")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
The Role of Cosmetology in an Effective Treatment of Rosacea: A Narrative Review
Authors Sobkowska D, Szałapska A , Pawlaczyk M , Urbańska M, Micek I, Wróblewska-Kończalik K, Sobkowska J , Jałowska M, Gornowicz-Porowska J
Received 16 March 2023
Accepted for publication 17 May 2023
Published 5 June 2023 Volume 2023:16 Pages 1419—1430
DOI https://doi.org/10.2147/CCID.S412800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Daria Sobkowska,1 Aleksandra Szałapska,1 Mariola Pawlaczyk,1 Maria Urbańska,1 Iwona Micek,1 Katarzyna Wróblewska-Kończalik,2 Julia Sobkowska,3 Magdalena Jałowska,4 Justyna Gornowicz-Porowska1
1Department and Division of Practical Cosmetology and Prevention of Skin Diseases, Poznan University of Medical Sciences, Poznan, 60-806, Poland; 2Kolasinski Clinic, Swarzedz, 62-020, Poland; 3Medical Centre Bonus 2001, Skorzewo, 60-185, Poland; 4Department of Dermatology, Poznan University of Medical Sciences, Poznan, 60-355, Poland
Correspondence: Daria Sobkowska, Poznan University of Medical Sciences, 3 Rokietnicka Street, Poznań, 60-806, Poland, Tel +48 61 848-04-75, Email [email protected]
Abstract: Rosacea is a chronic inflammatory facial skin disease usually occurring in middle-aged patients. It manifests itself as an inflammatory condition with perivascular infiltrate, dilated blood vessels, lymphoedema, hyperplasia of sebaceous glands, and disorders of connective tissue structures brought on by fibrosis. Rosacea is characterized by multifactorial inflammatory mechanisms, and therefore it requires an interdisciplinary approach including adequate skin care, topical and/or systemic therapy, and physical modalities to successfully treat the various symptoms and disease subtypes. However, data regarding the possible role of cosmetologists in rosacea remains scanty and equivocal. The objectives of cosmetology therapy include restoration and regeneration, anti-inflammatory effects, the strengthening of blood vessels and regulation of their permeability, and the regulation of keratinization. Vascular abnormalities can be targeted with specific light and laser devices. Therefore, the present paper aims to review the latest advances and summarize different aspects concerning skin care in rosacea. Particular attention has been paid to the co-operation of cosmetologists with other specialists in order to bring about the interdisciplinary management of rosacea. It is also important to keep in mind that it is usually necessary to combine various methods of treatment, as this approach is more effective than monotherapy for attaining satisfactory cosmetic results in rosacea patients.
Keywords: erythema, telangiectases, skin care, therapy, patient, cosmetologist
Introduction
Rosacea is a chronic skin disease usually occurring only in the facial area. Clinically, it manifests itself with an erythema, telangiectasias, and papules and pustules, while histopathologically – it is an inflammatory condition with a perivascular infiltrate, dilated blood vessels, lymphoedema, hyperplasia of sebaceous glands, and disorders of connective tissue structures brought on by fibrosis.1 Vascular lesions appear in the central part of the face and gradually spread circumferentially, occasionally spreading to the skin of the neck and decolletage.2 The typical location of the lesions, the accompanying inflammatory condition of the skin and the sensation of warmth and burning cause not only physical, but also mental discomfort to the patients, resulting in the lowering of their self-esteem.3 Rosacea is usually diagnosed in adults aged 45–60.2 It develops on the vascular skin, and the stage of prerosacea, which occurs in teenagers and young adults, precedes the appearance of the typical symptoms of the disease at the later stage of life.4 Vascular skin may affect both women and men, and according to the Fitzpatrick scale, usually with skin phototypes I and II.2
Pathological changes of rosacea occurring predominantly in the facial region are particularly exposed, often considered unesthetic not only by the patients themselves but also by others in their environment. It should be emphasized that the main reason for cosmetologic consultations in the event of rosacea is the aesthetic defect that causes stigmatization of patients followed by not so infrequent their social rejection. The facial and other changes that appear because of the disease may significantly affect the patients’ quality of life, self-esteem, and their mental health.5,6
Cosmetology has come to function as an essential complementary element of the treatment of diagnosed rosacea. Therefore, the cosmetic aspect of the therapy, based on the restoration of social confidence and self-esteem, may seem to function as a link between the physical beauty and the mental health of rosacea patients. Through this impact, cosmetology becomes an essential factor in the overall therapeutic process.
Methods
We conducted a review of the literature to provide an overview of the recent data concerning the role of cosmetology in rosacea treatment. The results are presented in the form of a topical review. Searches were conducted of the following databases: PubMed and the Google Scholar. Multiple search terms were used, including “skincare”, “cosmetics”, “rosacea” and “cosmetology”. Only English language papers published in peer-reviewed journals and book chapters have been included. Previously abstracts were read to assess their relevance. Then this method was used, 95 papers were identified and duly accessed. Each was subsequently read and analysed. This led to the identification of further relevant references, and further 68 relevant papers had been included in this paper.
Characteristics of Rosacea
Rosacea – Aetiopathogenesis and Epidemiology
The cause of the disease is not completely understood. What is known though is that occurrence is influenced by both the endogenous and exogenous factors, while polymorphic skin lesions reflect the multifactorial background of rosacea.1
A positive family history points to genetic predispositions. The study by Lynn et al7 demonstrated a single nucleotide polymorphism (SNP) in the genes encoding butyrophilin-like protein 2 (BTNL 2) and in the human leucocyte antigen (HLA-DRA) gene. It is probable that three specific HLA alleles, proteins of the major histocompatibility complex (MHC) class II, ie, HLA-DRB1*03:01, HLA-DQB1*02:01 and HLA-DQA1*05:01, are significantly associated with rosacea,7 which points to the role of the dysregulation of the immunological system in the pathogenesis of the disease.1
The imbalances of the cutaneous microbiome are implicated in the pathogenesis of rosacea,8,9 whereby several microorganisms (Demodex folliculorum, Bacillus oleronius, Staphylococcus epidermidis, and Cutibacterium acnes) were postulated to have been used to as a key players.
