")
Back to Journals » Clinical Ophthalmology » Volume 15
Two-Step Transepithelial Photorefractive Keratectomy with WaveLight EX500 Platform for Adolescents and Adults with Low to Moderate Myopia: A 12-Month Comparative Evaluation
Authors Tangmonkongvoragul C , Supalaset S , Tananuvat N , Ausayakhun S
Received 30 August 2021
Accepted for publication 1 October 2021
Published 13 October 2021 Volume 2021:15 Pages 4109—4119
DOI https://doi.org/10.2147/OPTH.S336727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Chulaluck Tangmonkongvoragul,1,2 Sumet Supalaset,3 Napaporn Tananuvat,1,2 Somsanguan Ausayakhun1,2
1Department of Ophthalmology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 2CMU LASIK Center, Center of Medical Excellence, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 3Department of Ophthalmology, Chulabhorn Hospital, HRH Princess Chulabhorn College of Medical Science, Chulabhorn Royal Academy, Bangkok, Thailand
Correspondence: Chulaluck Tangmonkongvoragul
Department of Ophthalmology, Faculty of Medicine, Chiang Mai University, 110 Inthawarorot Road, Sri Phum, Muang, Chiang Mai, 50200, Thailand
Tel +66 53-935512
Fax +66 53-936121
Email [email protected]
Purpose: To compare the visual and refractive results obtained after two-step TransPRK using an EX500 excimer laser for low to moderate myopic correction in adolescents and adults.
Patients and Methods: Retrospectively, 91 eyes of 52 patients were categorized into four groups based on age and level of myopia. The demographics, data of efficacy, safety, predictability, stability, and post-operative complications were evaluated at 1, 3, 6, and 12 months post-operatively.
Results: At 1-month, adolescents with low myopia achieved the highest mean efficacy index (P =0.034). The efficacy indices continuously increased during the 1-year follow-up in all groups, except in adolescents with moderate myopia. The highest safety and efficacy indices were recorded in adolescents with low myopia at 1-year. Post-operative spherical equivalent within ± 0.50 D at 1 year was 48.75% of all treated eyes; however, the final mean refractive spherical equivalent (MRSE) was under-corrected in all groups. By month 3, the percentage of eyes that had grade 0.5 haze was most prevalent in adolescents with moderate myopia (P < 0.001).
Conclusion: two-step TransPRK using an EX500 proved to be an effective, predictable, stable and safe procedure for the correction of low to moderate myopia with or without astigmatism at 1 year. Adolescents with low myopia achieved the best-post-operative UDVA, efficacy and safety indices. Adolescents tolerated night visual problems and dry eye symptoms better than adults.
Keywords: transepithelial photorefractive keratectomy, TransPRK, adolescent, two-step PRK, EX500
Plain Language Summary
1. Two-step TransPRK using EX500 is an effective, predictable, stable, and safe procedure for low to moderate myopia with or without astigmatism correction during 1-year follow-up period.
2. The highest safety and efficacy indices at 1-year post-operatively were remarkable in the adolescents with low myopic group.
3. Post-operative mean refractive spherical equivalent (MRSE) tended to be under-corrected, possibly due to the PTK mode. Therefore, the surgeon may add a PRK laser treatment aiming to over-correct between −0.25 and −0.50 diopters to subtract the myopic shift from the PTK.
4. Adolescents were more tolerant of postoperative night visual problems and dry eye symptoms than adults. Early post-operative detection and aggressive dry eye treatment may be essential to prevent corneal haze and regression.
Introduction
Transepithelial photorefractive keratectomy (TransPRK) was introduced in 1990.1 The procedure offers no instrument contact with the eye, providing the patient with a comfortable intraoperative experience. In TransPRK, the precise, smooth bed-edge, and regular epithelial ablation is created by the laser in an equal diameter as the ablation zone, which is smaller than using alcohol or mechanical epithelial debridement. Consequently, TransPRK comes with the potential to minimize the size of denuding epithelium related to faster reepithelization. TransPRK seems to be superior to alcohol-assisted PRK for treatment of low to moderate myopia in terms of safety and efficacy indices;2 less postoperative pain;2,3 faster reepithelization and visual recovery;2–7 less tissue removal; less haze; and shorter surgery time.8,9 The suspected temporary toxicity of alcohol to limbal stem cells and residual corneal epithelium might be responsible for the increased pain and slower healing time.3,10,11 In 2004, Celik et al also reported the advantages of TransPRK over mechanical PRK, including less pain, less haze, and faster epithelial healing.12 Another technique is the use of epikeratome for epithelial removal and replacement after excimer treatment (epi on LASEK); however, the speed of wound healing was not much different from previously described techniques.13
There are two methods of TransPRK: (1) two-step laser ablation which removes epithelium by phototherapeutic keratectomy (PTK) followed by the PRK for refractive correction and (2) single-step laser ablation where both the epithelium and stroma are ablated simultaneously.14 Two laser platforms that can perform single-step TransPRK are SmartSurfACE (SCHWIND eye-tech-solutions) and Streamlight (WaveLight Allegretto Wave Eye-Q Laser; Alcon Laboratories). No clinical data regarding the outcomes of the Streamlight platform have been reported in Asian eyes. The US FDA approved PRK for patients over the age of 18, due to instability of refractive error in adolescents. However, in Thailand, the age of the patients is lowered to 16 years, for those students applying to military school that requires an emmetropia. This technique is preferred as it does not create a flap, thus minimizing the severity of possible eye trauma during military training. All patients must be informed with consent from the parents. This situation enables us to examine the results of refractive surgery in this age group.
