")
Back to Journals » Journal of Blood Medicine » Volume 15
The Role of Direct Oral Anticoagulants in the Treatment of Cancer-Associated Venous Thromboembolism: Review by Middle East and North African Experts
Authors Bazarbashi S , El Zawahry HM, Owaidah T , AlBader MA, Warsi A , Marashi M, Dawoud E, Jaafar H, Sholkamy SM, Haddad F, Cohen AT
Received 22 May 2023
Accepted for publication 1 March 2024
Published 25 April 2024 Volume 2024:15 Pages 171—189
DOI https://doi.org/10.2147/JBM.S411520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Shouki Bazarbashi,1 Heba Mohamed El Zawahry,2 Tarek Owaidah,3 Mohammad A AlBader,4 Ashraf Warsi,5– 7 Mahmoud Marashi,8,9 Emad Dawoud,10 Hassan Jaafar,11 Sherif M Sholkamy,12 Fady Haddad,13 Alexander T Cohen14
1Section of Medical Oncology, Oncology Center, King Faisal Specialist Hospital and Research Center, Alfaisal University, Riyadh, Saudi Arabia; 2Department of Medical Oncology, The National Cancer Institute, Cairo University, Cairo, Egypt; 3Department of Pathology and Laboratory Medicine, King Faisal Specialist Hospital and Research Center, Alfaisal University, Riyadh, Saudi Arabia; 4Hematology Unit, Al Sabah Hospital, South Surra, Kuwait; 5Department of Adult Hematology, Princess Noorah Oncology Center, King Abdulaziz Medical City, Ministry of National Guard Health Affairs–Western Region, Jeddah, Saudi Arabia; 6College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Ministry of National Guard Health Affairs–Western Region, Jeddah, Saudi Arabia; 7King Abdullah International Medical Research Center, Ministry of National Guard Health Affairs-Western Region, Jeddah, Saudi Arabia; 8Hematology Department, Dubai Hospital, Dubai, United Arab Emirates; 9Department of Hematology, Mediclinic City Hospital, Dubai, United Arab Emirates; 10Department of Oncology, Tawam Hospital, Al Ain, United Arab Emirates; 11Department of Oncology, Sheikh Khalifa Specialty Hospital, Ras Al-Khaimah, United Arab Emirates; 12Department of Vascular Surgery, Ain Shams University, Cairo, Egypt; 13Vascular and Endovascular Surgery, American University of Beirut Medical Center, Beirut, Lebanon; 14Department of Haematological Medicine, Guy’s and St Thomas’ Hospitals NHS Foundation Trust, King’s College London, London, UK
Correspondence: Shouki Bazarbashi, Section of Medical Oncology, Oncology Center, King Faisal Specialist Hospital and Research Center, Alfaisal University, 1 Alzahrawi Street, Riyadh, 11211, Saudi Arabia, Tel +966 505443546, Email [email protected]
Abstract: Venous thromboembolism is a leading cause of morbidity and mortality in patients with active cancer who require anticoagulation treatment. Choice of anticoagulant is based on careful balancing of the risks and benefits of available classes of treatment: vitamin K antagonists, low-molecular-weight heparin (LMWH), and direct oral anticoagulants (DOACs). Results from randomized controlled trials have shown the consistent efficacy of DOACs versus LMWH in the treatment of cancer-associated venous thromboembolism (VTE). However, increased major gastrointestinal bleeding was observed for edoxaban and rivaroxaban, but not apixaban, compared with LMWH dalteparin. Most guidelines recommend DOACs for the treatment of cancer-associated VTE in patients without gastrointestinal or genitourinary cancer, and with considerations for renal impairment and drug–drug interactions. These updates represent a major paradigm shift for clinicians in the Middle East and North Africa. The decision to prescribe a DOAC for a patient with cancer is not always straightforward, particularly in challenging subgroups of patients with an increased risk of bleeding. In patients with gastrointestinal malignancies who are at high risk of major gastrointestinal bleeds, apixaban may be the preferred DOAC; however, caution should be exercised if patients have upper or unresected lower gastrointestinal tumors. In patients with gastrointestinal malignancies and upper or unresected lower gastrointestinal tumors, LMWH may be preferred. Vitamin K antagonists should be used only when DOACs and LMWH are unavailable or unsuitable. In this review, we discuss the overall evidence for DOACs in the treatment of cancer-associated VTE and provide treatment suggestions for challenging subgroups of patients with cancer associated VTE.
Plain Language Summary: Patients with cancer are at risk of blood clots forming in their veins, which can cause illness and death. To prevent such blood clots, most patients with cancer need anticoagulant therapy. There are three types of anticoagulants available for the treatment of cancer-associated blood clots in a vein, namely, vitamin K antagonists, low-molecular-weight heparin (LMWH), and direct oral anticoagulants (DOACs). Drug trials have shown that DOACs are more effective than LMWH; however, DOACs can have a greater risk of causing major gastrointestinal bleeding. Among DOACs, edoxaban and rivaroxaban are drugs associated with higher rates of gastrointestinal bleeding. Recently updated guidelines for doctors recommend that DOACs be used as the first treatment for patients with cancer at risk of blood clot formation in a vein. For doctors in the Middle East and North Africa, this new approach differs from existing practices. Notably, choosing a treatment also depends on the type of cancer, because gastrointestinal cancers and cancers of the genitals and urinary system have an especially high risk of gastrointestinal bleeding. The choice also depends on the presence of kidney problems, drug–drug interactions, and access to the drugs. Apixaban may be the preferred DOAC in patients with gastrointestinal cancer, but this drug should be used with care in patients with upper or unresected lower gastrointestinal tumors. For patients with upper or unresected lower gastrointestinal tumors, treatment with LMWH may be preferred. Vitamin K antagonists should be used only when DOACs and LMWH are unavailable or unsuitable.
Keywords: anticoagulation, apixaban, cancer, vitamin K antagonist, low-molecular-weight heparin
Introduction
Venous thromboembolism (VTE), which includes deep-vein thrombosis (DVT) and pulmonary embolism (PE), is a well-recognized complication and a leading cause of morbidity and mortality in patients with cancer.1–4 Active malignancy induces a prothrombotic state,5 and the risk of developing VTE, which is approximately 4–9 times as high in cancer patients as in those without cancer, increases with the extent of the malignancy.6–9 Active cancer, which is an independent risk factor for VTE,10 was associated with a very high incidence rate of first VTE (5.8 per 100 person-years) in a large European population–based cohort study.2 This study also showed that the most commonly occurring cancers (prostate, breast, lung, and colon cancers) were responsible for most active cancer-associated VTE.2 In an American population-based cohort study, patients with active cancer had a high cumulative 5-year rate of VTE recurrence (43% compared with 27% in patients with idiopathic VTE and 18% in non-cancer secondary VTE).11 Patients of African descent have been shown to be at greater risk of VTE than European populations. Consequently, incidence of initial and recurrent VTE in patients with cancer in the Middle East and North Africa (MENA) region is expected to be at least as high as that in Western populations, and may increase over time as diagnostic capabilities improve and anticancer therapies advance. This will eventually lead to patients with advanced, metastatic disease living longer with increasing risk of VTE.12–14
The treatment of VTE is particularly challenging in patients with cancer, who have a significantly greater risk of recurrent VTE and bleeding complications during anticoagulant therapy than non-cancer patients.15 Anticoagulation treatment is further complicated by patient- and cancer-related factors that influence VTE and bleeding risk, including age, cancer stage, type of malignancy, and cancer treatment.16,17 The clinical utility of anticoagulation is dependent on the net clinical benefit to individual patients in terms of VTE recurrence and bleeding. Therefore, after an assessment of patient- and cancer-related variables that may affect the efficacy and/or safety of anticoagulation, choice of anticoagulant is based on careful balancing of the risks and benefits of the three available classes of anticoagulation: vitamin K antagonists (VKAs), low-molecular-weight heparin (LMWH) and direct oral anticoagulants (DOACs).17–21
LMWH has historically been the standard of care for the treatment of cancer-associated VTE based on results from the CLOT study.22 The CLOT study reported a statistically significant reduction of 52% in the risk of VTE recurrence after 6 months’ treatment with the LMWH dalteparin versus VKA therapy (warfarin with LMWH bridging therapy), with no significant difference in major bleeding.22 The results of individual randomized controlled trials (RCTs) have not consistently shown an efficacy benefit of LMWH over VKA therapy for the treatment of cancer-associated VTE.22–25 However, meta-analyses of RCTs of VKA therapy versus LMWH had suggested superior efficacy of LMWH with similar safety.17,26,27 Owing to this and also the difficulty of maintaining therapeutic VKA levels in patients with cancer, LMWH has remained the preferred treatment. Despite recommendations for the use of LMWH in patients with cancer-associated VTE, physicians in some MENA regions may have continued to prescribe VKAs for the treatment of cancer-associated VTE because of the higher cost of LMWH and patients’ unease and poor compliance with long-term daily subcutaneous injections.16,19,28,29
Unlike VKAs, DOACs (direct factor Xa inhibitors: apixaban, edoxaban, rivaroxaban; direct thrombin inhibitor: dabigatran) can be orally administered in fixed doses and do not require regular laboratory monitoring of the anticoagulant effect.30 As such, DOACs are standard of care for the treatment of VTE in the general population31 but, until recently, there have been limited high-quality data on the use of DOACs in patients with cancer-associated VTE. Over the past few years, on the basis of convincing results from RCTs of apixaban, edoxaban or rivaroxaban versus the LMWH dalteparin for the treatment of cancer-associated VTE,32–36 these DOACs have been recognized as convenient and effective alternatives to LMWH in patients with cancer, although caution is advised in patients at high risk for bleeding, particularly in patients with gastrointestinal (GI) and genitourinary (GU) malignancies.37–42 The decision to prescribe a DOAC for a patient with cancer is therefore not always a straightforward one, and clinicians from MENA countries may refer to guidelines from international societies such as the American College of Chest Physicians (ACCP) and the European Society of Cardiology (ESC) to inform such decisions. While recent guidelines include recommendations on DOACs for the treatment of cancer-associated VTE,37–42 these recommendations vary according to the availability of RCT evidence at the time of publication, and certain areas lack clinical trial data to inform evidence-based recommendations.43
Here, we review the overall evidence for DOACs in the treatment of cancer-associated VTE and discuss the potential impact of recently published data on evidence-based recommendations. In addition to providing guidance for the use of DOACs for the treatment of cancer-associated VTE based on the most up-to-date evidence, treatment suggestions are made for challenging subgroups of patients with cancer-associated VTE where current clinical trial data to inform evidence-based recommendations may be lacking.
Evidence for DOACs in the Treatment of Cancer-Associated VTE
Although cancer patients only accounted for a small proportion of the study populations, early evidence supporting the use of DOACs in the treatment of cancer-associated VTE was obtained from the pooled subgroup of patients with cancer included in Phase 3 RCTs of DOACs (apixaban, dabigatran, edoxaban or rivaroxaban) versus conventional treatment (heparin followed by VKAs) in the general VTE population.44–49 A meta-analysis of data aggregated from these studies in patients with cancer showed nonsignificant reductions in major and clinically relevant nonmajor (CRNM) bleeding rates and a trend toward reduction of recurrent VTE of approximately 40% with DOACs treatment.50 However, some studies included in this meta-analysis had excluded patients with active cancers for whom treatment with LMWH would be considered more appropriate than with a VKA. Therefore, the study population included in the meta-analysis was unlikely to be representative of the DOAC target cancer patient population.50 The studies’ use of VKAs as the comparator rather than the LMWH standard of care for VTE in cancer patients further limited the relevance of the meta-analysis.
