")
Back to Journals » Open Access Journal of Contraception » Volume 15
United States Government-Supported Family Planning and Reproductive Health Outreach in the Democratic Republic of the Congo: Lessons Learned and Recommendations
Authors Ibrahimi S , Youssouf B, Potts C, Dumouza A, Duff R, Malaba LS, Brunner B
Received 24 October 2023
Accepted for publication 20 February 2024
Published 5 March 2024 Volume 2024:15 Pages 13—21
DOI https://doi.org/10.2147/OAJC.S446263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Sahra Ibrahimi,1– 3 Bamba Youssouf,4 Christine Potts,1 Alexandre Dumouza,1 Rani Duff,1 Landry-Serges Malaba,1 Bettina Brunner1
1International Development Division, Abt Associates, Rockville, MD, USA; 2Department of Global Health, Denison University, Granville, OH, USA; 3Department of Family Science, School of Public Health, University of Maryland, College Park, MD, USA; 4Matchboxology, Johannesburg, Gauteng, province, South Africa
Correspondence: Sahra Ibrahimi, Global Development Group, Abt Associates, 6130 Executive Blvd, Rockville, MD, USA, Tel +1 413-406-4401, Email [email protected]
Background: In response to limited contraception availability and a lack of knowledge about family planning (FP) in the Democratic Republic of the Congo (DRC), the United States Agency for International Development (USAID) Integrated Health Program (IHP) in the DRC has been providing FP services, including outreach programs in the DRC. Our study aims to assess the FP outreach program by understanding the participants’ perception of the campaign, its impact on their behavior, and their feedback regarding the campaign. Additionally, we draw insights from lessons learned and provide recommendations.
Methods: Between July and August 2022, we conducted 47 in-person participant interviews with women of reproductive age who used the outreach services provided by USAID IHP. Participants were randomly selected from Sud-Kivu, Kasai-Oriental, Haut-Katanga, and Tanganyika provinces. Consent and confidentiality were assured, and responses were recorded and transcribed in a Word document. We used Excel for data coding and analysis.
Results: The campaign reached 95.7% of women interviewed; however, some participants could not recall specific message details. Most respondents (89.3%) reported that the campaign motivated them to make FP decisions and change their behaviors. While 14.8% of women reported making FP decisions independently, 85.1% reported making the decision jointly with their partners. Our analysis resulted in three emerging themes: 1) Increased FP outreach and improved perception of FP, 2) Improved perceived behavioral changes due to FP outreach, and 3) The need for program improvement by including men and providing additional information about possible FP side effects.
Implications: Our study provides insights into how women receive information and whether they find it useful and share it with other women in their community. In particular, women’s feedback about the FP outreach program and our recommendations can inform future policies and interventions.
Keywords: DRC, family planning, reproductive health, community outreach, USAID
Corrigendum for this paper has been published.
