")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
The Platelet-to-Lymphocyte Ratio Predicts Diabetic Retinopathy in Type 2 Diabetes Mellitus
Authors Zeng J , Chen M, Feng Q, Wan H, Wang J, Yang F, Cao H
Received 14 June 2022
Accepted for publication 15 November 2022
Published 22 November 2022 Volume 2022:15 Pages 3617—3626
DOI https://doi.org/10.2147/DMSO.S378284
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Antonio Brunetti
Jing Zeng,1 Min Chen,1 Qiu Feng,1 Haiyan Wan,1 Jianbo Wang,2 Fan Yang,1 Hongyi Cao1
1Geriatric Diseases Institute of Chengdu/Cancer Prevention and Treatment Institute of Chengdu, Department of Endocrinology and Metabolism, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), Chengdu, People’s Republic of China; 2Geriatric Diseases Institute of Chengdu/Cancer Prevention and Treatment Institute of Chengdu, Department of Medical Record, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), Chengdu, People’s Republic of China
Correspondence: Hongyi Cao; Fan Yang, Geriatric Diseases Institute of Chengdu/Cancer Prevention and Treatment Institute of Chengdu, Department of Endocrinology and Metabolism, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), No. 33, Mashi Street, Wenjiang District, Chengdu, Sichuan, 611130, People’s Republic of China, Tel +86 13730683979, Fax +86 028-82713097, Email [email protected]; [email protected]
Introduction: As a severe and specific neurovascular complication of type 2 diabetes mellitus (T2DM), diabetic retinopathy (DR) remains the leading cause of vision loss and preventable blindness in adults aged 20 to 74. The pathogenesis of DR is not completely understood, however, studies indicate that chronic inflammation plays a significant role. Emerging evidence suggests that the neutrophil-to-lymphocyte ratio (NLR), the platelet-to-lymphocyte ratio (PLR), and the monocyte-to-lymphocyte ratio (MLR) are novel potential inflammatory response markers. The purpose of this study was to investigate the relationships between the NLR, PLR, MLR, and DR.
Patients and Methods: 290 patients who had been diagnosed with T2DM participated in the study. Patients were categorized into three groups: 142 control subjects with T2DM, 124 subjects with nonproliferative diabetic retinopathy (NPDR), and 24 patients with proliferative diabetic retinopathy (PDR). Characteristics, laboratory data, as well as NLR, PLR and MLR levels of the study groups were compared.
Results: In patients with DR, the median NLR, PLR, and MLR were significantly higher than in patients without DR (p = 0.012, p < 0.001, and p = 0.043, respectively). In the post hoc analysis, there was no correlation between the severity of retinopathy and the increase in NLR or PLR. Multiple logistic regression revealed that the PLR was an independent risk factor for DR (odds ratio [OR]: 1.020, 95% confidence interval [CI]: 1.010– 1.029 p = 0.026). Based on the receiver operating characteristic (ROC) curve, the cutoff value of PLR as an indicator for diagnosing DR was estimated to be 129.65, with a sensitivity and specificity of 53.4% and 76.1%, respectively, and an area under the curve of 0.668 (95% CI: 0.605– 0.730, p < 0.001).
Conclusion: Our findings suggest that PLR may be an independent risk factor for evaluating DR in type 2 diabetes patients.
Keywords: type 2 diabetes mellitus, diabetic retinopathy, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, inflammation
Introduction
Diabetes mellitus (DM) is a systemic metabolic disorder. Chronic hyperglycemia can lead to a variety of long-term micro- and macrovascular complications.1 Diabetic retinopathy (DR) is the most prevalent complication of DM, with a prevalence among diabetic patients of approximately 34.6%.2–4 As a severe and specific neurovascular complication of DM, DR continues to be the leading cause of vision loss and preventable blindness among adults aged 20–65.4–6 DR has an insidious onset and is typically asymptomatic in its early stages; consequently, many patients have missed the optimal time for treatment by the time DR is diagnosed. Therefore, early detection and timely treatment are crucial for enhancing the vision and quality of life of patients. Retinal photography, fundus examination (ophthalmoscopy), fundus fluorescein angiography (FFA), optical coherence tomography (OCT), optical coherence tomography angiography (OCTA), and ocular ultrasonography are conventional methods of retinal examination. However, national screening programs in many countries lack sufficient funding, making it imperative to find a simple and effective method for DR screening.
Duration of disease, high BMI, glycemic control, hypertension, diabetic nephropathy, puberty, pregnancy, anemia, dyslipidemia, serum bilirubin levels, and cataract surgery are risk factors for DR.4,7–10 The pathogenesis of DR is complex and multifactorial and is not fully understood; however, inflammation is widely acknowledged to play a significant role.11–13 White blood cell (WBC) count and its subtypes, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR), are potential novel indicators of systemic inflammation in various diseases, according to substantial evidence. It has been demonstrated that elevated NLR is a useful predictor of cardiovascular risk,14 a significant biomarker of disease severity in patients with inflammatory bowel disease (IBD),15 and a prognostic factor for multiple malignancies.16,17 In a similar vein, it has been evidenced that elevated PLR correlates with the severity of ankylosing spondylitis (AS),18 that PLR is significantly elevated in patients with rheumatoid arthritis (RA),19 and that PLR exhibits prognostic value in a variety of malignancies.20,21 Finally, it has been indicated that MLR is a prognostic factor in patients with cancer and tuberculosis.22,23 Intriguingly, mounting evidence reveals that these inflammatory markers are also prognostic factors for DM and related complications.24–26 As easily accessible and inexpensive inflammatory markers, the blood cell-associated inflammatory indices may hold promise as a new diagnostic tool for DR. However, only a handful of articles have assessed the relationship between these factors and DR. The purpose of this study was to evaluate the relationships between DR and the NLR, PLR, and MLR, considering this context.