To the best of our knowledge, there is only one report on two-step TransPRK performed with the PTK mode followed by wavefront-optimized ablation profile using the EX500 excimer laser.15 Our study aimed to evaluate the efficacy, predictability, stability, safety and post-operative complications of two-step TransPRK using the EX500 excimer laser for low to moderate myopic correction in patients under the age of 18 years compared to the older age group.
Patients and Methods
In accordance with the principle of the Declaration of Helsinki, this study was approved by the Research and Ethics Committee, Faculty of Medicine, Chiang Mai University. Additionally, due to the retrospective study design and the use of de-identified patient data, the reviewed board of Research Ethics Committee 4, Faculty of Medicine, Chiang Mai University waived the need for written informed consent.
Participants
The participants of this retrospective comparative study were consecutive patients with low to moderate myopia with or without astigmatism who underwent two-step TransPRK using WaveLight EX500 platform between July 2014 and December 2018 at Chiang Mai University LASIK center, Chiang Mai University Hospital, Chiang Mai, Thailand, with a 12-month post-operative follow-up. All procedures were performed by three surgeons (C.T., N.T., S.A.) with similar techniques. Inclusion criteria were as follows: primary myopia or compound myopic astigmatism; pre-operative manifest refraction spherical equivalent (MRSE) with 0.00 to −3.00 diopters for low myopia and −3.01 to −5.99 diopters for moderate myopia; stable refraction for at least 12 months; intraocular pressure less than 21 mmHg; a period without wearing contact lenses for more than 2 weeks; and no history of diabetes, autoimmune disease, ocular surgery or other eye diseases. Patients were categorized according to age, in either adolescent group (<18 years) or adult group (18–59 years).
Surgical Technique
The emmetropia was the aim in all treated eyes. Prior to surgery, each eye received three drops of topical anesthetic medication (Tetracaine hydrochloride 0.5%) followed by a periorbital scrubbing with povidone-iodine 10%. Then, a sterile surgical sheet was draped and the eyelid speculum was inserted. The eyes were rinsed with a balanced salt solution. No alcohol was used. All procedures were performed with the Wavelight EX500 excimer laser (WaveLight®; Alcon Laboratories, Ft Worth, TX, USA). PTK mode was used to ablate the corneal epithelium at a diameter of 8.3–8.9 mm with a depth of 50 µm, and stromal ablation was then performed with wavefront-optimized profile (WFO) using the Wellington nomogram. The laser parameters were as follows: wavelength, 193 nm; average fluency, 200 mJ/cm2; repetition rate, 500 Hz; and beam size, 0.95mm. The amount of ablation at each zone was determined by the software based on the WFO profile. Mitomycin-C (MMC) 0.02% was applied for 15 seconds, and then rinsed off with a cold balanced salt solution. A silicone hydrogel soft contact lens was placed for 7 days. Following surgery, topical moxifloxacin 0.5% combined with dexamethasone 0.1% eye drops (four times a day) and preservative-free artificial tears (every 1 hour for 1 week) were prescribed. The eye was examined at 1 day, 1 week, and 1, 3, 6 and 12 months post-operatively. After 2 weeks, the steroid eye drops were changed to fluorometholone 0.1% three times daily for the first month, twice daily in the second month, and then the dose was adapted according to the corneal haze. Preservative-free artificial tears were used every 1–2 hours for at least 1 month and then slowly tapered to once daily continuing up to 6 months.
Data Collection
The medical records of all eligible patients were reviewed for patient demographics and clinical data variables including manifest refraction, uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), keratometry, spherical equivalent and complications during the pre-operative, intra-operative, and post-operative visit at 1 day,1 week and 1, 3, 6 and 12 months. Post-operative complications, including corneal haze, night visual disturbance, and dry eye symptoms were accessed during every follow-up visit. Dry eye symptoms were recorded using a 5-point Likert scale from 0 (none) to 5 (severe). Corneal haze was assessed at the slit-lamp and graded using Hanna et al’s scale: 0 = no haze or clear; 0.5 = trace haze on oblique illumination; 1 = an opacity that could be seen on broad tangential illumination, and corneal cloudiness not interfering with the visibility of fine iris details; 2 = an opacity that could be faintly seen on direct focal illumination with mild effacement of fine iris details; 3 = an opacity that was easily visible on direct focal illumination and distorted iris detail somewhat; and 4 = an opacity that was visible without a slit lamp and obscured iris detail.16 The grading of night visual disturbance was as follows: 0 = no glare or halo; 1 = occasional experience of glare and halo with no disturbance on activities at night; 2 = the presence of glare and halo with mild disturbance on activities at night; 3 = the presence of glare and halo with moderate disturbance on activities at night; 4 = the presence of glare and halo with severe disturbance on activities at night; and 5 = the presence of glare and halo that is incompatible with activities at night.