Results from five pivotal RCTs (Hokusai VTE Cancer, SELECT-D, CASTA-DIVA, Caravaggio and ADAM VTE) comparing the safety and efficacy of individual factor Xa inhibitor DOACs with the standard CLOT regimen of dalteparin (200 IU/kg for 1 month, followed by 150 IU/kg) for the treatment of cancer-associated VTE are summarized in Table 1.32–36 The Hokusai VTE Cancer, SELECT-D, Caravaggio and ADAM VTE studies, which enrolled patients with predominantly advanced active cancer and a range of tumor types, showed ≥6 months’ therapy with apixaban, edoxaban or rivaroxaban to be at least as effective as dalteparin in preventing recurrent VTE. The smaller CASTA-DIVA trial, which investigated 3 months’ therapy with rivaroxaban, was unable to demonstrate noninferiority against dalteparin for the prevention of recurrent VTE.36 There was a greater risk of major bleeding, mainly at GI sites, with edoxaban in the Hokusai VTE Cancer study and rivaroxaban in the SELECT-D study,34,35,51 but not with rivaroxaban in CASTA-DIVA35 or apixaban in the Caravaggio and ADAM VTE studies.32,33,36 The PRIORITY trial, which compared the safety and efficacy of DOACs (apixaban or rivaroxaban) and dalteparin in patients with active advanced upper GI, hepatobiliary or pancreatic cancer, has provided further information regarding the use of DOACs in a high-risk patient population.52 In this small RCT (n=90), DOACs increased the risk of clinically relevant bleeding and major bleeding compared with dalteparin, with no improvement in the rate of recurrent VTE.52 Given that there are no known clinically meaningful differences between LMWH preparations,53 use of dalteparin as the comparator LMWH in these RCTs does not detract from the relevance of their findings for MENA countries in which enoxaparin is the most commonly used LMWH. There are currently no published data from RCTs comparing dabigatran with LMWH for the treatment of cancer-associated VTE. A recent unblinded RCT (CANVAS) has compared the efficacy and safety between groups of patients treated with either DOACs (apixaban and rivaroxaban were used in 58.5% and 37.0% of patients, respectively) or LMWHs (enoxaparin and fondaparinux were used in 89.9% and 7.5% of patients, respectively). The DOACs were noninferior to LMWHs, with a 6-month VTE recurrence rate of 6.1% in the DOAC group and 8.8% in the LMWH group (difference, −2.7%; 1-sided 95% CI, −100% to 0.7%). However, noninferiority was not observed in terms of major bleeding (major bleeding events were reported in 5.2% and 5.6% of patients from DOAC and LMWH groups, respectively). A lower proportion of patients experienced severe adverse events in the DOAC group (33.8%) than in the LMWH (35.1%) group. However, death occurred in 21.5% and 18.4% of patients in the DOAC and LMWH groups, respectively. Because enoxaparin is the most commonly used LMWH in MENA countries, results from the CANVAS trial will provide important information for the clinicians in MENA.54
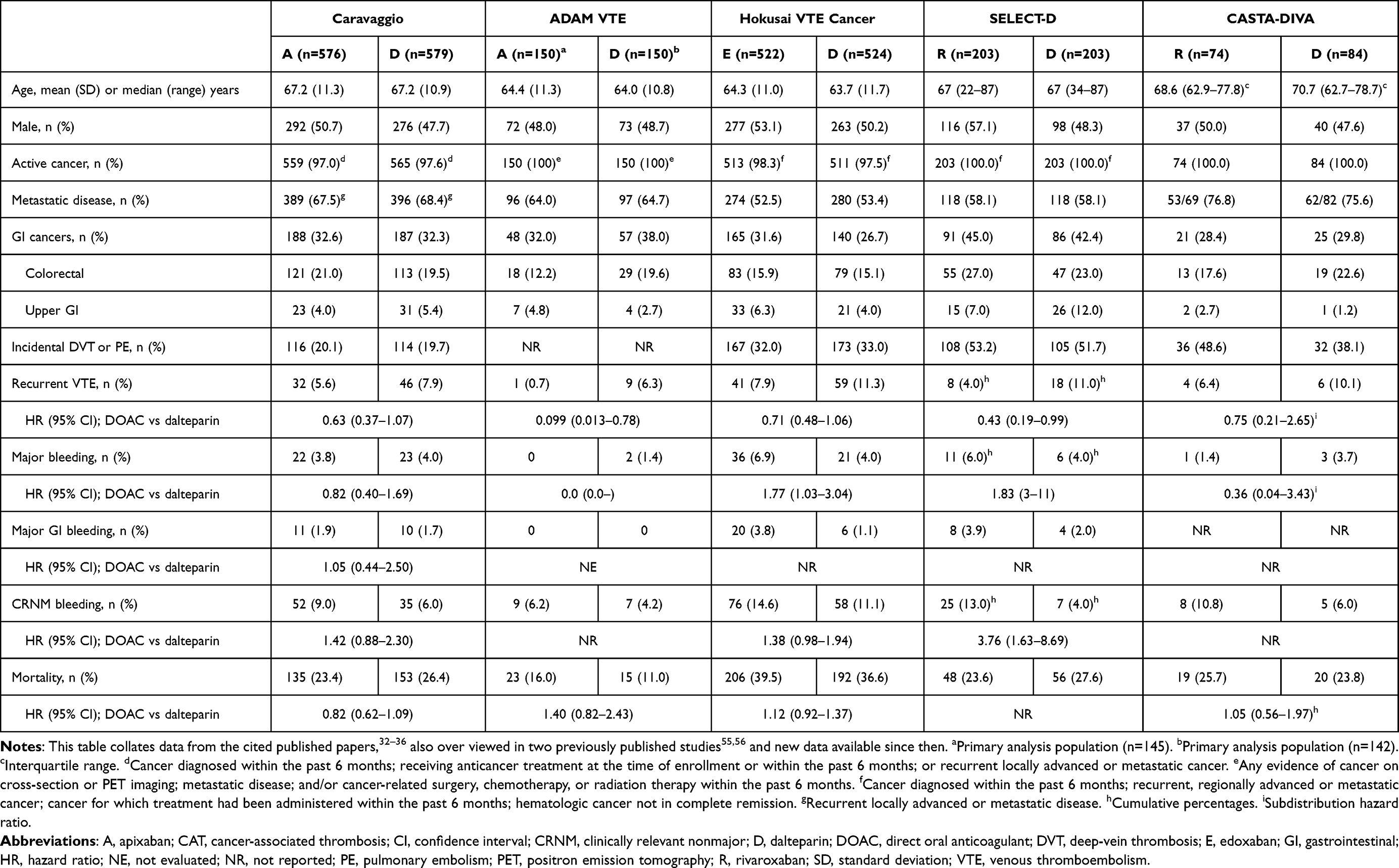 |
Table 1 Characteristics and Efficacy and Safety Outcomes of Randomized Trials Comparing the Safety and Efficacy of DOACs (Apixaban, Edoxaban or Rivaroxaban) and Dalteparin in the Treatment of CAT |
Edoxaban
The 12-month Hokusai VTE Cancer study, a noninferiority trial comparing edoxaban (n=522) with dalteparin (n=524), was the first RCT of a DOAC for the treatment of cancer-associated VTE.34 Patients included in the trial had active cancer or a diagnosis of cancer within the previous 2 years and presented with acute symptomatic or incidentally detected proximal leg DVT or PE. Once-daily dosing of edoxaban 60 mg was initiated after ≥5 days of lead-in therapeutic-dose LMWH. Patients with body weight <60 kg, strong P-glycoprotein (P-gp) inhibitors or creatinine clearance (CrCl) 30–50 mL/min received reduced-dose edoxaban (30 mg once daily). Patients were treated for 6–12 months. The primary outcome was a composite of recurrent VTE or major bleeding during the 12 months after randomization.
The primary outcome occurred in 12.8% of patients in the edoxaban arm and 13.5% of patients in the dalteparin arm (hazard ratio [HR], 0.97; 95% confidence interval [CI], 0.70–1.36; P=0.006 for noninferiority). The primary outcome components recurrent VTE, major bleeding and CRNM bleeding were further analysed separately, and a trend toward a reduction in recurrent VTE with edoxaban versus dalteparin (HR, 0.71; 95% CI, 0.48–1.06) was observed. However, a trend toward more CRNM bleeding with edoxaban was observed, with an almost 80% increase in the risk of major bleeding versus dalteparin (HR, 1.77; 95% CI, 1.03–3.04; P=0.04). The higher rate of major bleeding with edoxaban was mostly accounted for by GI bleeding (3.8% versus 1.1%), particularly upper GI bleeding (3.3% versus 0.6%), which occurred predominantly in patients with upper or lower GI cancer. There was also a suggestion of slightly more major GU bleeding with edoxaban (0.4% versus 0% major bleeds with dalteparin). A post hoc subgroup analysis found a significant increase in major bleeding with edoxaban in patients with GI cancers (12.7% versus 3.6% with dalteparin; HR, 4.0; 95% CI, 1.5–1.06; P=0.005), whereas there was no clear increase in major bleeding with edoxaban in patients with GU cancers (4.6% versus 1.4% with dalteparin).57 In patients with GI cancer, most (76.2%) of the 21 major bleeding events were upper GI bleeding in the edoxaban group, while none of the five major bleeding events were upper GI bleeding in the dalteparin group. Moreover, in patients with GI cancer, three-quarters of the upper GI bleeding events occurred in patients with unresected tumors, suggesting that patients with intact GI tumors were at highest risk of bleeding with edoxaban.
Rivaroxaban
Published soon after the Hokusai VTE Cancer trial results,34 SELECT-D was a pilot study conducted to assess VTE recurrence rates in patients with active cancer treated with rivaroxaban or dalteparin.35 A total of 406 patients presenting with acute symptomatic leg DVT or symptomatic or incidental PE were randomized to standard-dose rivaroxaban (15 mg twice daily for 3 weeks then 20 mg once daily) or dalteparin for 6 months. Compared with dalteparin, the cumulative rate of VTE recurrence at 6 months was reduced with rivaroxaban (HR, 0.43; 95% CI, 0.19–0.99), but at the cost of more bleeding, including a trend towards a doubling of major bleeding events (HR, 1.83; 95% CI, 0.68–4.96) and a marked increase in CRNM bleeding (HR, 3.76; 95% CI, 1.63–8.69). Most major bleeding events were GI bleeds, and most CRNM bleeding events were GI or GU bleeds. Patients with esophageal or gastroesophageal cancer tended to have more major bleeding events with rivaroxaban (36%) than with dalteparin (11%). Study recruitment of patients with esophageal or gastroesophageal junction cancer was stopped when the increased risk of major bleeding with rivaroxaban in patients with upper GI tumors became evident.
CASTA-DIVA was the most recently published randomized trial to compare rivaroxaban with dalteparin for the treatment of cancer-associated VTE.36 Recruitment for this trial was stopped prematurely after randomization of 158 patients because of slow patient enrollment, which limited its statistical power. CASTA-DIVA included patients with active cancer and symptomatic or incidental proximal lower-limb DVT, iliac vein thrombosis, inferior vena cava thrombosis and/or PE who were at high risk of recurrent VTE despite anticoagulation as estimated by a modified Ottawa score of ≥1. Patients received rivaroxaban (15 mg twice daily for 3 weeks then 20 mg once daily) or dalteparin for 3 months. The primary endpoint was the cumulative rate of VTE recurrence or worsening of pulmonary vascular or venous obstruction at 3 months, and occurred in 6.4% and 10.1% of rivaroxaban- and dalteparin-treated patients, respectively. These rates did not meet the predefined criteria for noninferiority of rivaroxaban versus dalteparin (subdistribution HR, 0.75; 95% CI, 0.21–2.66; P=0.13). Compared with dalteparin, the rate of major bleeding was numerically lower with rivaroxaban (subdistribution HR, 0.36; 95% CI, 0.04–3.43), while the rate of major bleeding or CRNM bleeding was numerically higher (HR, 1.27; 95% CI, 0.49–3.26).
