")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
The Role of Reflectance Confocal Microscopy in the Diagnosis and Therapeutic Evaluation of Rare Disease Eosinophilic Pustular Folliculitis
Authors Li Y , Wu M, Hu X, Chen G, Yao X, Zhou X, Lu J
Received 21 June 2023
Accepted for publication 20 August 2023
Published 25 August 2023 Volume 2023:16 Pages 2309—2314
DOI https://doi.org/10.2147/CCID.S423973
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Yuan Li,1,2,* Miaoting Wu,1,* Xiaohuan Hu,1,* Gaihe Chen,1,* Xiaojuan Yao,1 Xin Zhou,3 Jiejie Lu1
1Department of Cosmetic Dermatology, The Fifth People’s Hospital of Hainan Province, Haikou, Hainan, People’s Republic of China; 2Department of Dermatology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 3Medical Administration Department, The Fifth People’s Hospital of Hainan Province, Haikou, Hainan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiejie Lu, Department of Cosmetic Dermatology, The Fifth People’s Hospital of Hainan Province, No. 8 Longhua Road, Longhua District, Haikou, Hainan, 570100, People’s Republic of China, Email [email protected] Xin Zhou, Medical Administration Department, The Fifth People’s Hospital of Hainan Province, No. 8 Longhua Road, Longhua District, Haikou, Hainan, 570100, People’s Republic of China, Email [email protected]
Abstract: Eosinophilic pustular folliculitis (EPF) is a rare skin disease for which the gold standard of diagnosis relies on the invasive examination of pathological tissue sections. However, due to its invasive nature, many patients tend to refuse this diagnostic test. In such situations, reflectance confocal microscopy (RCM) can be a valuable diagnosis tool. Reflectance confocal microscopy (RCM) can accurately identify the specific structures for biopsy and provide objective imaging data to evaluate clinical symptoms following treatment. Therefore, we present a case report demonstrating the utility of RCM in diagnosing and assessing the treatment of the rare disease EPF for reference.
Keywords: eosinophilic pustular folliculitis, minocycline, reflectance confocal microscopy, non-invasive detection
Introduction
Eosinophilic pustular folliculitis (EPF), also known as Ofuji’s disease, was initially described by Ofuji et al in 19701 Xin. EPF presents as a chronic, pruritic, sterile skin condition with an unclear aetiology, considered a non-specific reaction. The disease typically follows a chronic course and is more prevalent among young men.2 The hallmark of a typical skin lesion is a whirlpool or creeping red patch, which eventually evolves into red, pinhead-sized follicular papules and pustules.3 These lesions may be clustered or arranged circularly, displaying clear boundaries. As the centre regresses, the skin lesions spread outward, resulting in residual pigmentation.4
The disease frequently affects seborrheic areas, such as the face. EPF may be accompanied by varying degrees of pruritus and tends to resolve spontaneously over time, but recurrences are possible.5 The gold standard for diagnosis relies on invasive histopathological examination; however, reflectance confocal microscopy (RCM) offers a non-invasive alternative that can readily suggest the disease, aiding in accurate diagnosis, avoiding misdiagnosis, and facilitating the precise localization of corresponding structures for biopsy.6 Moreover, RCM provides objective imaging data to evaluate clinical symptoms after treatment.7 Therefore, we present a case report that utilizes RCM for diagnosing and assessing the effectiveness of treatment for the rare disease, eosinophilic pustular folliculitis.
Case Presentation
A 22-year-old male patient presented with facial erythema and itching for two months. Over time, he developed multiple erythematous patches on his face, accompanied by mild pruritus. The patient had previously sought medical attention at an external hospital, where a fungal microscopy examination yielded negative results, and he was diagnosed with “eczema”. Subsequently, he underwent various treatments, including “moisturizing and anti-itch capsules”, “ebastine tablets”, “dichlorphenamide suspension”, multiple injections of “compound betamethasone sodium phosphate”, and topical application of “dermadex cream”, “terbinafine cream”, and “hydrocortisone cream”. Despite these interventions, the facial skin lesions persisted. Upon presenting to our hospital, the patient was diagnosed with “eosinophilic pustular folliculitis”. An initial attempt to treat the condition with “indomethacin enteric-coated tablets” resulted in the patient experiencing dizziness and nausea.