Primary post-operative outcomes for each follow-up visit were efficacy and safety indices, and refractive results. The TransPRK efficacy index was calculated as the post-operative UDVA divided by the pre-operative CDVA. The TransPRK safety index was derived from the post-operative CDVA divided by the pre-operative CDVA. The predictability was defined as the refraction results consisted of the post-operative mean residual spherical equivalent (MRSE) and the percentage of eyes in which the post-operative spherical equivalent (SE) is within the range of ± 0.50, ±1.0, ±1.5, ±2,0 diopters (D) from the attempted correction. Our enhancement procedures generally got delayed until achieving stable refraction at 1 year. Patients with corneal haze had to wait at least 6 to 12 months for symptoms to improve before enhancement surgery. The criteria of enhancement depended on the patient’s visual satisfaction and residual corneal thickness.
Statistical Analysis
The demographic data and the surgical outcomes were descriptively analyzed as the frequency for categorical data (eg, number of eyes, patients, sex, cumulative percentages of eyes in each categorized refractive error, and the percentage of eyes in each classified corneal haze), mean ± standard deviation or range for continuous data (eg, age, UDVA, CDVA, sphere, cylinder, spherical equivalent, keratometric power, pachymetry, scotopic pupil size, post-operative UDVA, efficacy index, safety index, post-operative SE, and post-operative dry eye and night visual disturbance scores). The data between groups were compared by analysis of variance (ANOVA) for data with normal distribution, Kruskal–Wallis test for data with non-normal distribution, and Chi-Square test or Fisher exact test for categorical data. A P-value of <0.05 was considered statistically significant. The SPSS program (version 23; IBM Corp, Armonk, New York, USA) was used for data analysis.
