")
Back to Journals » Clinical Interventions in Aging » Volume 17
Treating and Managing Laryngopharyngeal Reflux Disease in the Over 65s: Evidence to Date
Authors Lechien JR
Received 30 September 2022
Accepted for publication 4 November 2022
Published 15 November 2022 Volume 2022:17 Pages 1625—1633
DOI https://doi.org/10.2147/CIA.S371992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Jerome R Lechien1– 3
1Polyclinic of Poitiers, Elsan Hospital, Poitiers, France; 2Department of Anatomy and Experimental Oncology, Mons School of Medicine, UMONS Research Institute for Health Sciences and Technology, University of Mons (UMons), Mons, Belgium; 3Department of Otolaryngology–Head and Neck Surgery, EpiCURA Hospital, University of Mons, Baudour, Belgium
Correspondence: Jerome R Lechien, Department of Otolaryngology–Head and Neck Surgery, EpiCURA Hospital, University of Mons, Rue L. Cathy, Mons, Belgium, Tel +32 65 37 35 84, Email [email protected]
Purpose: The clinical presentation and therapeutic outcomes of elderly patients may be different from those in younger populations, leading to additional diagnostic and therapeutic difficulties. The present study reviewed the findings on the epidemiology, and clinical, diagnostic, and therapeutic outcomes of elderly patients with laryngopharyngeal reflux (LPR).
Methods: A PubMed, Cochrane Library, and Scopus literature search was conducted on the epidemiological, clinical, diagnostic, and therapeutic findings of elderly LPR patients.
Findings: The prevalence of LPR in the elderly population remains unknown. From a clinical standpoint, older LPR patients report overall lower symptom scores and related quality-of-life outcomes at the time of the diagnosis. The required treatment time to obtain symptom relief appears to be longer in older compared with younger patients. Particular attention needs to be paid to prolonged medication use because the elderly population is characterized by polypharmacy and there is a higher risk of proton-pump inhibitor (PPI) interactions and adverse events. The plasma clearance of most PPIs is reduced with age, which must be considered by practitioners in the prescription of antireflux therapy.
Conclusion: The clinical presentation and treatment efficacy of elderly LPR patients differ from those in younger patients. Practitioners need to carefully consider the risk of drug interactions and adverse events in elderly patients.
Keywords: laryngitis, laryngopharyngeal reflux, reflux, otolaryngology, head neck surgery, gastroesophageal reflux, voice, elderly, aging, age
Introduction
Laryngopharyngeal reflux (LPR) is an inflammatory disease of the upper aerodigestive tract tissues related to the backflow of gastroduodenal content reflux, which induces morphological changes in the upper aerodigestive tract.1 The diagnosis of LPR is based on non-specific symptoms and findings, the positive response to an empirical therapeutic trial, or the demonstration of pharyngeal reflux episodes upon hypopharyngeal–esophageal multichannel intraluminal impedance pH monitoring (HEMII-pH).1,2 The clinical diagnosis of LPR remains complicated owing to the non-specificity of symptoms and signs, and their overestimation by practitioners.3,4 Thus, elderly patients represent a challenging population because of their tendency to report atypical clinical presentations of many digestive diseases.5,6 In addition, this population is growing in Western countries, representing more than 16% of the US population in 2020.7
The aim of this state-of-the art review was to report the current knowledge on the epidemiology, and clinical, diagnostic, and therapeutic outcomes of elderly patients with LPR.
Methods
A PubMed, Cochrane Library, and Scopus database search was conducted for relevant peer-reviewed publications in English, Spanish, and French language related to epidemiology, clinical presentation, pathophysiology, diagnosis, and treatment of LPR in elderly populations. The following keywords were used (and/or): “reflux”, “laryngopharyngeal”, “gastroesophageal”, “extra-esophageal”, “elderly”, “aging”, “old”, “symptoms”, “findings”, “treatment”, and “physiology”. We included clinical prospective/retrospective controlled/uncontrolled studies, systematic reviews, and meta-analyses. From this initial review, papers were selected for inclusion in the final review if they focused on the epidemiology, pathophysiology, clinical picture, diagnosis, and treatment of LPR in the aging population. The authors should report the inclusion and exclusion criteria, diagnostic method, therapeutic outcomes, and treatment regimen. Critical analysis of this literature was carried out focusing on incidence and prevalence, clinical presentation, diagnosis, and treatment of elderly patients with LPR. From this review, implications for practice were summarized. Ethics committee approval was not required for this review. Individuals agreed (by informal consent) to the use of the photographs (Figure 1) for publication.
 |
Figure 1 Findings in patients with laryngopharyngeal reflux. Notes: Patients with laryngopharyngeal reflux often reported anterior pillar erythema (A), coated tongue (A), tongue tonsil hypertrophy and posterior coated tongue (B), granulations of the posterior wall of the oropharynx (C), sticky mucus in the throat and edema of the retrocricoid region (D), epiglottis erythema and posterior commissure hypertrophy (E), and laryngeal erythema (F). |
Note that a systematic review or meta-analysis was not performed because of the low number of studies and the important heterogeneity in inclusion/exclusion criteria, use of ambulatory reflux monitoring, treatment and outcome measures.
