmitted to the participants, and told the experimenters that they would apply a active or an inert cream to patients’ hands, followed by a thermal pain stimulation. However, both creams were inert. Before patients received the creams, doctors underwent a conditioning procedure that made them believe that one of the creams was active. Then, doctors administered the creams without talking about their expectations to patients. The results showed that patients had lower pain when caregivers delivered the cream they believed was active. Interestingly, cameras mounted on patients’ heads showed that doctors had different facial expressions while administering the placebo cream, suggesting doctors’ expectations were transmitted to participants through the facial expression of doctors. However, to date, no study has systematically compared the effects of different NBs of caregivers on modulation of pain reports.
In the present study, a videotaped experimenter guided participants through a pain experiment while expressing one positively enhanced NB and keeping other NBs neutral. The participants were thus exposed to either positive facial expressions (+FE), tone of voice (+TV), body movements (+BM), or neutral NBs control group (the NC). This allowed the investigation of the effects of singular NBs on pain and associated responses. We also investigated the effect of NBs on generation of expectations about the effects of treatment, and classical conditioning. Pain was induced in a pre-test, a conditioning phase where a placebo cream was applied before pain levels were surreptitiously lowered to induce expectations that the cream was a potent pain-reliever, and a post-test that was identical to the pre-test. Similar to Colloca et al19, “conditioning strength”, ie, the unconditioned pain response (UPR), was defined as the reduction in pain due to the reduced temperature in the conditioning phase.
The main aim of this study was to test the effect of NBs of the caregivers on pain and placebo effects, so no natural history group was included to act as a control for placebo effects. Rather, the control group in the present study controlled for the effects of the NBs by displaying only neutral NBs, and received the placebo treatment plus conditioning and information as the other three groups did. Therefore, a placebo effect could emerge in the control group as well as in the experimental groups.
Moreover, participants’ sex was manipulated, as males have been shown to have lower pain reports and larger placebo effects than females.20–23 Fear of pain24 was also investigated, as that has been shown to increase pain levels and decrease the inhibitory effect of contextual factors on pain.25 Heart rate and heart rate variability (HRV) were used as an index of physiological stress,26,27 as sympathetic and parasympathetic activations of autonomic nervous system modulate the descending pain inhibitory pathways.27–31
The following hypotheses were tested: 1) Positive NBs would cause a larger reduction in pain compared to the control group with neutral NBs. 2) Positive NBs would cause a larger positive expectations of treatment effects compared to the control group. 3) There would be a larger conditioning strength for the positive NB groups compared to the control group. 4) Males would have lower pain and stress reports than females. 5) The group with the lowest subjective and physiological stress would display the lowest pain. 6) The group with the largest reduction in pain would have higher rating of care and empathy than the other groups; and 7) fear of pain should predict pain and stress.
The study was approved by the Regional committee for medical and healthcare research ethics of Norway (REK; project number: 71,525) and the Norwegian centre for research data (NSD; project number: 167,011). Written informed consent was obtained from all participants, and the study complied with the declaration of Helsinki.
Methods
The experimental protocol including the development, standardization, validation of the NB conditions, and data for proof of concept is published elsewhere32. However, a resume of the information is also described here.
Participants
Recruitment was performed through distributing flyers and posters at the university’s (NTNU) campuses. Volunteers with a history of severe psychiatric disorder, chronic pain (ie, any pain that exists more than three months despite receiving treatment) eczema, injuries or scars on the lower right arm, pregnancy, and/or usage of prescription drugs (except birth control pills) were excluded. Participants were requested not to drink alcohol 24 hours prior to the experiment and abstain from large meals, nicotine and caffeine and energy drinks three hours prior to the experiment. A hundred and four healthy adult participants took part in the study. However, six participants were excluded due to low pain intensity (≤2) reports in the pre-test, and four more were excluded due to reporting expected efficacy of >0 of the placebo cream in the post-test before applying the placebo cream. Therefore, 94 participants (Mean age = 24.38; SD = 3.87) including 45 males (Mean age = 24.08; SD = 3.32) and 49 females (Mean age = 24.66; SD = 4.34) were included for the analyses of subjective data. Of 94 participants, the cardiac data from 86 participants (42 males and 44 females) were analyzed, as data from seven participants were deleted due to erroneous recordings.
Randomization
Using a pseudo-random number generator, 120 random numbers were pulled out and randomly assigned to four groups, resulting each group to have 30 numbers. The groups were sex-balanced, therefore, each group was split into two within-groups of 15 males and 15 females. The numbers assigned to males and females were separated and pooled together with an assistant who was not involved in later phases of the random assignment. For each participant who met the criteria a number was randomly picked from the pool that corresponded with their sex, which revealed the grouping of the participant.
Videotaped Experimenter Nonverbal Behaviour
The videoclip consisted of five main phases: introduction, calibration, pre-test, conditioning, and post-test. The videos for introduction, calibration, and the pre-test were recorded with a videotaped experimenter who expressed neutral NBs throughout the phases. For the conditioning, four different NB conditions (the +FE, +TV, +BM, and the NC) were developed which in three of them only one NB was positively enhanced while other NBs were kept as neutral as possible, and in the fourth condition (the neutral control; NC) all NBs were kept as neutral as possible. We defined positive NBs as NBs that conveyed a positive feeling to the observer. Neutral NBs were defined as NBs that did not convey a specific emotion to the observer and were significantly less positive than the positively enhanced NBs. In the +FE group, the videotaped experimenter expressed frequent smiling and nodding, enhanced eye contact (longer than a total of five minutes throughout the phase), more expressive eyebrows, lips, and cheek muscle movements. In the +TV, the videotaped experimenter spoke with a calm, friendly, expressive, positive tone of voice. In the +BM, the videotaped experimenter leaned toward the camera more frequently (to imply closer proximity to the participant) and had elaborate and expressive hand movements that facilitated the verbal speech such as indexing, counting with fingers, indicating sizes, timelines, and forms with hands. In each of these videos, only the intended NB was enhanced, and the other NBs were kept neutral, eg, the videotaped experimenter in the +FE group had elaborated facial expressions while she kept a flat tone of voice, held a standard distance (about a meter to the camera) without leaning forward, and had a straight body posture without gesturing. In the NC, all NBs were kept neutral, therefore, the videotaped experimenter showed a neutral facial expression without smiling nor did she display enhanced eye contact, used a monotonous tone of voice, and displayed a straight body posture without moving the hands frequently. The NBs of the videotaped experimenters in the introduction, calibration, and the pre-test were neutral in all nonverbal channels.
Videotaped Experimenters
Three female professional actors played the role and two of them were chosen to act as the videotaped experimenters. The actors were typecast to fit a usual health personnel stereotype,32 wearing a white lab coat and light makeup. All NB conditions were played by both actors. Before recording, each actor received about 10 hours of training and instructions to perform the positively enhanced NBs and the control condition. Videotaped experimenters like these have been used in previous studies.10,33
Proof of Concept
To ensure about validity and reliability of the video NB-videos, a preparatory study was carried out in which a group of psychology students from Norway and USA received training on nonverbal coding from the first and the second authors (HD and MAR) and then rated the degree of NBs of smiling, eye contact, gestures, positivity in tone of voice, and impressions of dominance, overall positivity, and expressivity from each NB. The manipulated NBs were shown to have construct validity and reliability. Moreover, both the +BM and the +FE groups were rated as more dominant than the +TV and the NC groups. The +FE and +BM groups were rated as the most positive and expressive, respectively.32 The actors were rated differently on the level of physical attractiveness, therefore, to control for attractiveness (halo) effects, both the actors with the higher and the lower rates of attractiveness were displayed to each group and participants were randomly assigned to one of the actors.32 Thus, collapsing across different levels of attractiveness within each group should ensure a halo effect was not driving the results.