Demodex folliculorum (D. folliculorum) mites are widespread on the skin of healthy people, however an excessive colonization of this microorganism plays a role in the pathogenesis of rosacea. A diagnosis of demodicosis in the presence of clinical symptoms, such as flushing, pruritus and a burning sensation of the skin, and also lacrimation and dryness of the conjunctiva accompanied by eyelid desquamation, is confirmed by microscopic examinations and the observation of more than 5 specimens/cm2.10 Long-term enzymatic processes and burrowing into the skin by Demodex mites may lead to perifollicular inflammation. By releasing the products of their decomposition and leaving chitinous exoskeletons on the surface of human skin, dying mites trigger an immune response by influencing the secretion of inflammatory cytokines, such as interleukin (IL) 8, and tumour necrosis factor-alpha (TNF-alpha), and the expression of the Toll-like receptor (TLR) by interacting with cells from the pilosebaceous unit.11 Clinical examinations have demonstrated an increased number of D. folliculorum on the skin of patients with rosacea in comparison with healthy individuals, and those with acne and seborrhoeic dermatitis.11
Once Demodex die, internal microbes including Bacillus oleronius (B. oleronius), and toxins are released within the sebaceous glands of the face and eyelashes.12,13 B. oleronius triggers inflammatory pathways by producing antigenic proteins that potentially play a role in rosacea.8 The two antigenic proteins from B. oleronius, sized 62kDa and 83kDa, have been found to react with the sera of rosacea patients.
It should be noted that microbiological changes do not occur on the skin only. Potential cutaneous effects of alterations have also been found in the gastrointestinal microbiome. It is therefore suggested that Helicobacter pylori (HP) infection may significantly influence the condition of rosacea skin. The data collected so far, however, are not homogenous, and sometimes even contradictory,14–16 which renders their interpretation difficult. HP infection may cause inflammation and redness of the skin by releasing angiogenic and vasomotor agents, and there are studies with evidence that these bacteria increase concentrations of nitrous oxide, thereby leading to the dilation of blood vessels.17,18
Classification of Rosacea
Four clinical subtypes of the disease have been distinguished: erythematotelangiectatic rosacea (ETR), papulopustular rosacea (PPR), phymatous rosacea (PhR), and ocular rosacea.19,20 ETR is characterized by an erythema that covers the central part of the face, and by the evolution of lesions from a transient redness of the skin and single telangiectasias (prerosacea) to the full-blown form. Patients often complain of symptoms of skin hypersensitivity and intolerance to cosmetics. PPR is also referred to as “classic rosacea”, with papules and pustules dominant in its course, and sometimes accompanied by a delicate desquamation of the epidermis and thickening of the skin due to swelling. Inflammatory lesions are usually accompanied by dryness and a burning sensation of the skin. Chronic inflammatory lesions may lead to the development of solid facial oedema and hypertrophic lesions, referred to as phymatous rosacea. This rare manifestation of the disease can affect various parts of the face, and thus, depending on the location, we distinguish skin lesions of the nose (rhinophyma), chin (gnatophyma) and eyelids (blepharophyma). In the main, it affects Caucasian males aged over 40. It is characterized by hyperplasia and thickening of the skin, which becomes livid red in colour, with clearly marked, dilated sebaceous glands, increased fibrosis and the presence of nodular lesions. Ocular rosacea affects the eyes and eyelids.20 The symptoms are not very specific, including photophobia, blurred vision, pain, swelling, fatigability of the eyelids, dryness of the eyes, foreign body sensation, burning and pruritus.20,21
The classification of rosacea had been updated based on new insight into the pathophysiology of the disease.20,21 Persistent centrofacial erythema and phymatous changes have been recognised as the diagnostic phenotype of rosacea. Major phenotypes include: flushing, papules and pustules, telangiectasia, ocular manifestations such as lid margin telangiectasia, interpalpebral conjunctival injection, spade-shaped infiltrates in the cornea, scleritis, and sclerokeratitis. Meeting two or more of these criteria may be considered diagnostic. Secondary signs and symptoms, such as a burning and/or stinging sensation of the skin, skin dryness, oedema and ocular manifestations (“honey crust” and collarette accumulation at the base of the lashes, irregularity of the lid margin, evaporative tear dysfunction), may appear with one or more diagnostic or major phenotypes.21
Various clinical types of rosacea are presented in Figure 1.
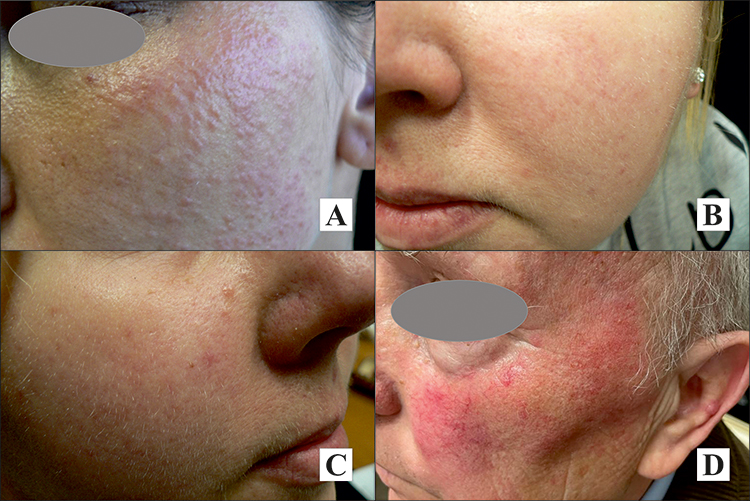 |
Figure 1 Clinical presentation of various clinical type of rosacea: (A) papules, (B) papules and telangiectases, (C) erythema and telangiectases, (D) erythema, telangiectases, and papules. Property of the author. |
Rosacea as an Interdisciplinary Problem
Rosacea is characterized by multifactorial, inflammatory mechanisms, therefore it requires an interdisciplinary approach including adequate skin care, topical and systemic pharmacotherapy, and physical modalities to successfully treat the various symptoms and disease subtypes.19–21
The association of gastrointestinal and neuropsychiatric disorders supports the concept of a gut-brain-skin interaction in rosacea.
The association with the gut-brain axis has also been established via multiple parallel pathways between them, including the autonomic nervous system and the pituitary-hypothalamus-adrenal axis.22,23 A schematic view of possible factors belonging to this axis and contributing to the molecular mechanisms of rosacea is presented in Figure 2.