Materials and Methods
This single-center retrospective study was conducted between January 2018 and June 2022 in the Department of Endocrinology and Metabolism of Chengdu Fifth People’s Hospital in Chengdu. Patients diagnosed with T2DM were enrolled in this study. The diagnosis of type 2 diabetes was rendered predicated on the criteria established by the World Health Organization in 1999.27 Patients were excluded if they were younger than 18 years of age, had type 1 diabetes, pregnancy, any acute inflammatory condition, acute or chronic renal failure, liver or heart disease, a history of cataract, glaucoma or other eye diseases, comorbid acute complications of diabetes, diabetic nephropathy, malignancy, autoimmune disease, inflammatory bowel disease, connective tissue disease, hematologic disorders, received oral steroids or had recently undergone surgery. Written informed consent was obtained from all participants. The study was approved by the Ethics Committee of Chengdu Fifth People’s Hospital.
Evaluation of DR
Using a non-mydriatic fundus camera, all included patients were examined for DR (CR-2AF, Canon, Tokyo, Japan). After a brief dark adaptation period (approximately five min), two 45° fundus photographs of the fundus were taken, each centered on the fovea and optic disc of one eye. After allowing the patient to rest for approximately three minutes, the other eye was photographed once the pupil had recovered. Evaluations of DR were performed by ophthalmologists who were blinded to the results of our study and had extensive training. The severity of DR was measured utilizing the International Clinical Diabetic Retinopathy Disease Severity Scale:28 (1) no apparent retinopathy: no abnormalities; (2) mild nonproliferative diabetic retinopathy (NPDR) with only microaneurysms; (3) moderate NPDR: greater than microaneurysms but less than severe NPDR (4) severe NPDR: any of the following: more than 20 intraretinal hemorrhages in each of the four quadrants; definite venous beading in two or more quadrants; prominent intraretinal microvascular abnormalities in one or more quadrants with no evidence of proliferative retinopathy; (5) Proliferative diabetic retinopathy (PDR): one or more of the following: neovascularization; vitreous/preretinal hemorrhage.
Clinical Information and Biochemical Examination
The following clinical data were collected from all participants: age, sex, systolic blood pressure (SBP), diastolic blood pressure (DBP), body mass index (BMI), smoking, history of hypertension, and diabetic peripheral neuropathy (DPN). Laboratory variables included glycosylated hemoglobin A1c (HbA1c), total bilirubin (TBL), albumin, serum creatinine (Scr), blood urea nitrogen (BUN), triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL), and low-density lipoprotein cholesterol (LDL), HGB(hemoglobin).
Definitions of Terms
The NLR, PLR, and MLR were calculated as the ratios of the absolute peripheral neutrophils, platelets, and monocytes to lymphocytes, respectively. The same automated blood sample measurements taken when participants were admitted to the study served as the basis for all counts.
Statistical Analysis
All statistical analyses were conducted with SPSS 23.0 and GraphPad Prism 6. For normally distributed numerical variables, all data are expressed as the mean (SD, standard deviation), and for non normally distributed variables, the median (IQR, interquartile range). Categorical variables are presented as numbers (percentages). To evaluate the distribution of variables, the Kolmogorov–Smirnov test was performed. We performed Student’s t-tests and one-way ANOVA on continuous variables with normal distribution, the Mann–Whitney U or Kruskal–Wallis H-test on continuous variables with non-normal distribution, and the chi-square test on categorical variables. Utilizing multivariable logistic regression, the independent risk factors for DR were evaluated. The cutoff values were determined using a receiver operating curve (ROC) analysis. Significance was defined as a two-sided P-value of < 0.05.
Results
In total, 290 patients were finally enrolled in the study. They were categorized into three groups: 142 control subjects with T2DM, 124 subjects with nonproliferative diabetic retinopathy (NPDR), and 24 patients with proliferative diabetic retinopathy (PDR). The baseline demographic and clinical characteristics of all 290 subjects are described in Table 1. The groups were similar in terms of age, gender, BMI, smoking, presence of hypertension, DBP, HbA1c, Scr, TG, TC, LDL-C, WBCs, neutrophils, lymphocytes, and monocytes levels (P > 0.05). Duration of DM, presence of DPN, SBP, TBIL, BUN, HDL-C, Platelets, HGB, NLR, PLR, and MLR were significantly different between DM and DR groups (p < 0.05). Specifically, DR patients had a longer duration of diabetes, higher levels of SBP, BUN, HDL-C, and Platelets, and a higher proportion of DPN presence compared to patients without DR. However, the levels of TBIL and HGB were lower in DR patients (p < 0.05). Patients with DR had significantly higher NLR, PLR, and MLR than patients without DR (p = 0.012, p < 0.001, and p = 0.0043, respectively). Patients with DR were classified into two groups dependent on severity (NPDR and PDR). The results are outlined in Table 2. The levels of NLR (2.84[2.08–4.17] in NPDR group versus 2.43[1.98–3.39] in patients without DR group, p = 0.020) and PLR (137.02[105.80–165.80] in NPDR group versus105.34 [92.41–128.98] in patients without DR group, p < 0.001) were significantly higher in NPDR group. In addition, neither NLR nor PLR were associated with the severity of retinopathy. The median MLR was 0.22 [0.18–0.27] in the PDR group, 0.21 [0.17–0.30] in the NPDR group, and 0.20 [0.15–0.27] in the control group, with no statistically significant difference (p = 0.115) between the three groups. The multiple logistic regression analysis revealed that independent risk factors for DR were DM duration (p = 0.017), SBP (p = 0.007), presence of DPN (p < 0.001), HGB (p = 0.024) and PLR (p = 0.026), as shown in Table 3. In addition, as the PLR increased by one unit, the risk of DR was determined to be 1.02 times greater. As an independent risk factor for DR, the PLR cutoff value was 129.65; the sensitivity and specificity of the PLR for DR diagnosis were 53.4% and 76.1%, respectively, with an area under the curve of 0.668 (95% CI: 0.605–0.730, p < 0.001). DM duration greater than 90 months have 60.1% sensitivity and 79.6% specificity in predicting DR (AUC: 0.733 [95% CI: 0.675−0.791]; p < 0.001). SBP levels greater than 142 mmHg have 27.0% sensitivity and 90.1% specificity in predicting DR (AUC: 0.60 [95% CI: 0.535−0.665]; p = 0.003). HGB levels lower than 133 g/dl have 56.1% sensitivity and 67.6% specificity in predicting DR (AUC: 0.653 [95% CI: 0.591−0.716]; p < 0.001). Figure 1 shows the ROC curves of the study parameters in determining DR.