Research Assistants
Four female assistants in the age range of 25–30 carried out the experiment. They followed a script for their interactions with the participants and received training on how to keep their nonverbal interactions at a minimum.
Manipulation of Assistants’ Beliefs
Gracely et al7 showed that the expectations of caregivers could be transmitted through subtle behaviours. Thus, to control for the assistants’ expectations, two types of information, certain and uncertain information about the cream were given to assistants. For 54 participants, the assistants were told that for half of the participants a cream containing a pain-reliever will be used and for the other half a placebo cream. They were told that they would not know which cream is the active cream and which is the placebo cream. These assistants are hereafter termed Uncertain Information (UI) assistants. For the other 50 participants, the assistants were told that from now on, all the participants will receive a cream containing a pain-reliever. These assistants are hereafter termed Certain Information (CI) assistants. Each group was tested by both the CI and UI assistants, thus, collapsing across both types of assistants’ information within each group should ensure that the assistants’ information about the placebo cream did not affect the results.
Conditioning of the Assistants
To reinforce a positive expectation and the belief about the effectiveness of the cream for the CI assistants, an active pain-relieving cream (lidocaine 5%) with an identical appearance and smell to the placebo cream was tested on them. To do so, the CI assistants underwent a conditioning with two ascending thermal stimulations to their forearm, starting from 32°C, with an increase rate of 0.25°C/second, until the assistant reported pain intensity of “5” on a numeric rating scale (NRS). Before the second stimulation, a cream containing 5% lidocaine was administered to another area of the forearm and a 15-minute break was given for the cream to take effect. Thereafter, the thermal stimulation identical to the first stimulation was administrated until the assistant reported pain intensity of “5”. Afterwards, the results from both stimulations were shown to the assistants, and it was discussed that after the administration of the pain-relieving cream, they reported the pain intensity of “5” at a higher temperature stimulation than when they received the stimulation without the cream, suggesting that they could stand a higher stimulation following the application of the cream.
Pain Induction System
Thermal pain stimulation was induced by a 30×30 mm thermode (metal plate) controlled by a Pathway ATS (Medoc) (TSA II, Medoc, Ramat Yishai, Israel).
Heart Rate and Heart Rate Variability (HRV)
Cardiac activity was measured using the BIOPAC MP150 system using the ECG100C module and Acqknowledge Software version 5 (Biopac Systems Inc., Goleta, CA). All signals were sampled at 1000 Hz, with a 50 Hz notch filter applied. ECG data were collected using three disposable Ag-AgCl electrodes placed on the clavicles and the fourth lower left rib. The ECG-data was inspected visually for artifacts, and analyses were performed offline using Kubios HRV version 3.5.34,35 Artifacts were corrected by the Kubios automatic correction algorithm,36 along with a thorough manual inspection of the signal and corrections. All samples were inspected and analyzed individually. The following measures were extracted from the data; the root mean square of successive differences (RMSSD), the normalized power of high (HF, 0.15–0.40 Hz) and low frequency (LF, 0.04–0.15 Hz) components in the signal using fast Fourier transform, LF/HF ratio and heart rate (beats per minute). ECG-data were recorded throughout the stimulation phases (pre-test, conditioning, and the post-test) and for three minutes after the conclusion of the experiment, as the baseline.
Questionnaires
Pain intensity and pain unpleasantness were rated on a NRS as described in Price et al.37 For pain intensity, “0” was anchored to “no pain at all”, “5” to “moderately painful”, and “10” was anchored to “worst pain possible”. For pain unpleasantness “0” was anchored to “no unpleasantness at all”, “5” anchored to “moderately unpleasant”, and “10” was anchored to “worst unpleasantness possible”.
Stress and arousal were assessed before and after the stimulations, by the Short Adjective Check List (SACL):38 two adjective pairs each that were rated on a scale from “0” to “10”. Stress was measured by asking participants to rate how “relaxed” or “tense”, or how “calm” or “nervous” they were, on a scale from “0” to “10”. Arousal was assessed the same way on the scales of “sleepy” or “awake”, and “tired” or “energetic”. SACL has been used in several studies on the role of stress and arousal in pain.21,39,40
CARE. Three items (item “1”, “6” and item “8”) from the 10-item Consultation and Relational Empathy (CARE)41 were selected to assess the satisfaction with the videotaped experimenters. The sum of the items was used for the analyses.
Expected efficacy. After receiving the placebo cream and before the pain stimulation in the conditioning and post-test phase, the participants were asked to rate how much they thought the cream would reduce their pain intensity on the same 11-point NRS.
Prior experience with the cream. Participants were asked if they had any former experience with thermal pain-relieving creams. If the answer was yes, they were then asked to rate the efficacy of the cream they used on the same NRS as pain intensity ratings.26 No participant reported any prior experience with thermal pain-relieving creams, so this item was not used, and all participants were retained in analyses.
The Fear of Pain Questionnaire III (FPQ III)24 was used to assess fear of pain. The FPQ III is a 30-item questionnaire that assesses fear of pain in situations in which pain is minor, severe, or induced by medical procedures. The rating scale for items is a 5-point Likert ranging from “1” anchored to “not at all”, to “5” anchored to “extreme”. The total score can range from “30” to “150”. FPQ III provides three subscales of severe, minor, and medical fear of pain and a total score of fear of pain. The psychometric properties of FPQ III in Norwegian samples have been reported acceptable.42
Personality43 was also assessed, however these data are not analyzed in the current paper.
The Procedure
The purpose of the study was introduced as to investigate the psychological and physiological reactions to a thermal pain stimulation and an over-The-counter pain-relieving cream for heat pain. The experiment was conducted by two videotaped experimenters, and an actual assistant carrying out the experiment with minimal interaction with participants. In the beginning, and after the participant was sitting and ECG electrodes were attached, the first videotaped experimenter introduced the experiment and guided participants to fill out the questionnaires, then the participant underwent the calibration phase in which three ascending pain stimulations were administered. The painful stimuli were individually calibrated to a pain level of “5” to allow the observation of both reduction and elevation of pain levels. The stimuli started at 32°C, with an increase rate of 0.25°C/second until the participant reported pain equal to “5” on the NRS. The built-in upper limit for the thermode temperature was at 51°C. Three ascending stimuli were administered, each time on a different area of the forearm. For each stimulation, as the stimulation temperature went up, the participant reported the increase in the intensity of pain from “1” to “5”. Pain equal to “5” was determined as the average of those three stimuli administered in the calibration phase, which were administered at the pre- and post-test. After a short break, the participant underwent the pre-test, the videotaped experimenter guided the participant to undergo a 4-minute thermal stimulation using the individually calibrated intensity of level “5” for the participant. After 30 seconds, two, and four minutes of pain stimulation, the videotaped experimenter asked the participant to report pain intensity and unpleasantness on an 11-point NRS from no pain at all, anchored to “0”, to the worst pain possible, anchored to “10”. Before and after the stimulation, the videotaped experimenter asked the participant to report their stress and arousal. After the pre-test, the participant was given a four-minutes break. The NBs of the videotaped experimenters in the introduction, calibration, and the pre-test were neutral in all channels. After the pre-test, the experimental manipulation began.
Prior to the conditioning phase, the second videotaped experimenter was displayed and introduced the placebo cream. The verbal information about the cream was as follows:
before the next pain stimulation, you will receive a pain-relieving cream. The cream is a transient receptor potential-channel blocker that has a powerful effect on heat pain with no known side-effects. In a couple of seconds, the assistant will administer the cream on your hand, gives it 10 minutes to work, and then induces the stimulation. Then, you will report how much pain intensity and unpleasantness you feel.