Results
A total of 91 eyes were included in this study, with 64 eyes (36 patients) in the low myopia group and 27 eyes (16 patients) in the moderate myopia group. Pre-operative baseline characteristics are listed in Tables 1 and 2. All the adolescents (age <18 years, 32 patients) were male and the majority were 16 years old.
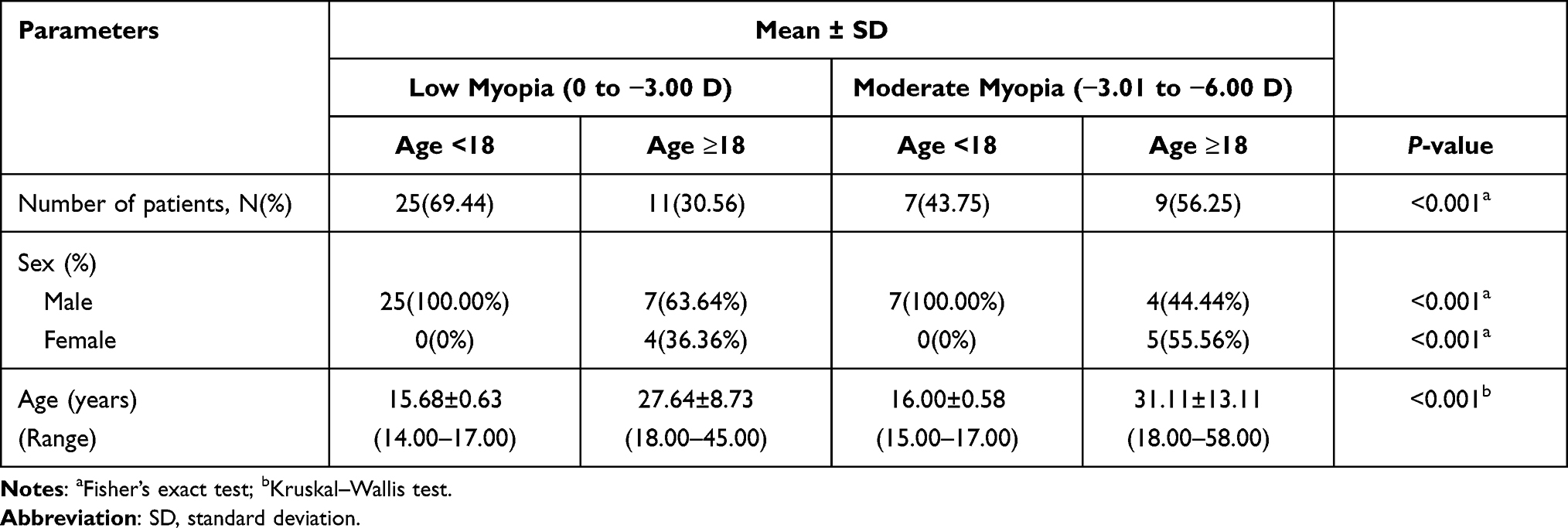 |
Table 1 Demographic Baselines of the Four Groups |
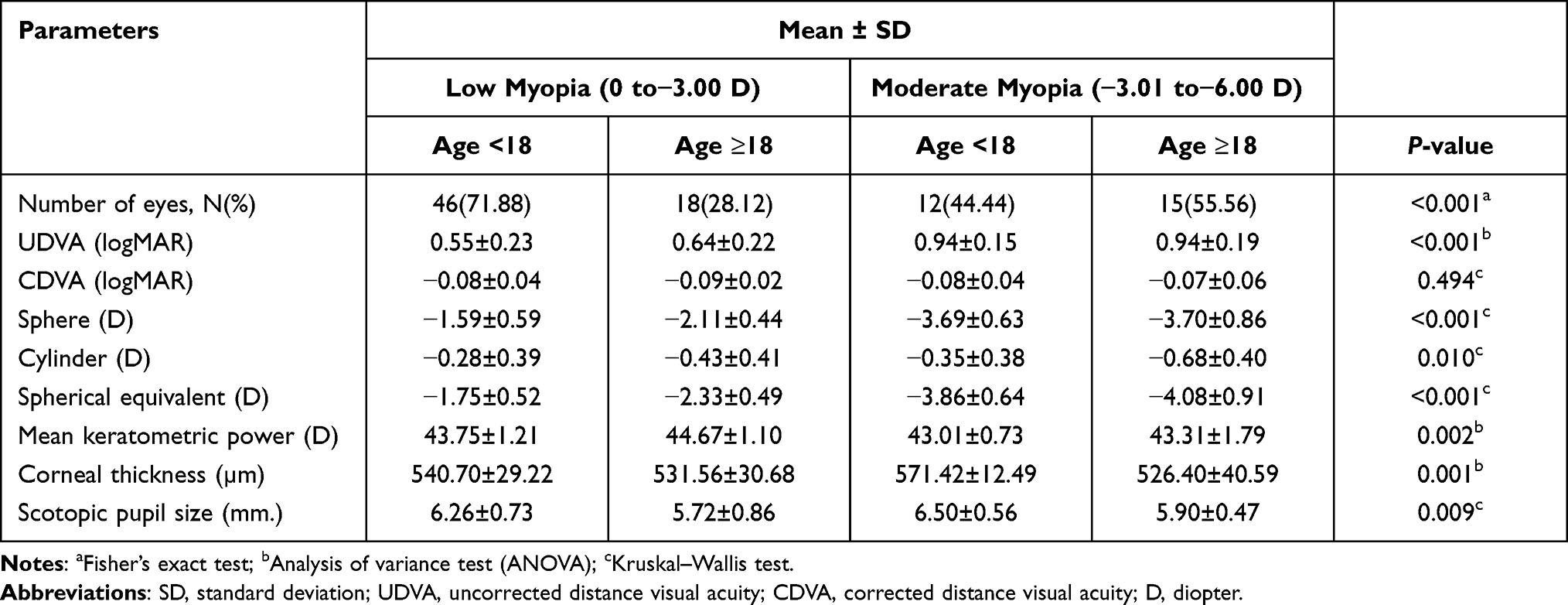 |
Table 2 Pre-Operative Baselines of the Four Groups |
Efficacy, Safety and Visual Acuity
The post-operative visual acuity outcomes were significantly improved at 1 month in all groups and continued improving up to 12 months in the low myopia group. One year after the operation, adolescents with low myopia significantly acquired best UDVA (logMAR −0.11±0.12) compared to the corresponding groups (Table 3). At the final visit, 5.56% (1 of 18 eyes) of adults with low myopia had a one-line loss of CDVA.
 |
Table 3 Post-Operative Efficacy, Safety and Visual Results of the Four Groups |
At 1-month follow-up, adolescents with low myopia achieved the highest mean efficacy index (0.92±0.33), whereas both moderate myopia groups had similar efficacy index results (P=0.034). The efficacy indices continued to increase during the 1-year follow up in all groups, except in adolescents with moderate myopia. The mean efficacy index was lowest in adolescents with moderate myopia at 1 year. This trend significantly corresponded to the mean UDVA result at 1 year (P=0.015), representing the reduction of predictability in this group. For the safety index, the results were stable at the 3-month follow-up in all groups (Table 3).