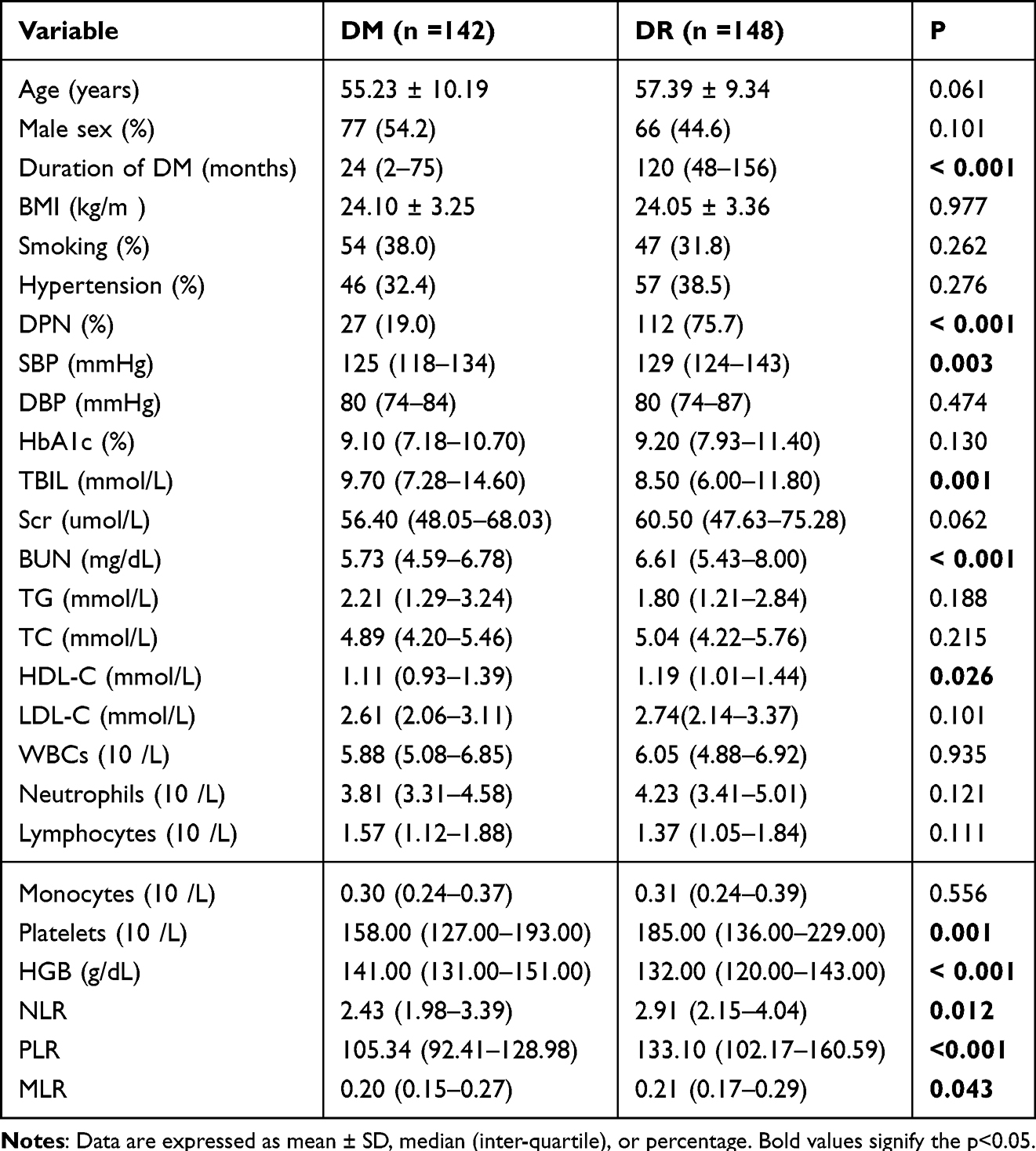 |
Table 1 Patients’ Baseline and Clinical Characteristics |
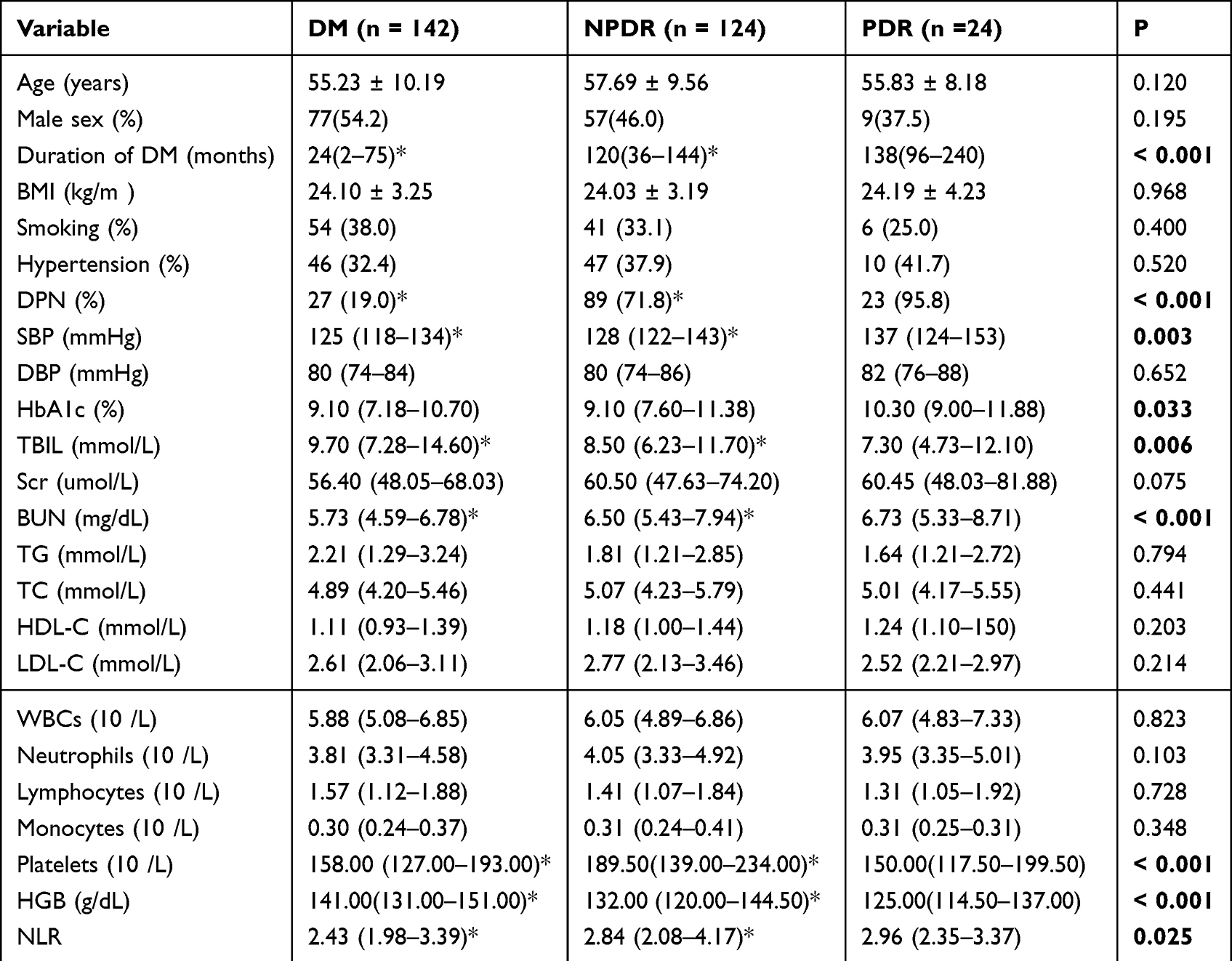 |
Table 2 Comparison of Clinical Characteristics and Hematological Parameters in Patients with and without Retinopathy and Its Severity |
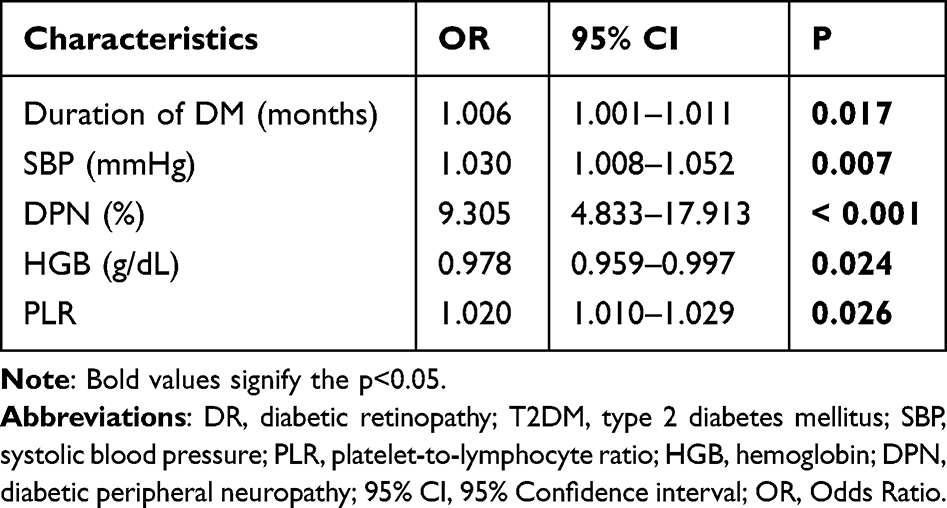 |
Table 3 Multivariate Analysis of DR in Patients with T2DM |
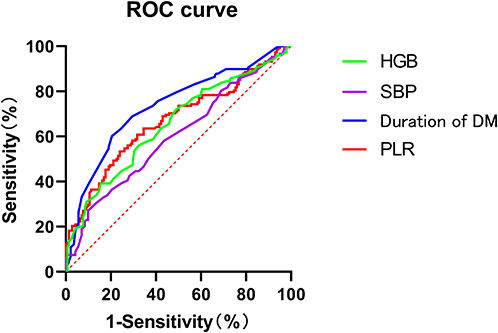 |
Figure 1 The receiver operating characteristic (ROC) curves for the optimal cut-off values of the platelet-to-lymphocyte (PLR) ratio, duration of diabetes mellitus (DM), systolic blood pressure (SBP) and HGB (hemoglobin) as predictors of diabetic retinopathy. |
Discussion
More than 415 million people worldwide had been diagnosed with diabetes by the year 2015, and the prevalence of the disease was gradually increasing.5 Diabetes can result in a variety of microvascular and macrovascular complications, such as cardiovascular disease, stroke, kidney disease, and retinopathy.29 The most severe form of ocular diabetes mellitus, diabetic retinopathy is also the leading cause of blindness in middle-aged and elderly people. There are several stages of diabetic retinopathy, including mild nonproliferative abnormalities characterized by increased vascular permeability; moderate and severe nonproliferative diabetic retinopathy (NPDR) characterized by vascular occlusion; and proliferative diabetic retinopathy (PDR) characterized by neovascularization of the retina and posterior vitreous surface. Early changes in diabetic retinopathy are typically asymptomatic, and many patients have already progressed to an irreversible stage before receiving treatment. Consequently, early detection and timely treatment for primary prevention will reduce the risk of vision loss.