Introduction
Universal access to sexual and reproductive health-care services including family planning (FP) is one of the global health priorities highlighted by Sustainable Development Goal 3.1 In addition to enabling women to space pregnancies and have their desired number of children, FP lowers child and maternal mortality and contributes to poverty reduction.2,3 From 2013 to 2022, the Democratic Republic of the Congo (DRC) experienced a slight improvement in reproductive health (RH) indicators; for example, the prevalence of contraception use increased from 8% to 16%, and the fertility index fell from 7 to 6.2 children per woman.4,5 However, barriers to accessing and adopting FP remain, and these barriers include insufficient FP/RH awareness and education, misinformation and hesitation due to contraceptive side effects, opposition from male partners, religious concerns, and patriarchal cultural norms which reinforce the role of men as primary decision makers.6–8
FP outreach and educational programs are important in raising awareness and improving informed decision making about FP in the community. A systematic review of evaluations of FP interventions in developing countries shows that community-based outreach interventions led to an increased use of contraception among women.9 In rural DRC, women have indicated openness to learning and using FP and modern contraceptive methods.8 However, misinformation and lack of information are key barriers to FP uptake in the DRC,8 while FP education in that area has been shown to be significantly positively associated with intention to use FP.10
The USAID Integrated Health Program in the Democratic Republic of the Congo (USAID IHP) works closely with the Government of the DRC’s Ministry of Public Health, Hygiene, and Prevention (MSPHP), along with other stakeholders, to strengthen their capacity in delivering high quality, integrated health services in several health areas, including FP. The USAID IHP is the largest USAID health project in the DRC. Initiated in January 2018, the Program has been implementing family planning (FP) activities in nine provinces since its inception and is scheduled to conclude in May 2025. Additional USAID implementing partners currently active in the DRC, providing FP activities, include Momentum Safe Surgery in Family Planning and Obstetrics,11 and Momentum Integrated Health Resilience.12 These programs focus on the training of providers, FP consultations, or the provision of FP products and reproductive health surgeries.11,12
USAID IHP aims to increase the use of FP services through raising awareness and disseminating information on FP by organizing mini campaigns, home visits by community-based distributors, large-scale media campaigns via community radio, and raising awareness in markets, churches, and schools by community relays and community leaders. To reduce barriers related to access to information, USAID IHP has set up confidential centers where adolescents and young people meet to obtain information and discuss with their peers questions of sexual and reproductive health. The information provided in these campaigns covers topics such as birth spacing, methods of contraception, where to access FP products and services, their use, menstrual hygiene, and other issues of sexual and reproductive health for adolescents and young people such as sexually transmitted infections (STIs.)13
While the literature notes unmet FP need and shows the effectiveness of FP campaigns in expanding FP uptake in low- and middle-income countries,14 little is known about the impact of FP outreach on knowledge, attitudes, and practices (KAP) in the DRC,7 and there is no published study on the effects of the USAID IHP’s FP outreach. This qualitative study aims to understand participants’ perception and attitude towards FP outreach. Objectives include a) understanding whether women noticed FP campaigns, and if yes, what were their perception of the campaign messages; b) whether they believed the campaign had any impact on their behavior change intentions; and c) what was their feedback on the FP messaging campaign including what they thought was useful and what was missing. This study is essential in understanding the effectiveness of current USAID IHP programming and what the program can do to improve outreach and further meet the needs of women in DRC. This study can also provide insight for future interventions.
Materials and Methods
Sampling and Data Collection
Participants were selected through random sampling in Sud-Kivu, Kasai-Oriental, Haut-Katanga, and Tanganyika, where USAID supported the implementation of FP/RH outreach and activities. Recruitment of participants occurred at or near health facilities, local markets, educational institutions, and their homes. The target respondents were sexually active women of reproductive age (18–49 years old) with diverse relationship statuses, education levels, and geographic distribution.
Data were collected through in-person interviews at health venues, where confidentiality was ensured. Additionally, informed consent was received verbally from all participants and recorded on forms before interviews and participation. The participants’ informed consent included permission for the publication of anonymized responses. The questionnaire was developed by the USAID IHP team, led by partner Matchboxology and pre-tested in Lubumbashi. A total of 48 participants were contacted to be interviewed, and 47 of them participated in the interviews, conducted from July 3, 2022, to August 3, 2022. One participant could not be interviewed because she stated that her plan to participate had changed, and she did not mention why. The 47 women interviewed included 12 each in Sud-Kivu, Haut-Katanga and Kasai-Oriental, and 11 in Tanganyika. We received Institutional Review Board (IRB) from Abt Associates on June 1, 2023. Our study complies with the Declaration of Helsinki.
Interviewers were female and trained in interview techniques, accurate data collection, and confidentiality and data security. At the beginning of the interview, the interviewers introduced themselves and the USAID IHP project. Additionally, each interview session was audio recorded with the consent of the participant. Responses were recorded in French or a local language, with verbatim translation where needed for additional information capture. Data were transcribed in a Word document, and then transferred into an Excel file for disaggregation and analysis.