Epidemiology
The first important epidemiological study on LPR was conducted in 1991 by Jamie Koufman.8 In this prospective study, Dr Koufman estimated that acid LPR was present in 10% of outpatients presenting to otolaryngology departments with laryngopharyngeal symptoms and findings.8 This study was the first report to differentiate LPR from gastroesophageal reflux disease (GERD), because 62% of patients had abnormal esophageal acid exposure but only 30% reported acid hypopharyngeal reflux events on dual-probe pH monitoring. Several studies estimated the prevalence of LPR symptoms to be 5–30% of outpatients consulting otolaryngological offices, but the authors based their evaluation of prevalence on the results of patient-reported outcome questionnaires without diagnostic confirmation.9–11 To date, the prevalence of LPR in the general population is still unknown. According to the largest cohort studies, the mean age of LPR patients ranged from 37 to 53 years old.4,12–15 Thus, LPR seems to be a disease of the forties, but the first episodes may appear earlier in acute or recurrent forms.16 There have been no population-based surveys evaluating the prevalence of LPR-related symptoms in elderly populations, although the prevalence of GERD has been investigated in many elderly populations.17 According to large-cohort studies, the prevalence of GERD increases with aging,17,18 affecting 6–17% of the elderly US population17,19 and up to 31.5% of European individuals >60 years of age.18 However, the prevalence of GERD in the elderly population may be underestimated owing to the aging of esophageal nerve sensitivity and the related decrease in GERD alarm symptoms, such as heartburn or non-cardiac chest pain. The exact proportion of GERD patients with laryngopharyngeal symptoms and findings was not investigated in these studies, making any estimation of LPR in elderly populations difficult.
Pathophysiology
Physiology of Laryngopharyngeal Reflux
The development of LPR symptoms and findings is related to the backflow of gastroduodenal content (eg pepsin, bile salts, and other gastrointestinal proteins) into the upper aerodigestive tract mucosa. The deposition of enzymes, especially pepsin, leads to mucosal injury, inflammatory reaction, mucus dryness, epithelial thickening, and microtrauma.20 The mucosal irritation leads to mucus production and dehydration through a down-regulation of mucin and carbonic anhydrase gene expression.21 The accumulation of sticky mucus induces postnasal drip, globus sensation, throat clearing, dysphagia, and cough. Depending on patients’ mucosa sensitivity, as well as unknown factors,22 patients with acute, recurrent, or chronic LPR may develop mild, moderate, or severe symptoms.
The recent use of HEMII-pH monitoring in otolaryngology has improved the understanding of LPR physiology and the differences between LPR and GERD. The profile of LPR at the HEMII-pH is characterized by daytime and upright gaseous weakly or non-acid hypopharyngeal reflux events in most patients.23,24 In more than 50% of cases, patients do not report GERD.25 The gaseous nature of events and the lack of GERD have led to a clinical picture characterized by otolaryngological symptoms without heartburn or abdominal findings.
Influence of Aging on Physiology
The main mechanisms of defense against reflux (eg esophageal motility, bicarbonate secretion, and lower [LES] and upper esophageal sphincter [UES] tonicity) appear to be impaired with aging.26,27 Older patients have decreased salivary flow and bicarbonate secretion, which is associated with a reduction in the neutralization of refluxed acid28 and an increase in pepsin activity.29 Others have reported that esophageal motility and the LES and UES pressure are weakened in elderly patients, leading to a theoretical increase in esophagopharyngeal reflux events.30,31 Mei et al observed that UES pressure and esophageal body motility responses to reflux and post-reflux residue were decreased in elderly populations, which may be associated with a higher proportion of hypopharyngeal reflux events and impaired airway protection.31 Moreover, it was suggested that elderly patients were found to have a higher proportion of hiatal hernia, present in 60% of >60-year-old patients, compared with young people.32 The presence of hiatal hernia is an additional predisposing factor for GERD but is also associated with recalcitrant LPR.33 All of these physiological aging changes were associated with more intense patterns of abdominal acid contact time and advanced erosive diseases on gastrointestinal endoscopy compared with younger patients.34,35
Elderly Diseases and Reflux
LPR is suspected to be associated with many prevalent conditions in the elderly population. Parkinson’s disease,36 pulmonary fibrosis,37 chronic obstructive pulmonary disease,38 systemic sclerosis,39 and other conditions increase in prevalence with aging, and their related impairments in respiratory, digestive, or swallowing physiology may be associated with an increased risk of reflux. In the same vein, the consumption of some medications (eg benzodiazepines, antidepressants, anticholinergics, theophylline, nitrates, calcium antagonists, lidocaine, and prostaglandins) increases the risk of GERD,40 although these associations have not been formally investigated in LPR patients. Note that, irrespective of their age, LPR patients are commonly not obese.41,42