Consequently, he discontinued this medication after three doses and switched to “minocycline capsules” instead. The facial erythema gradually improved throughout his treatment with minocycline capsules, and the patient continued taking the medication without experiencing any dizziness or nausea. Notably, the patient did not report any accompanying symptoms such as fever, cough, fatigue, or weight loss. He had no significant medical history, was unmarried, and had an unremarkable family medical history.
Physical examination revealed no abnormalities in various systems, and dermatological analysis unveiled patchy dark brown plaques on the face, with several green bean-sized follicular red papules on top (Figure 1A). Pathological examination of the skin lesions demonstrated excessive keratinization, patchy mixed inflammatory cell infiltration in the superficial dermis, dense infiltration of lymphocytes, and numerous eosinophils around some hair follicles and sebaceous glands, with partial destruction of structures (Figure 2A and B). Direct immunofluorescence and azan staining yielded negative results. Dermoscopic examination showed unclear boundaries of the lesion, irregular patches or clusters of red blood vessels on the dark red base, a few white scales on top, and follicular keratosis (Figure 3A). Direct microscopy and culture of facial skin flakes for fungi were also negative. The RCM examination of the facial area revealed hyperkeratosis and an abundant inflammatory infiltrate in the superficial dermis, composed of numerous sparse hyper-reflective cells.
 |
Figure 1 (A) The image shows facial patchy brownish-black spots, with several lentil-sized follicular red papules distributed on top. (B) The skin lesion on the posterior area has regressed after treatment. |
 |
Figure 2 (A) The image displays hyperkeratosis, with lamellar mixed inflammatory cell infiltration (indicated by black arrows) in the superficial dermis (HE, 40× magnification). (B) The image reveals dense lymphocytic and eosinophilic infiltration (indicated by black arrows) around hair follicles and sebaceous glands, disrupting some structures (HE, 200× magnification). |
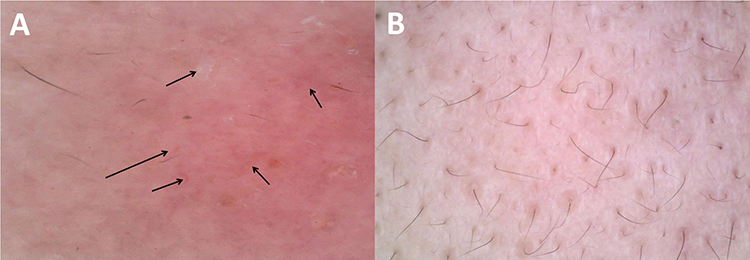 |
Figure 3 (A) The lesions are ill-defined, with irregular sheets or clusters of punctate vessels (indicated by black arrows) on a dark red base, covered with a few white scales, and seen as follicular corns. (B) The above dermoscopic manifestations subsided after treatment. |
Furthermore, a hyper-reflective inflammatory infiltrate was observed around specific hair follicles and sebaceous glands (Figure 4A). Laboratory and auxiliary examinations showed negative results for syphilis antibody, HIV antibody, antinuclear antibody, and antineutrophil cytoplasmic antibody. The patient’s white blood cell count was 11.6 × 10^9/L, with an absolute neutrophil count of 7.81 × 10^9/L and an absolute monocyte count of 0.61 × 10^9/L. Liver and kidney function tests were found to be within the normal range.
 |
Figure 4 (A) A sizeable inflammatory infiltrate in the superficial dermis, consisting of many sparse hyper-reflective cells. Additionally, a hyperreflective inflammatory infiltrate (indicated by red arrows) was observed around specific hair follicles and sebaceous glands. (B) After treatment, the hair follicle and the massive inflammatory cell mass-like infiltration around the hair follicle disappeared. |
In summary, the diagnosis was eosinophilic pustular folliculitis (classic). The patient was treated with minocycline 100mg/d orally daily; most of the erythema on the face disappeared, and the bumps dried up after ten days of treatment (Figures 1B, 3B and 4B). The eosinophilic granulocytes of the peripheral blood were restored to normal in a repeat examination. The minocycline was continued to be used at 100 mg/d. The medication was discontinued after the symptoms subsided after one month of treatment, and the patient was not seen to have any recurrence at three months of follow-up.