In the PRIORITY trial, patients with advanced active upper GI, hepatobiliary or pancreatic cancer were randomized to a DOAC (rivaroxaban 15 mg twice daily for 3 weeks, then 20 mg once daily; or apixaban 10 mg twice daily for 7 days, and then 5 mg twice daily) or dalteparin for 6 months.52 A total of 44 patients were assigned to the DOAC group (of whom 31 received rivaroxaban) and 46 were assigned to the dalteparin group. In a subgroup analysis by DOAC type, rivaroxaban increased the risk of clinically relevant bleeding compared with dalteparin (29.0% versus 13.0%, respectively [HR, 2.37; 95% CI, 0.84–6.66]). The risk of major bleeding was also increased (16.1% versus 4.3%, respectively [HR, 3.89; 95% CI 0.76–20.08]). The rate of recurrent VTE was 3.2% with rivaroxaban versus 2.2% with dalteparin (HR, 1.56; 95% CI, 0.10–24.93).
Apixaban
The most recently published results from RCTs comparing individual DOACs with dalteparin for the treatment of cancer-associated VTE were from the ADAM VTE and Caravaggio trials with apixaban.32,33 The first of these studies was ADAM VTE, a small safety study that enrolled 300 patients with active cancer and VTE, including lower or upper extremity DVT or PE.33 The second study was the Caravaggio trial, a noninferiority study in patients with symptomatic or incidental proximal lower-limb DVT or PE (n=1115).32 In both ADAM VTE and Caravaggio, patients received standard-dose apixaban (10 mg twice daily for 7 days, followed by 5 mg twice daily) or dalteparin over 6 months.
In the ADAM VTE trial, the primary outcome was major bleeding up to 6 months, which was experienced by none of the patients receiving apixaban and 1.4% of patients receiving dalteparin (P=0.14).33 The rate of recurrent VTE was significantly lower in patients receiving apixaban than in patients receiving dalteparin (HR, 0.099; 95% CI, 0.013–0.78; P=0.028). For the secondary composite bleeding endpoint of major or CRNM bleeding, 6% of patients in each treatment arm experienced an event.
The Caravaggio trial found apixaban to be noninferior to dalteparin with respect to the primary outcome of recurrent VTE, which occurred in 5.6% of patients treated with apixaban and 7.9% of patients in the dalteparin group (HR, 0.63; 95% CI, 0.37–1.07; P<0.001 for noninferiority, P=0.09 for superiority), with no increase in major bleeding (HR, 0.82; 95% Cl, 0.40–1.69) (Table 1).32 Event-free survival analysis showed a significant reduction in recurrent VTE, major bleeding or death with apixaban versus dalteparin (HR, 0.74; 95% CI, 0.57–0.95), thereby reflecting a net clinical benefit. Approximately one-third of patients in Caravaggio had GI cancer, but there was no significant difference in the risk of major GI bleeding with apixaban versus dalteparin (HR, 1.05; 95% CI, 0.44–2.50). Upper and lower GI bleeding occurred in similarly low numbers of patients treated with apixaban (0.9% and 1.0%, respectively) or dalteparin (1.0% and 0.7%, respectively). A subgroup analysis of the Caravaggio trial has shown that in patients with GI cancer, rates of major GI bleeding were low and similar between the two treatment groups. In the apixaban group, lower GI bleeding occurred in 3 patients and upper GI bleeding occurred in 4 patients of the 188 patients with GI cancer, whereas in the dalteparin group, lower and upper GI bleeding occurred in 3 patients each of the 187 patients.58 A slightly increased rate of major GU bleeding was observed with apixaban (0.7% vs 0.2%). This increase in GU bleeding contributed to a trend towards more CRNM bleeding (HR, 1.42; 95% Cl, 0.88–2.30) with apixaban versus dalteparin.32
Compared with the Hokusai VTE Cancer and SELECT-D trials, the small sample size, inclusion of patients with upper extremity DVT, and a slightly different distribution of cancer types in ADAM VTE, including a smaller proportion of patients with upper GI malignancy, may have resulted in a population with a relatively low risk of bleeding.19,20,59 In contrast, patients in the Caravaggio study were an older, at-risk population with a broad range of tumor types, including upper and lower GI tumors, and a high rate of metastatic disease.32 Rates of major bleeding in DOAC-treated patients differed across the ADAM VTE, Caravaggio, Hokusai Cancer VTE, SELECT-D and CASTA-DIVA trials, but with the exception of ADAM VTE, major bleeding consistently occurred in 4% of patients in the dalteparin treatment arms of these trials,32–36 indicating that, relative to ADAM VTE, the risk of bleeding was similarly high in the other trial populations.
In the PRIORITY trial of patients with advanced active upper GI, hepatobiliary or pancreatic cancer, 13 out of 40 patients randomized to the DOAC group received apixaban, and 46 patients received dalteparin. In a subgroup analysis by DOAC type, apixaban increased the risk of clinically relevant bleeding compared with dalteparin (46.2% versus 13.0%, respectively [HR 3.93; 95% CI 1.27–12.22]). The risk of major bleeding was also increased (23.1% versus 4.3%, respectively [HR 3.89; 95% CI 0.76–20.08]). There were no cases of recurrent VTE in the apixaban group and a rate of 2.2% in the dalteparin group (HR, 0.03; 95% CI, 0.0–).
A large retrospective analysis of US claims databases has generated real-world evidence to complement data from Caravaggio and ADAM VTE regarding trends toward reduced recurrent VTE and major bleeding with apixaban versus LMWH in patients with cancer-associated VTE.60 Additionally, apixaban was shown to be associated with a lower risk of recurrent VTE than warfarin, without an increased risk of major bleeding. In this real-world analysis, patients receiving apixaban (n=3393), LMWH (n=6108) and the VKA warfarin (n=4585) had active cancer. The cohorts were well matched for characteristics that influence the risk of VTE and bleeding, including age, type of malignancy, metastases and chemotherapy. At the 6-month follow-up, a 39% reduction in the risk of recurrent VTE in the apixaban cohort versus LMWH (HR, 0.61; 95% CI, 0.47–0.81) and a 32% reduction versus warfarin (HR, 0.68; 95% CI, 0.52–0.90) was observed. Compared with LMWH, patients treated with apixaban had a 37% reduction in the risk of major bleeding (HR, 0.63; 95% CI, 0.47–0.86), as well as a lower risk of CRNM bleeding (HR, 0.81; 95% CI, 0.70–0.94). Patients treated with apixaban had less major bleeding than those receiving LMWH, regardless of metastases, cancer treatment, chemotherapy, GI cancer or VTE event type (DVT only or PE with or without DVT).61 Compared with warfarin, apixaban-treated patients had a similar risk of major bleeding (HR, 0.73; 95% CI, 0.53–1.00) and CRNM bleeding (HR, 0.89; 95% CI, 0.77–1.04). When using the entire follow-up period (maximum length of follow-up: approximately 3 years), results were generally consistent with those of the 6-month follow-up.
Meta-Analyses
After publication of Caravaggio, a number of meta-analyses were performed in which the Caravaggio trial results were combined with the Hokusai VTE Cancer, SELECT-D and ADAM VTE trial results (Table 2).20,51,62–66 Despite employing different statistical methods, these meta-analyses had similar findings, with the results favoring the studied factor Xa inhibitor DOACs in relation to efficacy (recurrent VTE), without a significant increase in major bleeding compared with dalteparin. Low heterogeneity and the consistency of efficacy results across the Hokusai VTE Cancer, SELECT-D, ADAM VTE and Caravaggio trials illustrate the generalizability of the improved efficacy of oral factor Xa inhibitors versus dalteparin.20,62,63,67 In contrast, assessment of between-study heterogeneity for major bleeding showed that the ADAM VTE and Caravaggio trials, in which overall major bleeding risk was not increased with apixaban versus dalteparin,32,33 were the main contributors to heterogeneity and may have influenced overall rates of major bleeding.62 Indeed, after removal of the Caravaggio study results, meta-analysis of the remaining studies showed a significant increase in major bleeding risk with DOACs compared with dalteparin.63 Another meta-analysis using only the Hokusai VTE Cancer and SELECT-D studies reported similar results. Compared with dalteparin, edoxaban and rivaroxaban were more effective at preventing recurrent VTE but had an increased risk of major bleeding.51
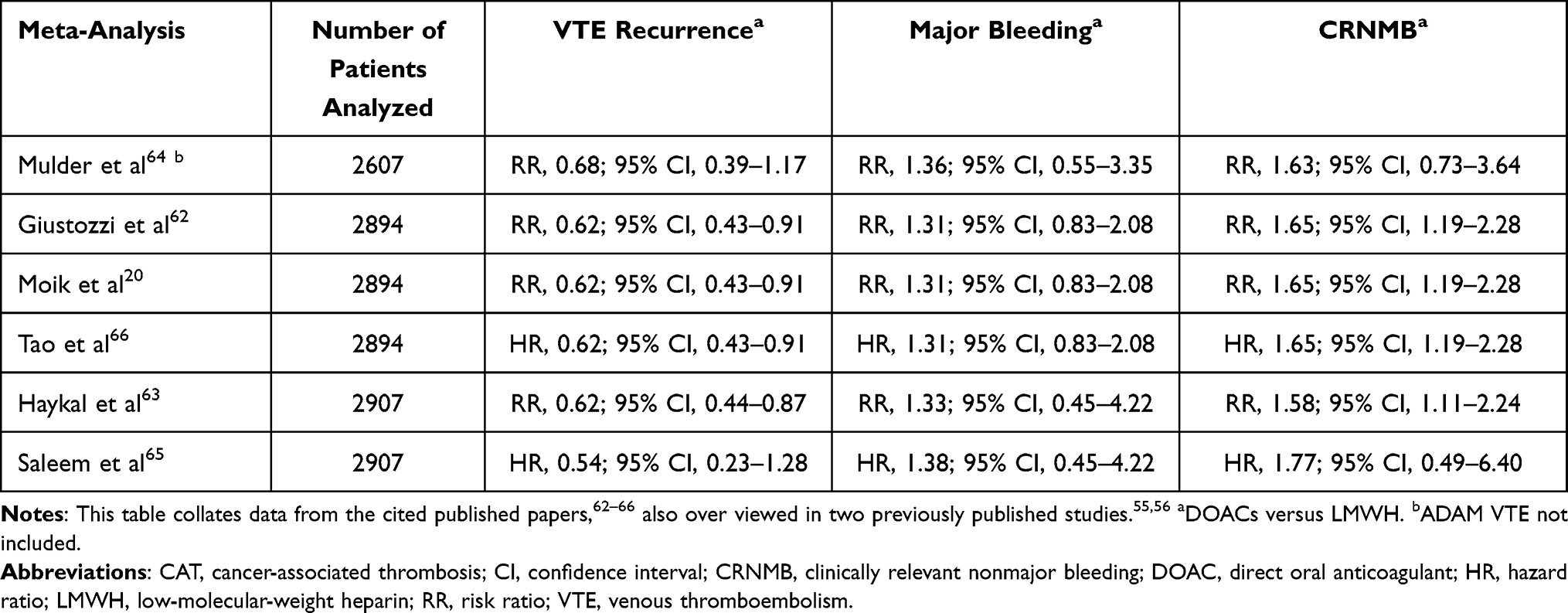 |
Table 2 Efficacy and Safety Outcomes of Meta-Analyses of the Hokusai VTE Cancer, SELECT-D, ADAM VTE and Caravaggio Trials of DOACs versus LMWH for the Treatment of CAT |
The CASTA-DIVA trial investigators conducted a meta-analysis incorporating CASTA-DIVA trial results with those of the Caravaggio, ADAM VTE, Hokusai VTE Cancer and SELECT-D trials.35 Results were very similar to those shown in Table 2, with DOACs showing an overall reduced risk of recurrent VTE compared with dalteparin (HR, 0.63; 95% CI, 0.47–0.86), an increased risk of major bleeding (HR, 1.26; 95% CI, 0.84–1.90) and an increased risk of major bleeding or clinically relevant nonmajor bleeding (HR, 1.48; 95% CI, 0.49–3.26).
