")
Back to Journals » Nursing: Research and Reviews » Volume 13
Time to Develop Phlebitis and Its Predictors Among Patients with Peripheral Intravenous Cannula at Public Hospitals of Bahir Dar City, Amhara, Ethiopia, 2022: A Prospective Observational Study
Authors Lidetu Bayeh T , Yirga Birhie A , Mesfin Alene E
Received 26 March 2023
Accepted for publication 17 November 2023
Published 27 November 2023 Volume 2023:13 Pages 51—60
DOI https://doi.org/10.2147/NRR.S414331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pariya Fazeli
Tadios Lidetu Bayeh,1 Alemshet Yirga Birhie,1 Elisabet Mesfin Alene2
1Department of Adult Health Nursing, Bahir Dar University, Bahir Dar, Ethiopia; 2Department of Nursing, Felege Hiwot Referral Hospital, Bahir Dar, Ethiopia
Correspondence: Tadios Lidetu Bayeh, P.O. Box 1072 Bahir Dar, Bahir Dar, Ethiopia, Tel +251955185671, Email [email protected]
Background: Phlebitis is an inflammation of vein and the common complication of peripheral intravenous cannula. Phlebitis leads patient to sepsis, pulmonary embolism and other serious complications that increase patient morbidity and mortality. Phlebitis-related literature is scarce in Ethiopia. Therefore, the incidence and predictors of phlebitis were the focus of this study.
Methods and Materials: An institution-based prospective observational study was carried out at public hospitals of Bahir Dar city. Four hundred sixty-two patients with peripheral intravenous cannulas who were admitted to the medical ward were selected using a systematic random sampling technique. Jackson’s Visual Infusion Phlebitis Scoring system was used to determine the presence of phlebitis. We used Cox proportional hazards regression model, to identify significant predictors of phlebitis.
Results: In this study, 462 patients included, and 171 (37.01%) of them developed phlebitis. The median survival time of phlebitis was six days. Patients whose age group > 60 years had low probability to develop phlebitis (AHR = 0.49, 95% CI 0.29– 0.82), whereas chronic-diseases (AHR = 1.50, 95% CI 1.09– 2.07), drugs and blood administer in one vein (AHR = 2.03, 95% CI 1.44– 2.86), inappropriate cannula dressing (AHR = 1.81, 95% CI 1.31– 2.51), large cannula size (AHR = 1.52, 95% CI 1.08– 2.15) and longer cannula dwelling time (AHR = 7.39, 95% CI 4.12– 13.32) had high probability to develop phlebitis.
Conclusion: The post-peripheral intravenous cannula phlebitis that frequently affects hospitalized cannulated patients requires particular attention and follow-up for cannulated patients with known risk factors.
Keywords: time, incidence, predictors, phlebitis, cannula, patients
Introduction
Post peripheral intravenous cannula (PIVC) is a device inserted into the peripheral veins for the purpose of administration of intravenous fluid, medication and blood.1 Post peripheral intravenous cannula phlebitis is an inflammation of the vein, which is characterized by pain, erythema, edema, induration and palpable of the vein and pyrexia.1 Most PIVC is done by a nurse practitioner, which accounts for 80% of all cannulation that is done at health facilities.2 Up to 70% of hospitalized patients using PIVC acquire phlebitis, which is a common complication of the procedure. Phlebitis usually takes four days to develop.3,4
Phlebitis can be caused on by a variety of mechanical, chemical, or bacterial factors and may appear alone or in combination with any of the other PIVC problems.5 The majority of medical facilities do not strictly follow the correct PIVC procedure.6,7 Hence, the majority of patients with PIVC are at risk of developing phlebitis.8 Phlebitis manifests in four grades, which are grade one (erythema around the puncture site, with or without local pain), grade two (pain at the puncture site with erythema and/or edema and hardening), grade three (pain at the puncture site with erythema, hardening and a palpable venous cord), and grade four (pain at the puncture site with erythema, hardening and a palpable venous cord that is >1 cm, with purulent discharge).9–12
The acceptable phlebitis incidence rate, according to the Infusion Nurses Society, should be five percent or below.9 But still, 70% of hospitalized patients acquired phlebitis following the use of PIVC.6,9 There is evidence that showed the incidence of phlebitis varies by country. According to studies, the incidence of phlebitis was 17% in Australia, 18% in Saudi Arabia, 10% in Brazil, 52% in Tunisia, and 70% in Ethiopia.6,13–16
With the insertion of PIVC, phlebitis can develop for a number of causes. The main causes are comorbidities, high cannula gauge sizes, and protracted cannula dwell periods.6 The size of the cannula has an impact on the vein’s physiology. The risk of phlebitis can be increased by choosing a cannula diameter that is too large.4,17 The risk of phlebitis is considerably reduced by properly stabilizing and securing the insertion site of PIVC.4,10,18 The administration of medications raises the risk that individuals will experience phlebitis after a cannulation.4,18 The problems of phlebitis are currently being addressed globally with various prevention and management strategies.19 The guideline states that PIVC should be removed if it has been in place for more than 96 hours because the risk of phlebitis increases with time.10,20
Despite various phlebitis prevention and management strategies, phlebitis remains a serious challenge in clinical settings. In Ethiopia, many patients that received PIVC suffered by phlebitis. Little evidence has been done on the incidence of phlebitis in Ethiopia. Therefore, this study was aimed to determine the incidence and identify predictors of phlebitis among patients with PIVC.
Methods and Materials
Study Design
Institutional-based prospective observational study design was conducted.
Study Area and Period
This study was conducted at public hospitals of Bahir Dar city. Bahir Dar city is the capital city of Amhara national regional state. In the city, there are three public hospitals. Those are Felege-Hiwot Referral Hospital, Tibebe Gion Compressive Specialized Teaching Hospital, and Adisalem Primary Hospital. This study was conducted from May/02 to June/17/2022.