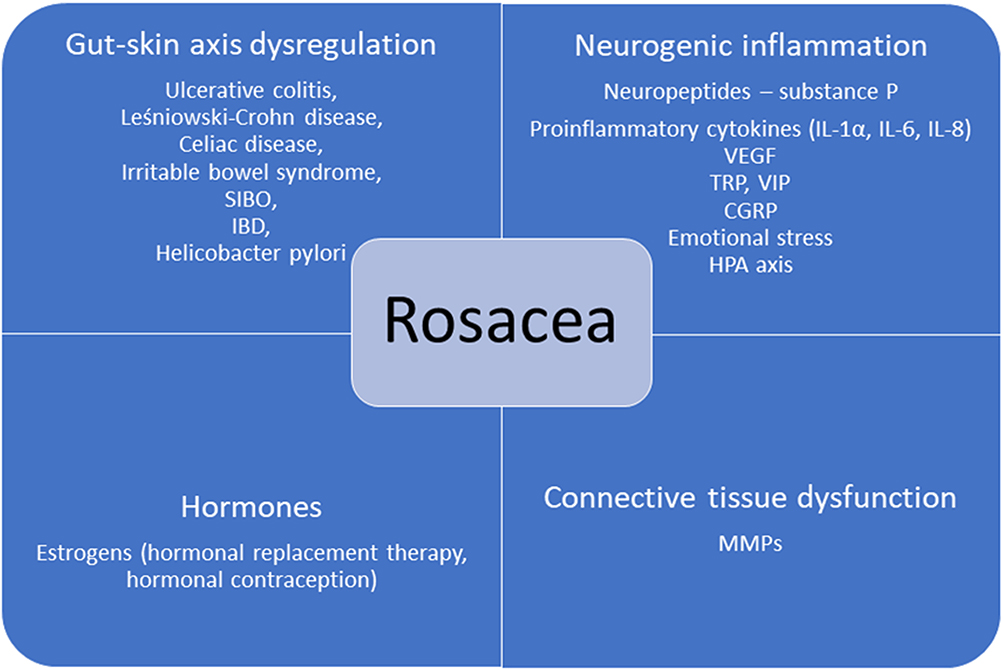 |
Figure 2 Schematic view of possible factors belonging to the gut-brain-skin axis and contributing to the molecular mechanisms of rosacea. Property of the author. |
The Role of the Gut-Skin Axis
The gut-skin axis plays an important role in the pathophysiology of rosacea, with diseases from the inflammatory bowel diseases (IBD) group having been identified as the most significant. The high risk of occurrence of IBD disorders and rosacea is most probably due to the genetic factors.14,24 Numerous studies have revealed the relationship between rosacea and SIBO (small intestinal bacterial overgrowth),25–28 and it has been postulated that SIBO-positive patients are more often representative of the papulopustular type of rosacea.25 It has been demonstrated that diarrhoea chylosa, too, causes a disturbance of the gut-skin axis and impacts the course of the disease.14,29 Altered gastrointestinal and skin microbiome of patients with rosacea may also play a role in the etiopathogenesis.1
Neurogenic Inflammatory Factors
Sunlight, changes in temperature, spicy food, alcohol and physical activity are all triggers for erythema, for these stimuli can activate sensory nerve endings in the skin, resulting in the emergence of inflammation. Keratinocytes stimulated by neuropeptides release pro-inflammatory cytokines, ie, IL-1α, IL-6 and IL-8.30 Another neuropeptide, substance P (SP), affects the Langerhans cells, intensifying their migration and bringing about the mast cell degranulation and increased histamine activity, which has a vasodilating effect. SP also induces the release of the vascular endothelial growth factor (VEGF) from mast cells, which, by increasing the vascularization and proliferation of endothelial cells, contributes to the worsening of the inflammatory condition and erythema.30 The skin of patients with rosacea shows a greater density of sensory neurons involved in the release of neuropeptides. An important role (the sensation of heat, nociception, activation by capsaicin) is also played by transient receptor potential (TRP) cation channels, which are present, among others, at sensory nerve endings.30 Stimulated TRP channels release SP and the calcitonin gene-related peptide (CGRP), which has a strong vasodilating effect, affecting the smooth muscle cells of arterioles.31 Rosacea is also characterized by an increased secretion of vasoactive intestinal peptide (VIP), which is able to stimulate the degranulation of mast cells, leading to the increased secretion of histamine and the dilation of blood vessels.31 The mechanism of neurogenic inflammation explains the impact of triggers on the skin, primarily due to its ultimate vasodilating and pro-inflammatory action through neuropeptides.
Disorders of the Connective Tissue Structure and the Process of Fibrosis
Studies have shown a significantly increased expression of extracellular matrix metalloproteinase (MMP), mainly MMP-9, in skin with rosacea (granulomatous subtype),32 which leads to the damage of the collagen and elastin fibres within the extracellular matrix and to fibrosis.33 It has also been documented that elastin fibres are thicker and more amorphous than tissue samples from the control group.32 This leads to skin remodelling and an increased influx of inflammatory cells.32,33
The Impact of Hormones on Vascular Endothelium
Oestrogens intensify the release of nitric oxide, which is responsible for the dilation of blood vessels that negatively affects the condition of vascular skin. Vasodilation is a feature of the skin ageing process, observed in particular in post-menopausal women.34 The risk of rosacea increases for women taking menopausal hormone therapy and hormonal contraception.35
Opportunities for Co-Operation Between Cosmetologists and Other Specialists
Rosacea is a dermatosis that is difficult to treat and frequently originates from systemic disorders. Therefore it requires close co-operation between dermatologists, cosmetologists, other physicians of different specialties, and dieticians. There are also specific products that will negatively affect the condition of the skin by causing paroxysmal flushing, namely, alcohol, hot foods and beverages, spicy dishes (especially those rich in capsaicin), and cinnamon.36
The selection of pharmacological and instrumental treatment depends on the phenotype of the disease.37 To date, it has been impossible to cure the disease completely, however properly selected topical and systemic pharmacotherapy, the use of instrumental methods, appropriate skin care and a change of lifestyle may all help to control it.
Therapy for Rosacea
The therapy depends on the phenotype of the disease and the topical as well as systemic medications are used. The most common topical medications include: alpha-adrenergic brimonidine gel, 0.33%, oxymetazoline hydrochloride cream, 1%, an alpha1A-adrenoceptor agonist, Ivermectin, azelaic acid, metronidazole, and retinoids.37,38 The beneficial impact of dermal injections of botulinum toxin has also been described.39
Doxycycline (subantimicrobial), Doxycycline, Minocycline, Tetracycline, Azithromycin, Trimethoprim/Sulfamethoxazole, Clindamycin and Isotretinoin – as well as Carvedilol, Clonidine and Propranolol – are applied orally.37
The action of individual light devices is presented in Table 1.