Clinical Picture
Symptom Presentation
The most prevalent symptoms of LPR include dysphonia, globus sensation, throat pain, odynophagia, accumulation of sticky mucus, throat clearing, and cough.1,4 These are summarized in the reflux symptom score (RSS), which is a validated patient-reported outcome questionnaire assessing symptom frequency, severity, and quality of life.43 The clinical presentation of elderly patients with LPR has been investigated in a few studies.44–47 In 2013, Lee et al investigated the influence of age on the clinical presentation and treatment of patients with suspected LPR.44 The authors reported that the oldest group (60–79 years old) had higher baseline clinical (reflux symptom index [RSI]) and quality of life (LPR health-related quality of life) scores than the 18–39-year-old group. The findings of Lee et al were not confirmed in a European multicenter study in which elderly patients (>60 years old) with suspected LPR showed lower RSI scores than younger individuals.45 Moreover, the impact of LPR on quality of life was lower in the elderly group compared with the younger group, which supported that aging reduces the subjective perception of LPR symptoms.45 The differences between the study of Lee et al and others may be related to their inclusion criteria. Lee et al based the LPR diagnosis on the presence of at least one laryngopharyngeal symptom and finding in all age groups, whereas they did not exclude some confounding conditions associated with laryngopharyngeal symptoms and findings, eg tobacco- or alcohol-related laryngopharyngitis, chronic rhinosinusitis, or radiation or trauma history. The use of such inclusion criteria in all patients irrespective of age may constitute a selection bias because elderly patients were selected with the same clinical criteria as the younger ones. In that way, the analysis of symptom presentation (at baseline) may be biased because these symptoms were similarly considered in the inclusion criteria. In other studies, diagnosis was based on pH/impedance findings or on criteria associated with validated thresholds in sign and symptom instruments. The lower symptom scores of elderly LPR populations were confirmed in a study of 237 patients with LPR at the HEMII-pH.46 In this study, individuals in the oldest group (>60 years) had lower RSS and lower quality-of-life scores than younger patients. Interestingly, the lower clinical scores concerned otolaryngological and digestive symptom scores. There were no difference in gastrointestinal endoscopy findings between age groups, while older patients exhibited significantly lower numbers of supine hypopharyngeal reflux events than younger individuals.46 The decrease in symptom scores with aging was supported by Cervera-Paz and Jordano-Cabrera, who reported a mean RSI of 9.8 in elderly patients, with only 28% of cases having an abnormal threshold score (RSI >12).47 Although this study did not compare clinical and pH monitoring findings between several age groups, the mean RSI was lower than those of large clinical studies.44,45
In sum, most studies reporting age features in LPR populations supported the occurrence of less symptom sensation and related quality-of-life impact in elderly patients. This observation may support the existence of neurological deterioration of the terminal sensitive laryngopharyngeal nerve endings, and strengthens the findings of gastrointestinal studies that reported less severe heartburn and related digestive complaints in older patients with esophageal lesions.34,48
Finding Presentation
The most common signs associated with LPR in aging individuals include posterior commissure hypertrophy, laryngeal erythema, anterior pillar erythema, laryngopharyngeal erythema, tongue tonsil hypertrophy, and retrocricoid edema (Figure 1).45–47 Irrespective of the clinical instrument used in the study (reflux finding score versus reflux sign assessment), the authors did not find any significant influence of age, smoking, drinking, or diet on the presentation of laryngeal, oral, or pharyngeal signs in LPR patients.44–46 Hence, the observations for LPR do not corroborate those for GERD, according to studies highlighting more advanced erosive disease in elderly patients with GERD.35,48,49
In gastroenterology, the body mass index is an important factor contributing to GERD and other digestive diseases. A high body weight in elderly patients increases the risk of GERD and hiatal hernia.34 In the study by Cervera-Paz and Jordano-Cabrera, 50 patients (59%) with suspected LPR had a high body mass index, which was associated with abnormal single-probe esophageal pH monitoring.47 The lack of comparison with younger groups, as well as the lack of HEMII-pH use, limit the drawing of clear conclusions on the influence of both age and weight on LPR findings. The above-mentioned studies did not report a significant influence of age on the body weight of LPR patients.44,46 The main symptoms and features found in elderly patients with LPR versus those with GERD are described in Table 1.