Duration of disease, high BMI, glycemic control, hypertension, diabetic nephropathy, puberty, pregnancy, anemia, dyslipidemia, serum bilirubin levels, and cataract surgery are all risk factors for DR.7–9 It has been demonstrated that oxidative stress (OS) is a key factor in the etiology of DR. Hyperglycemia causes an increase in reactive oxygen species (ROS) in the retina, including superoxide anion (O2⋅-), hydrogen peroxide (H2O2), peroxyl radicals (ROO⋅), and extremely reactive hydroxyl radicals (⋅OH), which induces abnormal metabolic pathways in the cells. The four most classic pathways are the following: activation of the protein kinase C (PKC) pathway, increased polyol pathway flux, induction of the hexosamine pathway, and accumulation of advanced glycosylation end products (AGEs).30–32 Positive feedback from the activation of the preceding pathway promotes ROS production further. In addition, excessive ROS production and hyperglycemia-mediated epigenetic modification inhibit the antioxidant defense system, giving rise to an imbalance between ROS clearance and production, thereby promoting OS.33 The retina is one of the tissues with the highest oxygen consumption and is rich in polyunsaturated fatty acids that are easily oxidized, making it especially susceptible to OS and oxygen-free radical damage. OS can deteriorate cell membrane integrity, induce apoptosis, microvascular damage, and barrier damage, and ultimately lead to DR.31
The pathogenesis of DR is complex and multifactorial and is not fully understood, however, it is a widely held belief that inflammation also plays a significant role.11,34 Chronic low-grade inflammation is a crucial factor in the onset and progression of diabetes and accelerates the deterioration of microvascular disease and macrovascular disease in diabetic patients.11,35–37 Neuregulin-4, an inflammatory cytokine, was found to be elevated in patients with diabetic microangiopathy complications, according to Kocak et al.38 The CARE TIME study demonstrated that the ratio of C-reactive protein to serum albumin (CAR), a serum inflammatory predictor, was elevated in type 2 diabetes nephropathy patients.39 In addition, it has been discovered that dysregulated activation of pattern recognition receptors (PRRs) contributes to inflammatory diseases and assumes a key part in the pathogenesis of diabetic vascular complications. Toll‐like receptors (TLRs), the most characteristic PRR, are increased in expression in patients with diabetic nephropathy, diabetic retinopathy, diabetic neuropathy, and diabetic cardiomyopathy.40 Leukocyte adhesion to the vascular system of the retina has been identified as a contributor to DR vascular pathology.11,41 Numerous inflammatory cytokines and chemokines, including interleukin1β (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), interleukin-6 (IL-2), tumor necrosis factor-α (TNF-α), interferon-γ, and monocyte chemotactic protein-1 (MCP1), have been reported to be elevated in serum and ocular samples (vitreous and atrial fluid) of DR patients.42 Hatori et al discovered that long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs) such as sulindac would be effective in preventing the progression of mild DR.43 There is growing evidence that inflammation plays a significant role in the onset and progression of DR.11
Numerous studieshave14–23 demonstrated that NLR, PLR, and MLR are potential inflammatory biomarkers for tumors, cardiovascular disease, ankylosing spondylitis, rheumatoid arthritis, and inflammatory bowel disease. In addition, there is mounting evidence connecting them to the progression of DM and its complications. Atak et al found that the median PLR of patients with type 2 diabetes was significantly higher than that of healthy controls, and PLR may be beneficial for predicting the development and control levels of type 2 diabetes.44 Huang et al discovered previously that NLR could be used to predict coronary artery vulnerable plaques (VPs) in T2DM patients.45 A 3-year follow-up study found that NLR predicted renal function decline in diabetic patients.46 In the study by Jaaban et al, elevated NLR and PLR were significantly associated with diabetic nephropathy, and high NLR and PLR could be used as predictors and prognostic risk indicators of diabetic nephropathy.47 Additionally, MLR can be employed as a predictive and effective marker of diabetic kidney injury (DKI).48 In accordance with the findings of Ulu et al49, our findings indicated that DM patients with DR had significantly higher NLR levels than those without DR. They also found a correlation between NLR and DR grades, but in our study, retinopathy severity was not associated with an increase in NLR. Similarly to the findings of Yue et al,50 our study discovered that the NLR, MLR and PLR levels of DR patients were higher than those of patients without DR. According to their research, the MLR is a risk factor for DR. In our study, however, we discovered that the PLR, rather than the MLR, was an independent risk factor for DR. The NLR and PLR levels were recently discovered to be significantly higher among DR patients without an associated family history compared to NDR patients in a study by Wang et al.51 After fully adjusting for confounding factors, they discovered that the NLR remained an independent risk factor for DR. Intriguingly, a meta-analysis of the prognostic value of blood cell-associated inflammation in 31 studies revealed that elevated NLR and PLR values could serve as diagnostic biomarkers for DR.52 This difference may be the result of different sample sizes, subject heterogeneity, and lifestyle differences.