The second videotaped experimenter expressed the positively enhanced NBs that corresponded to the group the participant was assigned to. Then, the assistant applied the cream and mounted the thermode on the forearm. The second videotaped experimenter informed the participant that the cream would be given 10 minutes to work. Unbeknownst to the participant, the temperature from the intensity of “5” was lowered to the temperature equal to intensity of “3”, to associate the administration of the cream with lower pain intensities. The pain level “3” was induced for four minutes. After 30 seconds (1st Timepoint), two (2nd Timepoint), and four minutes (3rd Timepoint) of the pain stimulation, the participant was asked to report pain intensity and unpleasantness. The post-test was identical to the conditioning, except that a temperature equal to intensity level of “5” was administered. Thus, the second videotaped experimenter informed the participant that the last pain stimulation would be repeated once again (see Figure 1).
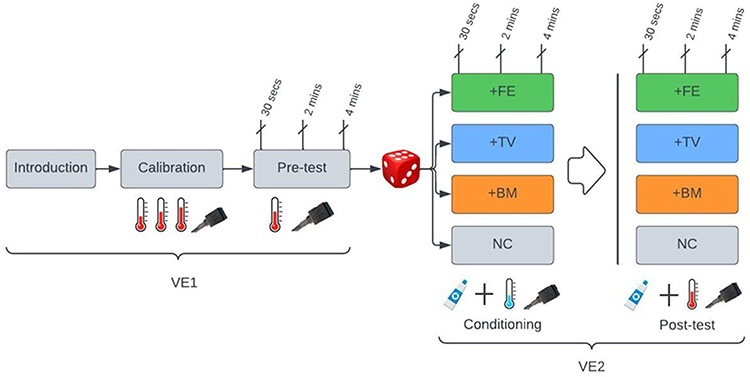 |
Figure 1 Experimental procedure.Grey boxes: phases with neutral NBs; During the calibration, the intensity (illustrated by a thermometer) of thermal pain (illustrated by a thermode) was calibrated to the individual average of pain intensity of “5” with three ascending stimulations. During the pre-test, the calibrated painful stimulation was induced. Next, participants were randomly assigned (illustrated by a dice) to one of the four groups. During the conditioning, a placebo cream was applied with suggestive information by the VE2, and a lower pain stimulation than the pre-test, unbeknown to participant, was induced. The suggestive information was accompanied with positively enhanced NBs in +FE, +TV, and +BM groups, and with neutral NBs in NC group. During the post-test, an identical procedure as the conditioning was administered, with the only difference that same stimulation intensity as in the pre-test was administered. At pre-test, conditioning and the post-test, the pain intensity and unpleasantness were recorded at 30 seconds (1st Timepoint), two (2nd Timepoint), and four minutes (3rd Timepoint) of the stimulation; and the stress and arousal were recorded before and after the stimulations. Cardiac activity was recorded throughout the pre-test, the conditioning, and the post-test. Abbreviation: +FE: positive facial expressions; +TV: positive tone of voice; +BM: positive body movements; NC: neutral control; VE1: the first videotaped experimenter who shows only neutral NBs; VE2: the second VE who had either positive or neutral NBs (colored grey) |
Statistical Power
The study was exploratory in nature, so the effect size for the experimenters’ singular NBs on pain reports was not clear from previous studies. However, Ruben et al10 reported eta square (η2) of 0.08 for the effects of videotaped caregivers’ high social support (both positive verbal suggestions and nonverbal behaviours) on pain tolerance in a study with two groups (high social support pain tolerance [in seconds] Mean = 450.68, SD = 278.08; low social support pain tolerance [in seconds] Mean = 313.22, SD = 198.09). Therefore, converting the η2p of 0.08 to Cohen f to make it comparable for multiple groups such as present study, an effect size of 0.295 was obtained.44 For the present study, assuming a statistical power of 0.80, alpha of 0.05 and an expected effect size of 0.29, for an ANOVA main and interaction effects with two fixed factors of Group (4 levels) and Sex (2 levels), and two within-subject factors of Test (2 levels) and Time (3 levels) a total sample size of 112 was required. However, considering limitations in time and resources and the exploratory nature of study, a total of 104 participants were recruited.
Sample Selection
As the expectations were considered to be the main mechanism for the potential reduction in pain, only participants who had an expected efficacy of >0 in the post-test were included. This criterion excluded four participants from the final sample.
Design and Statistics
To simplify the design and the figures for subjective data, the change scores (ie, pre-test minus post-test) for each Timepoint for pain, stress and arousal data (pain reports at 1st Timepoint measurements at 30 seconds, 2nd measurement at 2 minutes, and 3rd measurement at 4 minutes of the stimulation; and stress and arousal reports before and after the stimulation) were included as the dependent variable to investigate the reduction in pain and stress in the post-test. The change score in the conditioning phase ie, unconditioned pain response (UPR), was calculated as the pre-test minus the conditioning phase.
A repeated measures ANOVA design with Group (4 levels; +FE, +TV, +BM, and NC) and Sex (2 levels; male, female) as between-subjects factors, and Timepoints (pain reports with three timepoint measurements: at 30 seconds, 2 minutes, and 4 minutes of the stimulation; and stress and arousal reports with two timepoint measurements: before and after the stimulation) as within-subject factor was used to analyze the pain, stress, and arousal data.
For expected efficacy, a single ANOVA with Groups (4 levels) and Sex (2 levels) as the fixed factors, and the change score of expected efficacy (expected efficacy at conditioning minus expected efficacy at post-test) as the dependent variable was tested.
To test differences between groups in rating of caregivers’ empathy and warmth, the sum of the three items of Care (item “1”, “6” and item “8”) was entered as the dependent variable into a single ANOVA with the Group (4 levels) and Sex (2 levels) as factors.
To analyze the HRV data, the cardiac measurements from pre-test and post-test (Test; 2 levels) were entered into a linear mixed models analysis with an auto-regressive covariance structure, conducted separately for RMSSD, HR, LF, HF, and LF/HF ratio, with Group (4 levels), Sex (2 levels), and Test (2 levels, pre-test and post-test) as the factors.
The equality of the variance between groups (Mauchly Ws ps ≥ 0.14; Box’s M test ps ≥ 0.06), and equality of error variance (Levene statistic ps ≥ 0.16) for pain data were met, suggesting the sphericity and equality of variances. The visual inspection of data suggested normality of the distribution of the overall pain report across timepoints, even though ANOVAs are known to be robust against violations of normality assumptions.45,46 The follow-up tests for both subjective and physiological data were all conducted using Bonferroni post-hoc tests. For all the main and interaction effects and interactions that included a within-subjects factor, the Greenhouse–Geisser correction was used to correct for inflated degrees of freedom, which are also known to be robust against violations of sphericity.47
Separate linear regression analyses were used to test if change scores of stress, arousal, unconditioned pain response (UPR), heart rate and RMSSD predicted the pain change score. The dependent variables of all significant predictions were normally distributed through visual inspection, and other assumptions (linearity, homogeneity of variances and no multicollinearity) to conduct regression analyses were met.
Results
A total of 94 participants were included in the subjective data (pain, stress, and arousal) (Table 1). Of 94 participants, 45 were males and 49 were females (see Table 2), and the cardiac data of 86 participants (42 males and 44 females) were analyzed (23 in the +FE, 20 in the +TV, 24 in the +BM and 19 participants in the NC).
