")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Tuberculosis and Public Health Care Workers: Infection Prevention and Control Practices and Associated Factors Among Governmental Health Centers and Hospitals in Wolaita Zone, Southern Ethiopia
Authors Labena F, Kassa Y, Gambura E
Received 28 May 2021
Accepted for publication 21 July 2021
Published 10 August 2021 Volume 2021:14 Pages 2111—2122
DOI https://doi.org/10.2147/JMDH.S321592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fikru Labena,1 Yibeltal Kassa,2 Eyasu Gambura2
1Sodo Health Center, Wolaita Zone Health Department, Sodo, Ethiopia; 2School of Public Health, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Eyasu Gambura Tel +251901513048
Email [email protected]
Purpose: Institutional settings, including health care facilities, have been identified to be at high risk of tuberculosis (TB) transmissions. But no study has been conducted in hospitals and health centers concurrently in Wolaita Zone, Southern Ethiopia. Therefore, the aim of this study was to assess tuberculosis infection prevention and control (TBIPC) practices and associated factors among public health care workers in Wolaita Zone, Southern Ethiopia.
Material and Methods: A facility-based cross-sectional quantitative study supplemented with qualitative interview and observation was conducted in 16 sampled governmental health facilities in Wolaita Zone, Southern Ethiopia, from 25 July 2020 to 25 August 2020. A multistage sampling technique was used to select 748 health care workers, while purposive sampling was used to identify participants for the qualitative study.
Results: The proportion of proper TBIPC practices was 44.78%. Years of service (AOR=4.182, 95% CI: 2.024– 8.639), working in a TB clinic (AOR=4.009, 95% CI: 1.311– 12.261), working in an anti-retroviral therapy clinic (AOR=2.796, 95% CI: 1.009– 7.743), TB-related training (AOR=0.024, 95% CI: 11.483– 34.92), availability of personal protective equipment (AOR=1.712, 95% CI: 1.057– 2.776), good knowledge of TBIPC measures (AOR=2.66, 95% CI: 1.119– 4.196), and positive attitude (AOR=2.011, 95% CI: 1.242– 3.255) were significantly associated with proper TBIPC practices.
Conclusion and Recommendation: The proportion of proper TBIPC practices among public health care workers was low in the study area. For better intervention, further studies could focus on experimental research into possible factors that are responsible for TBIPC practices in health care facilities in the study area.
Keywords: health care workers, infection prevention, institutions, knowledge, tuberculosis
Introduction
Tuberculosis (TB) is an infectious disease which causes a high burden of morbidity and mortality in developing countries. Tuberculosis infection prevention and control (TBIPC) consists of different strategies designed to reduce the risk of Mycobacterium tuberculosis transmission. There are three levels in the hierarchy of control, namely administrative control, environmental control, and respiratory protection, which has been shown to minimize and prevent the risk of transmission of and exposure to M. tuberculosis.1
Different activities have been performed around the world to overcome the problems of TB, from stop-tuberculosis strategies to end-tuberculosis strategies following the initiation of sustainable development goals, with the targets of a 95% reduction in the number of TB deaths and 90% reduction in TB incidence rates by 2035.2 However, TB remains a global public health threat affecting millions of people every year, and the increasing incidence of drug resistance and the human immunodeficiency virus (HIV) pandemic mean that TB control efforts have now become more challenging, and this has led to greater concerns over TB infection control.3
Institutional settings, including health care facilities, have been identified as being at high risk of TB transmissions.4 Health care workers (HCWs) have the potential to have contact with TB patients and are very important stakeholders in health care settings to implement TB infection control.6 All HCWs managing outpatients and inpatients in health care facilities are at risk of health care-associated TB infection,7 and the poor practice of TB infection control may increase the risk of transmission of TB in health care settings.8
A survey conducted by the World Health Organization (WHO) identified that 9299 TB cases among health workers were reported from 60 countries only, with the notification rate for health care-associated transmission of M. tuberculosis being twice as high as the rate in the general adult population.1
The prevalence of TB among HCWs (nurses 42.3%, doctors 39.4%, and administrative staff members 11.3%) in China,10 and in a study conducted in general hospitals in Vietnam, showed that a high prevalence of latent TB infection among health professionals may also suggest the need to strengthen TB infection control, particularly among health professionals in the emergency department.11
Another study, conducted in the Southern Nations, Nationalities, and Peoples’ Region (SNNPR), South Omo, Ethiopia, found that the prevalence of latent TB infection control practice was 50.5%, and there were some difficulties with TB infection control measures at health care facilities, including poor understanding of self-protection using an N95 respirator and immediate isolation of patients with suspected TB.12
TBIPC measures are critical for the prevention and control of healthcare-associated TB infection. These measures are among the most cost-effective and available in health care settings and one of TBIPC measures recommended by the WHO in countries with a high prevalence of TB to reduce the disease burden. However, there has been limited study regarding TBIPC practices and associated factors among public HCWs in Southern Ethiopia, and no study has been conducted in hospitals and health centers concurrently in the current study area. Therefore, the aim of this study was to assess TBIPC practices and associated factors among public HCWs in Wolaita Zone, Southern Ethiopia. The findings of this study could enable planners and program managers to design appropriate interventions or strategies by filling the gaps in an attempt to improve TBIPC practices, to improve the extent and current practices of TBIPC in public health facilities.