Early detection of diabetic retinopathy is crucial for preventing irreversible vision loss; however, DR screening services are still unequally distributed between developing and developed countries; therefore, it is urgent to identify a simple, effective, and cost-effective screening method. In the current study, we found that PLR was an independent risk factor for DR after controlling for confounding variables such as the duration of diabetes, SBP, TBL, BUN, HDL-C, HGB, and other confounding variables. Each 1 unit increase in PLR was associated with a 1.020-fold increase in the risk of DR. In comparison to inflammatory cytokines such as IL-6, IL-8, IL-1β, and TNF-α, the calculation methods for the NLR, PLR, and LMR are quite straightforward, as they can be obtained through peripheral blood examination, which is inexpensive, convenient, and simple to explain. In addition, the NLR, PLR, and LMR are more stable than the neutrophil, lymphocyte, and total leukocyte counts when physiological, pathological, and physical factors of the WBC count change. Therefore, we propose PLR as a universal, non-invasive, cost-effective, and simple-to-apply test that might be used to assist in the assessment of DR risk in patients with diabetes.
We acknowledge that there are still some limitations to our study. First, the present study is a retrospective, single-center study. In addition, we were unable to confirm the predictive value of the factors in clinical practice due to the lack of follow-up. Therefore, additional research is necessary to determine the role of the PLR in predicting DR in diabetic patients.
Conclusions
In conclusion, the NLR, PLR, and MLR are significantly increased when DR is present. Our findings suggest that the PLR may be an independent risk factor when evaluating type 2 diabetes patients in terms of DR. However, further validation of these results is required through the undertaking of large-scale prospective studies.
Abbreviations
DM, diabetes mellitus; DR, diabetic retinopathy; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio; NPDR, non-proliferative diabetic retinopathy; PDR, proliferative diabetic retinopathy; ROC, Receiver operating curve; OR, odds ratio; FFA, fundus fluorescein angiography; OCT, optical coherence tomography; OCTA, optical coherence tomography angiography; IBD, bowel disease; AS, ankylosing spondylitis; RA, rheumatoid arthritis; DPN, diabetic peripheral neuropathy; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; TBL, total bilirubin; Scr, serum creatinine; BUN, blood urea nitrogen; TG, triglycerides; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; HGB, hemoglobin; WBC, white blood cell; Hgb, hemoglobin; OS, Oxidative stress; ROS, reactive oxygen species; PKC, protein kinase C; AGEs, advanced glycosylation end products; CAR, C-reactive protein to serum albumin ratio; PRRs, pattern recognition receptors; TLRs, Toll‐like receptors; IL-1β, interleukin1β; IL-6, interleukin-6; IL-8, interleukin-8; IL-2, interleukin-2; TNF-α, tumor necrosis factor-α; MCP1, monocyte chemotactic protein-1; NSAIDs, non-steroidal anti-inflammatory drugs; VPs, artery vulnerable plaques; DKI, diabetic kidney injury.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study complies with the Declaration of Helsinki and was approved by the Ethics Committee of Chengdu Fifth People’s Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Scientific Research Project of the Health and Family Planning Commission of Sichuan Province [Grant No. 18PJ352], the Scientific Research Project of the Health and Family Planning Commission of Chengdu Municipal [Grant Nos. 2018094 and 2018090], and the Scientific Research Fund of Chengdu Fifth People’s Hospital [Grant No.GSPZX2022-19].