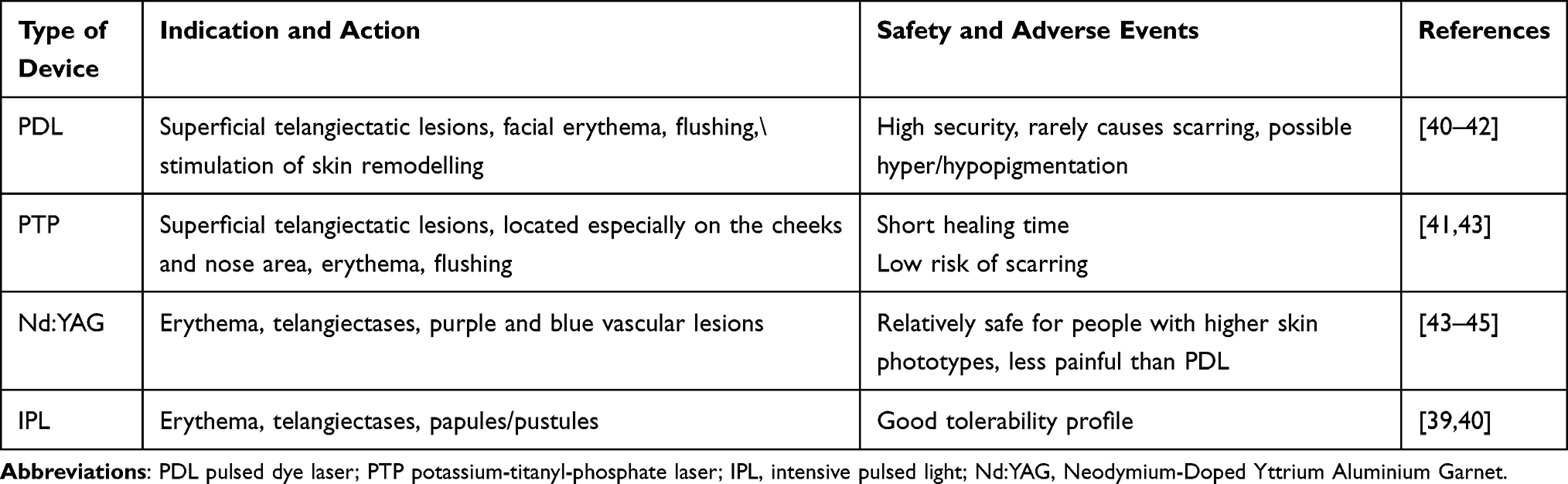 |
Table 1 Indications and Safety of Light Devices Used for the Treatment of Rosacea |
Rosacea therapy uses lasers for which haemoglobin and oxyhaemoglobin are the target chromophore. The energy absorbed by the target chromophore is converted into heat, which brings about the coagulation of blood vessels walls and their closure. PDL with a wavelength of 585/595 nm is considered as the “gold standard” in rosacea therapy due to its high efficacy and long-lasting effects, coupled with a good safety profile.41,42 The PTP laser with a wavelength of 532 nm is used less frequently due to shallow beam penetration. Neodymium-Doped Yttrium Aluminium Garnet (Nd:YAG) is used in the treatment of purple and blue vascular lesions. A Q-switched 595-nm Nd:YAG laser with low non-purpuragenic fluence proved to be safe and effective in treating early-stage erythematotelangiectatic lesions.45 It is less effective, however, in treating diffuse erythema.41–45 Carbon dioxide and erbium are used to remove phymas.40,45
Skin Care and Cosmetological Procedures in Rosacea
When deciding upon a most relevant cosmetological support for the treatment of rosacea, it is vital to take into account the clinical stage of the disease and a given patient’s expectations. A holistic therapeutic approach should always be determined on a case-by-case basis.
The objectives of cosmetology therapy are presented diagrammatically in Figure 3.
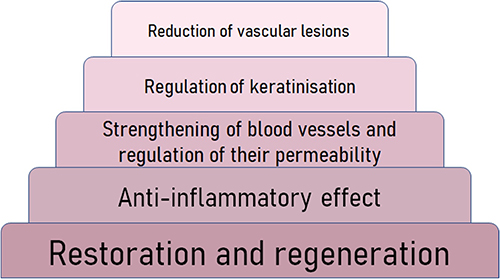 |
Figure 3 Pyramid of cosmetological effects on rosacea skin. Property of the author. |
Because of the damaged hydrolipid barrier, rosacea skin is usually dry, rarely seborrhoeic, and the epidermal hydration levels are uniformly low.46
Due to the strong reactivity of the skin to temperature changes, it is advisable to avoid warming products, lipid winter creams and algae masks that strengthen the skin barrier. Thus, hydrophilic formulations such as hydrogels, O/W creams with a low lipid content and lamellar products are preferred. Waterproof make-up cosmetics, the removal of which entails more intensive rubbing, should be avoided.47
Basic Principles for Rosacea Skin Care and Hygiene
Proper skin care can significantly improve the effects of pharmacotherapy and reduce subjective symptoms, such as pruritus, burning, and tightening of the skin.
The skin of persons suffering from rosacea is highly reactive and easily irritated, which forces the use of mild washing emulsions with a slightly acidic pH. Water temperature is also important – it should be lukewarm, so as not to additionally irritate the skin with another physical factor and not to cause vascular reactions.47 Mechanical peeling agents should be abandoned in favour of enzymatic peelings or delicate peelings based on polyhydroxy acids.48 It is advisable to use care products which are free from alcohol, essential oils, waxes and mineral oils. Men should also give up alcohol-based after-shaves due to the irritating effect of menthol.47 The impact of temperature changes on the condition of rosacea skin in winter may be to a certain extent mitigated by the use of cold creams.
It is recommended to gently remove make-up with the hands, using oil products containing emulsifiers49 so as not to remove lipids from the corneal layer of the epidermis and reduce the sensation of “skin tightening”.49,50
The composition and properties of skin care products applied in the treatment of rosacea must be properly adapted to the needs of the affected skin. The use in cosmetics of active substances – which have primarily a skin-calming, anti-inflammatory, or vessel-stabilizing effect – is of limited importance in rosacea. Moisturizing and regenerating cosmetics should be light preparations and rich in anti-inflammatory substances, for example, Centella asiatica extract. It is important that they additionally contain compounds which help restore the skin’s lipid barrier. Ingredients occurring naturally in the intercellular cement and their derivatives – ceramides, fatty acids and sterols – will work well.51 If the skin is irritated and strongly reactive, active ingredients should not be used specifically for vascular lesions. First of all, it will be necessary to strengthen the hydrolipid barrier. It is not recommended to apply cosmetic preparations that increase flow through skin blood vessels or those with an anti-ageing effect.47
Despite the presence of papules and pustules, active products should not contain ingredients typically used in acne skin therapy or stem cells. The desired ingredients include kinetin, retinaldehyde, Licochalcon A, tranexamic acid, azelaic acid and extracts from plants rich in polyphenols, eg red clover herb extract or Chinese tea leaf extract.47,52–58 Cosmetics should utilise natural raw materials with anti-inflammatory, soothing, moisturizing, antioxidant, radiation protective and blood vessel sealing properties. These make it possible to enhance therapeutic effects or prevent undesirable effects.
The topical use of vitamins and antioxidants in cosmetics can protect and correct skin damage in rosacea. It has been documented,59 that topical vitamin K provides rapid improvement in the flushing, non-transient erythema, telangiectasia, burning and dryness with mild and tolerable side effects. Vitamin PP presents a multidirectional action on cosmetics: (i) inhibition of histamine secretion associated with the intensification of erythema, (ii) reduction of inflammatory processes, (iii) an anti-swelling effect.6 Moreover, some antioxidant agents, such as topical vitamin C or vitamin E, are already used in skin care products. Vitamin C has been shown to repair and replenish barrier function in rosacea-prone skin.1
Raw materials proven to locally alleviate the symptoms of rosacea have been presented in Table 2.