Population
Patients admitted to medical ward with PIVC at public hospitals of Bahir Dar city.
Sample Size, Technique and Procedure
The sample size was calculated using two population-proportion formulas, confidence level = 95%, power = 80%. In considering of the adequate sample size and feasibility issues, the final sample size was 468. There are three hospitals in Bahir Dar city Administration from which the samples were taken. The total sample size was allocated to each hospital proportionally based on the number of patients they have. Then, patients were selected using systematic random sampling methods from each hospital.
Operational Definition
Event: Patients acquired phlebitis during the follow-up time.
Censored: Patients not acquired phlebitis during the follow-up time.
Follow-up period: The time interval between insertions of PIVC to the occurrence of phlebitis or removal time of the cannula.
Phlebitis: Phlebitis was diagnosed based on the Jackson’s Visual Infusion Phlebitis Scoring System, which means that patients have a score of two or higher.9–12
Good vein (visibility): The vein could be simple to see, visible, and large enough to accommodate an adult cannula.11,21,22
Appropriate cannula site dressing: Covering the site of the cannula insertion with an adhesive plaster in a V shape and applying an additional adhesive plaster over it at an angle of 180 degrees without tourniqueting the site a complete rotation.11
Data Collection Tools and Procedure
Interviewer-based structured questionnaires were adapted from validated and standardized existing tools to measure peripheral intravenous catheter-induced phlebitis. The PIVC insertion technique at hospitals is standardized based on the hospital policy and infection control protocol for procedures. Observational checklists were used to collect patient-related and PIVC-related characteristics. Three BSc nursing professionals and one general practitioner participated in the data collection process and the diagnosis of phlebitis. If disagreement happens on the diagnosis of phlebitis, the physician confirms whether it is phlebitis or not then the decision of the physician was taken as a final decision for this study. Patients with PIVC were followed two times per a day. Jackson’s Visual Infusion Phlebitis Scoring System, an internationally accepted diagnosis approach and set of criteria that has been studied in the scientific literature and applied in clinical settings all over the world, was utilized to make the diagnosis of phlebitis. The Jackson’s Visual Infusion Phlebitis Scoring System provides a score from zero to five in ascending order of severity of inflammation or phlebitis. Each grade identifies a more or less advanced state of phlebitis or thrombophlebitis and differs in the evidence of specific signs and actions to be taken.
Score zero - the insertion site appears healthy and there are no signs of phlebitis. Only continued observation of the cannula is indicated. Score one – one of the following signs is evident: slight pain or slight redness near intravenous insertion site. These are possible early signs of phlebitis. In addition, in this case it will simply be necessary to continue with monitoring. Score two – two of the following signs are evident: pain at intravenous insertion site, redness or swelling. This is the early stage of phlebitis, requiring repositioning of the peripheral venous catheter. Score three – all of the following signs are evident: pain along the path of the cannula, redness around the insertion site and swelling. This is the medium stage of phlebitis, so the catheter should be repositioned and treatment considered. Score four – all of the following signs are evident and extensive: pain along the path of the cannula, redness around the insertion site, swelling, palpable venous cord. This is the advanced stage of phlebitis or at the start of thrombophlebitis. It is recommended to reposition the catheter and consider treatment. Score five – all of the following signs are evident and extensive: pain along the path of the cannula, redness around the insertion site, swelling, palpable venous cord, pyrexia. This is the stage of advanced thrombophlebitis, which requires initiating treatment and repositioning the peripheral venous catheter. Clearly, it is important that detections and interventions are always documented for effective monitoring and prevention.6,12,23
Data Quality Assurance and Control
Data quality was assured through designed proper data abstraction questionnaires. Pre-test was done on five percent of the sample size. Training was given for data collectors and supervisor. The investigator and supervisor closely monitored and supervised the data collection process to ensure the quality of data. Every day, the data was checked for consistency and completeness, and any problems that arose during data collecting were addressed appropriately.
Data Management and Analysis
The questionnaires’ consistency and data completeness were carefully reviewed. The data was entered using Epi Data version 3.1 and exported to Stata version 15 for analysis. For categorical independent predictors, the Spearman's rank test was used to examine multicollinearity. To determine frequency, proportion, interquartile range, cumulative incidence, and person-time incidence-rate, descriptive analyses were performed. The proportional hazards assumption was checked using a graphic way (log minus log plot of survival estimation) and a statistical method (global test). The overall model fitness was examined using the Cox Snell residual test and the log-likelihood ratio test. The candidate predictors for the multivariable Cox proportional hazards regression analysis were selected using the bi-variable Cox proportional hazards regression method. In multiple Cox proportional hazards regression analysis, predictors were included if their p-value for bi-variable Cox proportional hazards regression analysis was ≤0.25 and they satisfied the Cox proportional hazards ratio assumption. Cox proportional hazards regression analysis with a 95% confidence level was used to find the predictors of phlebitis. The measure of association between the outcome variable and the independent variables was declared statistical significance at a P-value of less than five percent.
Results
Socio-Demographic Characteristics
Four hundred sixty-two patients participated in this study. Among those, 243 (52.60%) were females. The median age of the patients was 42 years old, with an interquartile range 27 to 60 years old. Majority of the patients, 286 (61.90%), were rural residents (Table 1).