International Guideline Recommendations for the Treatment of Cancer-Associated VTE
Practice guidelines published before 2018 consistently recommended LMWH as the preferred treatment for cancer-associated VTE due to the absence of robust evidence for use of DOACs against LMWH. There were no or relatively weak recommendations for DOACs as an alternative to LMWH.30 For example, local guidelines published in 2015 for the treatment of cancer-associated VTE in clinical practice in Saudi Arabia strongly recommended LMWH for the long-term treatment of VTE in patients with metastatic cancer.28 Adherence to these now outdated guidelines would prevent many patients with active cancers from receiving anticoagulation treatment for VTE in line with the RCT data on DOACs. However, during the submission of this review, a consensus for the management of cancer-associated VTE in Saudi Arabia has been published and recommends treatment either with LMWHs or DOACs.68 The consensus is evidence-based and specific to clinical experience, in line with the current health care policies and settings in Saudi Arabia. Therefore, this review in addition to the guidelines may benefit the other MENA countries.
Factor Xa inhibitor DOACs are now widely recommended by recent international guidelines in patients without active GI or GU cancer, who are not deemed to be at high risk of bleeding due to factors such as thrombocytopenia or renal insufficiency and are not receiving medication that may potentially cause a serious drug–drug interaction (DDI) (Table 3).31,37–42,69 Otherwise, LMWH is preferred. However, different guidelines differ in their recommendation of which DOACs to use. The 2021 ACCP, National Comprehensive Cancer Network (NCCN) and American Society of Hematology (ASH) guidelines, all of which were published after the Caravaggio trial, support the use of apixaban, edoxaban or rivaroxaban for the treatment of cancer-associated VTE.41,42 ACCP guidelines strongly recommend treatment with apixaban, edoxaban or rivaroxaban over LMWH, and specify that apixaban or LMWH may be preferred in patients with luminal GI malignancies.31 Similarly, NCCN guidelines specify that apixaban, edoxaban or rivaroxaban are preferred over LMWH for patients without gastric or gastroesophageal lesions, while acknowledging that apixaban may be safer than edoxaban or rivaroxaban in patients with such lesions.42 ASH guidelines suggest LMWH or DOACs (rivaroxaban or apixaban) for initial treatment, and DOACs (apixaban, edoxaban or rivaroxaban) for short- to long-term anticoagulation, with caution advised in patients with GI cancer because of the higher risk of bleeding.41 With the exception of 2020 National Institute for Health and Care Excellence (NICE) guidelines, which include a general recommendation for DOACs in cancer patients,69 guidelines published post-Hokusai VTE Cancer and SELECT-D and pre-Caravaggio specifically recommend edoxaban or rivaroxaban for patients with non-GI cancers at low bleeding risk; otherwise LMWH remains the preferred anticoagulant.37–40 The American Society of Clinical Oncology (ASCO) guidelines support the use of apixaban, rivaroxaban, or LMWH in selected high-risk outpatients with cancer, and rivaroxaban and edoxaban for extended VTE treatment.37 The updated 2023 ASCO guidelines for patients with cancer surgery added apixaban and rivaroxaban as options for extended pharmacologic thromboprophylaxis.70 The International Initiative on Thrombosis and Cancer (ITAC) guidelines, published in 2019 and updated in 2022, recommend the use of LMWHs or DOACs as initial treatment of established VTE, depending on the creatinine clearance and patient’s risk of GI or GU cancer.40,71 For early maintenance and long-term treatment, the 2022 guideline provides an update that LMWHs are preferred but apixaban, rivaroxaban and edoxaban can be used, depending on creatinine clearance and with caution in patients with GI or GU cancers.40,71 The 2023 European Society for Medical Oncology (ESMO) clinical practice guidelines for VTE in cancer patients recommend the use of LMWH, unfractionated heparin (UFH), fondaparinux, apixaban or rivaroxaban for acute phase (first 5–10 days after diagnosis), with a preference for LMWH than UFH and fondaparinux.72 For long term, the use of LMWH, apixaban, edoxaban or rivaroxaban is preferred over VKA. In patients with luminal GI cancer, patients at high risk of GI bleeding, receiving inducers and/or inhibitors of cytochrome P450 3A4 (CYP3A4) or P-gp, LMWH is preferred.72 Beyond the initial 6 months, the ESMO guidelines recommend LMWH, apixaban, edoxaban, rivaroxaban or VKAs if patients have active cancer and their risk of thrombosis outweighs the risk of bleeding.72 Going forward, the Caravaggio trial, which has clearly established the important role of DOACs, especially apixaban, in the treatment of cancer-associated VTE,67 will contribute to the guidelines as they are updated.
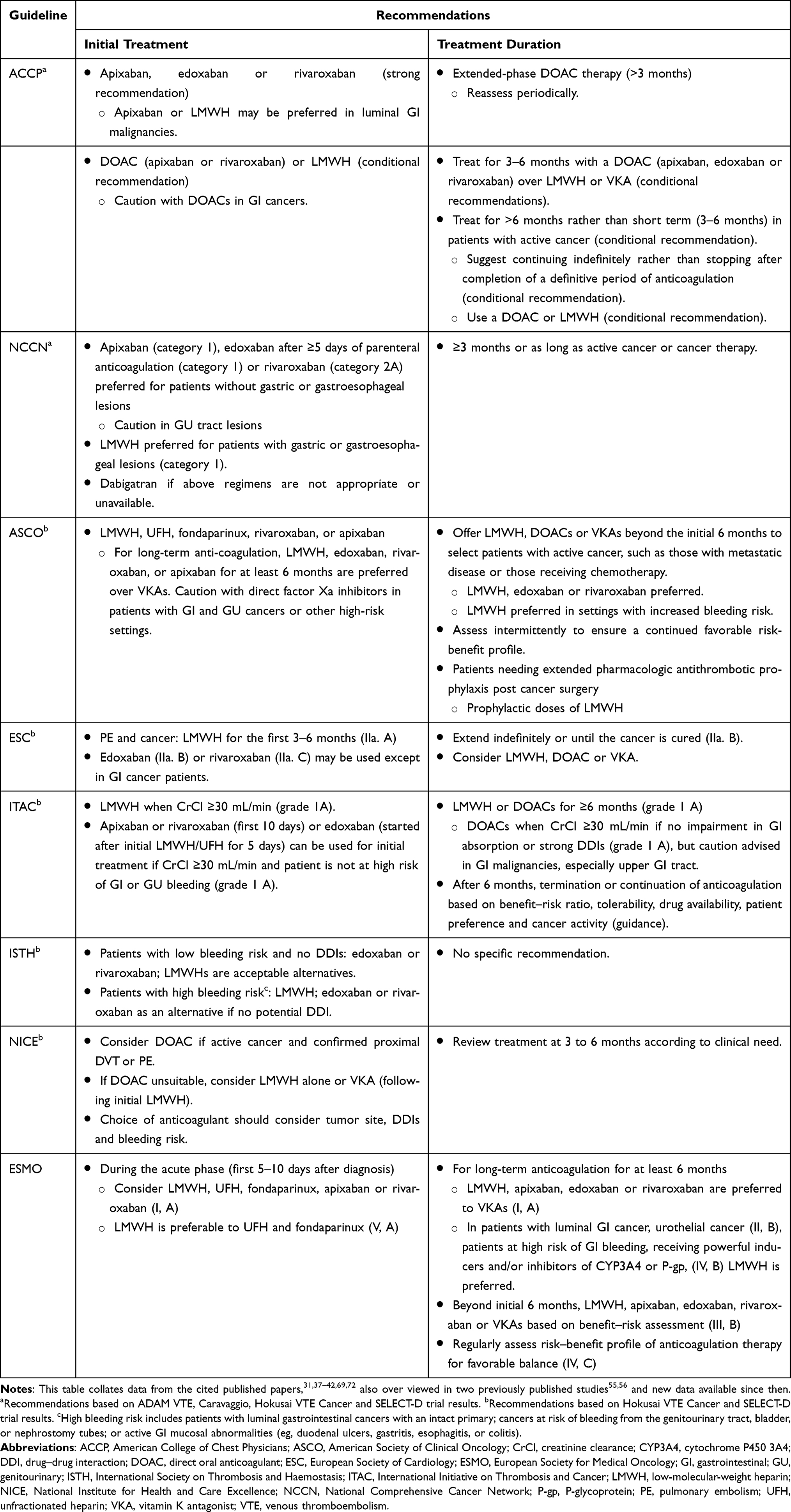 |
Table 3 Guideline Recommendations for the Treatment of Cancer-Associated VTE |
Because high-quality data for extended anticoagulation treatment are limited to the 6- to 12-month time period, recommendations regarding its extended use in cancer patients are mostly based on expert opinion.73 Although the optimal duration of DOAC or LMWH therapy is uncertain, there is general consensus that anticoagulation should be continued for ≥3–6 months or, given the high long-term risk of recurrent VTE in patients with active cancer,11 for as long as the cancer is active or being treated, unless there is a contraindication or unacceptable clinical risk.37–40,42 Extended anticoagulation is much more achievable with a DOAC than with LMWH therapy, which is often discontinued after 3–6 months.74,75 The recently completed 12-month EVE trial (NCT03080883) found similar rates of bleeding with apixaban 5 mg or 2.5 mg twice daily without increasing thrombotic outcomes.76 Additionally, an extended DOAC treatment study API-CAT (NCT03692065) comparing standard-dose apixaban (5 mg twice daily) with stepped down 2.5 mg dosing is ongoing.73 An ideal future study would be to compare a DOAC versus placebo after 6 months of standard treatment if the cancer is no longer active or if other thrombotic risk factors are resolved.