Materials and Methods
Study Design, Study Area, and Setting
A facility-based cross-sectional quantitative study design supplemented with qualitative interviews and observations was conducted in 16 sampled governmental health facilities in Wolaita Zone, Southern Ethiopia, from 25 July 2020 to 25 August 2020. This region is located at a distance of 380 km from Addis Ababa. The area of the Zone is 4208.64 km2. The mean annual temperature is 18.9°C and the average annual rainfall of the Zone is 1100 mm.21 The annual report for 2019 shows that Wolaita Zone health department has six administrative towns and 16 woredas, with a total population of 2,067,166, of whom 1,012,911 are males and 1,054,255 are females.
According to the data obtained from the human resources departments of different public health care facilities, currently, there are about 68 health centers, five primary hospitals, one teaching and referral hospital, and one general hospital. There are 5602 HCWs in Wolaita Zone, including 3610 nurses, 85 general practitioners, 258 laboratory technicians, 568 midwives, 313 health officers, 15 anesthesiologists, five radiology, seven emergency surgery, and 20 different types of specialists.
Source Population
The source population was all HCWs in governmental hospitals and health centers of the Wolaita Zone.
Study Population
The study population comprised randomly selected HCWs from two governmental hospitals and 12 governmental health centers for the quantitative study; and for the qualitative part, purposively selected TBIPC focal persons.
Inclusion and Exclusion Criteria
Inclusion Criteria
All health professionals who were working in a selected health facility with the qualification of doctors, health officers, nurses, midwives, X-ray technicians/radiologists, pharmacists/druggists, and laboratory personnel working in the direct care of patients were included in the quantitative study; and all TBIPC focal persons of each health care facility were included in the qualitative study.
Exclusion Criteria
HCWs who were not directly involved in patient care, and HCWs who were on maternity leave, annual leave, or sick leave were not included.
Sample Size Determination
The sample size for the study was calculated using a single population proportion formula considering 95% level of confidence, 5% margin of error, and 10% non-response rate. The proportion (p) of proper TB infection control practice is 38% in the study conducted in West Gojjam Zone, Northwest Ethiopia.9 The total sample size was 748.
Sampling Techniques for the Quantitative and Qualitative Studies
For the quantitative study, a multi-stage sampling method was used. In the first stage, five woredas and two administrative towns were selected using simple random sampling. From the total, 30% were included in the study. Then, they were stratified by type of health care facility into hospitals and health centers. To enhance representativeness, 30% of health care facilities from each stratum were randomly selected and included in the sample. From two hospitals and 12 health centers, selected at random, the sample size (N=748) of HCWs was allocated, proportional to their size. The sampling frame was obtained from the human resources department of each health care facility, and HCWs who participated in the study were selected by simple random sampling.
For the qualitative study, a criterion type of purposive sampling technique was employed to explore detailed information on TB infection control practices. TBIPC focal persons were recruited from each health care facility and the number of interviewees was sought until ideal saturation was reached.
Study Variables and Operational Definition
The dependent variable of the study was TBIPC practice. The independent variables were socio-demographic factors of HCWs (age, sex, marital status, educational status, profession), work experience of HCWs, current working department, previous TB-related training, availability of personal protective equipment (surgical masks, N95 respirators), and behavioral factors (knowledge of and attitude towards TBIPC.
Proper Tuberculosis Infection Control Practice
To determine the level of practice, respondents were asked 12 questions and those who scored ≥80.0% were considered as performing proper practice.
Improper Tuberculosis Infection Control Practice
Those who were scored <80.0% on the 12 questions were considered as performing improper practice.
Good Knowledge
To determine the level of knowledge, participants were asked 18 questions and those who scored ≥60.0% of knowledge questions correctly were classified as having a good level of knowledge.