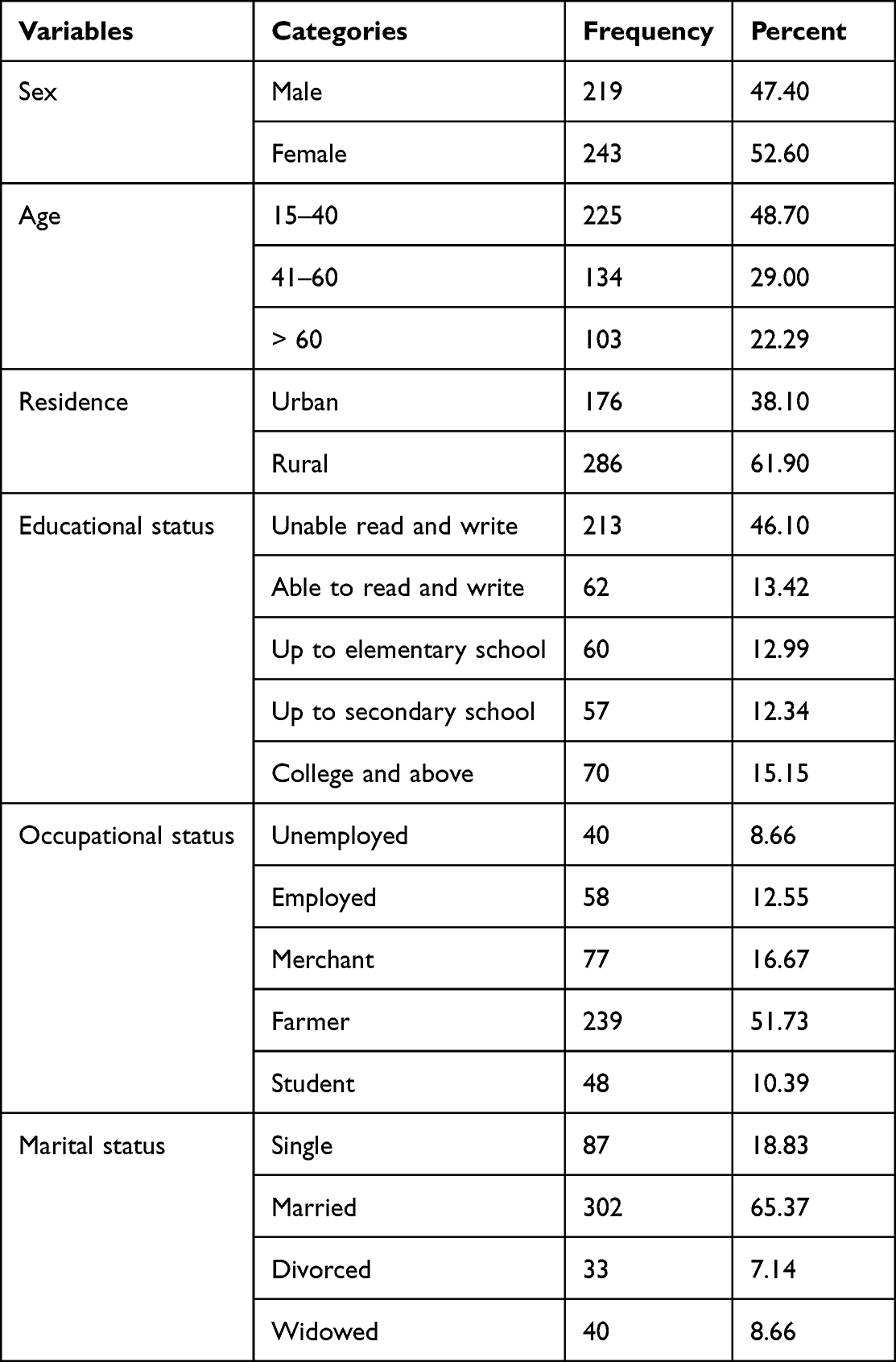 |
Table 1 Socio-Demographic Characteristics of Patients with PIVC at Bahir Dar City Public Hospitals, Amhara, Ethiopia, 2022 (N = 462) |
Clinical-Related Characteristics
From all (462) participated patients, 185 (40.04%) were admitted with two or more diseases. During the study period, 165 (35.71%) patients had at least one chronic disease (hypertension, heart diseases, chronic kidney diseases, asthma or diabetes mellitus). Most patients, 414 (89.61%) were treated through drugs (medications) (Table 2).