DOACs in Challenging Subgroups of Cancer Patients
Although recent cancer-associated VTE treatment guidelines include recommendations for the use of DOACs, many patient management questions remain unanswered due to the lack of clinical trial data.77 Patients with certain tumor types, thrombocytopenia, renal or hepatic impairment, and any other condition or concomitant medication associated with an increased risk of bleeding or unclear net clinical benefit for anticoagulation provide clinical challenges for which empiric management decisions must be made.17,43,78 To date, the shift towards using DOACs in these challenging subgroups of patients has been appropriately cautious, and guidance on their use is required (Table 4).43
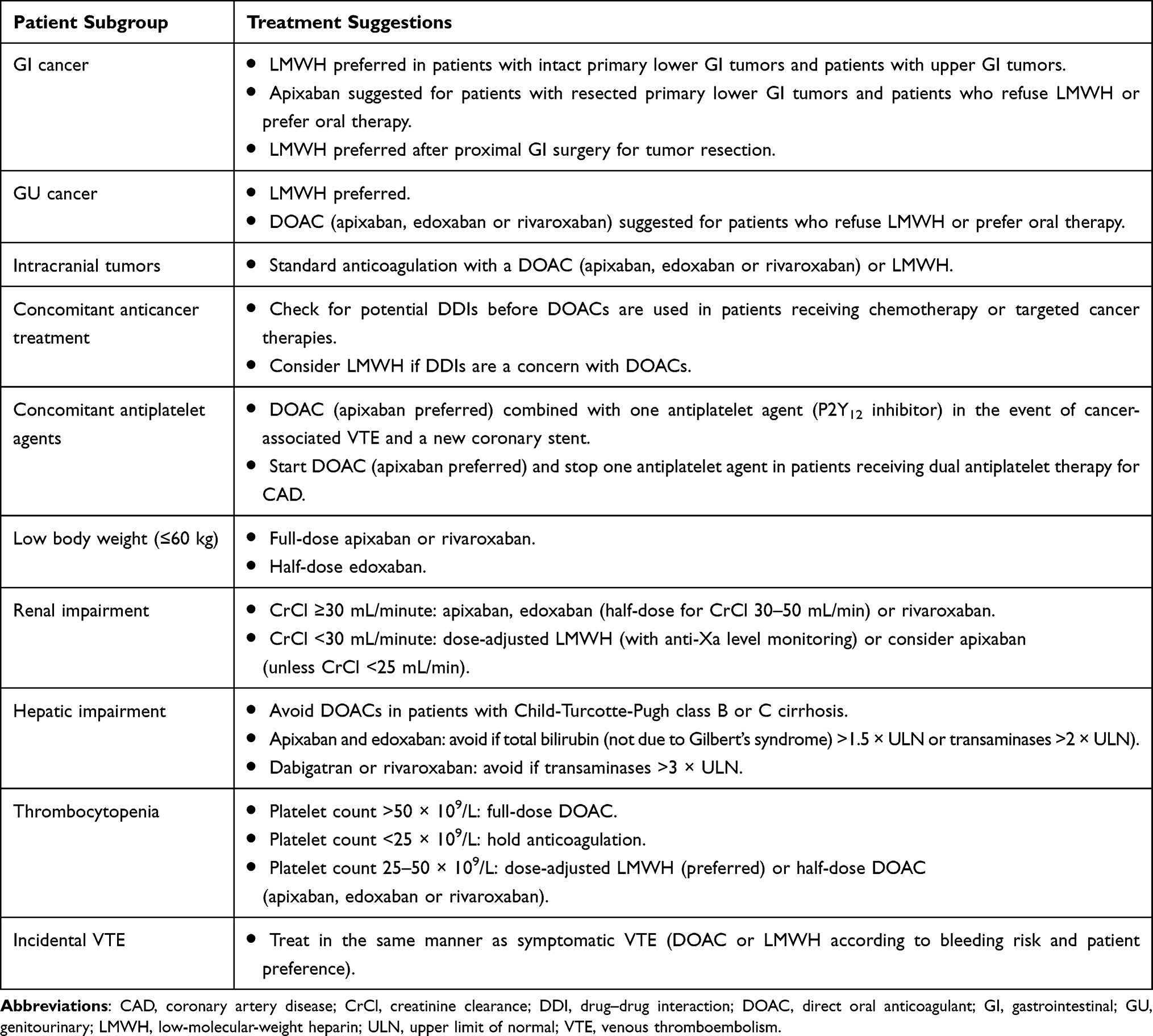 |
Table 4 Guidance for the Use of DOACs to Treat Cancer-Associated VTE in Challenging Patient Subgroups |
GI Cancer
In patients with GI cancer, edoxaban and rivaroxaban use is not recommended because of an increased risk of major GI bleeding versus dalteparin in the Hokusai VTE Cancer and SELECT-D trials.34,35 However, the Caravaggio trial does not report an increased risk of major upper or lower GI bleeding with apixaban versus dalteparin. This Caravaggio trial observation suggests that apixaban could be a safe alternative to LMWH in patients with GI cancer.32,78 It is unclear whether apixaban is safer than edoxaban or rivaroxaban in patients with GI cancer. However, it is possible that more stable plasma drug concentrations, lower peaks and higher troughs, obtained with twice-daily apixaban dosing compared with once-daily edoxaban or rivaroxaban dosing, could have an impact on safety79,80 and contribute to reduced risk of GI bleeding. Although the mechanism of bleeding in GI cancer patients treated with DOACs remains unclear, in the Hokusai VTE Cancer study, upper GI bleeding was reported in all types of GI cancer regardless of location,57 suggesting a possible direct effect on the upper GI tract.
Both the Hokusai VTE Cancer and Caravaggio trials had similar proportions of patients with GI cancer (~30%), and in both studies, approximately 5% of the total patients had upper GI cancer.32,34 Most of the GI bleeding events from the Hokusai VTE Cancer trial (patients receiving edoxaban) and all major GI bleeding events from the Caravaggio trial (patients receiving apixaban) occurred in patients with unresected tumors.58 Therefore, although results with apixaban from the Caravaggio trial are promising, apixaban should be used with caution in patients with GI cancer, particularly those with intact primary GI tumors.
Results of the PRIORITY trial, in which approximately 59% of patients had upper GI cancer, provide further evidence that caution is needed when choosing an anticoagulant for this patient population. Although the PRIORITY sample size was small, both apixaban and rivaroxaban increased the risks of clinically relevant bleeding and major bleeding compared with dalteparin. A total of 52% of clinically relevant bleeding events and 80% of major bleeding events occurred in the GI tract. In this trial, cancer involvement at the GI mucosa rather than the cancer type was a significant risk factor for clinically relevant bleeding.
Stomach cancer is the most common GI cancer in the MENA region, followed by liver cancer, colorectal cancer, and esophageal cancer, but rates of gastric and esophageal cancers vary between countries according to genetic and lifestyle factors.81 On the basis of the available evidence, LMWH should still be the anticoagulant of choice in patients with gastric or esophageal cancer, and apixaban should be the preferred DOAC when these high-risk patients refuse parenteral therapy.78
There are also limited data for the use of DOACs in patients after proximal GI surgery for tumor resection. In situations such as this, when GI absorption may be compromised, LMWH is often preferred to ensure adequate levels of anticoagulation.43,78
GU Cancer
In general, treatment guidelines acknowledge that the risk of GU tract bleeding may increase with DOACs, and advise caution in patients with active GU tract lesions.43 The Caravaggio and Hokusai VTE Cancer trial results32,34 suggested increased GU bleeding with apixaban and edoxaban but numbers were too small for meaningful analysis and, therefore, a conclusion regarding GU bleeding risk could not be drawn. Meta-analyses of subgroup data collected from the Hokusai VTE Cancer, SELECT-D, ADAM VTE and Caravaggio trials also showed that GU sites of major bleeding were more common with factor Xa inhibitor DOACs than with dalteparin.20,62 However, in patients with GU cancer, these DOACs were not significantly associated with a greater risk of major bleeding versus dalteparin (RR, 2.81; 95% CI, 0.45–17.40; P=0.27).63
Urothelial irritation from schistosomiasis infection contributes to high rates of squamous cell carcinoma of the bladder in some MENA countries, but a gradual shift to more urothelial carcinomas linked to cigarette smoking and other lifestyle changes linked to urbanization has been observed.82–84 Based on current evidence of a possible increase in the risk of urothelial bleeding with DOACs, LMWH may be preferred in patients with active, unresected luminal lesions in the GU tract, recent GU tumor surgery or recent major GU bleeding.78 When DOACs are used in such patients, vigilance for signs of urothelial bleeding is required.
Intracranial Tumors
Patients with intracranial tumors have an increased risk of VTE and also an increased risk of intracranial hemorrhage.78 In the Caravaggio trial, patients with brain tumors or intracerebral metastases were excluded as a precaution.32 A retrospective cohort study in patients with primary or metastatic brain tumors with brain lesions published after the start of Caravaggio showed that DOACs did not increase the risk of intracranial hemorrhage compared with LMWH.85 Therefore, patients who developed cerebral metastases during the Caravaggio trial were allowed to continue treatment. Furthermore, in the Hokusai VTE Cancer trial, which included 74 (7.1%) patients with primary or metastatic brain tumors, a similar low percentage of patients from the edoxaban (0.4%) and dalteparin (0.6%)57 groups experienced intracranial hemorrhage. In a recent retrospective study, numerically lower incidence rates and higher reduction in incidence of recurrent VTE, major bleeding, and CRNM bleeding were observed for apixaban versus LMWH in patients with brain cancer.86 Therefore, DOACs are considered to be at least as safe as LMWH in patients with primary or metastatic brain tumors.78
Concomitant Cancer Treatment
Although DOACs have fewer DDIs than VKAs77 do, all DOACs are substrates of P-gp. In addition, apixaban and rivaroxaban are also substrates of CYP3A4.87 Chemotherapies or targeted cancer therapies that affect P-gp and/or CYP3A4 pathways may therefore decrease or increase the anticoagulant effect of DOACs, and care is needed during concurrent treatment. Patients treated with powerful inducers and/or inhibitors of CYP3A4 or P-gp have been primarily excluded from RCTs of DOACs for the treatment of cancer-associated VTE;59,78 however, no anticancer therapy was excluded from Caravaggio. As such, patients were receiving a broad array of cytotoxic and biologic anticancer therapies, including new therapies, such as antiangiogenic monoclonal antibodies (~3% of patients) and checkpoint inhibitors (~2%).32 Concomitant administration of anticancer agents, including P-gp and/or CYP3A4 inhibitors or inducers, did not appear to affect the incidence of VTE recurrence and major bleeding associated with apixaban. This observation suggests that apixaban can be safely administered in patients with cancer-associated VTE even when they are receiving concomitant anticancer treatment.88 Despite this, uncertainty remains regarding DDIs between DOACs and cancer therapies, and potential DDIs should be checked before DOACs are used in patients receiving chemotherapy or targeted cancer therapies.18,59,78 In patients receiving concurrent strong dual CYP3A4 and P-gp inhibitors, a dose reduction to 2.5 mg twice daily is recommended for apixaban. Similarly, in patients on concurrent potent P-gp inhibitors, a dose reduction to 30 mg daily for edoxaban is recommended.78 DOACs should be avoided in all other instances in which DDI is a concern.18,78 In some practices, DOACs are avoided on the day of chemotherapy because of uncertainty about reactions between chemotherapy and DOACs; on these days, patients receive LMWH.
Concomitant Antiplatelet Agents
Antiplatelet agents are frequently indicated for coronary artery disease, which is a common comorbidity in cancer patients worldwide.89,90 There are no cancer-specific data to guide combined anticoagulant and antiplatelet therapy in patients with cancer-associated VTE and cardiovascular disease; thus, suggestions for treatment must be extrapolated from the best available evidence in the general population.78 An antiplatelet subgroup analysis of the AMPLIFY study showed that an improved safety profile of apixaban compared with VKA was seen in patients with VTE whether or not they were taking antiplatelet agents.91 The AUGUSTUS trial in patients with atrial fibrillation and recent acute coronary syndrome or percutaneous coronary intervention showed that apixaban plus a P2Y12 inhibitor antiplatelet agent resulted in fewer bleeding complications and hospitalizations than combination therapy with a VKA and a P2Y12 inhibitor with or without aspirin.92 On the basis of these findings, it has been suggested that patients with cancer associated thrombosis and a new coronary stent receive a DOAC, preferably apixaban, in combination with a PY12 inhibitor.78 In patients with stable coronary artery disease who experience cancer-associated VTE while receiving dual antiplatelet therapy, it is suggested that one of the antiplatelet agents is stopped and a DOAC be started.78 There are no data for LMWH in this population.