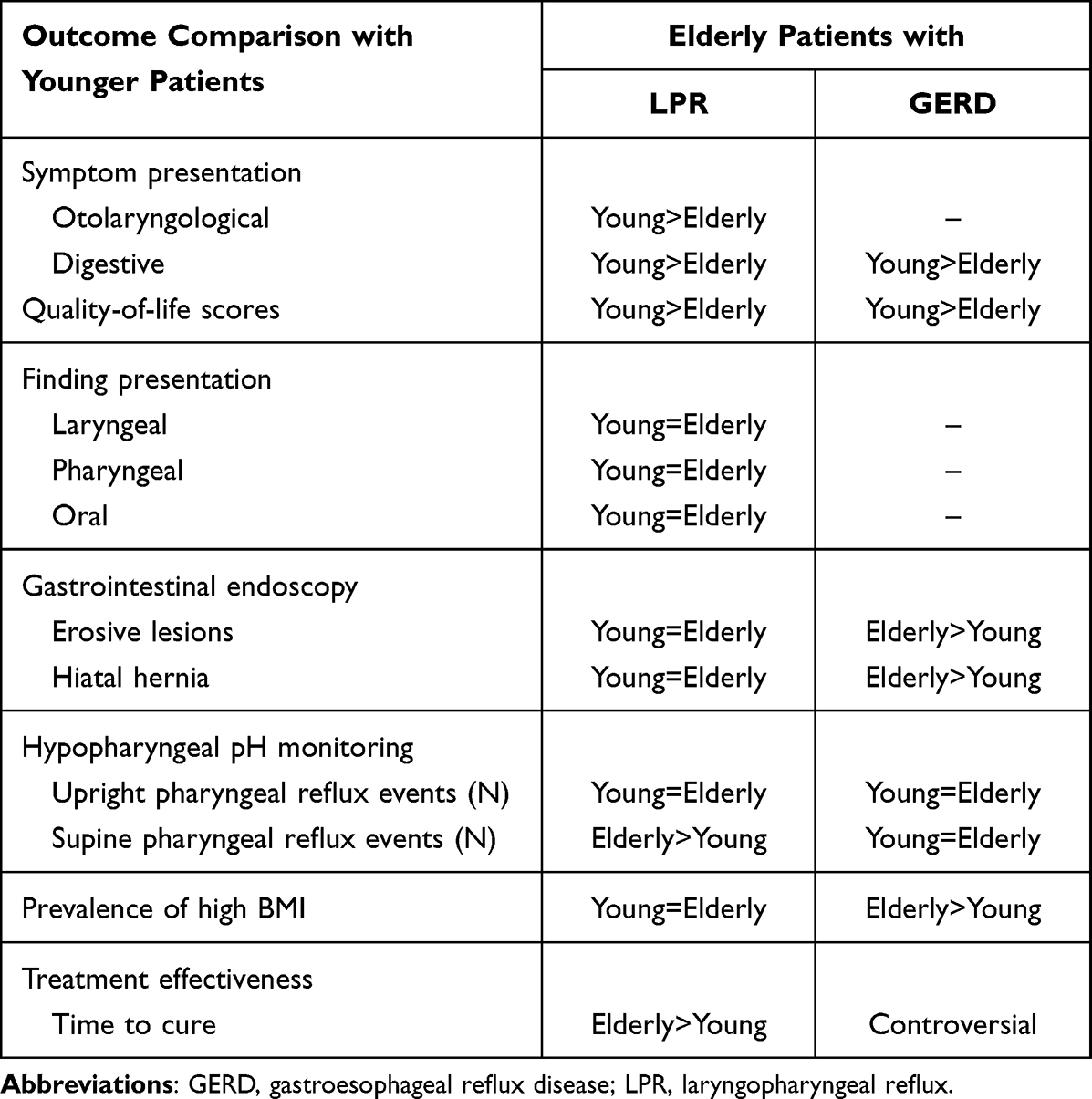 |
Table 1 Laryngopharyngeal and Gastroesophageal Reflux Features of Elderly Patients |
Therapeutic Outcomes
The treatment of LPR was long term, based on proton pump inhibitors (PPIs). However, meta-analyses suggested that the superiority of PPIs over placebo has still not been demonstrated.50,51 In practice, 60% of LPR patients reported a decrease in symptoms or relief of symptoms with once- or twice-daily PPIs.52 The low efficacy of PPIs is related to the high prevalence of weakly acid and non-acid (alkaline) LPR, which require treatment with alginate or magaldrate.53,54
According to data in the the literature, elderly LPR patients report different therapeutic responses from younger patients.44–46 Lee et al reported significantly more responders to PPI therapy, defined as those whose RSI score improved by more than 50%, in both the 18–39-year-old group (86%) and the 40–59-year-old group (75%), compared with the >60-year-old group (57%).44 These findings were corroborated in our 2017 study, in which elderly LPR patients at the HEMII-pH needed more time (6 months versus 3 months) to achieve cure than younger patients.45 Note that there were substantial therapeutic differences between these two studies. Indeed, Lee et al used PPIs only, whereas we used a combination of diet, PPIs, and alginate.46,53
In practice, many elderly patients take long-term PPI therapy for LPR, GERD, or other gastrointestinal conditions. According to a large population-based cross-sectional study, the percentages of 18–39, 40–59, and ≥60-year-old people taking PPIs in the UK were 23.1%, 35.1%, and 39.8%, respectively.55 The overprescription of long-term PPIs in elderly patients is an important issue for many reasons.56
First, most elderly individuals take several medications and there are some drug interaction risks between PPIs and many common medications, including antiretroviral (HIV) drugs, cytostatics (eg methotrexate, dasatinib, erlotinib, and nilotinib), anti-HCV, itraconazole, immunosuppressants, and clopidogrel (Table 2).57
 |
Table 2 Drug Interactions of Proton Pump Inhibitors |
There are potential harms of PPI treatment, and the related potential drug interactions in elderly individuals who are characterized by polypharmacy are associated with a higher risk of long-term adverse effects.58
Second, the long-term use of PPIs has for a long time been suspected to be associated with adverse events, eg altered mineral and vitamin absorption, fractures, orthopedic injury, acute coronary syndromes, colitis, infectious risks, and increased risk of mortality.59–63 Most patients on long-term PPIs and practitioners may be unaware about these interactions and adverse events.59,60,63 However, as stated by Kanno and Moayyedi,58 “association is not causation”, and many confounding factors have biased some PPI–adverse event studies, leading to overinterpretion of modest increases in odds ratios. For example, the association between PPIs and pneumonia may be related to the prescription of PPIs for a presumed reflux cough, which was, however, due to lung infection.58 The indication of long-term prescription of PPIs or other antireflux medication must be carefully assessed by the practitioner, who has to keep in mind that, irrespective of the patient’s age, more than 50% of LPR events are acute or recurrent,16 and, therefore, do not require long-term medication. According to studies, the weaning rates of antireflux therapy in LPR patients ranged from 64% to 75% of cases.59,64,65