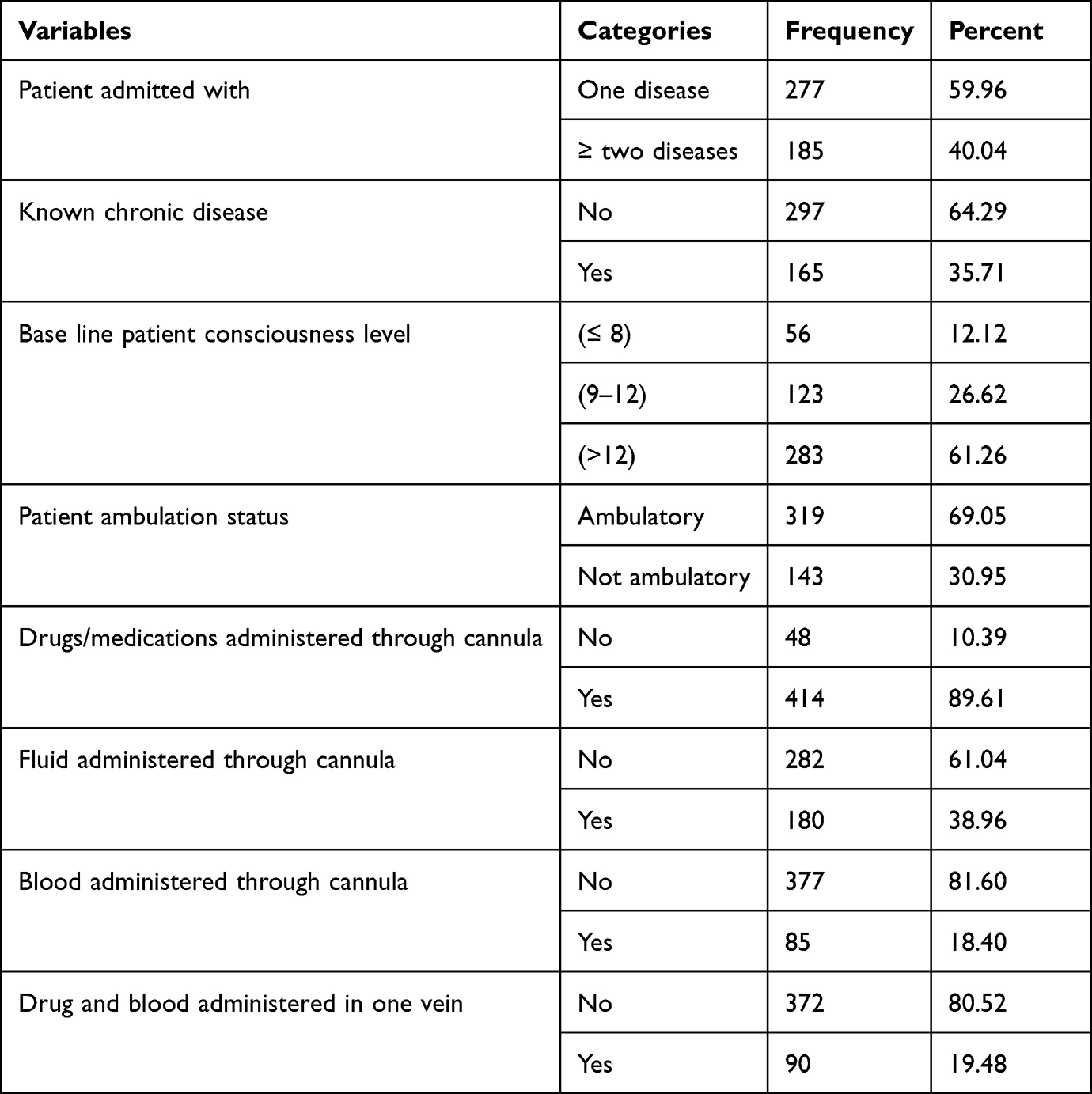 |
Table 2 Clinical Related Characteristics of Patients with PIVC at Bahir Dar City Public Hospitals, Amhara, Ethiopia, 2022 (N = 462) |
Cannula-Related Characteristics
In this study, to insert cannula, three different site superficial veins were used, which were dorsum of hand vein, radial vein and antecubital fossa vein. Most of the PIVC were inserted on the patient’s dorsum of hand that accounted, 210 (45.45%). Above half of the patients, 241 (52.16%) used 18-gauge cannula size. In this study, near to half of the PIVC dwelling time was more than four days (Table 3).
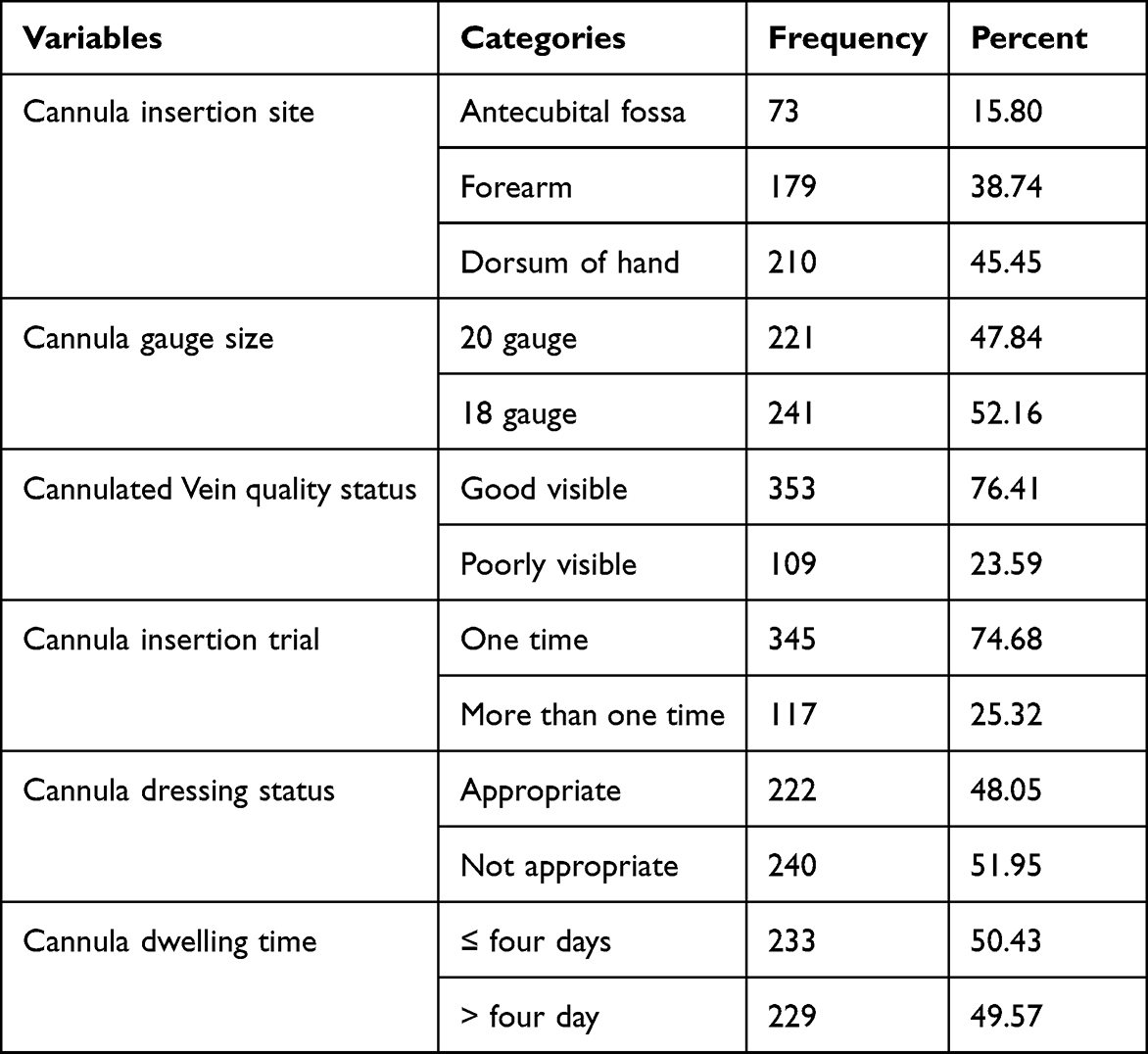 |
Table 3 Cannula-Related Characteristics of Patients with PIVC at Bahir Dar City Public Hospitals, Amhara, Ethiopia, 2022 (N = 462) |
Incidence and Median Survival Time of Phlebitis
The incidence rate of post-peripheral intravenous cannula phlebitis was 8/100 persons per day observation (95% CI 7/100 – 9/100). The overall median survival time of phlebitis was six days with a survival interquartile range of five up to seven days. During the study period, 171 (37.01%) patients developed phlebitis, while the rest 291 (62.99%) patients did not develop phlebitis.