Discussion
Currently, there are three main eosinophilic pustular folliculitis (EPF) types: classic EPF, immunosuppression-related EPF, and infantile EPF. However, some scholars have further divided EPF into six types: traditional, HIV-related, childish, palmoplantar, drug-related, and tumour-related.8 It is worth noting that there is no histopathological difference between the different types, suggesting that the variations may arise from different etiologies.9 Based on the patient’s medical history, clinical signs, and auxiliary examinations, this article considers EPF classic eosinophilic pustular folliculitis. This condition can increase the percentage and count of eosinophils in the patient’s blood routine, especially during the acute phase. Furthermore, white blood cells, erythrocyte sedimentation rate, C-reactive protein, and serum IgE levels may also elevate.10 Due to the patient’s initial misdiagnosis as “eczema” and the lack of Laboratory and pathological examinations during the early stages of the disease, along with multiple treatments involving glucocorticoids, the eosinophil count did not show abnormalities in the laboratory blood routine examination after the patient was referred to our hospital later in the course of the disease.
Therefore, it is crucial to differentiate this disease from eczema. Erythema, papules, and scales typically characterize eczema. Dermoscopically, eczema exhibits a reddish-brown background with a focal distribution of punctate blood vessels, and the scales are predominantly yellowish and appear in a sheet-like pattern.11 When using reflectance confocal microscopy (RCM) for diagnosis, eczema is distinguished by hyperkeratosis, prolonged epidermal protrusions, oedema of the stratum spinosum, and small blisters in cases of inflammation. Additionally, there is evident capillary dilation and a substantial number of infiltrating inflammatory cells in the superficial dermis, leading to a non-specific inflammatory pattern.12 However, it is essential to acknowledge that RCM features can indicate other conditions. For instance, in psoriasis, RCM shows evenly distributed hyperkeratosis with rounded or round-like, unevenly refracted granules within the stratum corneum. Thickening of the stratum spinosum is observed, along with clusters of polymorphonuclear cells visible within the epidermis as higher refracted granules, characterized by a sense of fluidity or shimmering on dynamic scanning (referred to as Munro microabscesses). Multiple blood vessels, displaying tortuous dilatation of superficial dermal blood vessels, can also be seen in the dermal papillae. In some patients, infiltration of inflammatory cells in the superficial dermis is also present. Additionally, tumour-like granuloma under RCM examination shows round, large polymorphic cells scattered in the epidermis. In the case of discoid lupus erythematosus, RCM manifests as superficial dermal inflammatory cell infiltration, with inflammatory cells scattered within the distribution of collagen fibers.13,14
Dermoscopy and Reflectance Confocal Microscopy (RCM) are becoming increasingly valuable as non-invasive detection tools in inflammatory skin diseases. Dermoscopy allows visualization of vascular morphology and distribution, making it a crucial tool in diagnosing such skin conditions.15 RCM utilizes skin structures with distinct reflection coefficients for laser light, enabling real-time and dynamic scanning, thus assisting in diagnosing various dermatological diseases. Its reproducible operation and non-invasive nature allow the observation of cells and tissues in their physiological state, providing valuable insights into their actual performance.16 Moreover, RCM allows real-time dynamic monitoring and multiple imaging of the same lesion at different times, facilitating follow-up observations.17 The skin CT scan results in this patient were in excellent agreement with the pathologic findings. The skin CT revealed hyperkeratosis, with the superficial dermis showing a rich inflammatory infiltrate composed of numerous sparse hyper-reflective cells. Additionally, a hyper-reflective inflammatory infiltrate was observed around some hair follicles and sebaceous glands, which concurred with the structures observed in the pathological examination.