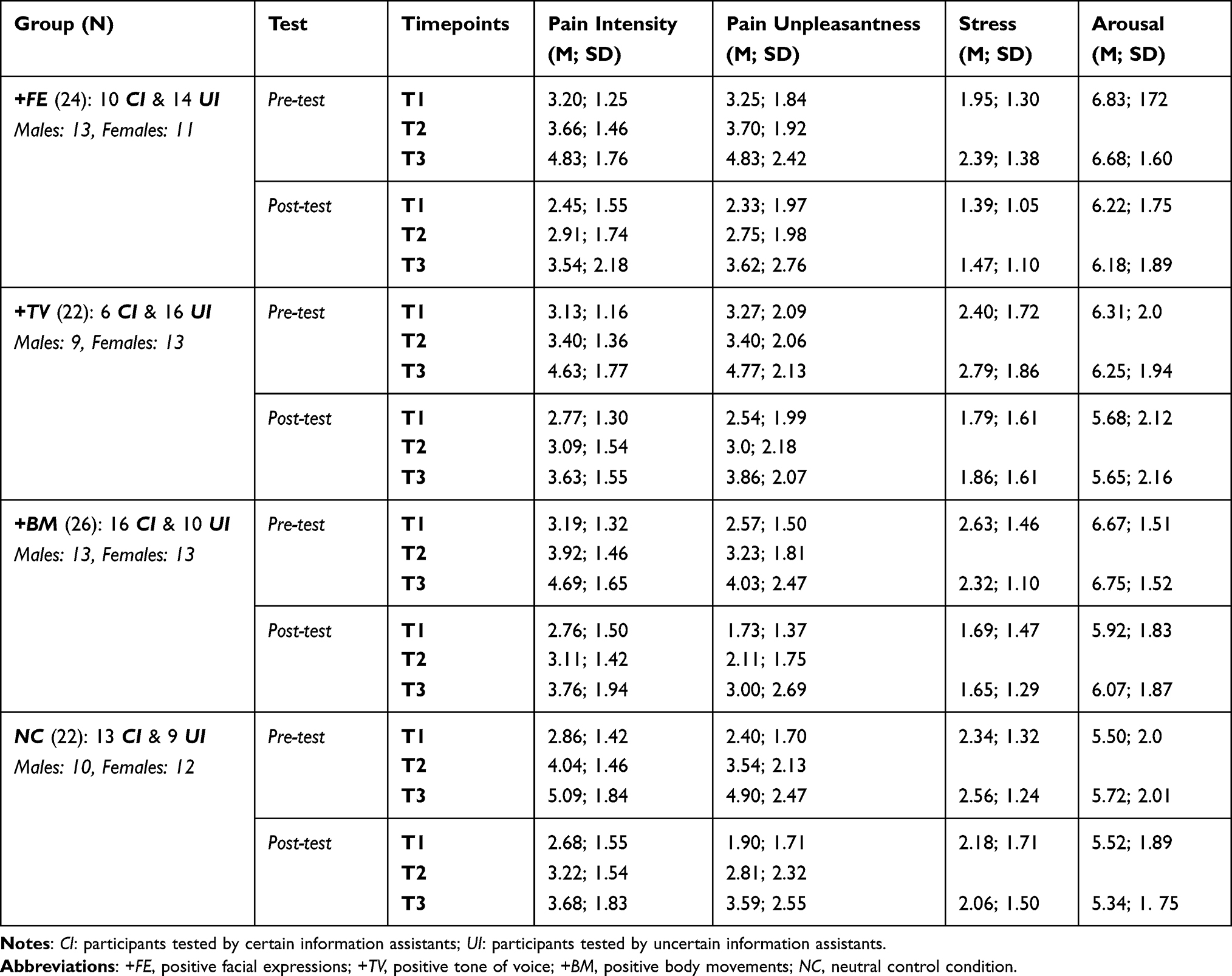 |
Table 1 Mean (M) and Standard Deviation (SD) of Pain Intensity, Pain Unpleasantness, Stress and Arousal for All Groups, Test (Pre and Post), and Timepoints |
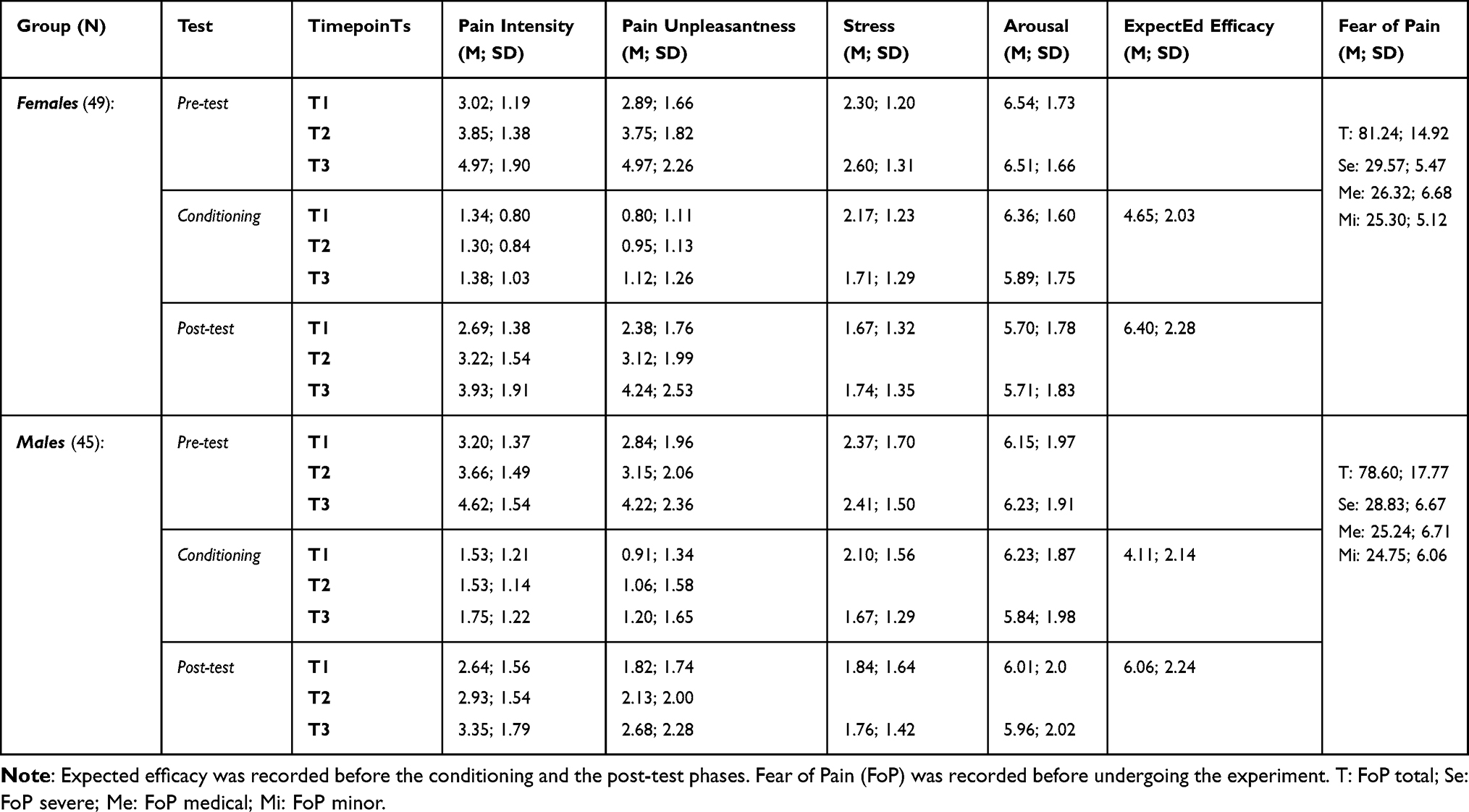 |
Table 2 Mean (M) and Standard Deviation (SD) of Pain Intensity, Pain Unpleasantness, Stress, Arousal, Expected Efficacy and Fear of Pain for Females and Males |
Pain Intensity
Pain intensity data mirrored pain unpleasantness data (rs ≥ 0.70; see Table 1 for raw pain scores), so only pain unpleasantness data is reported.