Low Body Weight
DOACs may be considered in cancer patients with low body weight (≤60 kg). Although half-dose edoxaban was used in patients with body weight ≤60 kg in the Hokusai VTE Cancer trial,34 there is no strong evidence for DOAC dose reduction in low-weight patients. All patients from the SELECT-D, CASTA-DIVA, ADAM VTE and Caravaggio trials32,34–36 received full-dose rivaroxaban or apixaban. On the basis of these trials, clinicians should feel comfortable using standard doses of these DOACs regardless of body weight.43
Obesity
In patients with cancer, obesity might increase the risk of VTE. Limited research is available on the efficacy and safety of DOACs in patients with cancer and obesity. A post-hoc analysis of data from the AVERT trial was conducted to investigate the efficacy and safety of apixaban thromboprophylaxis in obese (n=215) versus non-obese (n=348) patients with cancer. Patients were classified as obese (body mass index [BMI] ≥30 kg/m2) and non-obese (BMI <30 kg/m2) based on their BMI at randomization. Among the non-obese patients, 9 (5.1%) patients out of 178 receiving apixaban and 15 (8.8%) out of 170 patients receiving placebo had VTE. Among the obese patients, a significantly lower incidence of VTE was observed in patients receiving apixaban (n=4/110) than in patients receiving placebo (n=14/105) (HR, 0.26; 95% CI, 0.14–0.46; P<0.0001). Similarly, lower risks of PE and DVT were observed in patients treated with apixaban than placebo. A numerically higher but statistically non-significant risk of clinically relevant bleeding was observed in patients receiving apixaban than placebo (HR, 2.09; 95% CI, 0.96–4.51; P=0.062).93 However, interpretation of these results requires caution because the distribution of types of cancer with distinct thrombo-hemorrhagic risk profiles was significantly different between the groups. Another study assessed outcomes in patients with morbid obesity, acute VTE, and concurrent cancer receiving anticoagulation treatment from the Registro Informatizado Enfermedad TromboEmbólica.94 The patients were receiving anticoagulation either with VKA, LMWH, or DOACs. A lower mortality rate (HR, 0.34; 95% CI, 0.25–0.45) and lower rate of major bleeding (HR, 0.54; 95% CI, 0.28–0.96) were observed in patients with cancer and obesity (n=245) than in patients with cancer and had normal weight (n=4198), while the rate of VTE recurrence was similar between these groups (HR, 0.62; 95% CI, 0.34–1.05).94 Specific research on the efficacy and safety of DOACs in patients with cancer and obesity is lacking. However, these limited data point towards a possible use of DOACs in patients with cancer and obesity.
Renal Impairment
Renal insufficiency may develop in patients with cancer as a consequence of malignancy. Severe renal insufficiency treatment or associated complications increase the risk of VTE and bleeding.78,95 Most DOACs are at least partially renally cleared, and pivotal DOAC RCTs both in general and cancer populations excluded patients with CrCl <30 mL/min (<25 mL/min for apixaban).78 In general, no dose adjustment is required in patients with mild renal insufficiency.43 The edoxaban dose is halved in patients with CrCl 30–50 mL/min.34 Apixaban is the only DOAC approved for use in patients with CrCl <30 mL/min, but questions remain as to the optimal use of the drug in this population. Dose-adjusted LMWH (with anti-Xa monitoring) is an appropriate alternative in patients with CrCl <30 mL/min.17,78
Hepatic Impairment
Guidance for the use of DOACs in patients with liver disease is important in the MENA region, which has a high burden of chronic liver disease and cirrhosis secondary to hepatitis C infection.81,96,97 DOACs are not recommended for patients with Child-Turcotte-Pugh class B or C cirrhosis.17 Apixaban and edoxaban are contraindicated in patients with clinically significant liver disease, including transaminases >2 × upper limit of normal (ULN), and rivaroxaban is contraindicated in patients with transaminases >3 × ULN.
Thrombocytopenia
Thrombocytopenia resulting from chemotherapy and/or malignancy is common in patients with cancer. In this setting, the risk of bleeding is increased but the risk of VTE remains.78 In the Caravaggio trial, owing to the increased risk of bleeding associated with low platelet counts, patients with acute leukemia were excluded. Moreover, all five RCTs comparing DOACs with dalteparin in patients with cancer-associated VTE excluded patients with severe thrombocytopenia (Hokusai VTE Cancer and ADAM VTE trials: platelet count <50 × 109/L; SELECT-D trial: <100 × 109/L; CASTA-DIVA trial: <50 × 109/L; Caravaggio trial: <75 × 109/L).32–36 For patients with platelet count <25 × 109/L, it is safest to withhold anticoagulation until the platelet count has recovered.78 In the absence of data on the use of DOACs in patients with cancer-associated VTE and platelet count <50 × 109/L, dose-adjusted LMWH may be preferred for patients with a platelet count 25–50 × 109/L, but a half-dose DOAC has been suggested as a potentially acceptable alternative.78 Care should be taken when using DOACs in patients undergoing chemotherapy and a decrease in platelet counts is expected.17
Incidentally Diagnosed VTE
In some MENA regions, because of the use of high-resolution CT scanning for staging and follow-up of cancer patients, the incidence of incidentally diagnosed VTE is increasing. Incidental VTE was reported as the index event in approximately 20% to 50% of patients in the Hokusai VTE Cancer, SELECT-D, CASTA-DIVA and Caravaggio trials.32,34–36 Subgroup meta-analysis of data from the Hokusai Cancer VTE and Caravaggio trials with or without inclusion of SELECT-D showed that the risks of recurrent VTE and major bleeding with DOACs versus dalteparin were similar in patients with either incidental or symptomatic VTE as the index event, further favoring DOACs in terms of efficacy, without a significant increase in major bleeding.20,64 Although clinicians may question whether all incidentally discovered asymptomatic VTE should be treated with full-dose DOAC therapy,17 incidental VTE can generally be treated in the same manner as symptomatic VTE.37,42
Discussion
Factor Xa inhibitor DOACs are recommended for the treatment of VTE in patients with non-GI cancers at low bleeding risk with no potential for DDIs.31,37–42,69 Current practice favors LMWH in all other patients. The more recent Caravaggio and ADAM VTE trial results have added to the evidence from Hokusai Cancer VTE and SELECT-D trials of the consistent efficacy of factor Xa inhibitor DOACs for the treatment of cancer-associated VTE but have also showed some heterogeneity with regard to safety.32–35 Concerning major bleeding and major GI bleeding, the Caravaggio and ADAM VTE study results with apixaban compared favorably with those of the Hokusai VTE Cancer and SELECT-D trials of edoxaban and rivaroxaban, clearly demonstrating no increased risk of bleeding with apixaban versus dalteparin in contrast to increased risk with edoxaban or rivaroxaban. The efficacy and safety outcomes of rivaroxaban versus dalteparin in CASTA-DIVA were generally consistent with those of the Cancer VTE, SELECT-D, Caravaggio and ADAM VTE trials, despite the small sample size limiting statistical power in this trial.36 However, in the absence of any RCTs comparing the DOACs head-to-head, it is inappropriate to conclude that any one DOAC is safer than another.
The Caravaggio trial is a landmark study that has clearly established the important role of DOACs in the treatment of cancer-associated VTE,67 but with the exception of the ACCP, ASH and NCCN 2021 guideline recommendations,31,41,42 all major international practice guidelines for the treatment of CAT currently pre-date publication of the Caravaggio trial results.37–40,69 These guidelines tend to recommend edoxaban or rivaroxaban as preferred therapy for VTE in patients with non-GI cancer.37–40,42 The Caravaggio study finding that apixaban was noninferior to dalteparin for the treatment of cancer-associated VTE without an increased risk of major lower or upper GI bleeding, despite approximately one-third of the population having GI cancer,32 will contribute to the evolution of practice guidelines as they are updated. In the absence of up-to-date MENA-specific guidelines, physicians in MENA regions are advised to adhere to recommendations from the most up-to-date international guidelines31,41,42 and the most recent Saudi Arabia guidelines.68
The results of the Caravaggio trial should help clinicians to make informed decisions for the treatment of cancer-associated VTE. Regardless of tumor type, clinicians should consider prescribing a factor Xa inhibitor DOAC as a practical, long-term alternative to LMWH for patients with active cancer. Treatment should be extended beyond 6 months in patients with ongoing active malignancy such as metastatic disease and/or with ongoing anticancer therapy, and it should be assessed periodically to ensure continued net clinical benefit. The Caravaggio trial and real-world evidence support a recommendation for apixaban in patients with GI tumors, but caution is advised, particularly in patients with upper GI tumors or unresected lower GI tumors.31,32,42,58,78 Ultimately, the decision to use a DOAC requires careful consideration of bleeding risk, the cost–benefit and convenience of oral therapy, and patient needs and preferences, and these factors may change over the course of the cancer journey. This also applies when deciding whether to use a DOAC in other challenging subgroups of patients, including patients with GU cancers and patients with comorbidities that increase the risk of bleeding, such as patients with severe renal impairment or thrombocytopenia. LMWH may be preferred for patients at very high risk of bleeding who are willing and able to comply with daily subcutaneous injections. VKAs should only be used in patients for whom DOACs and LMWH are unavailable or unsuitable.
Conclusion
DOACs represent a major paradigm shift in the treatment of cancer-associated VTE in the MENA region. Cancer patients already have a major burden of illness, and long-term anticoagulation is generally much more achievable with oral anticoagulation than with LMWH. Therefore, in countries where they are available, DOACs should always be considered for the treatment of cancer-associated VTE. However, in patients with GI malignancies and upper or unresected lower GI tumors, LMWH may be preferred due to increased risk of major GI bleeding events. Vitamin K antagonists should be used only when DOACs and LMWH are unavailable or unsuitable.
Abbreviations
ACCP, American College of Chest Physicians; ASCO, American Society of Clinical Oncology; ASH, American Society of Hematology; CI, confidence interval; CrCl, creatinine clearance; CRNM, clinically relevant nonmajor; D, dalteparin; DDI, drug–drug interaction; DOAC, direct oral anticoagulant; DVT, deep-vein thrombosis; E, edoxaban; ESC, European Society of Cardiology; ESMO, European Society for Medical Oncology; GI, gastrointestinal; GU, genitourinary; HR, hazard ratio; ISTH, International Society on Thrombosis and Haemostasis; ITAC, International Initiative on Thrombosis and Cancer; LMWH, low-molecular-weight heparin; MENA, Middle East and North Africa; NCCN, National Comprehensive Cancer Network; NE, not evaluated; NICE, National Institute for Health and Care Excellence; NR, not reported; PE, pulmonary embolism; PET, positron emission tomography; P-gp, P-glycoprotein; R, rivaroxaban; RCT, randomized controlled trials; RR, risk ratio; SD, standard deviation; UFH, unfractionated heparin; ULN, upper limit of normal; VKA, vitamin K antagonist; VTE, venous thromboembolism.
Acknowledgments
We thank Joanne Dalton and Veena Ekbote, MIMS, for medical writing support with financial support from Pfizer.