Our findings demonstrate that reflectance confocal microscopy (RCM) holds significant diagnostic and therapeutic value in EPF. When imaged in RCM, closed pimples display well-defined funnel sections with thick bright borders, while open spots exhibit large funiculi and hyperreflective irregular edges filled with amorphous material.18 Additionally, papules imaged in RCM show epidermal spines with a rich inflammatory infiltrate comprising numerous sparse hyperreflective cells. In the case of pimples, RCM reveals the presence of a hyperreflective organized inflammatory infiltrate within the pustule lumen.19 By utilizing RCM based on the observed papules before treatment and evaluating pustule morphology in conjunction with the clinical presentation, the disease can be easily diagnosed, reducing the risk of misdiagnosis. After treatment, RCM imaging of papules and pustules significantly decreases, providing objective imaging data to assess the patient’s clinical symptoms (Figure 4B). Furthermore, to confirm the diagnosis, it is essential to identify the exact follicle and perifollicular inflammatory infiltration. A skin biopsy may sometimes fail to achieve this due to the inability to cut into follicular structures. In contrast, RCM can accurately locate the corresponding areas for biopsy, providing a valuable advantage in the diagnostic process.20
There are various treatment options available for this disease. Existing literature suggests that EPF can be managed with glucocorticoids, tetracyclines (such as doxycycline or minocycline), indomethacin, Tripterygium wilfordii, avian A, tacrolimus, and ultraviolet rays. Tetracyclines (specifically doxycycline or minocycline) are considered a second-line treatment for classic EPF.21 In this case, the patient’s treatment was adjusted to second-line therapy with minocycline at a daily oral dose of 100mg due to intolerance to the initial treatment with indomethacin. Notably, the patient demonstrated a significant improvement in response to this new treatment, as evidenced by the remarkable changes observed in Figures 1B, 3 B and 4B. However, it is essential to closely monitor the patient’s long-term response to this therapy, which necessitates further follow-up.
Conclusions
In conclusion, EPF is a relatively uncommon skin disease that can be easily misdiagnosed based solely on clinical presentation. Therefore, a comprehensive approach, considering clinical manifestations, laboratory tests, and histopathology, is crucial for accurate diagnosis.
In recent years, imaging technology has emerged as a valuable tool in diagnosing and prognosing the disease. Utilizing imaging techniques, such as reflectance confocal microscopy (RCM), can provide specific insights and aid in the diagnosis without the need for invasive procedures, thus reducing potential harm to patients. The non-invasive nature of these imaging methods makes them particularly advantageous in evaluating and managing EPF.
Data Sharing Statement
The data supporting this study’s findings are available from the Xin Zhou and Jiejie Lu upon reasonable request.
Ethics Statement
The publication of images was included in the patient’s consent to publish the case. The Hospital Ethics Committees of the Fifth People’s Hospital of Hainan Province approved to publish the case details.
Patient Consent Statement
The authors certify that they have obtained all appropriate patient consent forms for the use of patient photographs and data received.
Acknowledgment
We are thankful to our patient for her support and cooperation.
Funding
This project is supported by Hainan Province Clinical Medical Center.
Disclosure
Yuan Li, Miaoting Wu, Xiaohuan Hu and Gaihe Chen are the co-first authors of this study. Jiejie Lu and Xin Zhou are co-corresponding authors. The authors have no conflicts of interest to declare.
References
1. Shi W, Lu Y, Zhou F, He H, Jiang J, Xue X. Infantile Eosinophilic pustular folliculitis in a child aged 7 years: a case report. Clin Cosmet Investig Dermatol. 2023;16:717–720. doi:10.2147/CCID.S404316
2. Li Y, Nie R, Cao X, Wan C. Classic Eosinophilic pustular folliculitis in an immunocompetent patient with syphilis: are they related? Clin Cosmet Investig Dermatol. 2023;16:67–70. doi:10.2147/CCID.S393841