Predictors of Phlebitis
Ten of the twenty potential demographic, clinical, and cannula-related predictors were significantly associated in bi-variable regressions with phlebitis at a significance level of 0.25 and were therefore entered into the multivariable regression. Six of these predictors were significant at p-value of <0.05 in the final Cox proportional hazards model. When compared to individuals between the ages of 15 and 40, people older than 60 had a 51% lower risk of developing phlebitis (AHR = 0.49, 95% CI 0.29–0.82). Patients with chronic diseases had a 1.50 times greater risk of getting phlebitis than individuals without chronic disease (AHR = 1.50, 95% CI 1.09–2.07). When blood and medications were administered through a single vein as compared to independently, the risk of phlebitis increased by 2.03 times (AHR = 2.03, 95% CI 1.44–2.86). The risk of developing phlebitis was 1.52 times higher in patients who used an 18-gauge cannula size compared to those who used a 20-gauge cannula size (AHR = 1.52, 95% CI 1.08–2.15). Individuals who had improper cannula dressing had a 1.81 higher risk of developing phlebitis than those who had proper cannula dressing (AHR = 1.81, 95% CI 1.31–2.51). Phlebitis was 7.39 times more likely to develop in patients with a cannula dwelling time of more than four days as compared to individuals with a cannula dwelling time of less than or equal to four days (AHR = 7.39, 95% CI 4.12–13.32) (Table 4).
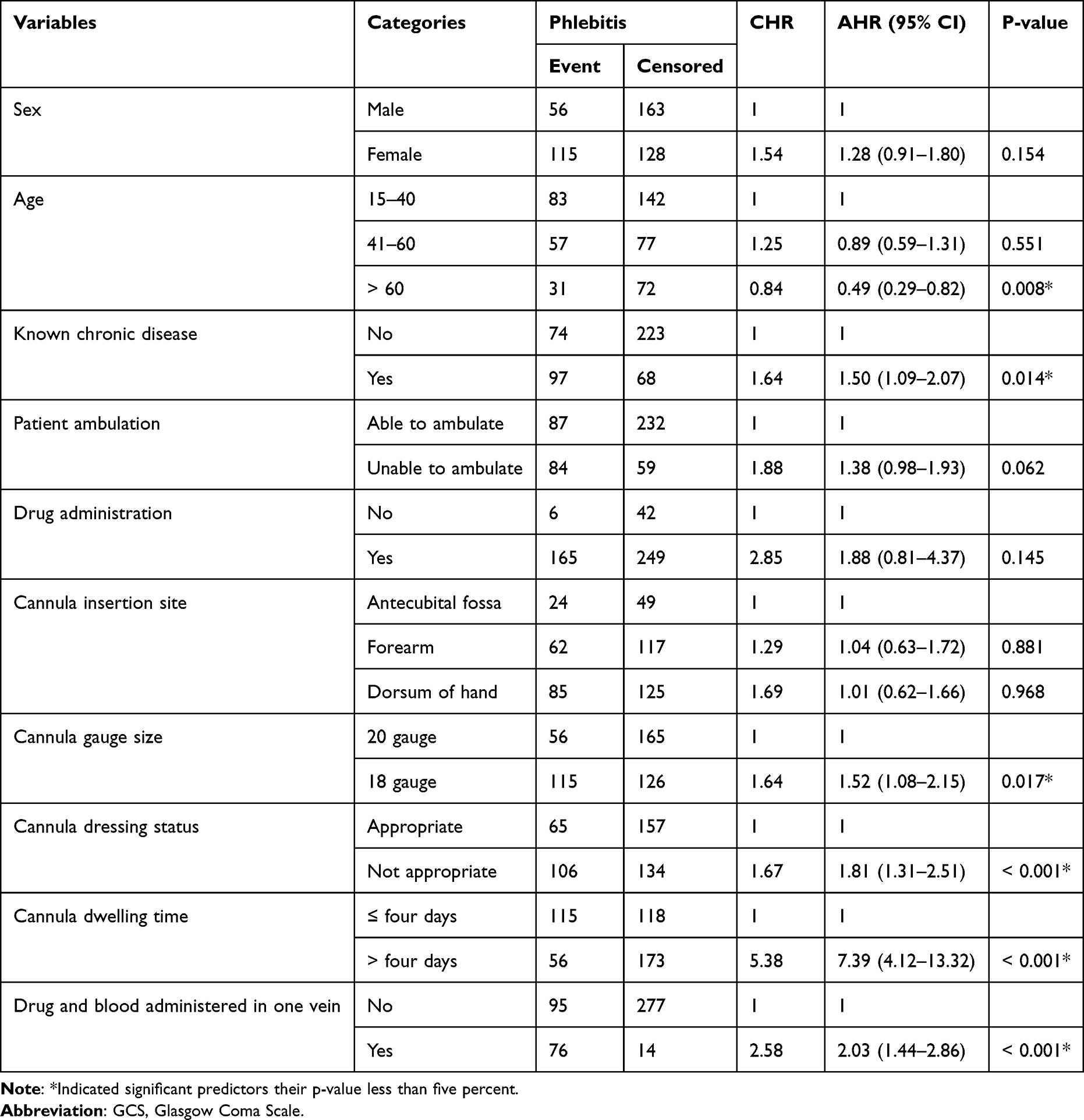 |
Table 4 Bi-Variable and Multi-Variable Cox Proportional Hazards Regression for the Predictors of Phlebitis Among Patients with PIVC at Bahir Dar City Public Hospitals, Amhara, Ethiopia |
Discussion
This study found that the incidence density rate of phlebitis was 8/100 persons per day of observation and the cumulative incidence of 37.01%. The incidence was far higher than the acceptable phlebitis rate of five percent or below, as recommended by the Infusion Nurses Society (INS).9 This might be a reference to poor PIVC procedures and unsuccessful prevention efforts. This result was in line with research conducted in Saudi Arabia.24 The similarities were because both studies used a comparable study design and phlebitis diagnosing approach.
The current finding was higher than studies done in Africa (13%) and other nations like Malaysia (15.41%) and Brazil (18.34%).13,19,25 The discrepancy might be due to diagnosis approach and sampling differences. A study carried out in Malaysia used a laboratory-based approach to diagnosing microorganisms, which is a reliable way of diagnostics that lowers the incidence of phlebitis. The study in Brazil was a retrospective follow-up study, but the current study was prospective follow-up; therefore, this difference might bring discrepancy between two studies on the incidence of post-cannula phlebitis.
However, the finding was lower than studies conducted in Ethiopia (Gondar) (70%) and Tunisia (51.90).6,15 The discrepancy of the study might be due to sampling technique and sample size difference. The current study used probability-sampling technique and relatively used large sample size. However, study conducted in Tunisia used small sample size and study conducted at the University of Gondar Compressive Specialized Hospital used nonprobability-sampling technique. Using small sample size and non-probability sampling techniques might increase the incidence of post-cannula phlebitis.