Author Contributions
Authors H.M.E-Z., T.O., M.A., A.W., M.M., S.B., F.H., and A.C. conceptualized the study. Authors A.W., M.M., E.D., H.J., S.M.S., F.H., and A.C. conducted the formal data analysis. The original draft was prepared by authors M.M., F.H., and A.C. All authors interpreted the data, revised and critically reviewed the article. All authors agreed on the journal to which the article was submitted. All authors gave approval to the final published version and agree to be accountable for all aspects of the work.
Funding
This research received no external funding. Medical writing support and article processing charges have been funded by Pfizer.
Disclosure
Alexander T Cohen has received contracts and consulting fees for other projects from Bristol Myers Squibb and Pfizer; payments for lectures and presentations from Bristol Myers Squibb and Pfizer; and Advisory Board fees for other projects from Bristol Myers Squibb and Pfizer, all paid to a consulting company. He also reports personal fees from AbbVie, AstraZeneca, Bayer AG, Daiichi Sankyo, and Pfizer, outside the submitted work. Mahmoud Marashi reports personal fees from Bayer, Pfizer and Sanofi during the conduct of the study; personal fees from Astra Zeneca, Janssen, Takeda, Amgen, Novartis, Roche, BMS, Novo, Sobi, Alexion, outside the submitted work. All the other authors declare no conflicts of interest in this work.
References
1. Chew HK, Wun T, Harvey D, Zhou H, White RH. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med. 2006;166(4):458–464. doi:10.1001/archinte.166.4.458
2. Cohen AT, Katholing A, Rietbrock S, Bamber L, Martinez C. Epidemiology of first and recurrent venous thromboembolism in patients with active cancer: a population-based cohort study. Thromb Haemost. 2017;117(01):57–65. doi:10.1160/TH15-08-0686
3. Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632–634. doi:10.1111/j.1538-7836.2007.02374.x
4. Khorana AA. Venous thromboembolism and prognosis in cancer. Thromb Res. 2010;125(6):490–493. doi:10.1016/j.thromres.2009.12.023
5. Lip GY, Chin BS, Blann AD. Cancer and the prothrombotic state. Lancet Oncol. 2002;3(1):27–34. doi:10.1016/S1470-2045(01)00619-2
6. Ahlbrecht J, Dickmann B, Ay C, et al. Tumor grade is associated with venous thromboembolism in patients with cancer: results from the Vienna cancer and thrombosis study. J Clin Oncol. 2012;30(31):3870–3875. doi:10.1200/JCO.2011.40.1810
7. Cronin-Fenton DP, Søndergaard F, Pedersen LA, et al. Hospitalisation for venous thromboembolism in cancer patients and the general population: a population-based cohort study in Denmark, 1997–2006. Br J Cancer. 2010;103(7):947–953. doi:10.1038/sj.bjc.6605883
8. Streiff MB. Thrombosis in the setting of cancer. Hematology. 2016;2016(1):196–205. doi:10.1182/asheducation-2016.1.196
9. Mulder FI, Horváth-Puhó E, van Es N, et al. Venous thromboembolism in cancer patients: a population-based cohort study. Blood. 2021;137(14):1959–1969. doi:10.1182/blood.2020007338
10. Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol. 2015;12(8):464–474. doi:10.1038/nrcardio.2015.83
11. Heit JA, Lahr BD, Ashrani AA, Petterson TM, Bailey KR. Predictors of venous thromboembolism recurrence, adjusted for treatments and interim exposures: a population-based case-cohort study. Thromb Res. 2015;136(2):298–307. doi:10.1016/j.thromres.2015.06.030
12. Addo-Tabiri NO, Chudasama R, Vasudeva R, et al. Black patients experience highest rates of cancer-associated venous thromboembolism. Am J Clin Oncol. 2020;43(2):94–100. doi:10.1097/COC.0000000000000639
13. Aleem A, Diab ARA, Alsaleh K, et al. Frequency, clinical pattern and outcome of thrombosis in cancer patients in Saudi Arabia. Asian Pac J Cancer Prev. 2012;13(4):1311–1315. doi:10.7314/APJCP.2012.13.4.1311
14. Omunakwe H, Nwagha T. Cancer-associated thrombosis in some African populations: a growing concern. Int J Noncommun Dis. 2016;1(2):87. doi:10.4103/2468-8827.192017
15. Prandoni P, Lensing AWA, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002;100(10):3484–3488. doi:10.1182/blood-2002-01-0108
16. Ay C, Pabinger I, Cohen AT. Cancer-associated venous thromboembolism: burden, mechanisms, and management. Thromb Haemost. 2017;117(02):219–230. doi:10.1160/TH16-08-0615
17. O’Connell C, Escalante CP, Goldhaber SZ, McBane R, Connors JM, Raskob GE. Treatment of cancer-associated venous thromboembolism with low-molecular-weight heparin or direct oral anticoagulants: patient selection, controversies, and caveats. oncologist. 2021;26(1):e8–e16. doi:10.1002/onco.13584
18. Attia D, Khorana AA. Evolving treatment options for cancer-related venous thromboembolism. JACC. 2020;2(3):441–442. doi:10.1016/j.jaccao.2020.06.003
19. Lee AYY. Anticoagulant therapy for venous thromboembolism in cancer. N Engl J Med. 2020;382(17):1650–1652. doi:10.1056/NEJMe2004220
20. Moik F, Posch F, Zielinski C, Pabinger I, Ay C. Direct oral anticoagulants compared to low‐molecular‐weight heparin for the treatment of cancer‐associated thrombosis: updated systematic review and meta‐analysis of randomized controlled trials. Res Pract Thrombo Haemost. 2020;4(4):550–561. doi:10.1002/rth2.12359
21. Yan Y-D, Ding Z, Pan M-M, et al. Net clinical benefit of direct oral anticoagulants in patients with cancer and venous thromboembolism: a systematic review and trade-off analysis. Front Cardiovas Med. 2020;7:586020. doi:10.3389/fcvm.2020.586020
22. Lee AY, Rickles FR, Julian JA, et al. Randomized comparison of low molecular weight heparin and coumarin derivatives on the survival of patients with cancer and venous thromboembolism. J Clin Oncol. 2005;23(10):2123–2129. doi:10.1200/jco.2005.03.133
23. Deitcher SR, Kessler CM, Merli G, Rigas JR, Lyons RM, Fareed J. Secondary prevention of venous thromboembolic events in patients with active cancer: enoxaparin alone versus initial enoxaparin followed by warfarin for a 180-day period. Clin Appl Thromb Hemost. 2006;12(4):389–396. doi:10.1177/1076029606293692
24. Hull RD, Pineo GF, Brant RF, et al. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am j Med. 2006;119(12):1062–1072. doi:10.1016/j.amjmed.2006.02.022
25. Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729. doi:10.1001/archinte.162.15.1729
26. Carrier M, Cameron C, Delluc A, Castellucci L, Khorana AA, Lee AYY. Efficacy and safety of anticoagulant therapy for the treatment of acute cancer-associated thrombosis: a systematic review and meta-analysis. Thromb Res. 2014;134(6):1214–1219. doi:10.1016/j.thromres.2014.09.039
27. Kahale LA, Hakoum MB, Tsolakian IG, et al. Anticoagulation for the long-term treatment of venous thromboembolism in people with cancer. Cochrane Database Syst Rev. 2018;2022(6). doi:10.1002/14651858.CD006650.pub5
28. Al-Hameed F, Al-Dorzi HM, Al Momen A, et al. Prophylaxis and treatment of venous thromboembolism in patients with cancer: the Saudi clinical practice guideline. Ann Saudi Med. 2015;35(2):95–106. doi:10.5144/0256-4947.2015.95
29. Dorgalaleh A, Beigi P, Pakjoo M, et al. Anticoagulation therapy in Iran. Ann Blood. 2019;4:26. doi:10.21037/aob.2019.11.01
30. Ay C, Beyer-Westendorf J, Pabinger I. Treatment of cancer-associated venous thromboembolism in the age of direct oral anticoagulants. Ann Oncol. 2019;30(6):897–907. doi:10.1093/annonc/mdz111
31. Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic therapy for VTE disease: second update of the CHEST guideline and expert panel report. Chest. 2021;160(6):e545–e608. doi:10.1016/j.chest.2021.07.055
32. Agnelli G, Becattini C, Meyer G, et al. Apixaban for the treatment of venous thromboembolism associated with cancer. N Engl J Med. 2020;382(17):1599–1607. doi:10.1056/NEJMoa1915103
33. McBane RD, Wysokinski WE, Le‐Rademacher JG, et al. Apixaban and dalteparin in active malignancy‐associated venous thromboembolism: the ADAM VTE trial. J Thromb Haemost. 2020;18(2):411–421. doi:10.1111/jth.14662
34. Raskob GE, van Es N, Verhamme P, et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. N Engl J Med. 2018;378(7):615–624. doi:10.1056/NEJMoa1711948
35. Young AM, Marshall A, Thirlwall J, et al. Comparison of an oral factor Xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: results of a randomized trial (SELECT-D). J Clin Oncol. 2018;36(20):2017–2023. doi:10.1200/JCO.2018.78.8034
36. Planquette B, Bertoletti L, Charles-Nelson A, et al. Rivaroxaban vs dalteparin in cancer-associated thromboembolism. Chest. 2022;161(3):781–790. doi:10.1016/j.chest.2021.09.037
37. Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2020;38(5):496–520. doi:10.1200/JCO.19.01461
38. Khorana AA, Noble S, Lee AYY, et al. Role of direct oral anticoagulants in the treatment of cancer-associated venous thromboembolism: guidance from the SSC of the ISTH. J Thromb Haemost. 2018;16(9):1891–1894. doi:10.1111/jth.14219
39. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543–603. doi:10.1093/eurheartj/ehz405
40. Farge D, Frere C, Connors JM, et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019;20(10):e566–e581. doi:10.1016/s1470-2045(19)30336-5
41. Lyman GH, Carrier M, Ay C, et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: prevention and treatment in patients with cancer. Blood Adv. 2021;5(4):927–974. doi:10.1182/bloodadvances.2020003442
42. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: cancer-associated venous thromboembolic disease, version 2.2021; 2021. Available from: https://www.nccn.org/professionals/physician_gls/default.aspx.