Poor Knowledge
Those who were scored <60.0% were considered to have a poor level of knowledge.
Positive Attitude
To determine the level of attitude, participants were asked 10 questions and composite scores were calculated. Those who were scored ≥70.0% were considered as having a positive attitude towards TBIPC Practices.
Negative Attitude
Those who were scored <70.0% were considered as having a negative attitude. The cut-off points on TB infection control knowledge, attitude, and practices were obtained from a similar study undertaken among HCWs.5,9,14,22
Data Collection
Data were collected using a self-administered structured questionnaire. The questionnaire was developed by adapting from different studies in the literature and TB infection control guidelines (Supplementary Material). The adapted questionnaire was translated into Amharic and then back-translated to English and pretested for consistency. The questionnaire was also tested for internal consistency by Cronbach’s alpha test. The reliability coefficient for attitude and knowledge items had a Cronbach’s alpha of ≥0.70 and qualitative data were collected using semi-structured open-ended key-informant interviews, which were translated into Amharic and then back-translated to English. Key informant interviews, note-taking, and tape-recording were conducted by trained data collectors to collect qualitative data until information saturation was reached.
Data Quality Control Measures
The questionnaires were prepared in English and translated into Amharic, then back-translated into English to maintain the consistency of the questions prior to data collection. Data collectors and supervisors were trained for two consecutive days, mainly on the objective of the study, ethical conduct of the research, and meaning of the questionnaire. The questionnaire was pretested on 5% of the HCWs one week prior to the actual data collection period at Wadu health center and Boditi town health center, in those who were not selected for the actual study, and close supervision was implemented by the investigator and supervisors. The completeness, consistency, and accuracy of the collected data were examined by the principal investigator on a daily basis. For the qualitative study, intensive and problem-oriented training was given to data collectors and supervisors. Pretesting of the probing questions was conducted in similar settings that were not included in the main research, and necessary modifications to the questions were incorporated.
Data Processing and Analysis
The quantitative data were cleaned, checked for completeness, and entered into EpiData version 3.1 statistical software package, then exported to SPSS version 20 for further analysis. Frequencies, means, standard deviations, and percentages were used to describe data. The odds ratio with 95% CI was calculated to ascertain the association between dependent and independent variables. Factors associated with the outcome variable, “tuberculosis infection prevention and control practice”, coded as “0” for improper practice and “1” for proper practice, were identified. Variables with a P-value less than 0.25 in the bivariate logistic regression analysis were taken into the multivariable logistic regression analysis. Hosmer and Lemeshow’s goodness-of-fit statistics were used to assess the fitness of the model (P ≥0.05). Multicollinearity was checked using a cut-off point based on the variance inflation factor >10 or tolerance test <0.1. The validity and reliability of the questionnaires were checked through Cronbach’s alpha, which was >0.89, and a P-value <0.05 was considered statistically significant. Finally, the results were presented as text and tables.
For qualitative data, the principal investigator transcribed each tape-recorded key informant interview, and notes taken in the field were read thoroughly and translated into English. Coding and categorizing were done using OpenCode version 4.02 software.25 Codes were given line by line and then related codes were categorized. Finally, thematic analysis was employed and the data was used to describe the quantitative findings.
Dissemination of Results
The findings of the study were disseminated to Wolaita Sodo University, School of Public Health, College of Health Sciences and Medicine, and Wolaita Zone Health Department.
Results
Socio-Demographic Characteristics of Health Care Workers
A total of 728 HCWs were enrolled in the study, with a response rate of 97.3%. The remaining 2.7% refused to participate. The mean±SD age of participants was 34.6±7.4 years. The majority of the participants, 426 (58.5%), were females and more than half of the participants, 396 (54.4%), were married. The HCWs had various professions: 23 (3.2%) were physicians, 333 (45.7%) were nurses, 122 (16.8%) were health officers, 93 (13.1%) were midwives, 83 (11.4%) were laboratory personnel, 42 (5.8%) were pharmacy personnel, and 29 (4%) were other health professionals. More than one-quarter of the participants, 217 (29.8%), were working in adult outpatient departments, emergency, and triage. The majority of participants, 507 (69.6%), were not trained in TB infection control (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Health Care Workers in Wolaita Zone, Southern Ethiopia, August 2020 (N=728) |
Knowledge of Tuberculosis Infection Prevention and Control Among Health Care Workers
Concerning participants’ knowledge of TBIPC, most participants responded correctly to knowledge-related questions. However, few correct answers were given to the questions “Tuberculosis cannot be transmitted from person to person by blood contacts”, 197 (27.1%), and “Mechanical ventilation is always not more effective than natural ventilation”, 320 (44.0%). Overall, 629 HCWs (86.4%) had good knowledge and 99 (13.6%) had poor knowledge (Table 2).