Third, the overprescription of PPIs, particularly in elderly patients, has a dramatic impact on the costs of healthcare systems. In the USA, the annual costs for treating LPR and GERD are estimated at between US$9.3 and US$50 billion, making reflux one of the costliest diseases to manage.66,67 Thus, cost-effective therapeutic approaches (including an antireflux diet) should be prioritized over medication therapy in mild and moderate LPR.68
The usefulness of H2-histamine blockers was not assessed in the present review because they are less potent than PPIs6 and these drugs have proven to be less effective in terms of healing rates and symptom relief for GERD, esophagitis, or LPR.69 Finally, PPIs appear to have different clearance properties, which is an important issue to consider in older patients. Esomeprazole has a more rapid onset of action and less variation in clearance rates than omeprazole. The drug clearance decreases with age, exaggerating some of the differences between the PPIs. The reduction of PPI clearance may increase the risk of drug interactions. The reduction of PPI plasma clearance particularly concerns pantoprazole, rabeprazole, and lansoprazole, and was found to increase by up to 50–100%.70,71 However, clearance of esomeprazole is not significantly affected by age, supporting its usefulness in elderly populations.
Conclusion
The clinical presentation and treatment efficacy of elderly patients with reflux differ from those in younger patients. Adverse events, clearance outcomes of PPIs, and drug interactions should be considered in future therapeutic approaches to guide more effective personalized treatment plans for elderly patients with LPR.
Ethics Committee Approval and Informed Consent
Not requested for a review paper.
Funding
There is no funding to report.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Lechien JR, Akst LM, Hamdan AL, et al. Evaluation and management of laryngopharyngeal reflux disease: state of the art review. Otolaryngol Head Neck Surg. 2019;160(5):762–782. doi:10.1177/0194599819827488
2. Ford CN. Evaluation and management of laryngopharyngeal reflux. JAMA. 2005;294(12):1534–1540. doi:10.1001/jama.294.12.1534
3. Mahieu HF. Review article: the laryngological manifestations of reflux disease; why the scepticism? Aliment Pharmacol Ther. 2007;26(Suppl 2):17–24. doi:10.1111/j.1365-2036.2007.03474.x
4. Thomas JP, Zubiaur FM. Over-diagnosis of laryngopharyngeal reflux as the cause of hoarseness. Eur Arch Otorhinolaryngol. 2013;270(3):995–999. doi:10.1007/s00405-012-2244-8
5. Janowska A, Dini V, Oranges T, Iannone M, Loggini B, Romanelli M. Atypical ulcers: diagnosis and management. Clin Interv Aging. 2019;14:2137–2143. doi:10.2147/CIA.S231896
6. Calabrese C, Fabbri A, Di Febo G. Long-term management of GERD in the elderly with pantoprazole. Clin Interv Aging. 2007;2(1):85–92. doi:10.2147/ciia.2007.2.1.85