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhang Y, Sun X, Icli B, et al. Emerging roles for MicroRNAs in diabetic microvascular disease: novel targets for therapy. Endocr Rev. 2017;38(2):145–168. doi:10.1210/er.2016-1122
2. Cole J, Florez J. Genetics of diabetes mellitus and diabetes complications. Nat Rev Nephrol. 2020;16(7):377–390. doi:10.1038/s41581-020-0278-5
3. Solomon S, Chew E, Duh E, et al. Diabetic retinopathy: a position statement by the American diabetes association. Diabetes Care. 2017;40(3):412–418. doi:10.2337/dc16-2641
4. Vujosevic S, Aldington S, Silva P, et al. Screening for diabetic retinopathy: new perspectives and challenges. Lancet Diabetes Endocrinol. 2020;8(4):337–347. doi:10.1016/S2213-8587(19)30411-5
5. Sabanayagam C, Banu R, Chee M, et al. Incidence and progression of diabetic retinopathy: a systematic review. Lancet Diabete Endocrinol. 2019;7(2):140–149. doi:10.1016/S2213-8587(18)30128-1
6. The Lancet Diabetes Endocrinology. Under the lens: diabetic retinopathy. Lancet Diabetes Endocrinol. 2020;8(11):869. doi:10.1016/S2213-8587(20)30347-8
7. Schorr S, Hammes H, Müller U, et al. The prevention and treatment of retinal complications in diabetes. Dtsch Arztebl Int. 2016;113(48):816–823. doi:10.3238/arztebl.2016.0816
8. Ahlqvist E, Van Zuydam N, Groop L, et al. The genetics of diabetic complications. Nat Rev Nephrol. 2015;11(5):277–287. doi:10.1038/nrneph.2015.37
9. Wong TY, Cheung CMG, Larsen M, et al. Diabetic retinopathy. Nat Rev Dis Primers. 2016;2:16030. doi:10.1038/nrdp.2016.30
10. Ding Y, Zhao J, Liu G, et al. Total bilirubin predicts severe progression of diabetic retinopathy and the possible causal mechanism. J Diabetes Res. 2020;2020:7219852. doi:10.1155/2020/7219852
11. Forrester J, Kuffova L, Delibegovic M. The role of inflammation in diabetic retinopathy. Front Immunol. 2020;11:583687. doi:10.3389/fimmu.2020.583687
12. Dehdashtian E, Mehrzadi S, Yousefi B, et al. Diabetic retinopathy pathogenesis and the ameliorating effects of melatonin; involvement of autophagy, inflammation and oxidative stress. Life Sci. 2018;193:20–33. doi:10.1016/j.lfs.2017.12.001
13. Spencer B, Estevez J, Liu E, et al. Pericytes, inflammation, and diabetic retinopathy. Inflammopharmacology. 2020;28(3):697–709. doi:10.1007/s10787-019-00647-9
14. Agarwal R, Aurora R, Siswanto B, et al. The prognostic value of neutrophil-to-lymphocyte ratio across all stages of coronary artery disease. Coron Artery Dis. 2022;33(2):137–143. doi:10.1097/MCA.0000000000001040
15. Fu W, Fu H, Ye W, et al. Peripheral blood neutrophil-to-lymphocyte ratio in inflammatory bowel disease and disease activity: a meta-analysis. Int Immunopharmacol. 2021;101:108235. doi:10.1016/j.intimp.2021.108235
16. Gemenetzis G, Bagante F, Griffin J, et al. Neutrophil-to-lymphocyte ratio is a predictive marker for invasive malignancy in intraductal papillary mucinous neoplasms of the pancreas. Ann Surg. 2017;266(2):339–345. doi:10.1097/SLA.0000000000001988
17. Patel A, Ravaud A, Motzer R, et al. Neutrophil-to-lymphocyte ratio as a prognostic factor of disease-free survival in postnephrectomy high-risk locoregional renal cell carcinoma: analysis of the S-TRAC trial. Clin Cancer Res. 2020;26(18):4863–4868. doi:10.1158/1078-0432.CCR-20-0704
18. Liang T, Chen J, Xu G, et al. Platelet-to-lymphocyte ratio as an independent factor was associated with the severity of ankylosing spondylitis. Front Immunol. 2021;12:760214. doi:10.3389/fimmu.2021.760214
19. Erre G, Paliogiannis P, Castagna F, et al. Meta-analysis of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in rheumatoid arthritis. Eur J Clin Invest. 2019;49(1):e13037. doi:10.1111/eci.13037
20. Liu D, Czigany Z, Heij L, et al. The value of platelet-to-lymphocyte ratio as a prognostic marker in cholangiocarcinoma: a systematic review and meta-analysis. Cancers. 2022;14:2.
21. Yu Y, Wang L, Cao S, et al. Pre-radiotherapy lymphocyte count and platelet-to-lymphocyte ratio may improve survival prediction beyond clinical factors in limited stage small cell lung cancer: model development and validation. Transl Lung Cancer Res. 2020;9(6):2315–2327. doi:10.21037/tlcr-20-666
22. Chen L, Liu C, Liang T, et al. Monocyte-to-lymphocyte ratio was an independent factor of the severity of spinal tuberculosis. Oxid Med Cell Longev. 2022;2022:7340330. doi:10.1155/2022/7340330
23. Jakubowska K, Koda M, grudzińska M, et al. Monocyte-to-lymphocyte ratio as a prognostic factor in peripheral whole blood samples of colorectal cancer patients. World J Gastroenterol. 2020;26(31):4639–4655. doi:10.3748/wjg.v26.i31.4639
24. Liu J, Liu X, Li Y, et al. The association of neutrophil to lymphocyte ratio, mean platelet volume, and platelet distribution width with diabetic retinopathy and nephropathy: a meta-analysis. Biosci Rep. 2018;38:3. doi:10.1042/BSR20180172
25. Verdoia M, Schaffer A, Barbieri L, et al. Impact of diabetes on neutrophil-to-lymphocyte ratio and its relationship to coronary artery disease. Diabetes Metab. 2015;41(4):304–311. doi:10.1016/j.diabet.2015.01.001
26. Duman T, Aktas G, Atak B, et al. Neutrophil to lymphocyte ratio as an indicative of diabetic control level in type 2 diabetes mellitus. Afr Health Sci. 2019;19(1):1602–1606. doi:10.4314/ahs.v19i1.35