 |
Table 2 Knowledge of Tuberculosis Infection Prevention and Control Among Health Care Workers in Wolaita Zone, Southern Ethiopia, August 2020 (N=728) |
Attitude Towards Tuberculosis Infection Prevention and Control Among Health Care Workers
Overall, 487 HCWs (66.9%) had a positive attitude towards TBIPC and 241 (33.1%) had a negative attitude towards TBIPC (Table 3).
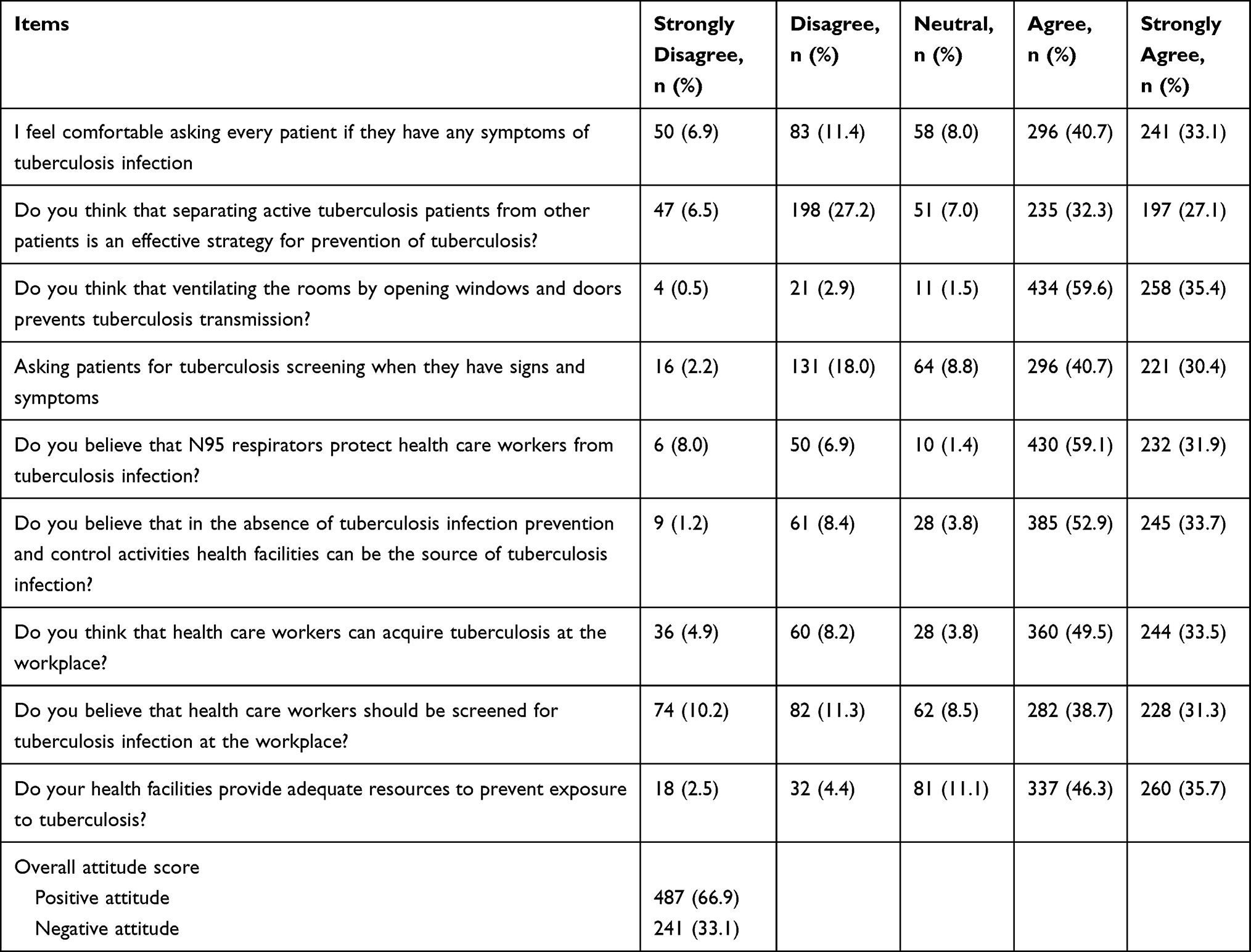 |
Table 3 Attitude Towards Tuberculosis Infection Prevention and Control Among Health Care Workers in Wolaita Zone, SNNPR, Ethiopia, 2020 (N=728) |
Tuberculosis Infection Prevention and Control Practice Among Health Care Workers
The overall proportion of proper TBIPC practice among HCWs was 44.78% (95% CI: 41.10–48.40). A total of 326 HCWs (44.78%) scored ≥80.0% but more than half of the respondents, 402 (55.22%), had improper TBIPC practice, scoring <80.0%.