According to this study, the median cannula dwelling time was four days, ranging from two to eight days. This finding was similar to study conducted in Saudi Arabia and 25 European countries.26,27 The median survival time to develop phlebitis was six days with a survival inter-quartile range of five up to seven days. This showed that 50% of the patients acquired phlebitis before six days of after PIVC inserted. In the other ways, 50% of the patients could survive to develop phlebitis beyond six days. This finding was inconsistent with studies conducted in Saudi Arabia and Australia.10,27 The discrepancy might be due to difference in sampling and diagnosis criteria of phlebitis.
The current study’s findings showed that patients between the ages of 15 and 40 years had a higher risk of developing phlebitis than patients older than 60 years. This finding contradicted with studies conducted in Spain and Australia.28,29 Patients in the adult age group had more sensitive immune systems than old age group, which caused them to experience an inflammatory process because of an antigen–antibody response that led to an infection-like phlebitis.9,19 Patients with chronic disease were more risk for phlebitis as compared to patients free from chronic disease. This finding was similar to studies conducted at other parts of Ethiopia and Qatar.6,12 Because patients with chronic disease are physiologically unstable compared to healthy individuals, patients with chronic conditions like diabetes mellitus, hypertension, and others are more immune-compromised and unable to combat infection/inflammation such as phlebitis.4,18
Evidence showed that when drugs and blood were administered through one vein, the vein become infiltrated more quickly as a result of the drugs’ and blood’s irritating effects of the blood vessel.30,31 The irritation effects of intravenous medication and reaction of blood make the blood vessels become inflamed. As a result, drugs and blood lead the blood vessel more susceptible to post-cannula phlebitis.32
Patients who used 18-gauge cannula size were more risk to develop phlebitis as compared to patients that used 20-gauge cannula size. This result was similar to studies conducted in Qatar.12 Eighteen-gauge cannula size is comparably large in its diameter and length as compared to 20 gauge cannula sizes. A smaller diameter cannula accommodates the patient’s vein that minimizes the risk of phlebitis. However, choosing larger cannula diameter size can increase the rate of phlebitis, and the risk rises with increasing the diameter of the cannula. This is because of the physical properties and the size of the cannula that affect the physiology of the vein tissues by irritating and physically damaging the cannulated vein.4,17
Patients with improper PIVC dressing experienced more phlebitis than those with appropriate PIVC securing or dressing. This finding was similar to studies conducted in Spain and Saudi Arabia.9,24 To minimize the risk of blood clotting from over-tightening the vein and phlebitis from direct contamination, the cannula insertion site should be secured and dressed appropriately.4,10,18 Patients who had longer cannula dwelling time (greater than four days) were more risk to develop phlebitis as compared to patients who had shorter cannula dwelling time (less than or equal to four days). The finding was consistent with studies done in other counties.1,24 Different factors like shortage of medical supply (cannula), low human resources (healthcare providers) and poor coordination of resources at healthcare settings increase dwelling time of the cannula. As a result, prolonged cannula dwell times cause continued trauma of the vein due to longer contact to irritant drugs and colloids that contribute to high chance of inflammation or phlebitis.6,33
Limitation of the Study
This study included patients who admitted at medical wards but did not incorporate/included patients that admitted to other wards.