Pain Unpleasantness
The ANOVA showed a main effect of Sex (F(1, 86) = 5.35, p = 0.02) which was due to males having larger reduction in pain unpleasantness than females from pre-test to post-test (Mean diff = 0.59, SE = 0.25, p = 0.02). No significant differences in reduced pain were observed between the NB groups. No other main or interaction effect was significant.
Conditioning Strength
The main effect of Timepoint (F(1.47, 127.20) = 33.34, p = 0.001) showed that the UPR was stronger at the 3rd Timepoint than the 1st and the 2nd Timepoints (Mean diffs ≥ 0.45, SE ≥ 0.15, p = 0.01). The interaction of Group by Sex (F(3, 86) = 3.36, p = 0.02) showed that in the +BM and the NC groups females had larger UPR than males (+BM Mean diff = 1.53, SE = 0.61, p = 0.01; NC Mean diff = 1.48, SE = 0.66, p = 0.03; Figure 2). No other main or interaction effect was significant.
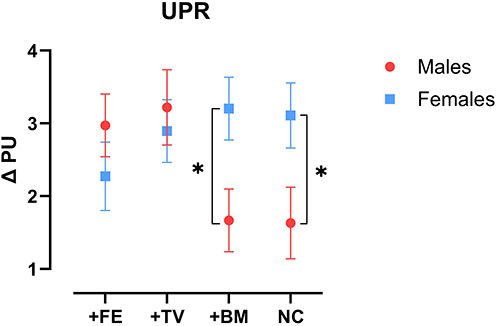 |
Figure 2 Change in unconditioned pain response in each group and sex. Abbreviation: UPR, unconditioned pain response; +FE, positive facial expressions; +TV, positive tone of voice; +BM, positive body movements; NC, neutral condition. Note. ∆ PU: change in pain unpleasantness from pre-test to conditioning, with higher scores meaning higher conditioning strength. Females in the +BM and NC groups had larger UPR than males. *p ≤ 0.05. Error bars: ± 2 SE. |
Subjective Stress
Stress levels were low and below three on the 11-point scale during the experiment proper. No main or interaction effect was significant for subjective stress.
Subjective Arousal
Arousal levels were high in the calibration (M = 6.51, SE = 0.30) and pre-test (M = 6.31, SE = 0.17) and were slightly, but significantly reduced in the post-test (M = 5.83 (SE = 0.19) (F(1.0, 86.0) = 19.79, p = 0.001). The main effect of Sex (F(1, 86) = 7.50, p = 0.007) was due to females having larger reduction in arousal from pre-test to post-test, than males (Mean diff = 0.60, SE = 0.21, p = 0.007). There was an interaction of Group by Sex (F(3, 86) = 4.73, p = 0.004) which was due to females in the +TV and the +BM groups having larger reduction in arousal than males in the same groups (Mean diffs ≥ 1.17, SE ≥ 0.45, p = 0.01) (Figure 3).
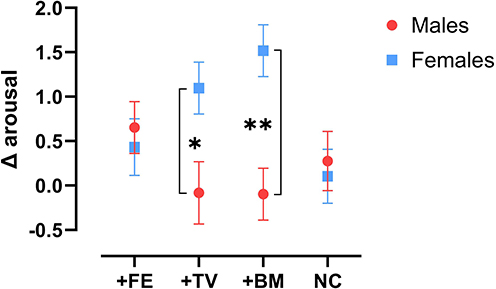 |
Figure 3 Arousal change scores (delta) across Group and Sex. Abbreviation: +FE, positive facial expressions; +TV, positive tone of voice; +BM, positive body movements; NC, neutral condition. Note. ∆ arousal: change in arousal from pre-test to post-test, with higher scores meaning lower arousal in the post-test. Females in the +TV and the +BM groups had larger reduction in arousal than males in the post-test. *p ≤ 0.05. **p ≤ 0.01. Error bars: ± 2 SE. |
Expected Cream Efficacy
The expected efficacy increased from the conditioning (M = 4.04, SE = 1.98) to the post-test (M = 6.91, SE = 1.98) (F(1.0, 86.0) = 58.05, p = 0.001). No other main or interaction effect was significant in the reinforced expectations about the cream.
The UPR was associated with the change in expected efficacy of the cream only in females (F(1,47) = 9.86, B = 0.54, β = 0.41, t = 3.14, p = 0.003), and not in males (F(1,43) = 1.54, B = 0.28, β = 0.18, t = 1.24, p = 0.22).
The level of expected efficacy before the conditioning was not associated with the UPR (F(1,92) = 0.31, B =0.04, β =0.05, t = 0.55, p = 0.57).
Care and Empathy
The main effect of Group (F(3, 83) = 3.29, p = 0.029) showed that the +FE group was perceived as more empathic and caring than the NC group (Mean diff = 2.28, SE = 0.80, p = 0.03). No other main or interaction effect was significant (Figure 4).
 |
Figure 4 Perceived care and empathy in each Group. Abbreviation: +FE, positive facial expressions; +TV, positive tone of voice; +BM, positive body movements; NC, neutral condition. Note: The +FE was perceived as more caring and empathic than the NC. The dependent variable is the sum of the three items of Care and empathy scale. Max score (sum of three items): 15; Min score (sum of three items): 2. *p ≤ 0.05. Error bars: ± 2 SE. |
The perceived care and empathy was not associated with the pain reports neither in the post-test nor the in the conditioning.
Fear of Pain
There were no differences between males and females in fear of pain, neither in the total score nor in the subscales (ps ≥ 0.48). Fear of minor pain was negatively associated with the UPR, only in females (F(1,47) = 7.11, B = −0.11, β = −0.36, t = −2.66, p = 0.01), and not in males (F(1,43) = 0.68, B = −0.03, β = −0.12, t = −0.82, p = 0.41). Fear of minor pain was also negatively associated with the reinforced expected efficacy, only in females (F(1,47) = 4.89, B = −0.12, β = −0.30, t = −2.21, p = 0.03), and not in males (F(1,43) = 0.05, B = −0.01, β = −0.03, t = −0.22, p = 0.82).
HR and HRV
HR: the main effect of Test (F(1, 78.01) = 35.89, p ˂ 0.001) showed that HR was reduced from pre-test to post-test (Mean diff = −2.0, SE =0.34, p ˂ 0.001). No other main or interaction effects were significant in any other HRV indexes.
Discussion
The main findings are that there were no differences in the reduced pain between NB groups. Males had larger reduction in pain unpleasantness than females from the pre-test to post-test, and females had larger reduction in arousal, and larger unconditioned pain response (UPR) compared to males in the +BM and the NC groups. For females, the UPR was associated with the reinforced expectation about the effectiveness of the cream, and fear of minor pain was negatively associated with both the UPR and the reinforced expectation, but not for males. The videotaped experimenters with positive facial expressions were rated higher in care and empathy compared to the VE with neutral NBs.
Pain and stress were reduced from pre-test to post-test in all groups; however, the reduction in pain cannot be excluded to placebo effects, as this study did not have a natural history control group with no treatment, and the control group in this study just controlled for the NBs of the caregiver. Thus, the reduced pain and stress could have been due to other factors such as habituation, as evidenced by pain reports lower than “5” in pre-test,39 and a placebo effect may have emerged in control group as well.