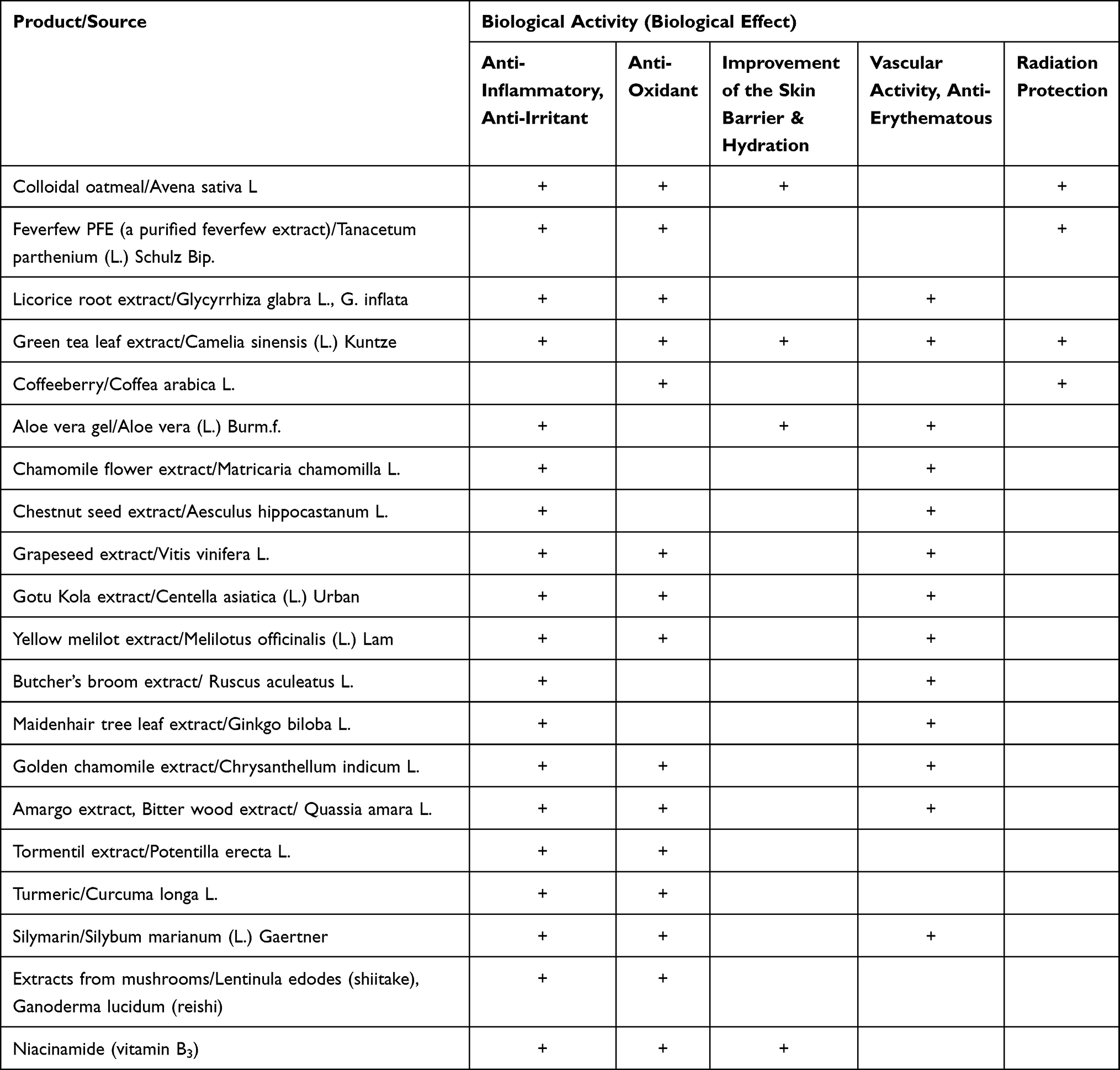 |
Table 2 Effects of Selected Natural Raw Materials Used in the Treatment of Rosacea56–58,60–62 |
The skin of patients with rosacea is very sensitive to solar radiation, which is one of the environmental factors inducing and exacerbating skin lesions.47 Protection against the sun should be based primarily on the avoidance of exposure. The daily use of photoprotective products with an SPF≥30 and their reapplication every two hours is a fundamental element of care. Reinholz et al62 recommend that these should be formulations containing physical filters, that is, zinc oxide or titanium dioxide, however there are no studies comparing the tolerance of different filters in individuals affected with rosacea.47 A study by Cole et al63 invalidated the established belief that a majority of physical filters reflect light, and thereby allegedly do not cause the skin to warm up. Zinc oxide and titanium oxide act primarily as ultraviolet (UV) absorbers. Achieving adequate protection against UVA and UVB rays by using physical filters alone carries with it the risk of skin whitening. Thus, it is the skin’s reaction to specific filters that should be the decisive indicator of whether or not a product is suitable.
Masks, which soothe and calm skin redness, are an excellent ad hoc alleviating solution. Anti-redness masks usually have the form of gels and contain ingredients which reduce skin reactivity, and have a moisturizing and refreshing effect. It is recommended to select dermocosmetics that are intended for rosacea and therefore have a lower allergenic potential.62,63
Make-Up
For most patients, and especially those with self-perceived severe erythema and no inflammatory lesions, the erythema associated with rosacea brings with it a significant decrease in the health-related quality of life, and should therefore be treated as an important medical problem requiring medical intervention.64 Make-up can help immediately cover skin imperfections and improve one’s self-evaluation, however it should not aggravate the underlying dermatosis. It should therefore be considered as a useful adjuvant, the advantage of which is its immediate effectiveness in the absence of significant adverse effects.65–67 Skin redness can be camouflaged with care creams or light green or yellow coloured make-up. The base of these products should be adapted to the condition of the skin and must be free of mineral oils, fragrances and preservatives. Coloured skin care products or make-up should be applied at least 10 minutes after the administration of topical medications.47,65,67 High-coverage products are less suitable for use in rosacea due to their content of pigments, fats and waxes.47
A multicentre retrospective study concerning daily care showed that the use of traditional make-up (more than 6 times a week) and the excessive use of facial cleansers (twice or more times daily) were closely correlated with the development of rosacea.67 If make-up is necessary, a simple medical make-up with mineral products should be recommended in order to minimize the risk of developing rosacea.63 Mineral make-up provides excellent coverage and is easy to use, protects against UV radiation, and is non-comedogenic and anti-inflammatory. It is presently considered that mineral make-up should be free of talc and consist mainly of a combination of titanium dioxide (TiO2), zinc oxide (ZnO), iron oxides, mica, bismuth oxychloride (BiOCl), or boron nitride (BN) Mineral powders require the skin to be clean and prepared with a moisturizing cream, and thus it is necessary to wait until the cream is fully absorbed before their application.68 The personal skincare procedures recommended in rosacea are presented in Table 3.