Measurement and Analysis
Family planning outreach recall was assessed by asking women the following three questions,
Have you noticed any USAID information campaigns about family planning or reproductive health in the area you live or work? Can you remember what the message was telling you? Where do you normally get advice or information about family planning and reproductive health?
In addition, to find out whether participant’s perception of the campaign may have contributed to active FP and RH decision making, women were asked,
Did the messaging motivate you to make any decisions regarding your family planning or reproductive health? Did you decide on your own or with a partner? Has it made you change your behavior in an ongoing way?
Furthermore, to assess whether participants share messages and information with family, partners, and community members, women were asked, “Did you share messaging information from the campaign with anyone? Who?” To gain insights for ongoing campaign refinements and future recommendations, participants’ feedback was obtained by asking,
What do you think about public health campaigns? What would you change about the campaign or specific messages to make it more helpful and effective? Do you have any questions [related to family planning] for me?
Finally, to measure the demographic distribution of the sample, questions were asked about age, marital status, education, employment status, and parity (number of children).
Based on the distribution of the data, we categorized age into two groups: 18–29 and 30 and above. Marital status was categorized into married, single, and relationship. Education was grouped into no education, primary, secondary, or higher. Employment status was classified as student, employed, and unemployed or housewife. Parity was grouped as 0–1 child, 2–4, and 5 or more. We used a