7. Greenwald DA. Aging, the gastrointestinal tract, and risk of acid-related disease. Am J Med. 2004;117 Suppl 5A:8–13.
8. Koufman JA. The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope. 1991;101(4Pt 2 Suppl 53):1–78. doi:10.1002/lary.1991.101.s53.1
9. Spantideas N, Drosou E, Bougea A, Assimakopoulos D. Laryngopharyngeal reflux disease in the Greek general population, prevalence and risk factors. BMC Ear Nose Throat Disord. 2015;15(1):7. doi:10.1186/s12901-015-0020-2
10. Kamani T, Penney S, Mitra I, Pothula V. The prevalence of laryngopharyngeal reflux in the English population. Eur Arch Otorhinolaryngol. 2012;269(10):2219–2225. doi:10.1007/s00405-012-2028-1
11. Chen XM, Li Y, Guo WL, Wang WT, Lu M. Prevalence of laryngopharyngeal reflux disease in Fuzhou region of China. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2016;51(12):909–913. doi:10.3760/cma.j.issn.1673-0860.2016.12.006
12. Lee YS, Choi SH, Son YI, Park YH, Kim SY, Nam SY. Prospective, observational study using rabeprazole in 455 patients with laryngopharyngeal reflux disease. Eur Arch Otorhinolaryngol. 2011;268(6):863–869. doi:10.1007/s00405-010-1475-9
13. Habermann W, Schmid C, Neumann K, et al. Reflux symptom index and reflux finding score in otolaryngologic practice. J Voice. 2012;26(3):e123–7. doi:10.1016/j.jvoice.2011.02.004
14. Chappity P, Kumar R, Deka RC, Chokkalingam V, Saraya A, Sikka K. Proton pump inhibitors versus solitary lifestyle modification in management of laryngopharyngeal reflux and evaluating who is at risk: scenario in a developing country. Clin Med Insights Ear Nose Throat. 2014;7:1–5. doi:10.4137/CMENT.S13799
15. Youssef TF, Ahmed MR. Treatment of clinically diagnosed laryngopharyngeal reflux disease. Arch Otolaryngol Head Neck Surg. 2010;136(11):1089–1092. doi:10.1001/archoto.2010.165
16. Lechien JR, Hans S, Calvo-Henriquez C, Baudouin R, Saussez S. Laryngopharyngeal reflux may be acute, recurrent or chronic disease: preliminary observations. Eur Arch Otorhinolaryngol. 2022;279(9):4629–4632. doi:10.1007/s00405-022-07426-3
17. Mold JW, Reed LE, Davis AB, et al. Prevalence of gastroesophageal reflux in elderly patients in a primary care setting. Am J Gastroenterol. 1991;86:965–970.
18. Kennedy T, Jones R. The prevalence of gastro-oesophageal reflux symptoms in a UK population and the consultation behaviour of patients with these symptoms. Aliment Pharmacol Ther. 2000;14(12):1589–1594. doi:10.1046/j.1365-2036.2000.00884.x
19. Locke GR, Talley NJ, Fett SL, et al. Prevalence and clinical spectrum of gastro- esophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112(5):1448–1456. doi:10.1016/S0016-5085(97)70025-8
20. Klimara MJ, Randall DR, Allen J, Figueredo E, Johnston N. Proximal reflux: biochemical mediators, markers, therapeutic targets, and clinical correlations. Ann N Y Acad Sci. 2020;1481(1):127–138. doi:10.1111/nyas.14366
21. Lechien JR, Saussez S, Harmegnies B, Finck C, Burns JA. Laryngopharyngeal reflux and voice disorders: a multifactorial model of etiology and pathophysiology. J Voice. 2017;31(6):733–752. doi:10.1016/j.jvoice.2017.03.015
22. Lechien JR, De Vos N, Everard A, Saussez S. Laryngopharyngeal reflux: the microbiota theory. Med Hypotheses. 2021;146:110460. doi:10.1016/j.mehy.2020.110460
23. Lechien JR, Chan WW, Akst LM, et al. Normative ambulatory reflux monitoring metrics for laryngopharyngeal reflux: a systematic review of 720 healthy individuals. Otolaryngol Head Neck Surg. 2021;1945998211029831. doi:10.1177/01945998211029831
24. Lechien JR, Bobin F, Dapri G, et al. Hypopharyngeal-esophageal impedance-ph monitoring profiles of laryngopharyngeal reflux patients. Laryngoscope. 2021;131(2):268–276. doi:10.1002/lary.28736
25. Salgado S, Borges LF, Cai JX, Lo WK, Carroll TL, Chan WW. Symptoms classically attributed to laryngopharyngeal reflux correlate poorly with pharyngeal reflux events on multichannel intraluminal impedance testing. Dis Esophagus. 2022;doac041. doi:10.1093/dote/doac041
26. Pilotto A. Aging and upper gastrointestinal disorders. Best Pract Res Clin Gastroenterol. 2004;18:Suppl:73–81. doi:10.1016/j.bpg.2004.06.015
27. Pilotto A, Maggi S, Noale M, et al. Association of upper gastrointestinal symptoms with functional and clinical characteristics in elderly. World J Gastroenterol. 2011;17(25):3020–3026. doi:10.3748/wjg.v17.i25.3020