Refraction
Predictability and accuracy are shown in Figure 1. Post-operative SE within ± 0.50 diopters at 1 year in all treated eyes was 48.75%. For low myopia, the adolescents had SE within ±0.50 diopters and ±1.00 diopters more than the adults group at 1-year post-operatively, and vice versa for moderate myopia. By the last visit, all treated eyes were within the target ±2.00 diopters refraction.
 |
Figure 1 Post-operative spherical equivalent refractive accuracy at 12 months after TransPRK. |
The stability indices of refractive corrections are presented in Figure 2. One month after surgery, all groups had the MRSE within ±1.0 D, except in adults with low myopia. Final MRSE at 1 year tended to be under-corrected in all groups.
 |
Figure 2 The trends of the mean refractive spherical equivalent (MRSE) of eyes after TransPRK at pre- and post-operation at 1, 3, 6 and 12 months. |
MRSE in adolescents with low myopia (−0.45±0.61; P=0.001) was the nearest to emmetropia, compared to the other groups at 1 month post-operatively and gradually corrected towards emmetropia at 3, 6, and 12 months. MRSE in adults with low myopia was under-corrected at 1 month and gradually corrected towards emmetropia over time. There was myopic regression in adolescents with moderate myopia after 3 months post-operatively with a significant final myopic shift. In addition, a similar myopic regression was observed earlier in adults with moderate myopia from 1 to 3 months post-operatively, and then corrected towards emmetropia at 6 and 12 months.
Post-Operative Adverse Effects
Post-operative haze was assessed at each time point (Figure 3). By month 3, the percentage of eyes in adolescents with moderate myopia with grade 0.5 haze was significantly higher than the other groups (P<0.001). Grade 1 haze was only present in adult groups (11.11% and 20% of eyes in low and moderate myopia, respectively). After 12 months, haze in all eyes had cleared, except for one eye with grade 1 haze in the adults with low myopia group.
 |
Figure 3 Post-operative haze assessment at 3 months after TransPRK. |
Mean dry eye score in adults with moderate myopia was the most significant at every visit (Table 4). Night visual disturbance was the highest in adults with low myopia at every visit, but not statistically significant.
 |
Table 4 Post-Operative Dry Eye Score and Night Visual Disturbance After TransPRK |
Only one eye (5.56%) of adults with low myopia and one eye (8.33%) of adolescents with moderate myopia, required enhancement. After the enhancement, both eyes had final UDVA of at least 20/20. No other complications, such as infection or glaucoma, were reported in this study.
Discussion
There are several studies on two-step TransPRK using various platforms. In 2005, Lee et al compared conventional PRK, two-step TransPRK, and LASEK using the same laser system (Visx Star S3).7 The CDVA was similar in the three groups, but TransPRK resulted in a slight over-correction at 6 months post-operatively. However, our data demonstrated an under-correction in all groups. This discrepancy may be attributable to the different nomograms and laser techniques used in two different settings. When using Visx Star S3 during the PTK, some regions of the basal lamina and Bowman’s layer may be unintentionally ablated, which may explain the hyperopic shift.17 In 2007, Ghadhfan et al reported that two-step TransPRK using Nidek EC-5000 excimer laser provided slightly better visual outcomes than LASIK or LASEK in patients with low to moderate myopia.18 In 2009, Buzzonetti et al also showed good efficacy and safety of two-step TransPRK using the Flex scan algorithm PTK mode with the Nidek CXIII excimer laser.17
Until now, there was only one report of two-step TransPRK using the EX500 excimer laser (WaveLight) for the treatment of low to moderate myopia, published in 2015.15 The procedures started with the PTK mode at the depth of 50 µm followed by the standard nomogram for PRK, similar to our study. Compared with our results, they reported less efficacy (0.72 ± 0.31) and safety (0.99 ± 0.17) indices at 1-year follow-up, but similar results for stability and predictability indices. The previous study had a significant final under-correction with the MRSE at 1 year of −0.65 ± 0.69 D. Similar to our study, nearly half of the patients achieved the post-operative SE within ± 0.50 D at 1 year (48% vs 48.75%).15
Outcomes after treatment of low to moderate myopia were reported in 2016 by Naderi et al, using single-step TransPRK (SCHWIND eye-tech-solutions).2 The mean efficacy and safety indices were slightly different from our study (0.2 ± 0.16 and 1.36 ± 0.11, respectively). However, comparing the clinical outcomes between the two techniques of TransPRK is problematic due to variations in surgeons, surgical applications, laser platforms, nomograms, intra-operative and post-operative procedures. Therefore, identifying the method with the best outcomes remains elusive.
In our study, 91 eyes were observed for 1 year after two-step TransPRK. A high percentage of both low and moderate myopic eyes had good UDVA during a 1-year follow-up. In group analysis, the highest safety and efficacy indices were recorded in adolescents with low myopia at 1 year post-operatively. In 2018, Gomel et al published similar outcomes of PRK using B&L Keracor 217z excimer laser, indicating that younger age and low myopia were positively correlated with better safety and efficacy indices. Moreover, male gender was also associated with better efficacy index than female.19 In 2019, Hecht et al reported the visual outcomes in adolescents (<18 years, mean age = 17 years), with predominantly males (73%), after treatment using alcohol-assisted PRK with EX200 excimer laser (WaveLight). The adolescents show relatively more favorable outcomes with slightly better safety and efficacy indices and lower retreatment rates, than adults.20 From previous studies, superior results in the younger age group could be attributed to the more effective and faster healing properties of their corneas.