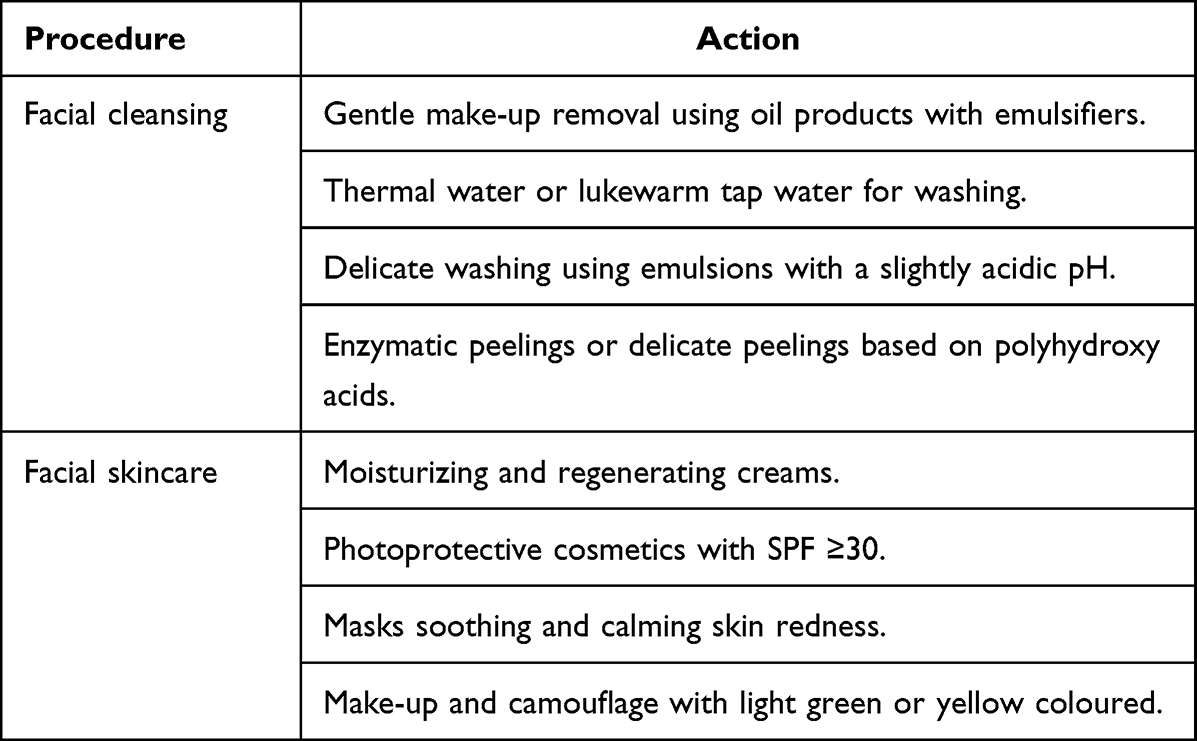 |
Table 3 Most Commonly Recommended Cosmetic Procedures in the Treatment of Rosacea |
Conclusion
The role of a cosmetological procedure may be seen as an essential complement to the treatment of rosacea. The implementation of an appropriate treatment and proper skincare brings about positive outcomes and improves the rosacea patients’ quality of life. What should be remembered though is that usually a combination of various treatments rather than monotherapy is more effective and leads to satisfactory results. Combining pharmacological and cosmetic procedures successfully - requires, however, an individual approach to every patient whose particular needs should be fostered as best as possible. This is more likely to be achieved when the cosmetological treatment proposed is consulted with a dermatologist.
Abbreviations
BTNL 2, Butyrophilin-Like Protein 2; CGRP, calcitonin gene-related peptide; ETR, erythematotelangiectatic rosacea; FDA, Food and Drug Administration; HLA-DRA, Major Histocompatibility Complex, Class II, DR Alpha; HP, Helicobacter pylori; IBD, inflammatory bowel disease; IL, interleukin; IPL, intensive pulsed light; KTP, potassium-titanyl-phosphate laser; MMP, matrix metalloproteinase; ND:YAG, Neodymium-Doped Yttrium Aluminium Garnet; PDL, pulsed dye laser; PHA, polyhydroxy acids; PhR, phymatous rosacea; PPR, papulopustular rosacea; PTP, potassium titanyl phosphate; SIBO, small intestinal bacterial overgrowth; SNP, single nucleotide polymorphism; SP, substance P; TLR, Toll-like receptor; TNF-alpha, tumor necrosis factor-alpha; TRP, transient receptor potential cation; UV, ultraviolet; VEGF, vascular endothelial growth factor; VIP, vasoactive intestinal peptide.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marson JW, Baldwin HE. Rosacea: a wholistic review and update from pathogenesis to diagnosis and therapy. Int J Dermatol. 2020;59(6):e175–e182. doi:10.1111/ijd.14757
2. Clanner-Engelshofen BM, Bernhard D, Dargatz S, et al. S2k guideline: rosacea. J Dtsch Dermatol Ges. 2022;20:1147–1165. doi:10.1111/ddg.14849
3. van Zuuren EJ, Arents BWM, van der Linden MMD, et al. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22(4):457–465. doi:10.1007/s40257-021-00595-7
4. Vemuri RC, Gundamaraju R, Sekaran SD, Manikam R. Major pathophysiological correlations of rosacea: a complete clinical appraisal. Int J Med Sci. 2015;12(5):387–396. doi:10.7150/ijms.10608
5. Yang F, Zhang Q, Song D, Liu X, Wang L, Jiang X. A cross-sectional study on the relationship between rosacea severity and quality of life or psychological state. Clin Cosmet Investig Dermatol. 2022;15:2807–2816. doi:10.2147/CCID.S390921
6. Nowicka D, Chilicka K, Dzieńdziora-Urbińska I, Szyguła R. Skincare in rosacea from the cosmetologist’s perspective: a narrative review. J Clin Med. 2022;12(1):115. doi:10.3390/jcm12010115
7. Lynn A, Chang S, Raber I, et al. Assessment of the genetic basis of rosacea by genome-wide association study. J Invest Dermatol. 2015;135(6):1548–1555. doi:10.1038/jid.2015.53
8. Daou H, Paradiso M, Hennessy K, Seminario-Vidal L. Rosacea and the microbiome: a systematic review. Dermatol Ther. 2021;11(1):1–12. doi:10.1007/s13555-020-00460-1
9. Hu XM, Li ZX, Zhang DY, et al. Current research and clinical trends in rosacea pathogenesis. Heliyon. 2022;8(10):e10874. doi:10.1016/j.heliyon.2022.e10874
10. Forton F, Seys B. Density of Demodex folliculorum in rosacea: a case control study using standardized skin surface biopsy. Br J Dermatol. 1993;128(6):650–659. doi:10.1111/j.1365-2133.1993.tb00261.x
11. Aktaş Karabay E, Aksu Çerman A. Demodex folliculorum infestations in common facial dermatoses: acne vulgaris, rosacea, seborrheic dermatitis. An Bras Dermatol. 2020;95(2):187–193. doi:10.1016/j.abd.2019.08.023
12. Jarmuda S, McMahon F, Żaba R, et al. Correlation between serum reactivity to Demodex-associated Bacillus oleronius proteins, and altered sebum levels and Demodex populations in erythematotelangiectatic rosacea patients. J Med Microbiol. 2014;63(Pt 2):258–262. doi:10.1099/jmm.0.065136-0
13. Szkaradkiewicz A, Chudzicka-Strugała I, Karpiński TM, et al. Bacillus oleronius and Demodex mite infestation in patients with chronic blepharitis. Clin Microbiol Infect. 2012;18(10):1020–1025. doi:10.1111/j.1469-0691.2011.03704.x
14. Egeberg A, Weinstock LB, Thyssen EP, Gislason GH, Thyssen JP. Rosacea and gastrointestinal disorders: a population-based cohort study. Br J Dermatol. 2017;176:100–106. doi:10.1111/bjd.14930