28. Sonnenberg A, Steinkamp U, Weise A, et al. Salivary secretion in reflux esophagitis. Gastroenterology. 1982;83(4):889–895. doi:10.1016/S0016-5085(82)80021-8
29. Block BB, Kuo E, Zalzal HG, Escobar H, Rose M, Preciado D. In vitro effects of acid and pepsin on mouse middle ear epithelial cell viability and MUC5B gene expression. Arch Otolaryngol Head Neck Surg. 2010;136(1):37–42. doi:10.1001/archoto.2009.199
30. Lee J, Anggiansha A, Anggiansah R, et al. Effects of age on the gastroesoph- ageal junction, esophageal motility, and reflux disease. Clin Gastroenterol Hepatol. 2007;5(12):1392–1398. doi:10.1016/j.cgh.2007.08.011
31. Mei L, Dua A, Kern M, et al. Older age reduces upper esophageal sphincter and esophageal body responses to simulated slow and ultraslow reflux events and post-reflux residue. Gastroenterology. 2018;155(3):760–770.e1. doi:10.1053/j.gastro.2018.05.036
32. Khajanchee YS, Urbach DR, Butler N, et al. Laparoscopic antireflux surgery in the elderly. Surg Endosc. 2002;16(1):25–30. doi:10.1007/s00464-001-8157-z
33. Lechien JR, Saussez S, Muls V, et al. Laryngopharyngeal reflux: evolution and predictive value of symptoms and pH-impedance features on clinical evolution. Otolaryngol Head Neck Surg. 2022;1945998221075009. doi:10.1177/01945998221075009
34. Achem SR, DeVault KR. Gastroesophageal reflux disease and the elderly. Gastroenterol Clin North Am. 2014;43(1):147–160. doi:10.1016/j.gtc.2013.11.004
35. Patti MG, Goldberg HI, Arcerito M, et al. Hiatal hernia size affects lower esoph- ageal sphincter function, esophageal acid exposure, and the degree of mucosal injury. Am J Surg. 1996;171(1):182–186. doi:10.1016/S0002-9610(99)80096-8
36. Su A, Gandhy R, Barlow C, Triadafilopoulos G. Clinical and manometric characteristics of patients with Parkinson’s disease and esophageal symptoms. Dis Esophagus. 2017;30(4):1–6. doi:10.1093/dote/dow038
37. Su Y, Shen L, Zhang F, et al. Laryngopharyngeal pH monitoring in patients with idiopathic pulmonary fibrosis. Front Pharmacol. 2021;12:724286. doi:10.3389/fphar.2021.724286
38. Eryuksel E, Dogan M, Olgun S, Kocak I, Celikel T. Incidence and treatment results of laryngopharyngeal reflux in chronic obstructive pulmonary disease. Eur Arch Otorhinolaryngol. 2009;266(8):1267–1271. doi:10.1007/s00405-009-0922-y
39. Chwiesko A, Kowal-Bielecka O, Sierakowski S. Perspectives on the interlinked nature of systemic sclerosis and reflux disease. Expert Rev Gastroenterol Hepatol. 2019;13(3):213–227. doi:10.1080/17474124.2019.1561274
40. Storr M, Allescher HD. Esophageal pharmacology and treatment of primary motility disorders. Dis Esophagus. 1999;12(4):241–257. doi:10.1046/j.1442-2050.1999.00059.x
41. Jung SY, Park DC, Kim SH, Yeo SG. Role of obesity in otorhinolaryngologic diseases. Curr Allergy Asthma Rep. 2019;19(7):34. doi:10.1007/s11882-019-0865-3
42. Halum SL, Postma GN, Johnston C, Belafsky PC, Koufman JA. Patients with isolated laryngopharyngeal reflux are not obese. Laryngoscope. 2005;115(6):1042–1045. doi:10.1097/01.MLG.0000162656.05715.57
43. Lechien JR, Bobin F, Muls V, et al. Validity and reliability of the reflux symptom score. Laryngoscope. 2020;130(3):E98–E107. doi:10.1002/lary.28017
44. Lee YC, Lee JS, Kim SW, Kwon KH, Eun YG. Influence of age on treatment with proton pump inhibitors in patients with laryngopharyngeal reflux disease: a prospective multicenter study. JAMA Otolaryngol Head Neck Surg. 2013;139(12):1291–1295. doi:10.1001/jamaoto.2013.5556
45. Lechien JR, Finck C, Huet K, et al. Impact of age on laryngopharyngeal reflux disease presentation: a multi-center prospective study. Eur Arch Otorhinolaryngol. 2017;274(10):3687–3696. doi:10.1007/s00405-017-4671-z
46. Lechien JR, Carroll TL, Bobin F, et al. Influence of age and sex on clinical and therapeutic features of laryngopharyngeal reflux. Otolaryngol Head Neck Surg. 2022;166(3):468–476. doi:10.1177/01945998211020284
47. Cervera-Paz FJ, Jordano-Cabrera M. Characterisation of laryngo-pharyngeal reflux disease in old and ageing patients. Acta Otorrinolaringol Esp. 2019;70(3):151–157. doi:10.1016/j.otorri.2018.05.002
48. Becher A, Dent J. Systematic review: aging and gastroesophageal reflux disease symptoms, esophageal function and reflux esophagitis. Aliment Pharmacol Ther. 2011;33(4):450. doi:10.1111/j.1365-2036.2010.04542.x
49. Zhu H, Pace F, Sangaletti O, et al. Features of symptomatic gastroesophageal reflux in elderly patients. Scand J Gastroenterol. 1993;28(3):235–238. doi:10.3109/00365529309096078