In the current study, the efficacy of visual outcomes, safety profiles, and refractive results at different periods after treatment were different between groups. For group analysis, adolescents with low myopia achieved the best post-operative UDVA, efficacy and safety indices as early as 1 month post-operatively and at subsequent follow-up visits. Adults with low myopia tended to have an under-correction in every visit. Because of lower accommodative capability, adults were more sensitive to post-operative residual myopia than adolescents, contributing to their lower efficacy index. One eye (5.56%) lost one line of CDVA and underwent enhancement with mechanical PRK. Adolescents with moderate myopia tended to have myopic regression after 3 months, which resulted in the lowest efficacy index at 12 months after surgery. This might relate to refractive instability in adolescents, but only one eye (8.33%) required enhancement. However, adults with moderate myopia had good results in both efficacy and safety indices.
For predictability, we observed under-correction over long-term follow-up in all groups. This result was similar to the study by Shapira et al, in which no eyes had an over-correction or hyperopic shift.15 We presumed that this finding might be from the PTK mode with two possible reasons. Firstly, the laser is programmed with an approximation of the uniform epithelial thickness. However, the human cornea has a different epithelial thickness which is approximately 53 µm at center and 65 µm at 8.0-mm at periphery.21 Our laser setting at 50-µm depth may be inadequate, which leaves some residual epithelium, resulting in a final result of under-correction. Secondly, laser tends to ablate more tissue in the periphery which may induce myopic shift.22 Single-step TransPRK with SmartSurfACE (SCHWIND eye-tech-solutions) and Streamlight (WaveLight Allegretto Wave Eye-Q Laser; Alcon Laboratories) claimed to eliminate this problem. For the Streamlight platform, the epithelial ablation utilizes the Optimized ablation profile, where more pulses are used outside the 4-mm zone to prevent epithelial remnants, but not enough to ablate into the stroma and induce a myopic shift. This platform using a card for Streamlight is more expensive than the conventional two-step TransPRK. Moreover, the platform has been introduced in Asia in late 2019 and no clinical outcomes in Asian eyes have yet to be reported.
During the operations, there were no complications. However, post-operative complications such as corneal haze, night visual disturbance, and dry eye were reported. Corneal haze formation is time-dependent. Several studies reported the peak incidence and severity of corneal haze is within the first 3 months.23 In our study, all groups had eyes with corneal haze, especially in adolescents with moderate myopia at 3 months post-surgery. The severity of haze was related to older age. However, corneal haze improved over time and at 1 year after surgery, all eyes were clear except one eye of an adult with low myopia still had grade 1 haze. Interestingly, Ang et al reported that the risk for early post-operative corneal haze increased with younger age and in patients with higher degrees of pre-operative myopia and astigmatism.24 According to faster re-epithelialization were both improved patient’s comfort and reduced the risk of haziness. The use of topical and systemic therapies such as basic fibroblast growth factor eye drops and L-cysteine oral supplements were the additional options that showed the benefit from more rapid corneal re-epithelialization and reduced haze.25–27
Adults with moderate myopia had the highest score of dry eye symptoms at every visit after surgery. Older age and a higher degree of laser correction were suspected to worsen the dryness. Younger people have a higher level of tears that help in epithelial cell viability and ameliorate dryness symptoms. Moreover, there is a higher prevalence of dry eye disease in advancing age.28 These could possibly hinder the healing process and affect the final outcome after TransPRK. Regarding one eye that still had haze at 1 year after surgery, the patient was a 45-year-old woman with low myopia in one eye. She had mild dry eye before surgery and developed epithelial healing line with severe punctate epithelial erosion at 1-week post-operatively. At 1 month, she developed grade 1 haze with myopic regression. Even after increasing steroids, the haziness was unchanged, and her final SE became more myopic shift. At 1 year, her vision was 20/40, and required enhancement. Dry eye in the early post-operative period may be responsible of corneal haze and myopic regression. A surgeon should be aware of this condition and rapidly initiate aggressive treatment to prevent unfavorable outcomes. For the night visual disturbance, symptoms were mostly found in adults, especially in low myopia groups, but there was no statistical significance. In 2013, Puell et al found that the halo size increases with age.29 Unfortunately, there was not sufficient evidence to show the relationship between age and night visual disturbance after TransPRK.
Our study is the first study to compare the outcomes of vision and post-operative complications of two-step TransPRK using EX500 between adolescents and adults with mild or moderate myopia. There have been a few trials that compared results between adolescents and adults using different laser machines and nomograms.19,20 Compared to the Streamlight, two-step TransPRK using EX500 required no additional cost to perform the procedure. To prevent under-correction from the PTK mode, the surgeon should add PRK laser to over-correct between −0.25 and −0.50 diopters to subtract that myopic shift.