Almost three-quarters of HCWs used N95 respirators when suspecting TB infection and interacting with patients, 571 (78.4%) and 561 (77.0%), respectively. More than two-thirds, 506 (69.5%), opened windows and doors to increase natural ventilation, and 439 (60.3%) explained to patients the importance of keeping windows and doors open. The qualitative study also showed that
… to tell you the reality, in our health center, some of the windows and doors were broken and cannot open easily, and also not parallel and suitable for cross ventilation. (33-year-old male participant)
More than half of the HCWs, 393 (54.0%), screened TB-suspected clients and over half, 378 (51.9%), placed TB-suspected clients in a separate waiting area. A respondent in the qualitative study also explained that
… in our health center, there was not enough room for tuberculosis clinic and also no separate waiting area for coughing and non-coughing patients, to promote tuberculosis infection prevention and control activities. (35-year-old male participant)
More than half of the HCWs, 415 (57.0%), provided surgical masks for TB suspects/TB patients to cover their mouth. The findings of qualitative study support that
… there are not enough surgical masks for tuberculosis patients and tuberculosis suspects. So that, they use locally prepared ordinary masks in health care facilities when they come to use services. This is because of a shortage of funds to purchase masks for our health center. (26-year-old female participant)
The majority of respondents, 594 (81.6%), asked each patient whether they had been coughing, and for how long (Table 4).
 |
Table 4 Tuberculosis Infection Prevention and Control Practices Among Health Care Workers in Wolaita Zone, SNNPR, Ethiopia, August 2020 (N=728) |
Factors Associated with Tuberculosis Infection Prevention and Control Practices
In the bivariate logistic regression analysis, age, sex, profession, service years, working in the TB clinic, anti-retroviral therapy (ART) clinic, and laboratory room, TB-related training, availability of personal protective equipment (PPE) (N95 respirators, surgical masks), knowledge, and attitude were factors significantly associated with TBIPC practices. However, only service years, working in the TB clinic and ART clinic, TB-related training, availability of PPE (N95 respirators, surgical masks), knowledge of and attitude towards TBIPC practice showed statistically significant associations with TBIPC practice in the multivariable logistic regression analysis.
HCWs who had more than 16 years’ work experience were 4.182 times more likely to properly practice TBIPC practices compared with those who had work experience of less than 5 years (AOR=4.182, 95% CI: 2.024–8.639). Those working in TB clinics (AOR=4.009, 95% CI: 1.311–12.261) were four times more likely to have proper practice in TBIPC, compared with those who were working in pharmacy departments.
HCWs who were working in ART clinics were 2.8 times more likely to have proper practice in TBIPC practices, compared with those who were working in pharmacy departments (AOR=2.796, 95% CI: 1.009–7.743). This finding also agrees with the qualitative results:
… Health care workers, those working in anti-retroviral treatment clinic, a tuberculosis clinic, and tuberculosis ward, are focused on tuberculosis infection prevention and control measures, and health care workers on the other departments are more focused on treatment parts rather than tuberculosis infection prevention and control measures. (28-year-old female participant)
In addition, HCWs who had ever taken TB-related training were about 20.024 times more likely to practice proper TBIPC than those who have not received training (AOR=20.024, 95% CI: 11.483–34.92). One participant said that
The majority of health care workers are not trained on tuberculosis infection prevention and control measures in our health facility and they don’t give attention to whether tuberculosis infection prevention and control activities are practiced as the standard or not. (30-year-old male participant)
HCWs who had good knowledge of TBIPC were 2.66 times more likely to properly practice TBIPC compared with those who had poor knowledge (AOR=2.66, 95% CI: 1.119–4.196), and HCWs who had a positive attitude towards TBIPC were two times more likely to properly practice TBIPC compared with those who had a negative attitude towards TBIPC (AOR=2.011, 95% CI: 1.242–3.255) (Table 5).
 |
Table 5 Bivariate and Multivariate Logistic Regression Analysis of Factors Associated with Tuberculosis Infection Prevention and Control Practices of Health Care Workers in Wolaita Zone, SNNPR, Ethiopia, August 2020 (N=728) |
Discussion
The level of proper TBIPC practice among HCWs in Wolaita Zone was 44.78% (95% CI: 41.10–48.40). Service years, working in TB and ART clinics, ever having had TB-related training, availability of PPE (N95 respirators, surgical masks) in the working room, and knowledge of and attitude towards TBIPC practice were shown to have statistically significant associations with proper TBIPC practice.