15. Szlachcic A. The link between Helicobacter pylori infection and rosacea. J Eur Acad Dermatol Venereol. 2002;16(4):328–333. doi:10.1046/j.1468-3083.2002.00497.x
16. Sharma VK, Lynn A, Kaminski M, Vasudeva R, Howden CW. A study of the prevalence of Helicobacter pylori infection and other markers of upper gastrointestinal tract disease in patients with rosacea. Am J Gastroenterol. 1998;93(2):220–222. doi:10.1111/j.1572-0241.1998.00220.x
17. Jørgensen AR, Egeberg A, Gideonsson R, Weinstock LB, Thyssen EP, Thyssen JP. Rosacea is associated with Helicobacter pylori: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol. 2017;31:2010–2015. doi:10.1111/jdv.14352
18. Bonamigo RR, Leite CS, Wagner M, Bakos L. Rosacea and Helicobacter pylori: interference of systemic antibiotics in the study of possible association. J Eur Acad Dermatol Venereol. 2000;14(5):424–425. doi:10.1046/j.1468-3083.2000.00090-3.x
19. Gallo RL, Granstein RD, Kang S, et al. Standard classification and pathophysiology of rosacea: the 2017 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2018;78:148–155. doi:10.1016/j.jaad.2017.08.037
20. Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182(5):1269–1276. doi:10.1111/bjd.18420
21. Tan J, Berg M, Gallo RL, Del Rosso JQ. Applying the phenotype approach for rosacea to practice and research. Br J Dermatol. 2018;179(3):741–746. doi:10.1111/bjd.16815
22. Woo YR, Han YJ, Kim HS, Cho SH, Lee JD. Updates on the risk of neuropsychiatric and gastrointestinal comorbidities in rosacea and its possible relationship with the Gut–Brain–Skin Axis. Int J Mol Sci. 2020;21(22):8427. doi:10.3390/ijms21228427
23. Wang FY, Chi CC. Rosacea, germs, and bowels: a review on gastrointestinal comorbidities and Gut–Skin Axis of rosacea. Adv Ther. 2021;38:1415–1424. doi:10.1007/s12325-021-01624-x
24. Pathan S, Gowdy RE, Cooney R, et al. Confirmation of the novel association at the BTNL2 locus with ulcerative colitis. Tissue Antigens. 2009;74(4):322–329. doi:10.1111/j.1399-0039.2009.01314.x
25. Drago F, De Col E, Agnoletti AF, et al. The role of small intestinal bacterial overgrowth in rosacea: a 3-year follow-up. J Am Acad Dermatol. 2016;75:113–115. doi:10.1016/j.jaad.2016.01.059
26. Parodi A, Paolino S, Greco A, et al. Small intestinal bacterial overgrowth in rosacea: clinical effectiveness of its eradication. Clin Gastroenterol Hepatol. 2008;6:759–764. doi:10.1016/j.cgh.2008.02.054
27. Salem I, Ramser A, Isham N, Ghannoum MA. The gut microbiome as a major regulator of the Gut-Skin Axis. Front Microbiol. 2018;9:1459. doi:10.3389/fmicb.2018.01459
28. Weinstock LB, Steinhoff M. Rosacea and small intestinal bacterial overgrowth: prevalence and response to rifaximin. J Am Acad Dermatol. 2013;68:875–876. doi:10.1016/j.jaad.2012.11.038
29. Egeberg A, Hansen PR, Gislason GH, Thyssen JP. Clustering of autoimmune diseases in patients with rosacea. J Am Acad Dermatol. 2016;74(4):667–672. doi:10.1016/j.jaad.2015.11.004
30. Choi JE, Di Nardo A. Skin neurogenic inflammation. Semin Immunopathol. 2018;40:249–259. doi:10.1007/s00281-018-0675-z
31. Schwab V, Sulk M, Seeliger S, et al. Neurovascular and neuroimmune aspects in the pathophysiology of rosacea. J Investig Dermatol Symp Proc. 2011;V15(1):53–62. doi:10.1038/jidsymp.2011.6
32. Jang Y, Sim J, Kang H, Kim Y, Lee E-S. Immunohistochemical expression of matrix metalloproteinases in the granulomatous rosacea compared with the non-granulomatous rosacea. J Eur Acad Dermatol Venereol. 2011;25(5):544–548. doi:10.1111/j.1468-3083.2010.03825.x
33. Ahn CS, Huang WW. Rosacea Pathogenesis. Dermatol Clin. 2018;36(2):81–86. doi:10.1016/j.det.2017.11.001
34. Mendelsohn ME, Karas RH, Epstein FH. The protective effects of estrogen on the cardiovascular system. N Engl J Med. 1999;340(23):1801–1811. doi:10.1056/NEJM199906103402306
35. Wu WH, Geng H, Cho E, et al. Reproductive and hormonal factors and risk of incident rosacea among US White women. J Am Acad Dermatol. 2022;87(1):138–140. doi:10.1016/j.jaad.2021.06.865
36. Weiss E, Katta R. Diet and rosacea: the role of dietary change in the management of rosacea. Dermatol Pract Concept. 2017;7(4):31–37. doi:10.5826/dpc.0704a08
37. Thiboutot D, Anderson R, Cook-Bolden F, et al. Standard management options for rosacea: the 2019 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2020;82(6):1501–1510. doi:10.1016/j.jaad.2020.01.077
38. Wolf JE, Del Rosso JQ. The CLEAR trial: results of a large community-based study of metronidazole gel in rosacea. Cutis. 2007;79(1):73–80.