Some limitations need to be addressed. First, adolescents were comprised mainly of 16-year-old males, so these results might not reflect younger or predominantly female adolescent populations. Second, this study had a relatively small sample size with a 1-year follow-up period, which prospective large-sample-sized with a long-term study is required in the future. Third, the data of pain scores and the epithelial healing times were not recorded. The epithelial defect could not be evaluated until the removal of bandage contact lenses at 1-week follow-up. Future studies may compare between single-step and two-step TransPRK using EX-500 excimer laser is needed in terms of visual and refractive outcomes. From our results, we presumed that early post-operative detection with aggressive dry eye treatment might be important to prevent corneal haze and myopic regression. This would also require further study.
Conclusion
During 1-year period, two-step TransPRK using EX500 excimer laser is an effective, predictable, stable, and safe procedure for low to moderate myopia with or without astigmatism correction. Adolescents with low myopia achieved the best post-operative UDVA, efficacy and safety indices from 1 month post-operatively. Adolescents were more tolerant to night visual problems and dry eye symptoms than adults.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (CT) upon reasonable request.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the principle of the Declaration of Helsinki, this study was approved by the Research and Ethics Committee, Faculty of Medicine, Chiang Mai University before initiated. This article does not contain any studies with animals performed by any of the authors.
Acknowledgments
We thank Barbara Metzler, a director of the Chiang Mai University English Language Team, Chiang Mai University and Dr Susama Choksuwattanaskul of the Chiang Mai University, for help with manuscript editing.
Author Information
Asst Prof. Chulaluck Tangmonkongvoragul completed her residency training in Ophthalmology at Chiang Mai University, Thailand (2008–2011) and corneal fellowship at Chulalongkorn University, Bangkok, Thailand (2012). She also completed her International corneal fellowship at Jules Stein Eye Institute of UCLA, Los Angeles, USA (2015). She took an international observership in lamellar corneal transplantation at University of Erlangen-Nuremberg, Germany (2016). Currently, she is an Assistant professor at the Department of Ophthalmology, Chiang Mai University, Thailand. Her fields of interest include and refractive surgery, ocular surface diseases, corneal infection, corneal transplantation, and eye banking.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive support from any organization for the submitted work.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Alio JL, Ismael MM, Artola A. Laser epithelium removal before photorefractive keratectomy. Refract Corneal Surg. 1993;9(5):395.
2. Naderi M, Jadidi K, Mosavi SA, Daneshi SA. Transepithelial photorefractive keratectomy for low to moderate myopia in comparison with conventional photorefractive keratectomy. J Ophthalmic Vis Res. 2016;11(4):358–362. doi:10.4103/2008-322X.194070
3. Fadlallah A, Fahed D, Khalil K, et al. Transepithelial photorefractive keratectomy: clinical results. J Cataract Refract Surg. 2011;37(10):1852–1857. doi:10.1016/j.jcrs.2011.04.029
4. Aslanides IM, Padroni S, Arba Mosquera S, Ioannides A, Mukherjee A. Comparison of single-step reverse transepithelial all-surface laser ablation (ASLA) to alcohol-assisted photorefractive keratectomy. Clin Ophthalmol. 2012;6:973–980. doi:10.2147/OPTH.S32374
5. Clinch TE, Moshirfar M, Weis JR, Ahn CS, Hutchinson CB, Jeffrey JH. Comparison of mechanical and transepithelial debridement during photorefractive keratectomy. Ophthalmology. 1999;106(3):483–489. doi:10.1016/S0161-6420(99)90135-5
6. Korkmaz S, Bilgihan K, Sul S, Hondur A. A Clinical and confocal microscopic comparison of transepithelial PRK and LASEK for myopia. J Ophthalmol. 2014;2014:784185. doi:10.1155/2014/784185
7. Lee HK, Lee KS, Kim JK, Kim HC, Seo KR, Kim EK. Epithelial healing and clinical outcomes in excimer laser photorefractive surgery following three epithelial removal techniques: mechanical, alcohol, and excimer laser. Am J Ophthalmol. 2005;139(1):56–63. doi:10.1016/j.ajo.2004.08.049
8. Bakhsh AM, Elwan SAM, Chaudhry AA, El-Atris TM, Al-Howish TM. Comparison between transepithelial photorefractive keratectomy versus alcohol-assisted photorefractive keratectomy in correction of myopia and myopic astigmatism. J Ophthalmol. 2018;2018:5376235. doi:10.1155/2018/5376235
9. Kaluzny BJ, Cieslinska I, Mosquera SA, Verma S. Single-step transepithelial PRK vs alcohol-assisted PRK in myopia and compound myopic astigmatism correction. Medicine. 2016;95(6):e1993. doi:10.1097/MD.0000000000001993
10. Browning AC, Shah S, Dua HS, Maharajan SV, Gray T, Bragheeth MA. Alcohol debridement of the corneal epithelium in PRK and LASEK: an electron microscopic study. Invest Ophthalmol Vis Sci. 2003;44(2):510–513. doi:10.1167/iovs.02-0488
11. Chen CC, Chang JH, Lee JB, Javier J, Azar DT. Human corneal epithelial cell viability and morphology after dilute alcohol exposure. Invest Ophthalmol Vis Sci. 2002;43(8):2593–2602.