Conclusion
The incidence of post-PIVC phlebitis was much higher than the acceptable rate. The median time to develop phlebitis was six days with the survival inter-quartile range of five up to seven days. Hence, all patients with PIVC better to be screened for phlebitis at least once daily. It is also important to have appropriate nursing care and patient education to reduce the associated risk factors that were identified in this study. An observation chart to document the development of signs of phlebitis may be developed in hospitals, which may help detect PIVC complications (phlebitis) much earlier. The use of an adequate cannula size and a shorter cannula dwell time significantly lowers the risk of phlebitis. Therefore, in order to prevent PIVC phlebitis healthcare providers should consequently emphasize using proper medical equipment, such as choosing the appropriate cannula size and lowering cannula dwell duration. Future researchers should incorporate patients who were admitted to other than medical wards for better generalizability of the problem of PIVC phlebitis.
Abbreviations
AIDS, Acquired Immune Deficiency Syndrome; BDU, Bahir Dar University; DVT, Deep Vein Thrombosis; HR, Hazard Ratio; HIV, Human Immune Virus; PIVC, Peripheral Intravenous Cannula; VIPS, Visual Infusion Phlebitis Score.
Availability of the Data
The data used to support the findings of this study are available from one of the authors for reasonable request.
Ethical Approval and Consent
Ethical clearance was obtained from Institutional Review Board (IRB) of Bahir Dar University College of Medicine and Health Sciences. A letter of cooperation was written for all public hospitals of Bahir Dar city with a letter written on April/22, 2022, with a protocol number of 418/2022. During the study period, written informed consent was taken from each patient that participated in this study. However, for patients whose age was under 18 years, informed consent was taken from the parent. Confidentiality of the information was secured throughout the study by excluding names and patient medical record numbers on the data extraction form and the data were used only for the proposed study. This study followed the ethical standard of the declaration of Helsinki.
Acknowledgment
We want to acknowledge Bahir Dar University for the opportunity and financial aid to collect these study data. We would like to extend our sincere thanks to the employees of public hospitals of Bahir Dar city (research coordinator, ward coordinator, card room workers, and others) for their help during the data collection for this thesis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The funding source for the current research is from Bahir Dar University College of Medicine and Health Sciences. The funder had no role in the data collection, analysis, drafting, manuscript, preparation, and publication of this paper.
Disclosure
This paper is based on the thesis of Tadios Lidetu, Alemshet Yirga and Elisabet Mesfin Alene. It has been uploaded on the website of College of Medicine and Health Sciences, Bahir Dar University. Even if, the thesis has been uploaded on the institutional website, it does not mean thesis publication in formal way. The authors report no conflicts of interest in this work.
References
1. Lee S, Kim K, Kim J-S. A model of phlebitis associated with peripheral intravenous catheters in orthopedic inpatients. Int J Environ Res Public Health. 2019;16(18):3412. doi:10.3390/ijerph16183412
2. López JG, Vilela AA, Del Palacio EF, Corral JO, Martí CB, Portal PH. Indwell times, complications and costs of open vs closed safety peripheral intravenous catheters: a randomized study. J Hosp Infect. 2014;86(2):117–126. doi:10.1016/j.jhin.2013.10.008
3. Furlan M, Lima AFC. Evaluation of phlebitis adverse event occurrence in patients of a clinical inpatient unit. Rev Esc Enferm USP. 2021;2021:55.
4. Milutinović D, Simin D, Zec D. Risk factor for phlebitis: a questionnaire study of nurses’ perception. Rev Lat-Am Enferm. 2015;23:677–684. doi:10.1590/0104-1169.0192.2603
5. Ray‐Barruel G, Polit DF, Murfield JE, Rickard CM. Infusion phlebitis assessment measures: a systematic review. J Eval Clin Pract. 2014;20(2):191–202. doi:10.1111/jep.12107
6. Lulie M, Tadesse A, Tsegaye T, Yesuf T, Silamsaw M. Incidence of peripheral intravenous catheter phlebitis and its associated factors among patients admitted to University of Gondar hospital, Northwest Ethiopia: a prospective, observational study. Thromb J. 2021;19(1):1–8. doi:10.1186/s12959-021-00301-x
7. Palese A, Ambrosi E, Fabris F, et al. Nursing care as a predictor of phlebitis related to insertion of a peripheral venous cannula in emergency departments: findings from a prospective study. J Hosp Infect. 2016;92(3):280–286. doi:10.1016/j.jhin.2015.10.021
8. Birhane E, Kidanu K, Kassa M, et al. Lifespan and associated factors of peripheral intravenous Cannula among infants admitted in public hospitals of Mekelle City, Tigray, Ethiopia, 2016. BMC Nurs. 2017;16(1):1–8. doi:10.1186/s12912-017-0227-1
9. Guanche-Sicilia A, Sánchez-Gómez MB, Castro-Peraza ME, Rodríguez-Gómez JÁ, Gómez-Salgado J, Duarte-Clíments G. Prevention and Treatment of Phlebitis Secondary to the Insertion of a Peripheral Venous Catheter: a Scoping Review from a Nursing Perspective. In: Healthcare. Multidisciplinary Digital Publishing Institute; 2021.
10. Keogh S, Mathew S. Peripheral Intravenous Catheters: A Review of Guidelines and Research. Sydney: ACSQHC; 2019.
11. Book PICR. Peripheral Cannulation.
12. Abolfotouh M, Salam M, White D, Balkhy H. Prospective study of incidence and predictors of peripheral IV Catheter–induced complications.