The reduction in pain from pre-test to post-test was not different between the positive NB groups and the NC group, and this disconfirms hypotheses for the effects of singular NBs (hypotheses 1–3). Probably due to weak effects of singular NBs, because the NBs were disassembled to individual NBs. Ruben et al10 showed that when the videotaped caregiver had a warm communication style with positive NBs such as extended eye contact, leaning forwards, elaborative hand movements and a positive tone of voice, there were no effects on pain intensity reports, but participants had higher pain tolerance. However, it was not clear what NB had the most effects, as the NBs were displayed simultaneously. When the singular NBs of the videotaped experimenters were tested in this study, the results did not suggest a difference between the NBs in their effect on pain intensity and unpleasantness reports, which can be due to weaker effects of separated singular NBs. Even separating NBs from positive verbal suggestions have shown to produce similar results. For instance, He et al48 tested the effects of a warm communication style (including positive NBs) separated from suggestive information about a sham training program to improve physical balance, and showed that warm communication style apart from positive information did not improve physical balance. In contrast, suggestive information about treatment without the positive nonverbal cues of the caregivers have also been shown to be ineffective. Our dental experiment (Daniali, Hunsbeth, and Flaten; under review)49 showed that when the suggestive information about a dental treatment was given to patients without the subtle cues of dentists administering the treatment, the positive information did not reduce the procedural dental pain. Therefore, a more plausible explanation is that the singular NBs of videotaped experimenters were not different in their effect in reducing pain, and conclusively, there is no NB of caregivers that have a superior effect in reducing pain than other NBs, and that the caregivers NBs are most influential when they are presented collectively and altogether, and not separately.
Another explanation is that the positivity in NBs probably had small effects in reducing pain, as the pain was not reduced more in the +FE compared to the NC, even though the +FE was rated as more caring and empathic than the NC, in alignment with what has been observed in the preparatory study;32 moreover, the difference between all positively enhanced groups and the NC group with neutral NBs was insignificant. The lower effects of positive NBs compared to other forms of NBs have been pointed out in former studies as well. Valentini et al15 for example showed a series of facial expressions of neutral, grimacing (facial pain expressions), and smiling of strangers during a classical placebo conditioning of a painful laser stimulation, meaning that facial cues were paired with sham treatment with a lowered pain. The results showed that seeing facial expressions with emotional content, especially concomitant to the painful stimulation, enhanced the placebo analgesic effect. Similar results have been reported by others.17
Even though the NBs did not differ in their effect on pain and stress, the +FE was rated as more caring and empathic than the NC, suggesting that the positive facial expressions of the caregivers made them to be perceived as more caring and empathic than the videotaped experimenter with neutral NBs. This finding is in line with the preparatory study results which showed the +FE as the most positive NB group,50 and confirmed that the overall positivity in the +FE was transmitted to the participants. However, this finding rejected the hypothesis “6” as the +FE was not the NB group with significantly highest reduction in pain. Kraft-Todd et al16 showed that photos of caregivers with enhanced eye-contact were perceived as more empathic and warmer, thus positive NBs contribute to the perception of care and empathy. However, static photos were used in that study, whereas in this study videotaped experimenters tested actual participants. Even though the preparatory study32 showed that the +BM and the +TV were rated as significantly more positive than the NC group, the participants in the pain experiment did not perceive the +BM and the +TV as more caring than the NC, suggesting that the positivity/expressivity may not always translate to perception of care and empathy.
Males had larger reduction in pain unpleasantness than females from pre-test to post-test which partially confirmed hypothesis “4” that presumed males to have lower pain reports than females, and is in line with previous studies suggesting males show larger placebo effects than females.22 The lower report of pain and larger placebo effects in males have been suggested to be associated with reduced stress; however, no such association was observed in this experiment. Subjective stress levels were low in the present study, below three on an 11-point scale, and this floor effect might have masked any differences between males and females. Thus, it could be that the effects of positive information plus conditioning were more effective in males compared to females to reduce the pain from pre-test to post-test.
In the conditioning phase, pain was reduced more in females than males in the +BM and the NC, thus, females in these groups showed larger unconditioned pain response (UPR) than males. However, the lowered pain in females in the conditioning was not translated to the post-test, probably due to low reports of pain, which may have made the reduction in pain difficult to perceive. It has been shown previously that the placebo effect may be less likely to emerge in stimulations with low intensities.39,51 Moreover, in all NB groups females had relatively similar UPR amplitudes, but for males the UPR amplitude was high in two groups and low in two other groups. Therefore, the UPR response was more consistent in females than males. However, we cannot attribute the larger UPR in females of these groups to the effects of NBs, as females in both the +BM group and the NC group showed larger UPR than males, thus, no meaningful between-group differences could explain the larger UPR in females in these groups. Moreover, the regressions showed that the UPR was associated with the reinforced expectations in females, and with no difference between the groups. Therefore, the larger UPR in females than males is more likely to be related to a sex difference in response to the suggestive information and conditioning, with females showing larger reduction in pain during the conditioning compared to males. The larger UPR in female cannot be attributed to the conditioning solely, as positive information about the effectiveness of the cream was given to participants during the conditioning. Thus, it was the positive information plus conditioning that reduced pain more in females than males in the conditioning, as our data is inconclusive on whether the conditioning or the suggestive information that made the larger UPR in females. A previous systematic review from our group22 suggested conditioning procedures to be more effective to elicit nocebo effects in females. There were no studies that reported a sex difference in placebo effects due to the conditioning procedures. Based on the included studies, Vambheim and Flaten22 concluded that the sex difference in placebo analgesia may be due to the modulatory effects of stress, and/or psychophysiological underlying mechanisms. Enck and Klosterhalfen23 who updated the review by Vambheim and Flaten22, found two more studies with small samples that reported females to have larger placebo effects in nausea following a conditioning procedure, and concluded that the conditioning procedures can be more effective in females compared to males to elicit both nocebo and placebo effects. It is still not clear why conditioning procedure is more effective for females compared to males, and this is despite the attempts that have been made to understand the sex difference in response to the method of placebo generation.22,23
Females had larger reduction in arousal than males from pre-test to post-test, specifically in NB groups of +TV and +BM, which rejected part of hypothesis “4” that presumed males to have lower stress (and arousal). Arousal levels had a mean of 6.56 on an 11-point scale at the start of the study, thus arousal levels were high. However, it is unlikely that larger reduction of arousal in females was related to the NB manipulations, due to no indication of any between-group differences.
Expectations about the effectiveness of the cream increased from conditioning to post-test in both males and females. However, in females, the UPR was associated with the reinforced expectations, meaning that the larger reduction in pain during the conditioning was associated with increased expectations in the post-test in females. This finding suggests a tendency for females to show larger expectations about the efficacy of the placebo agent following a conditioning procedure, as the more the pain was reduced during the conditioning, a more positive expectation about the efficacy of the cream in the post-test was reported by females. However, the reinforced expectation was not associated with the reduced pain in the post-test for females. Therefore, the enhancement of positive expectations may not be necessarily related to the reduction in pain.