27. Puavilai G, Chanprasertyotin S, Sriphrapradaeng A. Diagnostic criteria for diabetes mellitus and other categories of glucose intolerance: 1997 criteria by the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (ADA), 1998 WHO consultation criteria, and 1985 WHO criteria World Health Organization. Diabetes Res Clin Pract. 1999;44(1):21–26. doi:10.1016/S0168-8227(99)00008-X
28. Wilkinson C, Ferris F, Klein R, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 2003;110(9):1677–1682. doi:10.1016/S0161-6420(03)00475-5
29. Defronzo R, Ferrannini E, Groop L, et al. Type 2 diabetes mellitus. Nat Rev Dis Primers. 2015;1:15019. doi:10.1038/nrdp.2015.19
30. Kang Q, Yang CJ. Oxidative stress and diabetic retinopathy: molecular mechanisms, pathogenetic role and therapeutic implications. Redox Biol. 2020;37:101799. doi:10.1016/j.redox.2020.101799
31. Wu M, Yiang G, Lai T, et al. The oxidative stress and mitochondrial dysfunction during the pathogenesis of diabetic retinopathy. Oxid Med Cell Longev. 2018;2018:3420187. doi:10.1155/2018/3420187
32. Li C, Miao X, Li F, et al. Oxidative stress-related mechanisms and antioxidant therapy in diabetic retinopathy. Oxid Med Cell Longev. 2017;2017:9702820. doi:10.1155/2017/9702820
33. Bokhary K, Aljaser F, Abudawood M, et al. Role of oxidative stress and severity of diabetic retinopathy in type 1 and type 2 diabetes. Ophthalmic Res. 2021;64(4):613–621. doi:10.1159/000514722
34. Semeraro F, Morescalchi F, Cancarini A, et al. Diabetic retinopathy, a vascular and inflammatory disease: therapeutic implications. Diabetes Metab. 2019;45(6):517–527. doi:10.1016/j.diabet.2019.04.002
35. Chen J, Tan W. Platelet activation and immune response in diabetic microangiopathy. Clin Chim Acta. 2020;507:242–247. doi:10.1016/j.cca.2020.04.042
36. Nwadiugwu M. Inflammatory activities in type 2 diabetes patients with co-morbid angiopathies and exploring beneficial interventions: a systematic review. Public Health Front. 2020;8:600427. doi:10.3389/fpubh.2020.600427
37. Rohm T, Meier D, Olefsky J, et al. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55(1):31–55. doi:10.1016/j.immuni.2021.12.013
38. Kocak M, Aktas G, Atak B, et al. Is Neuregulin-4 a predictive marker of microvascular complications in type 2 diabetes mellitus? Eur J Clin Invest. 2020;50(3):e13206. doi:10.1111/eci.13206
39. Bilgin S, Kurtkulagi O, Atak Tel B, et al. Does C-reactive protein to serum Albumin Ratio correlate with diabEtic nephropathy in patients with Type 2 dIabetes Mellitus? Care Time Study. 2021;15(6):1071–1074.
40. Wang X, Antony V, Wang Y, et al. Pattern recognition receptor-mediated inflammation in diabetic vascular complications. Med Res Rev. 2020;40(6):2466–2484. doi:10.1002/med.21711
41. Pauline HE, Gaucher D. Diabetic retinopathy. Rev Prat. 2017;67(9):1001–1008.
42. Rübsam A, Parikh S, Fort P. Role of inflammation in diabetic retinopathy. International journal of molecular sciences. Int J Mol Sci. 2018;19:4. doi:10.3390/ijms19040942
43. Hattori Y, Hashizume K, Nakajima K, et al. The effect of long-term treatment with sulindac on the progression of diabetic retinopathy. Curr Med Res Opin. 2007;23(8):1913–1917. doi:10.1185/030079907X218770
44. Atak B, Aktas G, Duman TT, et al. Diabetes control could through platelet-to-lymphocyte ratio in hemograms. Rev Assoc Med Bras. 2019;65(1):38–42. doi:10.1590/1806-9282.65.1.38
45. Huang X, Yang S, Zhao Q, et al. Predictive value of non-high-density lipoprotein cholesterol and neutrophil-lymphocyte ratio for coronary artery vulnerable plaques in type 2 diabetes mellitus. Front Cardiovasc Med. 2022;9:927768. doi:10.3389/fcvm.2022.927768
46. Azab B, Daoud J, Naeem FB, et al. Neutrophil-to-lymphocyte ratio as a predictor of worsening renal function in diabetic patients (3-year follow-up study). Ren Fail. 2012;34(5):571–576. doi:10.3109/0886022X.2012.668741
47. Jaaban M, Zetoune AB, Hesenow S, et al. Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as novel risk markers for diabetic nephropathy in patients with type 2 diabetes. Heliyon. 2021;7(7):e07564. doi:10.1016/j.heliyon.2021.e07564
48. Kocak MZ, Aktas G, Duman TT, et al. Monocyte lymphocyte ratio As a predictor of diabetic kidney injury in type 2 diabetes mellitus; The MADKID Study. J Diabetes Metab Disord. 2020;19(2):997–1002. doi:10.1007/s40200-020-00595-0
49. Ulu S, Dogan M, Ahsen A, et al. Neutrophil-to-lymphocyte ratio as a quick and reliable predictive marker to diagnose the severity of diabetic retinopathy. Diabetes Technol Ther. 2013;15(11):942–947. doi:10.1089/dia.2013.0097
50. Yue S, Zhang J, Wu J, et al. Use of the monocyte-to-lymphocyte ratio to predict diabetic retinopathy. Int J Environ Res Public Health. 2015;12(8):10009–10019. doi:10.3390/ijerph120810009
51. Wang J, Chen Z, Yang K, et al. Association between neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and diabetic retinopathy among diabetic patients without a related family history. Diabetol Metab Syndr. 2020;12:55. doi:10.1186/s13098-020-00562-y
52. Luo W, Zhang W. The relationship of blood cell-associated inflammatory indices and diabetic retinopathy: a Meta-analysis and systematic review. Int J Ophthalmol. 2019;12(2):312–323. doi:10.18240/ijo.2019.02.20
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.