codebook to organize, code, and analyze data in Excel. Three major themes emerged from the data analysis: 1) Increased FP outreach and improved perception of participants about FP, 2) Improved perceived behavioral changes due to FP outreach, and 3) The need to include men and provide additional information about possible FP side effects.
Results
Table 1 presents the demographic characteristics of our sample. About 53% of participants were aged between 18 and 29, and the remaining 47.8% were 30 years or older. Most participants were married (46.8%) or in relationship (31.9%), and about 21% were single. While the majority had primary (38%) and secondary or higher education (40%), some women had no education (8.5%). In terms of employment, the majority were unemployed and housewifes (51%) compared to 19% employed, and 23.4% students. Unemployment was highest among women in Kasai-Oriental providence (n = 9). About half of the participants had one or no child (44.6%), 40% had 2–4 children, and some other women had five or more children (14.8%).
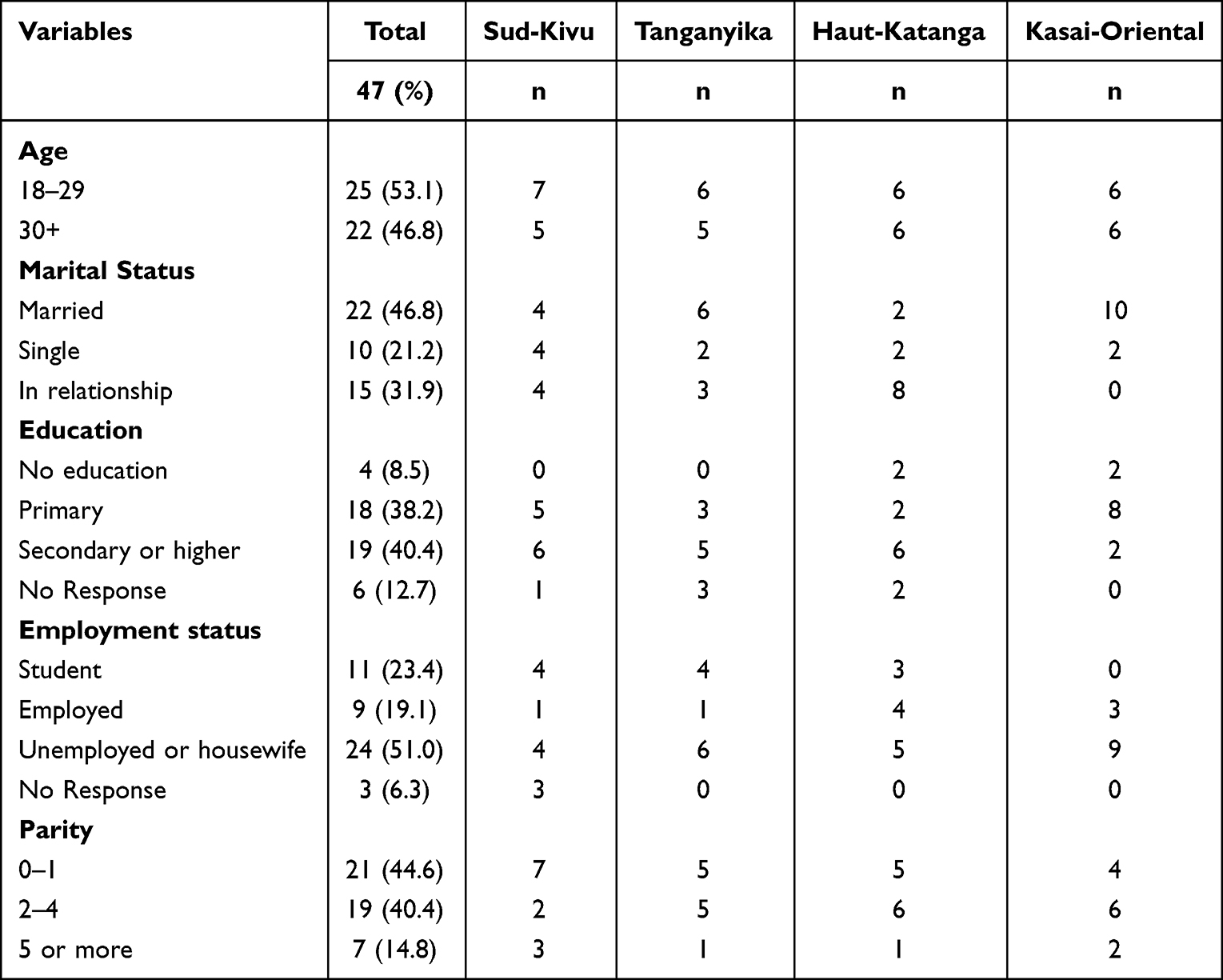 |
Table 1 The Characteristics of Study Participants by Province, DRC 2023 |
Increased Family Planning Outreach and Improved Perception of Participants About FP
USAID IHP’s FP campaign reached 95.7% of women interviewed (Table 2). Women reported noticing USAID FP/RH information campaigns about birth spacing, contraceptive methods, where to access and how to use contraception, menstrual hygiene, and sexually transmitted diseases. Several women shared:
Yes, we noticed these campaigns showing how vulnerable mothers should plan births, and the different methods to use for family planning.
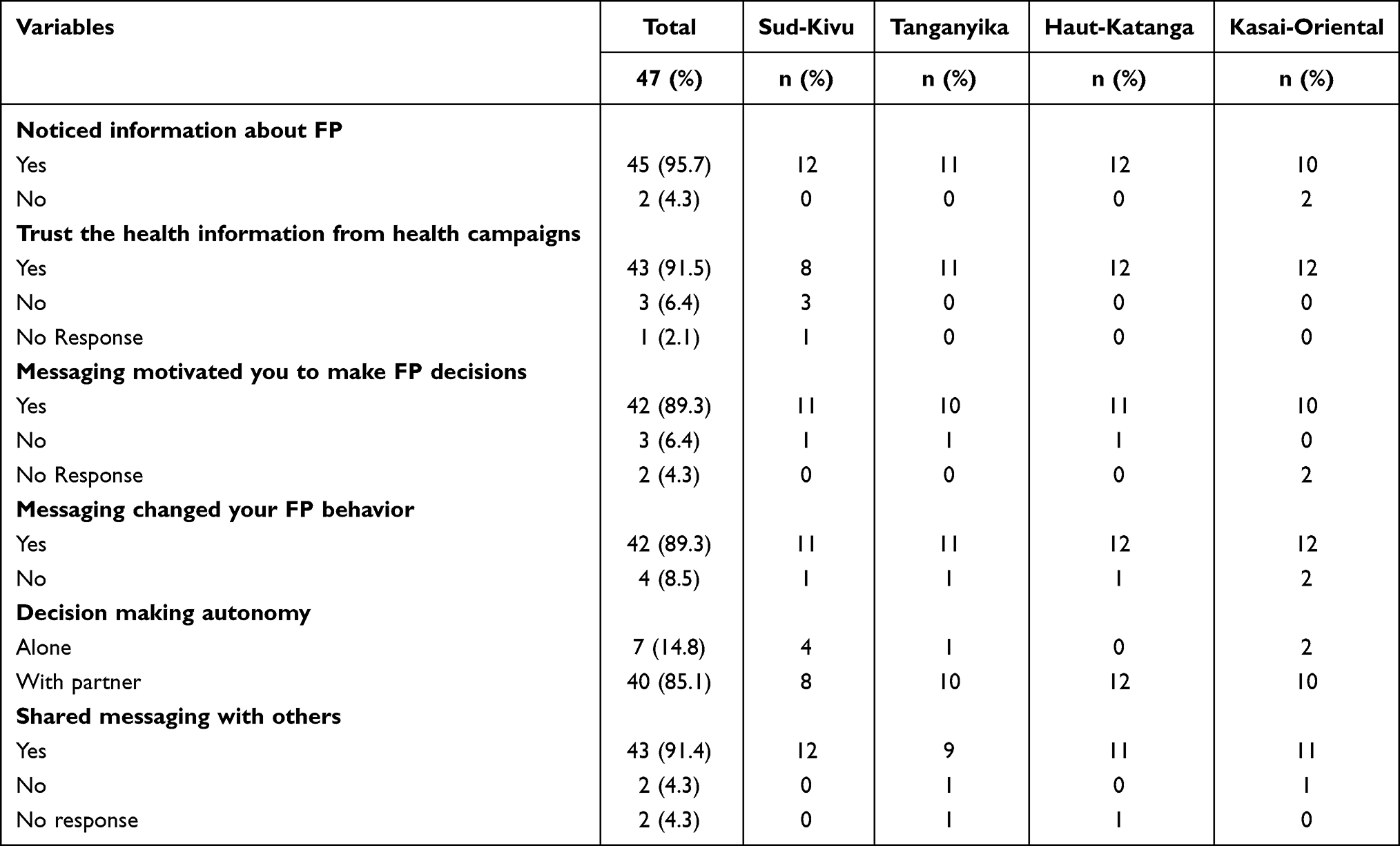 |
Table 2 Summary of FP Outreach and Participant’s Perception and Behavior Change |
Another woman said:
Yes, I have already been made aware of the FP and RH campaign… hygiene, prevention of sexually transmitted infections, [and] treatment as a couple in the event of STIs.
However, several answers to the prompts reflect that women could not describe or recall more detailed information that was shared. Among the campaign messages delivered, women’s perception and recall of outreach on birth spacing and its benefits was the highest. For instance, when women were asked, “Can you remember what the message was telling you?” several women stated:
It [the message] was about family planning so to give birth you have to wait at least 2 years like me; I just conceived three years and eight months after my last birth.
Many women also highlight the benefit of FP and birth spacing:
The message was saying that it is necessary to plan the births for a better life because some people give birth a lot and unfortunately lack the means to educate the children and to clothe them.
Similarly, other women mentioned:
The message said FP helps us to space births. Given the precariousness of life that pushes some parents to abandon their children on [the] street. We must plan births to avoid this problem.
Women reported receiving FP/RH information in health facilities, hospitals, schools, and churches, as well as by radio, media, community workers, and relatives. For example, several women mentioned:
I get these messages in health centers, through radio channels, in the church, through the teaching of mothers, and even community workers who go to the house raising awareness on FP by different methods.
Furthermore, data shows frequent sharing of information among people in all provinces. The majority of women (91.4%) indicated sharing some type of FP outreach with friends, sisters, or other family members, including partners. This sharing of knowledge aids in expanding outreach even further.