The findings of the present study revealed that the overall level of proper TBIPC practice was 44.78%. This finding is consistent with a study conducted in Addis Ababa, Ethiopia (48.0%).18 However, the current finding is higher than in studies conducted in Gondar University referral hospital (19.6%), West Gojjam Zone, Northern Ethiopia (38.0%), and in South Africa (36.4%).7–9 This difference may be due to differences in sample size, study period, study set-up, patient flow, and health facilities. The finding of the current study is lower compared with studies conducted in Ondo State, Nigeria (68.0%), Free State Province, South Africa (72.9%), North-Western Nigeria (85.3%), and India (53%).13–16,28
In this study, the number of HCWs using N95 respirators when suspecting TB infection was 571 (78.4%). This finding is consistent with a study conducted in Zaria, North-Western Nigeria (77.92%).14 However, the finding of this study is higher than in studies conducted in South Africa (52.2%); Addis Ababa (27.3%), West Gojjam Zone (23%), and Bahir Dar City administration (35.6%), Ethiopia; Free State Province, South Africa (38.8%); and Moyen-Ogooue Province, Gabon (54.4%); and a study conducted in China found that N95 respirators were not available for HCWs and surgical masks were not available for TB patients and suspects.7–9,13,20,26,27 The different results could be attributed to supply differences, study period, the current study being conducted during the coronavirus disease 2019 (COVID-19) pandemic, study setting, and type of health care facilities.
The current study found that taking steps to increase natural ventilation (by opening windows and doors when possible) was implemented by most HCWs, 506 (69.5%). This finding is much better than results from Addis Ababa (43.2%) and Northwest Ethiopia (64.9%).8,19 This discrepancy may be due to the current study settings using natural ventilation systems alone to increase ventilation or differences in weather conditions, with colder weather in Addis Ababa compared to the current study area. However, this finding is lower than in studies conducted in clinical trial sites in low- and middle-income countries (80.6%), and in North-Western Nigeria (88.5%).14,23 This discrepancy may be due to study set-up differences and variation in the weather conditions and type of ventilation system used.
In this study, 439 HCWs (60.3%) explained to patients why it was important to keep windows open. This finding is lower than in a study conducted in South Africa (91.8%).13 This inconsistency may be due to differences in the characteristics of the study population and study set-ups. The current study found that 393 HCWs (54.0%) reported that they were carrying out TB screening at their working unit. This finding is higher than in studies conducted in Uganda (43.0%) and in Addis Ababa, Ethiopia (27.0%).22,24
The present study also revealed that 378 HCWs (51.9%) separated TB suspects or TB patients from non-coughing patients. This finding is in line with studies conducted in South Africa (53.0%)13 and Uganda (54.9).24 However, the finding of this study is lower than in another study, conducted in Nigeria (65.0%).15 This difference may be due to differences in sample size, population characteristics, and study set-ups.
The results of the present study showed that 594 HCWs (81.6%) asked patients about their cough history. This finding is higher than in a study conducted in Ibadan, South-west Nigeria (40.0%).15 The difference could be attributed to the fact that TBIPC practice activities are currently receiving due attention, and the effect of the study period, the current study having been conducted during the COVID-19 pandemic.
The findings of the study illustrated that HCWs who had more than 16 years’ work experiences were 4.182 times more likely to practice properly compared with those who had work experience of less than 5 years. This finding is consistent with the findings of related studies from Bahir Dar City and West Arsi District, Southeast Ethiopia.17,20 This could be due to the fact that, as the number of service years increases, HCWs are more exposed to infection prevention and control standards and become more experienced.
HCWs who were working in the TB clinic and the ART clinic were four times and 2.79 times, respectively, more likely to properly practice compared with those who were working in pharmacy departments. This finding is consistent with a study conducted in West Gojjam Zone, Ethiopia.8 This could be due to the fact that the management of TB patients at TB clinics and ART patients linked to TB screening may emphasize TBIPC activities by HCWs in TB and ART clinics.