3. Sufyan W, Tan KB, Wong ST, Lee YS. Eosinophilic pustular folliculitis. Arch Pathol Lab Med. 2007;131(10):1598–1601. doi:10.5858/2007-131-1598-EPF
4. Kim BR, Kim M, Choi CW, Cho S, Youn SW. Predictive model for differential diagnosis of inflammatory papular dermatoses of the face. Ann Dermatol. 2020;32(4):298–305. doi:10.5021/ad.2020.32.4.298
5. Marasca C, Ruggiero A, Fabbrocini G, Megna M. A case of ofuji disease successfully treated with the combination of low-dose indomethacin and topical tacrolimus. Case Rep Dermatol. 2020;12(2):155–158. doi:10.1159/000509176
6. Guida S, Pellacani G, Ciardo S, Longo C. Reflectance confocal microscopy of aging skin and skin cancer. Dermatol Pract Concept. 2021;11(3):e2021068. doi:10.5826/dpc.1103a68
7. Csuka EA, Ward SC, Ekelem C, Csuka DA, Ardigò M, Mesinkovska NA. Reflectance confocal microscopy, optical coherence tomography, and multiphoton microscopy in inflammatory skin disease diagnosis. Lasers Surg Med. 2021;53(6):776–797. doi:10.1002/lsm.23386
8. Long H, Zhang G, Wang L, Lu Q. Eosinophilic skin diseases: a comprehensive review. Clin Rev Allergy Immunol. 2016;50(2):189–213. doi:10.1007/s12016-015-8485-8
9. Marzano AV, Genovese G. Eosinophilic dermatoses: recognition and management. Am J Clin Dermatol. 2020;21(4):525–539. doi:10.1007/s40257-020-00520-4
10. Ashworth J, Nogueira M, Freitas E, Ferreira L, Tente D, Machado S. Eosinophilic pustular folliculitis in infancy: a rare disease. Eur J Dermatol. 2022;32(6):812–814. English. doi:10.1684/ejd.2022.4384
11. Adabala SS, Doshi BR, Manjunathswamy BS. A cross-sectional study to assess the role of dermoscopy in differentiating palmar psoriasis, chronic hand eczema, and eczema in psoriatico. Indian Dermatol Online J. 2022;13(1):78–85. doi:10.4103/idoj.IDOJ_782_20
12. Hoogedoorn L, Peppelman M, van de Kerkhof PC, van Erp PE, Gerritsen MJ. The value of in vivo reflectance confocal microscopy in the diagnosis and monitoring of inflammatory and infectious skin diseases: a systematic review. Br J Dermatol. 2015;172(5):1222–1248. doi:10.1111/bjd.13499
13. Braghiroli NF, Sugerik S, Freitas LAR, Oliviero M, Rabinovitz H. The skin through reflectance confocal microscopy - historical background, technical principles, and its correlation with histopathology. An Bras Dermatol. 2022;97(6):697–703. doi:10.1016/j.abd.2021.10.010
14. Shahriari N, Grant-Kels JM, Rabinovitz H, Oliviero M, Scope A. Reflectance confocal microscopy: principles, basic terminology, clinical indications, limitations, and practical considerations. J Am Acad Dermatol. 2021;84(1):1–14. doi:10.1016/j.jaad.2020.05.153
15. Grazzini M, Stanganelli I, Rossari S, et al. Dermoscopy, confocal laser microscopy, and hi-tech evaluation of vascular skin lesions: diagnostic and therapeutic perspectives. Dermatol Ther. 2012;25(4):297–303. doi:10.1111/j.1529-8019.2012.01547.x
16. Guida S, Longhitano S, Ardigò M, et al. Dermoscopy, confocal microscopy and optical coherence tomography features of main inflammatory and autoimmune skin diseases: a systematic review. Australas J Dermatol. 2022;63(1):15–26. doi:10.1111/ajd.13695
17. Lu Q, Jiang G. Progress in the application of reflectance confocal microscopy in dermatology. Postepy Dermatol Alergol. 2021;38(5):709–715. doi:10.5114/ada.2021.110077
18. Alma A, Sticchi A, Chello C, et al. Dermoscopy, reflectance confocal microscopy and optical coherence tomography features of acne: a systematic review. J Clin Med. 2022;11(7):1783. doi:10.3390/jcm11071783
19. Rossi E, Mandel VD, Paganelli A, Farnetani F, Pellacani G. Plasma exeresis for active acne vulgaris: clinical and in vivo microscopic documentation of treatment efficacy by means of reflectance confocal microscopy. Skin Res Technol. 2018;24(3):522–524. doi:10.1111/srt.12452
20. Heibel HD, Hooey L, Cockerell CJ. A review of non-invasive techniques for skin cancer detection in dermatology. Am J Clin Dermatol. 2020;21(4):513–524. doi:10.1007/s40257-020-00517-z
21. Brito FF, Martelli AC, Cavalcante ML, Pinto AC, Itimura G, Soares CT. Ofuji disease: a rare dermatosis and its challenging therapeutic approach. An Bras Dermatol. 2016;91(5):646–648. doi:10.1590/abd1806-4841.20164778
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.