43. Streiff MB, Abutalib SA, Farge D, Murphy M, Connors JM, Piazza G. Update on guidelines for the management of cancer-associated thrombosis. Oncologist. 2021;26(1):e24–e40. doi:10.1002/onco.13596
44. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799–808. doi:10.1056/NEJMoa1302507
45. EINSTEIN Investigators, Bauersachs R, Berkowitz SD, et al. Oral Rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363(26):2499–2510. doi:10.1056/NEJMoa1007903
46. EINSTEIN–PE Investigators, Büller HR, Prins MH, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366(14):1287–1297. doi:10.1056/NEJMoa1113572
47. Hokusai-VTE Investigators, Büller HR, Décousu H, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. 2013;369(15):1406–1415. doi:10.1056/NEJMoa1306638
48. Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361(24):2342–2352. doi:10.1056/NEJMoa0906598
49. Schulman S, Kakkar AK, Goldhaber SZ, et al. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129(7):764–772. doi:10.1161/CIRCULATIONAHA.113.004450
50. Vedovati MC, Germini F, Agnelli G, Becattini C. Direct oral anticoagulants in patients with VTE and cancer. Chest. 2015;147(2):475–483. doi:10.1378/chest.14-0402
51. Li A, Garcia DA, Lyman GH, Carrier M. Direct oral anticoagulant (DOAC) versus low-molecular-weight heparin (LMWH) for treatment of cancer associated thrombosis (CAT): a systematic review and meta-analysis. Thromb Res. 2019;173:158–163. doi:10.1016/j.thromres.2018.02.144
52. Kim JH, Yoo C, Seo S, et al. A Phase II study to compare the safety and efficacy of direct oral anticoagulants versus subcutaneous dalteparin for cancer-associated venous thromboembolism in patients with advanced upper gastrointestinal, hepatobiliary and pancreatic cancer: PRIORITY. Cancers. 2022;14(3). doi:10.3390/cancers14030559
53. White RH, Ginsberg JS. Low-molecular-weight heparins: are they all the same? Review Br J Haematol. 2003;121(1):12–20. doi:10.1046/j.1365-2141.2003.04196.x
54. Schrag D, Uno H, Rosovsky R, et al. Direct oral anticoagulants vs low-molecular-weight heparin and recurrent VTE in patients with cancer: a randomized clinical trial. JAMA. 2023;329(22):1924–1933. doi:10.1001/jama.2023.7843
55. Athanazio RA, Ceresetto JM, Marfil Rivera LJ, et al. Direct oral anticoagulants for the treatment of cancer-associated venous thromboembolism: a Latin American perspective. Clin Appl Thromb Hemost. 2022;28:10760296221082988. doi:10.1177/10760296221082988
56. Lee LH, Danchaivijitr P, Uaprasert N, et al. Safe and effective treatment of venous thromboembolism associated with cancer: focus on direct oral anticoagulants in Asian patients. Exp Hematol Oncol. 2022;11(1):79. doi:10.1186/s40164-022-00331-9
57. Kraaijpoel N, Di Nisio M, Mulder F, et al. Clinical impact of bleeding in cancer-associated venous thromboembolism: results from the Hokusai VTE cancer study. Thromb Haemost. 2018;118(08):1439–1449. doi:10.1055/s-0038-1667001
58. Ageno W, Vedovati MC, Cohen A, et al. Bleeding with apixaban and dalteparin in patients with cancer-associated venous thromboembolism: results from the Caravaggio study. Thromb Haemost. 2021;121(05):616–624. doi:10.1055/s-0040-1720975
59. Sabatino J, De Rosa S, Polimeni A, Sorrentino S, Indolfi C. Direct oral anticoagulants in patients with active cancer. JACC. 2020;2(3):428–440. doi:10.1016/j.jaccao.2020.06.001
60. Cohen A, Keshishian A, Lee T, et al. Effectiveness and safety of apixaban, low-molecular-weight heparin, and warfarin among venous thromboembolism patients with active cancer: a U.S. claims data analysis. Thromb Haemost. 2021;121(03):383–395. doi:10.1055/s-0040-1718728
61. Cohen A, Keshishian A, Lee T, et al. Effectiveness and safety of apixaban, low-molecular weight heparin, and warfarin among high-risk subgroups of venous thromboembolism patients with active cancer. Eur Heart J. 2020;41(Supplement_2):ehaa946. doi:10.1093/ehjci/ehaa946.3369
62. Giustozzi M, Agnelli G, Del Toro-Cervera J, et al. Direct oral anticoagulants for the treatment of acute venous thromboembolism associated with cancer: a systematic review and meta-analysis. Thromb Haemost. 2020;120(07):1128–1136. doi:10.1055/s-0040-1712098
63. Haykal T, Zayed Y, Deliwala S, et al. Direct oral anticoagulant versus low-molecular-weight heparin for treatment of venous thromboembolism in cancer patients: an updated meta-analysis of randomized controlled trials. Thromb Res. 2020;194:57–65. doi:10.1016/j.thromres.2020.06.025
64. Mulder FI, Bosch FTM, Young AM, et al. Direct oral anticoagulants for cancer-associated venous thromboembolism: a systematic review and meta-analysis. Blood. 2020;136(12):1433–1441. doi:10.1182/blood.2020005819
65. Saleem M, Osman M, Farid S, et al. Direct oral anticoagulants for treatment of venous thromboembolism associated with cancer: a systematic review and meta-analysis. Clin Oncol Res. 2020:3(6)1–7. doi:10.31487/j.COR.2020.06.14
66. Tao DL, Olson SR, DeLoughery TG, Shatzel JJ. The efficacy and safety of DOACs versus LMWH for cancer‐associated thrombosis: a systematic review and meta‐analysis. Eur J Haematol. 2020;105(3):360–362. doi:10.1111/ejh.13453
67. Haykal T, Adam S, Ortel TL. Meta-analysis fever in the wake of CARAVAGGIO. Thromb Res. 2020;196:141–142. doi:10.1016/j.thromres.2020.08.036
68. Alsheef M, Bazarbashi S, Warsi A, et al. The Saudi consensus for the management of cancer-associated thromboembolism: a modified Delphi-based study. TH Open. 2023;7(1):e14–e29. doi:10.1055/s-0042-1758856
69. National Institute for Health and Care Excellence. Venous thromboembolic diseases: diagnosis, management and thrombophilia testing, NICE Guideline NG158. 2020. Available from: https://www.nice.org.uk/guidance/ng158.
70. Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO guideline update. J Clin Oncol. 2023;41(16):3063–3071. doi:10.1200/jco.23.00294
71. Farge D, Frere C, Connors JM, et al. 2022 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer, including patients with COVID-19. Lancet Oncol. 2022;23(7):e334–e347. doi:10.1016/s1470-2045(22)00160-7
72. Falanga A, Ay C, Di Nisio M, et al. Venous thromboembolism in cancer patients: ESMO clinical practice guideline. Ann Oncol. 2023;34(5):452–467. doi:10.1016/j.annonc.2022.12.014
73. Vedovati MC, Giustozzi M, Becattini C. Venous thromboembolism and cancer: current and future role of direct-acting oral anticoagulants. Thromb Res. 2019;177:33–41. doi:10.1016/j.thromres.2019.02.031
74. Kahn SR, Springmann V, Schulman S, et al. Management and adherence to VTE treatment guidelines in a national prospective cohort study in the Canadian outpatient setting: the Recovery study. Thromb Haemost. 2012;108(09):493–498. doi:10.1160/TH12-03-0169
75. van der Wall SJ, Klok FA, den Exter PL, et al. Continuation of low-molecular-weight heparin treatment for cancer-related venous thromboembolism: a prospective cohort study in daily clinical practice. J Thromb Haemost. 2017;15(1):74–79. doi:10.1111/jth.13563
76. McBane R, Loprinzi C, Dakhil S, et al. Extending venous thromboembolism secondary prevention with apixaban in cancer patients: EVE trial. Eur J Haematol. 2020;104(2):88–96.
77. Connors JM. NATF cancer-associated thrombosis project: introduction. Oncologist. 2021;26(1):e1–e1. doi:10.1002/onco.13615
78. Wang T-F, Billett HH, Connors JM, Soff GA. Approach to cancer-associated thrombosis: challenging situations and knowledge gaps. Oncologist. 2021;26(1):e17–e23. doi:10.1002/onco.13570
79. Clemens A, Noack H, Brueckmann M, Lip GYH. Twice- or once-daily dosing of novel oral anticoagulants for stroke prevention: a fixed-effects meta-analysis with predefined heterogeneity quality criteria. PLoS One. 2014;9(6):e99276. doi:10.1371/journal.pone.0099276
80. Ageno W, Beyer-Westendorf J, Rubboli A. Once- versus twice-daily direct oral anticoagulants in non-valvular atrial fibrillation. Expert Opin Pharmacother. 2017;18(13):1325–1332. doi:10.1080/14656566.2017.1361405
81. Sepanlou SG, Malekzadeh F, Delavari F, et al. Burden of gastrointestinal and liver diseases in Middle East and North Africa: results of global burden of diseases study from 1990 to 2010. Middle East J Dig Dis. 2015;7(4):201–215.
82. Adeloye D, Harhay MO, Ayepola OO, et al. Estimate of the incidence of bladder cancer in Africa: a systematic review and Bayesian meta-analysis. Int J Urol. 2019;26(1):102–112. doi:10.1111/iju.13824
83. Richters A, Aben KKH, Kiemeney LALM. The global burden of urinary bladder cancer: an update. World J Urol. 2020;38(8):1895–1904. doi:10.1007/s00345-019-02984-4
84. Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of bladder cancer. Med Sci. 2020;8(1):15. doi:10.3390/medsci8010015
85. Carney BJ, Uhlmann EJ, Puligandla M, et al. Intracranial hemorrhage with direct oral anticoagulants in patients with brain tumors. J Thromb Haemost. 2019;17(1):72–76. doi:10.1111/jth.14336
86. Cohen A, Noxon V, Dhamane A, et al. Effectiveness and safety of anticoagulants among venous thromboembolism cancer patients with and without brain cancer. Thromb Res. 2023;226:117–126. doi:10.1016/j.thromres.2023.04.009
87. Gelosa P, Castiglioni L, Tenconi M, et al. Pharmacokinetic drug interactions of the non-vitamin K antagonist oral anticoagulants (NOACs). Pharmacol Res. 2018;135:60–79. doi:10.1016/j.phrs.2018.07.016
88. Verso M, Munoz A, Bauersachs R, et al. Effects of concomitant administration of anticancer agents and apixaban or dalteparin on recurrence and bleeding in patients with cancer-associated venous thromboembolism. Eur J Cancer. 2021;148:371–381. doi:10.1016/j.ejca.2021.02.026
89. Al-Kindi SG, Oliveira GH. Prevalence of preexisting cardiovascular disease in patients with different types of cancer. Mayo Clin Proc. 2016;91(1):81–83. doi:10.1016/j.mayocp.2015.09.009
90. Mamas MA, Brown S-A, Sun LY. Coronary artery disease in patients with cancer: it’s always the small pieces that make the bigger picture. Mayo Clin Proc. 2020;95(9):1819–1821. doi:10.1016/j.mayocp.2020.07.006
91. Cohen A, Agnelli G, Buller H, et al. Characteristics and outcomes in patients with venous thromboembolism taking concomitant anti-platelet agents and anticoagulants in the AMPLIFY trial. Thromb Haemost. 2019;119(03):461–466. doi:10.1055/s-0038-1676983
92. Lopes RD, Heizer G, Aronson R, et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N Engl J Med. 2019;380(16):1509–1524. doi:10.1056/NEJMoa1817083
93. Potere N, Di Nisio M, Porreca E, et al. Apixaban thromboprophylaxis in ambulatory patients with cancer and obesity: insights from the AVERT trial. Thromb Res. 2023;226:82–85. doi:10.1016/j.thromres.2023.04.015
94. Giorgi-Pierfranceschi M, Lopez-Nunez JJ, Monreal M, et al. Morbid obesity and mortality in patients with VTE: findings from real-life clinical practice. Chest. 2020;157(6):1617–1625. doi:10.1016/j.chest.2019.12.040
95. Jegatheswaran J, Hundemer GL, Massicotte-Azarniouch D, Sood MM. Anticoagulation in patients with advanced chronic kidney disease: walking the fine line between benefit and harm. Can J Cardiol. 2019;35(9):1241–1255. doi:10.1016/j.cjca.2019.07.001
96. Harfouche M, Chemaitelly H, Kouyoumjian SP, et al. Hepatitis C virus viremic rate in the Middle East and North Africa: systematic synthesis, meta-analyses, and meta-regressions. PLoS One. 2017;12(10):e0187177. doi:10.1371/journal.pone.0187177
97. Poortahmasebi V, Baghi HB. Living in the shadows of hepatitis. Lancet Infect Dis. 2019;19(11):1171–1172. doi:10.1016/S1473-3099(19)30534-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.