50. Karkos PD, Wilson JA. Empiric treatment of laryngopharyngeal reflux with proton pump inhibitors: a systematic review. Laryngoscope. 2006;116(1):144–148. doi:10.1097/01.mlg.0000191463.67692.36
51. Jin X, Zhou X, Fan Z, Qin Y, Zhan J. Meta-analysis of proton pump inhibitors in the treatment of pharyngeal reflux disease. Comput Math Methods Med. 2022;2022:9105814. doi:10.1155/2022/9105814
52. Lechien JR, Muls V, Dapri G, et al. The management of suspected or confirmed laryngopharyngeal reflux patients with recalcitrant symptoms: a contemporary review. Clin Otolaryngol. 2019;44(5):784–800. doi:10.1111/coa.13395
53. Lechien JR, Bobin F, Muls V, et al. The efficacy of a personalised treatment depending on the characteristics of reflux at multichannel intraluminal impedance-pH monitoring in patients with acid, non-acid and mixed laryngopharyngeal reflux. Clin Otolaryngol. 2021;46(3):602–613. doi:10.1111/coa.13722
54. Lechien JR. Clinical update findings about pH-impedance monitoring features in laryngopharyngeal reflux patients. J Clin Med. 2022;11(11):3158. doi:10.3390/jcm11113158
55. Abrahami D, McDonald EG, Schnitzer M, Azoulay L. Trends in acid suppressant drug prescriptions in primary care in the UK: a population-based cross-sectional study. BMJ Open. 2020;10(12):e041529. doi:10.1136/bmjopen-2020-041529
56. Yailian AL, Huet E, Charpiat B, et al. Characteristics of pharmacists’ interventions related to proton-pump inhibitors in French hospitals: an observational study. Int J Clin Pract. 2022;2022:9619699. doi:10.1155/2022/9619699
57. Toth JM, Jadhav S, Holmes HM, Sharma M. Prescribing trends of proton pump inhibitors, antipsychotics and benzodiazepines of medicare part d providers. BMC Geriatr. 2022;22(1):306. doi:10.1186/s12877-022-02971-2
58. Kanno T, Moayyedi P. Proton pump inhibitors in the elderly, balancing risk and benefit: an age-old problem. Curr Gastroenterol Rep. 2019;21(12):65. doi:10.1007/s11894-019-0732-3
59. Verhasselt M, Rodriguez A, Dequanter D, Lechien JR. Chronic course, weaning, and awareness of patients with reflux toward proton pump inhibitor therapy. J Voice. 2021. doi:10.1016/j.jvoice.2021.03.002
60. Luo H, Fan Q, Bian T, et al. Awareness, attitude and behavior regarding proton pump inhibitor among medical staff in the Southwest of China. BMC Health Serv Res. 2019;19(1):880. doi:10.1186/s12913-019-4725-6
61. Rameau A, Andreadis K, Bayoumi A, Kaufman M, Belafsky P. Side effects of proton pump inhibitors: what are patients’ concerns? J Voice. 2020;35(5):809.e15–809.e20. doi:10.1016/j.jvoice.2020.01.018
62. Lanas-Gimeno A, Hijos G, Lanas Á. Proton pump inhibitors, adverse events and increased risk of mortality. Expert Opin Drug Saf. 2019;18(11):1043–1053. doi:10.1080/14740338.2019.1664470
63. Chapman DB, Rees CJ, Lippert D, Sataloff RT, Wright SC
64. Lin RJ, Sridharan S, Smith LJ, Young VN, Rosen CA. Weaning of proton pump inhibitors in patients with suspected laryngopharyngeal reflux disease. Laryngoscope. 2018;128(1):133–137. doi:10.1002/lary.26696
65. Lechien JR, Bobin F, Muls V, et al. Changes of laryngeal and extralaryngeal symptoms and findings in laryngopharyngeal reflux patients. Laryngoscope. 2021;131(6):1332–1342. doi:10.1002/lary.28962
66. Sandler RS, Everhart JE, Donowitz M, et al. The burden of selected digestive diseases in the United States. Gastroenterology. 2002;122(5):1500–1511. doi:10.1053/gast.2002.32978
67. Francis DO, Rymer JA, Slaughter JC, et al. High economic burden of caring for patients with suspected extraesophageal reflux. Am J Gastroenterol. 2013;108(6):905–911. doi:10.1038/ajg.2013.69
68. Lechien JR, Crevier-Buchman L, Distinguin L, et al. Is diet sufficient as laryngopharyngeal reflux treatment? A cross-over observational study. Laryngoscope. 2021. doi:10.1002/lary.29890
69. Desilets AR, Asal NJ, Dunican KC. Considerations for the use of proton-pump inhibitors in older adults. Consult Pharm. 2012;27(2):114–120. doi:10.4140/TCP.n.2012.114
70. Huber R, Hartmann M, Bliesath H, et al. Pharmacokinetics of pantoprazole in man. Int J Clin Pharmacol Ther. 1996;34(5):185–194.
71. Flouvat B, Delhotal-Landes B, Cournot A, et al. Single and multiple dose pharmacokinetics of lansoprazole in elderly subjects. Br J Clin Pharmacol. 1993;36(5):467–469. doi:10.1111/j.1365-2125.1993.tb00398.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.