HCWs who had good knowledge were 2.166 times more likely to properly practice TBIPC compared with their counterparts. This finding is consistent with findings in Free State Province, South Africa.13 Also, respondents who had a positive attitude towards TBIPC practice were 2.011 times more likely to conduct proper practices compared with those who had a negative attitude. This finding is consistent with findings in South Africa and in Bahir Dar City administration.20,23 This may be due to the fact that knowing about TBIPC practice activities, infection prevention and control standards, and positive feelings provided a base for proper practice.
Conclusion and Recommendations
The proportion of proper TBIPC practices among public HCWs was low in the study area. The proper practice of TBIPC was determined by service years, working in the TB clinic and ART clinic, TB-related training, availability of PPE (N95 respirators and surgical masks) in the service rooms, and knowledge of and attitude towards TBIPC practices. Governments and other concerned bodies should facilitate good practice by providing TB-related training for HCWs and providing PPE for both HCWs and TB patients. For better intervention, further studies could focus on experimental research into possible factors that are responsible for TBIPC practices in health care facilities in the study area.
Abbreviations
AOR, adjusted odds ratio; ART, anti-retroviral therapy; HCW, health care worker; N95, not resistant to oil, and 95% filter efficiency; TBIPC, tuberculosis infection prevention and control practice.
Ethical Considerations
Before starting the study, the research protocol was submitted for consideration, comment, and approval to the ethical review committee (ERC) of the College of Health Sciences and Medicine, Wolaita Sodo University. Then, ethical clearance and approval was obtained from the ERC of the College of Health Sciences and Medicine (project number: CHSM/ERC/116), Wolaita Sodo University. Permission was also obtained from Wolaita Zone Health Department and Woreda Administrative Health Offices of the selected health care facilities. This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from each study participant and the participants’ informed consent also included the publication of anonymized responses. The participants’ confidentiality was completely maintained.
Acknowledgments
First and foremost, we would like to extend our appreciation to Wolaita Zone Health Department, Woreda Health Offices, and health facility managers for their cooperation in providing the information. We also extend our gratitude to Wolaita Sodo University, College of Health Sciences and Medicine, School of Public Health, for their guidance during study development. Furthermore, we would like to thank the data collectors, respondents, and supervisors for their overall support during the data collection process.
Author Contributions
All authors made a great contribution to the conception and design of the study, analysis and interpretation of data; took part in drafting, revising or critically reviewing the article; agreed to submit to the Journal of Multidisciplinary Healthcare; gave final approval of the revised version to be published; and agree to be accountable for all aspects of the work.
Funding
Funding for this study was made possible through grants offered by Wolaita Sodo University, Sodo, Ethiopia. But the University has no competing interest on manuscript writing or editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Guidelines on Tuberculosis Infection Prevention and Control. Geneva; 2019.
2. World Health Organization. Global Tuberculosis Report,Global TB Programme. Geneva: WHO/CDS/TB; 2019.
3. World Health Organization. Global Tuberculosis Report: WHO Global TB Programme. Geneva; 2016.
4. World Health Organization. Policy on TB Infection Control in Health-Care Facilities, Congregate Settings and Households. Geneva; 2009.
5. Anita S, Barsha T, Prem B, Rajendra R, Wagle RR. Health care workers’ knowledge, attitudes and practices on tuberculosis infection control, Nepal. BMC Infect Dis. 2017;17(1):724. doi:10.1186/s12879-017-2828-4
6. Asfaw A, Tadesse A, Nebiyu H, et al. Improvement in tuberculosis infection control practice via technical support in two regions of Ethiopia. BMC Infect Dis. 2018;18(1):557.
7. Lesley T, Bhebhe CVR, Wilhelm J. Attitudes, knowledge and practices of healthcare workers regarding occupational exposure of pulmonary tuberculosis. Afr J Prm Healthcare Fam Med. 2014;6(1):1–6.
8. Alene K, Yifiru S. Knowledge and practice of health workers about control and prevention of multidrug-resistant tuberculosis in referral hospitals, Ethiopia: a Cross-Sectional Study. BMJ. 2019;9:e022948.
9. Kassahun T, Wasie B, Azage M. Tuberculosis infection control practices and associated factors among health care workers in health centers of West Gojjam Zone, Northwest Ethiopia: a Cross-Sectional Study. BMC Health Serv Res. 2016;16(1):359. doi:10.1186/s12913-016-1608-y
10. Xiao-Ning W, Meng-Jie G, Yu-Dan S, et al. Prevalence of and risk factors for tuberculosis among healthcare workers in Chinese tuberculosis facilities. BMC Health Serv Res. 2018;7:26.