12. Celik U, Bozkurt E, Celik B, Demirok A, Yilmaz OF. Pain, wound healing and refractive comparison of mechanical and transepithelial debridement in photorefractive keratectomy for myopia: results of 1 year follow-up. Contact Lens Anterior Eye. 2014;37(6):420–426. doi:10.1016/j.clae.2014.07.001
13. Magone MT, Engle AT, Easter TH, Stanley PF, Howells J, Pasternak JF. Flap-off epi-LASIK versus automated epithelial brush in PRK: a prospective comparison study of pain and reepithelialization times. J Refract Surg. 2012;28(10):682–689. doi:10.3928/1081597X-20120921-02
14. Adib-Moghaddam S, Soleyman-Jahi S, Sanjari Moghaddam A, et al. Efficacy and safety of transepithelial photorefractive keratectomy. J Cataract Refract Surg. 2018;44(10):1267–1279. doi:10.1016/j.jcrs.2018.07.021
15. Shapira Y, Mimouni M, Levartovsky S, et al. Comparison of three epithelial removal techniques in PRK: mechanical, alcohol-assisted, and transepithelial laser. J Refract Surg. 2015;31(11):760–766. doi:10.3928/1081597X-20151021-05
16. Hanna KD, Pouliquen YM, Savoldelli M, et al. Corneal wound healing in monkeys 18 months after excimer laser photorefractive keratectomy. Refract Corneal Surg. 1990;6(5):340–345. doi:10.3928/1081-597X-19900901-09
17. Buzzonetti L, Petrocelli G, Laborante A, et al. A new transepithelial phototherapeutic keratectomy mode using the NIDEK CXIII excimer laser. J Refract Surg. 2009;25(1 Suppl):S122–124. doi:10.3928/1081597X-20090115-08
18. Ghadhfan F, Al-Rajhi A, Wagoner MD. Laser in situ keratomileusis versus surface ablation: visual outcomes and complications. J Cataract Refract Surg. 2007;33(12):2041–2048. doi:10.1016/j.jcrs.2007.07.026
19. Gomel N, Negari S, Frucht-Pery J, Wajnsztajn D, Strassman E, Solomon A. Predictive factors for efficacy and safety in refractive surgery for myopia. PLoS One. 2018;13(12):e0208608. doi:10.1371/journal.pone.0208608
20. Hecht I, Achiron A, Ben Haim L, Sorin V, Mimouni M, Kaiserman I. Refractive surgery in the late adulthood and adolescent age groups. Graefes Arch Clin Exp Ophthalmol. 2019;257(9):2057–2063. doi:10.1007/s00417-019-04396-x
21. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ. Epithelial thickness in the normal cornea: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg. 2008;24(6):571–581.
22. Li Y, Yokogawa H, Tang M, Chamberlain W, Zhang X, Huang D. Guiding flying-spot laser transepithelial phototherapeutic keratectomy with optical coherence tomography. J Cataract Refract Surg. 2017;43(4):525–536. doi:10.1016/j.jcrs.2017.03.004
23. Chen L, Ye T, Yang X. Evaluation of the long-term effects of photorefractive keratectomy correction for myopia in China. Eur J Ophthalmol. 2011;21(4):355–362. doi:10.5301/EJO.2011.6226
24. Ang BC, Foo RC, Lim EW, et al. Risk factors for early-onset corneal haze after photorefractive keratectomy in an Asian population: outcomes from the Singapore Armed Forces Corneal Refractive Surgery Programme 2006 to 2013. J Cataract Refract Surg. 2016;42(5):710–716. doi:10.1016/j.jcrs.2016.01.047
25. Scorolli L, Meduri A, Morara M, et al. Effect of cysteine in transgenic mice on healing of corneal epithelium after excimer laser photoablation. Ophthalmologica. 2008;222(6):380–385. doi:10.1159/000151691
26. Meduri A, Scalinci SZ, Morara M, et al. Effect of basic fibroblast growth factor in transgenic mice: corneal epithelial healing process after excimer laser photoablation. Ophthalmologica. 2009;223(2):139–144. doi:10.1159/000187686
27. Meduri A, Scorolli L, Scalinci SZ, et al. Effect of the combination of basic fibroblast growth factor and cysteine on corneal epithelial healing after photorefractive keratectomy in patients affected by myopia. Indian J Ophthalmol. 2014;62(4):424–428. doi:10.4103/0301-4738.119420
28. Gipson IK. Age-related changes and diseases of the ocular surface and cornea. Invest Ophthalmol Vis Sci. 2013;54(14):Orsf48–53. doi:10.1167/iovs.13-12840
29. Puell MC, Pérez-Carrasco MJ, Barrio A, Antona B, Palomo-Alvarez C. Normal values for the size of a halo produced by a glare source. J Refract Surg. 2013;29(9):618–622. doi:10.3928/1081597X-20130819-03
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.