Improved Perceived Behavioral Changes Due to FP Outreach
As indicated in Table 2, 89.3% of women reported that the campaign and outreach programs had motivated them to make FP/RH decisions and change their behavior in an ongoing way. As an example, one woman said:
Thanks to this message I managed to space all my births because before that I was giving birth every year.
Another woman stated:
These messages are good and motivate me. I call on other women to listen to them and follow them because for me I no longer give birth every year and it’s good for my life.
As for whether the messages had changed their behavior, most women responded positively. Two main messages that motivated women to consider FP were about the benefits of FP on health and financial well-being (eg, being able to provide for their children). One woman asserted:
I was motivated first by my state of health – sometimes it happens after I have a child-- The womb can deteriorate and sometimes even heavy bleeding, and [second because of] the [the need for] providing for the lives of children.
When asked whether they decided about FP/RH on their own or with a partner, only 14.8% women (four single and three married) stated they had decided on their own. In contrast, 85.1% of the women (six single and nineteen married) reported having made the decision with their partner. A couple of women mentioned:
When I followed the messages, I told my husband about it, and we decided on the [FP].
Improving the Program by Including Men and Providing Information About FP Side Effects
The women also had some feedback on how to strengthen the campaigns and make them more effective. Most women recommended educating not only women but also men about FP/RH through these campaigns. Some women also suggested to “add training and multiply awareness sessions in the community.” Utilizing various mediums to continue to spread messages was also common feedback for ensuring the campaigns reached as many people as possible. Several women made comments similar to the following:
I think you have to talk to men because the decision comes from them.
Please involve men in those FP/RH campaign so that they will support us for it.
When asked if they trusted the health information that comes from the public health campaigns, 91.5% of women responded “yes”, in comparison with 6.4% who said “no”, while 2.1% did not respond. The concerns among those 6.4% of women who did not trust the information from the campaign were related to possible side effects of contraception that were not communicated during the FP campaign. For example, one woman stated, “I don’t trust health campaigns because they never talk about undesirable effects”, and another woman mentioned, “I don’t have 100% confidence in public health campaigns because we have noticed undesirable effects related to contraceptives.” Trust was lowest in Sud-Kivu providence (n = 3).
However, several of the women expressed trust and confidence, highlighting the importance of learning about contraceptive methods. One woman said:
I have confidence in health campaigns because of contraceptives effectiveness and we consult qualified personnel in health facilities. But we wish to interact more with nurses.
Another woman stated:
This campaign is good because it helps the person to develop further her contraceptive methods.
Finally, some common questions from respondents centered around contraceptive use, asking:
How can we know the best contraceptive method for us?
Is it necessary to go to [a] health facility before using contraceptives?
Do those who use the injection as a means of contraception no longer see their periods?
Discussion and Recommendations
Our findings show that women noticed FP messages from various platforms, shared them with other community members, and found them useful in improving their FP/RH decision making. This indicates the positive contribution of USAID IHP in raising awareness about FP and RH. Additionally, about 55% of women (n=26) were able to recall the message about the link between family planning/birth spacing and financial health/ability to care for and educate current children. This conveys that many women are not only concerned about adverse health outcomes due lack of FP, but they are also concerned about the economic consequences of it. This finding is aligned with previous studies that showed partners, who were educated about the benefits of FP regarding families’ economic well-being, were more likely to attend FP services.15 Therefore, future FP campaigns should focus on both the health and economic benefits of FP.
Furthermore, in some cases, narrative comments from the women reflect that male partners lack information about FP and RH yet hold some or all of the couple’s decision-making power. Previous research also shows that in developing countries, often FP decisions are not made only by women but rather jointly with their husband or their husband make the decision for them.16–19 Educating women alone about FP may also lead to spousal violence as some women may encounter resistance from their partner about use of contraception.20 Therefore, we recommend FP campaigns increase focus on men and include effective and evidence-based FP outreach programs aimed directly toward men.