11. Chau Quy N, Giap Van V, Hanh Thi C, et al. Difficulties in tuberculosis infection control in a general hospital of Vietnam: a knowledge, attitude, and practice survey and screening for latent tuberculosis infection among health professionals. BMC Infect Dis. 2019;19(1):951. doi:10.1186/s12879-019-4593-z
12. Takele T, Girmay M, Medhin G. Latent tuberculosis infection and associated risk indicators in pastoral communities in southern Ethiopia: a Community Based Cross-Sectional Study. BMC Public Health. 2018;18(1):266. doi:10.1186/s12889-018-5149-7
13. Michelle E, Gladys K, Kigozi G, van Rensburg H. Factors associated with good TB infection control practices among primary healthcare workers in the Free State Province, South Africa. BMC Infect Dis. 2016;16(1):633. doi:10.1186/s12879-016-1984-2
14. Isiyaku O. Knowledge and practice of TB infection control by health care workers at national tuberculosis and leprosy training Centre, Zaria, North Western Nigeria. Acta Sci Med Sci.2019;3(1):38–46.
15. Kuyinu Y, Adeyeye O, Odugbemi B, Goodman O, Odusanya O. Tuberculosis infection control measures in health care facilities offering tb services in Ikeja local government area, Lagos, South West, Nigeria. BMC Infect Dis. 2016;16(126):1–7. doi:10.1186/s12879-016-1453-y
16. Wasiu O, Adebimpe W, Abdulwahab A, Shittu Maryam A. Infection prevention and control practices among health-care workers in tuberculosis clinics in Ondo State, Nigeria. Libyan J Med Sci. 2020;3:51–56.
17. Biniyam S, Geberemariyam G. Assessment of knowledge and practices of healthcare workers towards infection prevention and associated factors in healthcare facilities of West Arsi District, Southeast Ethiopia: a Facility-Based Cross-Sectional Study. BMC Health Serv Res. 2018;76:69.
18. Girma D, Gizaw Z. Assessment of knowledge and practice of health workers towards tuberculosis infection control and associated factors in public health facilities of Addis Ababa, Ethiopia: a Cross-Sectional Study. Archi Public Health.2015;73(15):1–9.
19. Temesgen C, Demissie M. Knowledge and practice of tuberculosis infection control among health professionals in Northwest Ethiopia. BMC Health Serv Res. 2014;14(1):593. doi:10.1186/s12913-014-0593-2
20. Kelemua G. Assessment of knowledge, attitude and practice of health care workers on infection prevention in health institution Bahir Dar City administration. Sci J Public Health. 2014;2(5):384–393. doi:10.11648/j.sjph.20140205.13
21. Adugna A. Southern Nations Nationalities and Peoples Demography and Health. EthioDemographyAndHealth.Org; 2017.
22. Admasu T, Edward A, Margoles L, Kacha E, Blumberg HM, Kempker RR. Infection control knowledge, attitudes, and practices among healthcare workers in Addis Ababa, Ethiopia. Infect Control Hosp Epidemiol. 2013;34(12):1289–1296. doi:10.1086/673979
23. Catherine G, Sally H, Melissa A, et al. Practices at the NIH/NIAID/DAIDS- supported clinical trial sites in low and middle income countries. BMC Infect Dis.2016;16(269):1–7.
24. Esther B, Suzanne V, Bart C, et al. Implementation of tuberculosis infection control in health facilities in Mukono and Wakiso districts, Uganda. BMC Infect Dis. 2013;13(1):360. doi:10.1186/1471-2334-13-360
25. ICT Services and System Development and Division of Epidemiology and Global Health. OpenCode 4.0. Umeå and department of public health and clinical medicine, Umeå University, Sweden; 2011. Available from: http://www.phmed.umu.se/enheter/epidemiologi/forskning/open-code/
26. Anja V, Bayode R, Pacome A, et al. Knowledge, attitudes and practices regarding tuberculosis amongst healthcare workers in Moyen-Ogooué Province, Gabon. BMC Infect Dis. 2021;21(486):2–7.
27. Guang Xue H, Marieke J, Guo Jie W, et al. Infection control and the burden of tuberculosis infection and disease in health care workers in china: a Cross-Sectional Study. BMC Infect Dis. 2010;10(1):313. doi:10.1186/1471-2334-10-313
28. Karishma K, Charlet J. Infection control prevention practices on pulmonary TB transmission among health care personnel of selected hospital in India. J Clin Diagn Res. 2018;12(11). doi:10.7860/JCDR/2018/36029.12235.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.