39. Yuraitis M, Jacob CI. Botulinum toxin for the treatment of facial flushing. Dermatol Surg. 2004;30:102–104. doi:10.1111/j.1524-4725.2004.30017.x
40. Dahan S. Laser and intense pulsed light management of couperose and rosacea. Ann Dermatol Venereol. 2011;138(Suppl 3):219–222. doi:10.1016/S0151-9638(11)70094-1
41. Baskan EB, Belli AA. Evaluation of long-term efficacy, safety, and effect on life quality of pulsed dye laser in rosacea patients. J Cosm Las Ther. 2019;21(4):185–189. doi:10.1080/14764172.2018.1502453
42. Maxwell EL, Ellis DA, Manis H. Acne rosacea: effectiveness of 532 nm laser on the cosmetic appearance of the skin. J Otolaryngol Head Neck Surg. 2010;39(3):292–296.
43. Alam M, Voravutinon N, Warycha M, et al. Comparative effectiveness of nonpurpuragenic 595-nm pulsed dye laser and microsecond 1064-nm neodymium:yttrium-aluminum-garnet laser for treatment of diffuse facial erythema: a double-blind randomized controlled trial. J Am Acad Dermatol. 2013;69(3):438–443. doi:10.1016/j.jaad.2013.04.015
44. Goo BL, Kang JS, Cho SB. Treatment of early-stage erythematotelangiectatic rosacea with a Q-switched 595-nm Nd:YAG laser. J Cosmet Laser Ther. 2015;17(3):139–142. doi:10.3109/14764172.2014.1003239
45. Hofmann MA, Lehmann P. Physical modalities for the treatment of rosacea. J Dtsch Dermatol Ges. 2016;14:38–43.
46. Addor FA. Skin barrier in rosacea. An Bras Dermatol. 2016;91(1):59–63. doi:10.1590/abd1806-4841.20163541
47. Kresken J, Kindl U, Wigger-Alberti W, Clanner-Engelshofen BM, Reinholz M. Dermocosmetics for use in rosacea: guideline of the Society for Dermopharmacy. Skin Pharmacol Physiol. 2018;31:147–154. doi:10.1159/000486688
48. Algiert-Zielińska B, Mucha P, Rotsztejn H. Lactic and lactobionic acids as typically moisturizing compounds. Int J Dermatol. 2019;58(3):374–379. doi:10.1111/ijd.14202
49. Chen W, He M, Xie L, Li L. The optimal cleansing method for the removal of sunscreen: water, cleanser or cleansing oil? J Cosmet Dermatol. 2020;19(1):180–184. doi:10.1111/jocd.12995
50. Li G, Wang B, Zhao Z, et al. Excessive cleansing: an underestimating risk factor of rosacea in Chinese population. Arch Dermatol Res. 2021;313(4):225–234. doi:10.1007/s00403-020-02095-w
51. Jensen JM, Proksch E. The skin’s barrier. G Ital Dermatol Venereol. 2009;144(6):689–700.
52. Elewski BE, Fleischer AB, Pariser DM. A comparison of 15% azelaic acid gel and 0.75% metronidazole gel in the topical treatment of papulopustular rosacea: results of a randomized trial. Arch Dermatol. 2003;139(11):1444–1450. doi:10.1001/archderm.139.11.1444
53. Bageorgou F, Vasalou V, Tzanetakou V, Kontochristopoulos G. The new therapeutic choice of tranexamic acid solution in treatment of erythematotelangiectatic rosacea. J Cosmet Dermatol. 2019;18(2):563–567. doi:10.1111/jocd.12724
54. Domingo DS, Camouse MM, Hsia AH, et al. Anti-angiogenic effects of epigallocatechin-3-gallate in human skin. Int J Clin Exp Pathol. 2010;3(7):705–709.
55. Rigopoulos D, Kalogeromitros D, Gregoriou S, et al. Randomized placebo-controlled trial of a flavonoid-rich plant extract-based cream in the treatment of rosacea. J Eur Acad Dermatol Venereol. 2005;19(5):564–568. doi:10.1111/j.1468-3083.2005.01248.x
56. Działo M, Mierziak J, Korzun U, Preisner M, Szopa J, Kulma A. The potential of plant phenolics in prevention and therapy of skin disorders. Int J Mol Sci. 2016;17(2):160. doi:10.3390/ijms17020160
57. Emer J, Waldorf H, Berson D. Botanicals and anti-inflammatories: natural ingredients for rosacea. Semin Cutan Med Surg. 2011;30(3):148–155. doi:10.1016/j.sder.2011.05.007
58. Gonçalves MMBM, Pina MESRT. Dermocosmetic care for rosacea. Braz J Pharm Sci. 2017;53(4):e00182. doi:10.1590/s2175-97902017000400182
59. Abdullah GA. The effectiveness of topical vitamin K cream 1% in the treatment of steroid-induced rosacea. Res J Pharm and Tech. 2020;13(8):3883–3886. doi:10.5958/0974-360X.2020.00687.3
60. Hoffmann J, Gendrisch F, Schempp SM, Wölfle U. New herbal biomedicines for the topical treatment of dermatological disorders. Biomedicines. 2020;8(2):27. doi:10.3390/biomedicines8020027
61. Fisk WA, Lev-Tov HA, Clark AK, Sivamani RK. Phytochemical and botanical therapies for rosacea: a systematic review. Phytother Res. 2015;29(10):1439–1451. doi:10.1002/ptr.5432
62. Reinholz M, Tietze JK, Kilian K, et al. Rosacea - S1 Guideline. J Dtsch Dermatol Ges. 2013;11(8):768–780. doi:10.1111/ddg.12101
63. Cole C, Shyr T, Ou-Yang H. Metal oxide sunscreens protect skin by absorption, not by reflection or scattering. Photodermatol Photoimmunol Photomed. 2016;32(1):5–10. doi:10.1111/phpp.12214
64. Bewley A, Fowler J, Schöfer H, et al. Erythema of rosacea impairs health-related quality of life: results of a meta-analysis. Dermatol Ther. 2016;6:237–247.
65. Seité S, Deshayes P, Dréno B, et al. Interest of corrective makeup in the management of patients in dermatology. Clin Cosmet Investig Dermatol. 2012;5:123–128. doi:10.2147/CCID.S33172
66. Peuvrel L, Quéreux G, Brocard A, et al. Evaluation of quality of life after a medical corrective make-up lesson in patients with various dermatoses. Dermatology. 2012;224:374–380. doi:10.1159/000339478
67. Huang YX, Li J, Zhao ZX, et al. Effects of skin care habits on the development of rosacea: a multi-center retrospective case-control survey in Chinese population. PLoS One. 2020;15(4):e0231078. doi:10.1371/journal.pone.0231078
68. Iredale J, Linder J. Mineral makeup and its role with acne and rosacea. Cosmet Dermatol. 2009;22(8):407–412.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.