Fear of minor pain was negatively associated with the UPR in females, so higher fear of minor pain was associated with a smaller reduction in pain from the pre-test to the conditioning phase. Previous studies have shown that higher levels of fear of pain are associated with lower placebo effects,25,52 and this study shows that fear of minor pain in females weakened the UPR amplitude that in turn was associated with a weaker conditioned pain response. In females, fear of minor pain was also negatively associated with the reinforced expectations, suggesting that being more afraid of minor pain inhibited the generation of larger expectations about the effectiveness of the cream, suggesting that negative emotions may inhibit the generation of positive expectations about treatment. It has been previously suggested that negative emotions like anxiety modulate placebo effects.53 More specifically for females, Colloca et al54 showed that compared to males, intranasal inhalation of vasopressin enhanced the placebo analgesic response only in females, and the larger placebo analgesic effects in females were modulated by lower dispositional anxiety levels. Consistently, what our findings add is that the negative emotions may also weaken the UPR and generation of positive expectations in females. Lastly, the negative association between fear of pain and lower reduction in pain can have potential implications in clinical settings with pain patients with tendencies to exhibit maladaptive patterns of pain-related fear and pain catastrophizing, that may eventually reduce the treatment outcome.55
Limitations
This study has several limitations. First is the lack of a natural history control group with no placebo intervention. The cream with treatment-related information and the conditioning procedure were applied in the NC group as in the other three groups, to compare the differences between the positive and neutral NBs, as the lack of positive NBs would be the only difference between the control group and the experimental groups. However, this design did not distinguish a placebo effect from a reduction in pain. To distinguish the effect of conditioning and treatment-related information from the effect of the positive NBs of the experimenters, a control group with no placebo intervention would be needed. Therefore, we cannot conclude with certainty that the reduction in pain was a placebo effect. The use of videotaped experimenters provides a high level of control over the manipulated NBs,56 but it can reduce the ecological validity of the study. That of course depends on the area of usage of such experimenters, and videotaped health personnel are already in use in hospitals. Another threat to the ecological validity was the isolation of singular NBs. Nonverbal messages are normally transmitted through multiple NBs and not through a singular NB.57 Moreover, despite the sample being smaller than what was suggested by the power analysis, we believe the results may still hold validity. This is evidenced by the absence of differences in pain reports between the aggregated positive nonverbal behaviour groups (combining +FE, +BM, and +TV) and the neutral control group, suggesting that the nonverbal behaviours may have had a weak effect on pain reports. However, these possible limitations are subject to empirical testing, and a previous study on the impressions imparted by the singular NBs found that the singular NBs induced impressions of expressivity, dominance, and positivity more than absence of NBs.50 Lastly, the use of a binary category to identify sex was a limitation, as the identification of sex was not accompanied by more detailed information about sex of participants, for example, the phase of their menstrual cycle eg.58 Moreover, the results of this study cannot entirely be attributed to the biological sex of the participants, as contextual and other confounding factors might have also modulated the way males and females responded to the manipulations.59 However, the results regarding male and female differences in response to the placebo manipulations were in line with former studies, therefore, likely that the results were more related to the sex of participants and not the interplay of the sex of participants with other factors.
Conclusion
The results from this study suggested that the singular NBs of videotaped experimenters were not different in their effect on pain reports, however, positive facial expressions resulted in the caregiver being perceived as more caring and empathic. Females tend to have larger reduction in pain during conditionings with verbal suggestions, and higher pain-related negative emotions like fear of minor pain weaken the conditioned pain response and the generation of positive expectations in females.
Data Sharing Statement
Data can be made available upon request from the corresponding author (HD).
Acknowledgments
The authors would like to thank the research assistants and actors Rosanna Matthäus, Nora Sofie Trohaug, Shunmathi Vijayaraj, Sonja Maria Mellberg, Ane Eikemo, Ingrid Endal, and Synne Ørsleie for their contribution in this study. The study protocol was previously posted as a pre-print at Researchsquare.com and published.50
Funding
The Norwegian University of Science and Technology (NTNU), and the Bial foundation (Grant number: 36/20) funded this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kelley JM, Kraft-Todd G, Schapira L, Kossowsky J, Riess H. The influence of the patient-clinician relationship on healthcare outcomes: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2014;9(4):e94207. doi:10.1371/journal.pone.0094207
2. Kirsch I. Specifying nonspecifics: psychological mechanisms of placebo effects. Placebo Effect. 1997;1:166–186.
3. Levine J, Gordon N, Fields H. The mechanism of placebo analgesia. Lancet. 1978;312(8091):654–657. doi:10.1016/S0140-6736(78)92762-9
4. Miller FG, Kaptchuk TJ. The power of context: reconceptualizing the placebo effect. J R Soc Med. 2008;101(5):222–225. doi:10.1258/jrsm.2008.070466
5. Kállai I, Barke A, Voss U. The effects of experimenter characteristics on pain reports in women and men. Pain. 2004;112(1–2):142–147. doi:10.1016/j.pain.2004.08.008
6. Levine FM, De Simone LL. The effects of experimenter gender on pain report in male and female subjects. Pain. 1991;44(1):69–72. doi:10.1016/0304-3959(91)90149-R
7. Gracely R, Dubner R, Deeter W, Wolskee P. CLINICIANS’ EXPECTATIONS INFLUENCE PLACEBO ANALGESIA. Lancet. 1985;325(8419):43. doi:10.1016/S0140-6736(85)90984-5
8. Kaptchuk TJ, Kelley JM, Conboy LA, et al. Components of placebo effect: randomised controlled trial in patients with irritable bowel syndrome. BMJ. 2008;336(7651):999–1003. doi:10.1136/bmj.39524.439618.25
9. Daniali H, Flaten MA. A qualitative systematic review of effects of provider characteristics and nonverbal behavior on pain, and placebo and nocebo effects. Frontiers in Psychiatry. 2019;10:432431.
10. Ruben MA, Blanch-Hartigan D, Hall JA. Nonverbal communication as a pain reliever: the impact of physician supportive nonverbal behavior on experimentally induced pain. Health Communication. 2017;32(8):970–976. doi:10.1080/10410236.2016.1196418
11. Ambady N, Gray HM. On being sad and mistaken: mood effects on the accuracy of thin-slice judgments. J Person Soc Psycho. 2002;83(4):947. doi:10.1037/0022-3514.83.4.947
12. Knapp ML, Hall JA, Horgan TG. Nonverbal Communication in Human Interaction. Cengage Learning; 2013.
13. Ambady N, Bernieri FJ, Richeson JA. Toward a histology of social behavior: judgmental accuracy from thin slices of the behavioral stream. In: Mark P. Zanna Advances in Experimental Social Psychology. Vol32. Elsevier; 2000:201–271.
14. Necka EA, Amir C, Dildine TC, Atlas LY. Expectations about pain and analgesic treatment are shaped by medical providers’ facial appearances: evidence from five online clinical simulation experiments. Soc sci med. 2021;281:114091. doi:10.1016/j.socscimed.2021.114091
15. Valentini E, Martini M, Lee M, Aglioti SM, Iannetti G. Seeing facial expressions enhances placebo analgesia. PAIN. 2014;155(4):666–673. doi:10.1016/j.pain.2013.11.021
16. Kraft-Todd GT, Reinero DA, Kelley JM, Heberlein AS, Baer L, Riess H. Empathic nonverbal behavior increases ratings of both warmth and competence in a medical context. PLoS One. 2017;12(5):e0177758. doi:10.1371/journal.pone.0177758
17. Chen P-HA, Cheong JH, Jolly E, Elhence H, Wager TD, Chang LJ. Socially transmitted placebo effects. Nat Human Behav. 2019;3(12):1295–1305. doi:10.1038/s41562-019-0749-5
18. Czerniak E, Biegon A, Ziv A, et al. Manipulating the placebo response in experimental pain by altering doctor’s performance style. Frontiers in Psychology. 2016;7:874. doi:10.3389/fpsyg.2016.00874
19. Colloca L, Akintola T, Haycock NR, et al. Prior therapeutic experiences, not expectation ratings, predict placebo effects: an experimental study in chronic pain and healthy participants. Psycho Psychos. 2020;89(6):371–378. doi:10.1159/000507400
20. Aslaksen PM, Bystad M, Vambheim SM, Flaten MA. Gender differences in placebo analgesia: event-related potentials and emotional modulation. Psychosomatic Med. 2011;73(2):193–199. doi:10.1097/PSY.0b013e3182080d73
21. Lyby PS, Aslaksen PM, Flaten MA. Is fear of pain related to placebo analgesia? J Psycho Res. 2010;68(4):369–377. doi:10.1016/j.jpsychores.2009.10.009
22. Vambheim SM, Flaten MA. A systematic review of sex differences in the placebo and the nocebo effect. J Pain Res. 2017;Volume 10:1831–1839. doi:10.2147/JPR.S134745
23. Enck P, Klosterhalfen S. Does sex/gender play a role in placebo and nocebo effects? Conflicting evidence from clinical trials and experimental studies. Front Neurosci. 2019;13:160. doi:10.3389/fnins.2019.00160
24. McNeil DW, Rainwater AJ. Development of the fear of pain questionnaire-III. J Behaviorl Med. 1998;21(4):389–410. doi:10.1023/A:1018782831217
25. Lyby PS, Aslaksen PM, Flaten MA. Variability in placebo analgesia and the role of fear of pain—an ERP study. PAIN. 2011;152(10):2405–2412. doi:10.1016/j.pain.2011.07.010
26. Aslaksen PM, Flaten MA. The roles of physiological and subjective stress in the effectiveness of a placebo on experimentally induced pain. Psychosomatic Med. 2008;70(7):811–818. doi:10.1097/PSY.0b013e31818105ed
27. Daniali H, Flaten MA. Placebo analgesia, nocebo hyperalgesia, and the cardiovascular system: a qualitative systematic review. Front Physiol. 2020;11:549807. doi:10.3389/fphys.2020.549807
28. Pollo A, Vighetti S, Rainero I, Benedetti F. Placebo analgesia and the heart. Pain. 2003;102(1–2):125–133. doi:10.1016/s0304-3959(02)00345-7
29. Frangos E, Richards EA, Bushnell MC. Do the psychological effects of vagus nerve stimulation partially mediate vagal pain modulation? Neurobiol Pain. 2017;1:37–45. doi:10.1016/j.ynpai.2017.03.002
30. Koenig J, Jarczok M, Ellis R, Hillecke T, Thayer JF. Heart rate variability and experimentally induced pain in healthy adults: a systematic review. Eur J Pain. 2014;18(3):301–314. doi:10.1002/j.1532-2149.2013.00379.x
31. Thayer JF, Lane RD. Claude Bernard and the heart–brain connection: further elaboration of a model of neurovisceral integration. Neurosci Biobehav Rev. 2009;33(2):81–88. doi:10.1016/j.neubiorev.2008.08.004
32. Daniali H, Ruben MA, Flaten MA. Systematic manipulation of experimenters’ non-verbal behaviors for the investigation of pain reports and placebo effects. Frontiers in Psycho. 2023;14:1248127.