13. Alexandrou E, Ray-Barruel G, Carr PJ, et al. Use of short peripheral intravenous catheters: characteristics, management, and outcomes worldwide. J Hosp Med. 2018;13(5):E1–E7. doi:10.12788/jhm.3039
14. Marsh N, Webster J, Larson E, Cooke M, Mihala G, Rickard CM. Observational study of peripheral intravenous catheter outcomes in adult hospitalized patients: a multivariable analysis of peripheral intravenous catheter failure. J Hosp Med. 2017;13(2):83–89. doi:10.12788/jhm.2867
15. Ben Abdelaziz R, Hafsi H, Hajji H, et al. Peripheral venous catheter complications in children: predisposing factors in a multicenter prospective cohort study. BMC Pediat. 2017;17(208). doi:10.1186/s12887-017-0965-y
16. Glover KR, Stahl BR, Murray C, et al. A simulation-based blended curriculum for short peripheral intravenous catheter insertion: an industry–practice collaboration. J Contin Educ Nurs. 2017;48(9):397–406. doi:10.3928/00220124-20170816-05
17. Yasuda H, Yamamoto R, Hayashi Y, et al. Occurrence and incidence rate of peripheral intravascular catheter-related phlebitis and complications in critically ill patients: a prospective cohort study (AMOR-Venus study). J Intensive Care. 2021;9(1):1–12. doi:10.1186/s40560-020-00518-4
18. Arias-Fernández L, Suérez-Mier B, Del Carmen Martinez-Ortega M, Lana A. Incidence and risk factors of phlebitis associated to peripheral intravenous catheters. Enfermería Clínica. 2017;27(2):79–86. doi:10.1016/j.enfcli.2016.07.008
19. Ng R, Johari BM, Kuppusamy P, Ponnampalavanar S, Sohail A. A quality improvement study to reduce peripheral intravenous catheter-related complications in the medical ward of a tertiary hospital in Malaysia. Int J Infect Dis. 2020;101:311–312. doi:10.1016/j.ijid.2020.09.813
20. Foumani SA, Paryad E, Khanghah AG, Leili EK. Routine replacement or clinically indicated replacement of peripheral intravenous catheters. J Pharm Res Int. 2018;1–10. doi:10.9734/JPRI/2018/38767
21. Alexandrou E, Ray‐Barruel G, Carr PJ, et al. International prevalence of the use of peripheral intravenous catheters. J Hosp Med. 2015;10(8):530–533. doi:10.1002/jhm.2389
22. Høvik LH, Gjeilo KH, Lydersen S, et al. Monitoring quality of care for peripheral intravenous catheters; feasibility and reliability of the peripheral intravenous catheters mini questionnaire (PIVC-miniQ). BMC Health Serv Res. 2019;19(1):1–10. doi:10.1186/s12913-019-4497-z
23. Gu MO, Cho Y, Eun Y, et al. Updates of nursing practice guideline for intravenous infusion. J Korean Clin Nurs Res. 2017;23(3):361–375.
24. Abolfotouh MA, Salam M, Bani-Mustafa DW A, Balkhy HH. Prospective study of incidence and predictors of peripheral intravenous catheter-induced complications. Ther Clin Risk Manag. 2014;10:993. doi:10.2147/TCRM.S74685
25. Danski MTR, Johann DA, Vayego SA, Oliveira GR, Lind J. Complications related to the use of peripheral venous catheters: a randomized clinical trial. ACTA Paul Enferm. 2016;29:84–92. doi:10.1590/1982-0194201600012
26. Cooke M, Ullman AJ, Ray-Barruel G, Wallis M, Corley A, Rickard CM. Not” just” an intravenous line: consumer perspectives on peripheral intravenous cannulation (PIVC). An international cross-sectional survey of 25 countries. PLoS One. 2018;13(2):e0193436. doi:10.1371/journal.pone.0193436
27. Shinde MB, Zagade TB, Potdar NJ, Pawar S. Occurance and predictors of peripheral intravenouscatheter induced complications at tertiary care hospital. age. 2020;29(02):2928–2934.
28. Rodriguez-Calero MA, de Pedro-Gomez JE, Molero-Ballester LJ, et al. Risk factors for difficult peripheral intravenous cannulation. The PIVV2 multicentre case-control study. J Clin Med. 2020;9(3):799. doi:10.3390/jcm9030799
29. Wallis MC, McGrail M, Webster J, et al. Risk factors for peripheral intravenous catheter failure: a multivariate analysis of data from a randomized controlled trial. Infect Control Hosp Epidemiol. 2014;35(1):63–68. doi:10.1086/674398
30. Sijabat M, Nduru SD, Sitanggang YF, Hutasoit EO. Incidence of phlebitis following the use of peripheral IV Line at X hospital. Indones Contemp Nurs J. 2021;79–86. doi:10.20956/icon.v5i2.10859
31. Sharp R, Turner L, Altschwager J, Corsini N, Esterman A. Adverse events associated with home blood transfusion: a retrospective cohort study. J Clin Nurs. 2021;30(11–12):1751–1759. doi:10.1111/jocn.15734
32. Kreidieh FY, Moukadem HA, El Saghir NS. Overview, prevention and management of chemotherapy extravasation. World J Clin Oncol. 2016;7(1):87. doi:10.5306/wjco.v7.i1.87
33. Flores Moreno M, Pueblas Bedoy KS, Ojeda Sánchez A, Zurita-Cruz J. Risk factors associated with complications that required the removal of peripherally inserted central venous catheters in a tertiary pediatric hospital. Bol Med Hosp Infant. 2017;74(4):289–294. doi:10.1016/j.bmhimx.2017.03.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.