33. Hunter T, Siess F, Colloca L. Socially induced placebo analgesia: a comparison of a pre‐recorded versus live face‐to‐face observation. Eur J Pain. 2014;18(7):914–922. doi:10.1002/j.1532-2149.2013.00436.x
34. Niskanen J-P, Tarvainen MP, Ranta-Aho PO, Karjalainen PA. Software for advanced HRV analysis. Comput Meth Prog Biomed. 2004;76(1):73–81. doi:10.1016/j.cmpb.2004.03.004
35. Tarvainen M, Lipponen J, Niskanen J, Ranta-aho p. kubios HRV software: user’s guide. kubios oy; 2021.
36. Lipponen JA, Tarvainen MP. A robust algorithm for heart rate variability time series artefact correction using novel beat classification. J Med Eng Technol. 2019;43(3):173–181. doi:10.1080/03091902.2019.1640306
37. Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17(1):45–56. doi:10.1016/0304-3959(83)90126-4
38. Mackay C, Cox T, Burrows G, Lazzerini T. An inventory for the measurement of self-reported stress and arousal. British J Soc Clini Psycho. 1978;17(3):283–284. doi:10.1111/j.2044-8260.1978.tb00280.x
39. Vambheim SM, Daniali H, Flaten MA. Placebo effects on stress, but not on pain reports. a multi-experiment study. Frontiers in Psycho. 2021;12:639236. doi:10.3389/fpsyg.2021.639236
40. Bjørkedal E, Flaten MA. Interaction between expectancies and drug effects: an experimental investigation of placebo analgesia with caffeine as an active placebo. Psychopharmacology. 2011;215(3):537–548. doi:10.1007/s00213-011-2233-4
41. Crosta Ahlforn K, Bojner Horwitz E, Osika W. A Swedish version of the Consultation and Relational Empathy (CARE) measure. Scand j Primary Health Care. 2017;35(3):286–292. doi:10.1080/02813432.2017.1358853
42. Vambheim SM, Lyby PS, Aslaksen PM, Flaten MA, Åsli O, Martinussen LM. The fear of pain questionnaire-III and the fear of pain questionnaire-short form: a confirmatory factor analysis. J Pain Res. 2017;Volume 10:1871–1878. doi:10.2147/JPR.S133032
43. John OP, Donahue EM, Kentle RL. Big five inventory. J Person Soc Psycho. 1991;113(1):117
44. Olejnik S, Algina J. Generalized eta and omega squared statistics: measures of effect size for some common research designs. Psycho Meth. 2003;8(4):434. doi:10.1037/1082-989X.8.4.434
45. Wilcox RR. Introduction to Robust Estimation and Hypothesis Testing. Academic press; 2011.
46. Blanca Mena MJ, Alarcón Postigo R, Arnau Gras J, Bono Cabré R, Bendayan R. Non-normal data: is ANOVA still a valid option? Psicothema. 2017;29(num 4):552–557. doi:10.7334/psicothema2016.383
47. Johnson RA, Wichern DW Applied multivariate statistical analysis. 2002.
48. He X, Sun Q, Stetler C. Warm communication style strengthens expectations and increases perceived improvement. Health Communication. 2018;33(8):939–945. doi:10.1080/10410236.2017.1322482
49. Daniali H, Hunsbeth PL, Flaten MA. Effects of open and hidden administration of treatment-related information; a multi-experiment study. Psychol Health. 2023.
50. Daniali H, Ruben MA, Flaten MA Systematic manipulation of experimenter’s nonverbal behaviors for the investigation of placebo effects. 2023.
51. Flaten MA, Bjørkedal E, Lyby PS, Figenschau Y, Aslaksen PM. Failure to find a conditioned placebo analgesic response. Frontiers in Psycho. 2018;9:1198. doi:10.3389/fpsyg.2018.01198
52. Lyby PS, Forsberg JT, Åsli O, Flaten MA. Induced fear reduces the effectiveness of a placebo intervention on pain. PAIN. 2012;153(5):1114–1121. doi:10.1016/j.pain.2012.02.042
53. Flaten MA, Aslaksen PM, Lyby PS, Bjørkedal E. The relation of emotions to placebo responses. Philos Trans R Soc B. 2011;366(1572):1818–1827. doi:10.1098/rstb.2010.0407
54. Colloca L, Pine DS, Ernst M, Miller FG, Grillon C. Vasopressin boosts placebo analgesic effects in women: a randomized trial. Biol Psychiatry. 2016;79(10):794–802. doi:10.1016/j.biopsych.2015.07.019
55. Pei J, Chen H, Ma T, et al. Pain catastrophizing and associated factors in preoperative total knee arthroplasty in Lanzhou, China: a cross-sectional study. BMC Musculo Dis. 2022;23(1):1–8. doi:10.1186/s12891-022-05435-1
56. van Osch M, van Dulmen S, Van Vliet L, Bensing J. Specifying the effects of physician’s communication on patients’ outcomes: a randomised controlled trial. Patient Educ Couns. 2017;100(8):1482–1489. doi:10.1016/j.pec.2017.03.009
57. Andersen JF, Andersen PA, Jensen AD. The measurement of nonverbal immediacy. J app commun res. 1979;7(2):153–180. doi:10.1080/00909887909365204
58. Iacovides S, Avidon I, Baker F. Does pain vary across the menstrual cycle? A review. Eur J Pain. 2015;19(10):1389–1405. doi:10.1002/ejp.714
59. Keogh E. Sex and gender differences in pain: past, present, and future. Pain. 2022;163(S1):S108–S16. doi:10.1097/j.pain.0000000000002738
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.