Our data also shows that about 27.6% of women (n = 13) could not describe or recall more detailed information that was shared with them through these campaigns. Placing details in a story context and/or tying them to common everyday life analogies may improve internalization and retention. Research shows that the use of stories or storytelling can be effective in sharing knowledge, as stories can yield knowledge, attitudes, beliefs and behaviors from individuals by displaying a simple image.21 We also recommended that future USAID FP outreach programs include early-stage co-creation with women and partners, along with short longitudinal specific content recall/internalization testing prior to launch and scale-up. According to Synder, conducting formative research with members of the community, including community boards and even hiring local staff can create a viable campaign which could result in a robust program.22 Additionally, a mid-program or mid-campaign dipstick evaluation on beneficiary perception and experience of campaign structure (in addition to content recall/update indicators) may be useful for strategic iteration.
Finally, several women indicated a desire for more extensive information about FP methods, especially regarding side effects. Many women are aware of the side effects of contraception through personal experiences. For example, some women shared concerns about the stopping of menses. Some prefer that the FP method does not interfere with menstruation. Women did not know about scheduled bleeding or amenorrhea. Some women pointed out that the potential side effects of contraception were not communicated by health professionals or the campaigns. If such interventions and campaigns are not transparent and explicit about the side effects, it can erode community trust in the campaigns.
Educating women and discussing possible side effects of contraception not only builds trust but also offer additional benefits, such as empowering women to make informed choices and actively participate in their healthcare.23 Moreover, being aware of potential side effects can enhance patient compliance. When individuals are prepared for potential temporary discomfort or changes in their bodies, they are more likely to continue using the chosen contraceptive method as prescribed, thus reducing the risk of discontinuation.23 Additionally, since every individual’s body reacts differently to medications, including contraceptives, discussing side effects enables healthcare providers to tailor their recommendations based on a patient’s medical history, lifestyle, and preferences. This ensures not only reduced side effects but also a more personalized and effective contraceptive method.23
Our study also has some limitations. While interviewers asked specifically about USAID FP campaigns, there could be a small number of women who may have heard about FP from other sources and might be unable to discern or accurately remember if it was from a USAID campaign or another source. In addition, the generalizability of these findings may be limited due to the small sample size. However, our study provides insight as to how women receive information and whether they find the information useful and pass it to other women in their community. In particular, women’s feedback about the FP/RH campaign and our recommendations can inform future FP programs and interventions.
Conclusion
Our study shows that, overall, the USAID IHP’s FP campaigns had a positive impact on communities in the DRC. Women noticed and shared FP messages, particularly recognizing the link between FP and financial well-being. Therefore, the program helped with informed FP/RH decision-making and women’s perceived behavior changes. However, our study also highlights the need to target men in these campaigns and improve information retention. Additionally, transparent communication about side effects is essential to maintain community trust. Despite limitations, our research provides valuable insights for future FP programs, emphasizing the importance of including both women and men in outreach efforts and continuous evaluation.
Ethics Approval and Informed Consent
We received Institutional Review Board (IRB) from Abt Associates on (on June 1, 2023). Data were collected through in-person interviews at health venues, where confidentiality was ensured. Additionally, informed consent was received verbally and recorded on forms. The participants’ informed consent included permission for the publication of anonymized responses. We only interviewed participants between ages 18 to 49 and participants under the age of 18 were not considered for this study.
Consent for Publication
All authors consent to the publication of this manuscript and its content.
Acknowledgments
We thank Dr. Richard Matendo, USAID DRC, Dr. Houleymata Diarra, and Dr. Narcisse Embeke for their leadership of USAID IHP and this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by United States Agency for International Development (USAID) in accordance with the Integrated Health Program. Contract No: AEP-C-72066018C00001.
Disclosure
The authors report no conflicts of interest in this work.
References
1. SDG Goal 3: good Health and Well-being. UNICEF DATA. Available from: https://data.unicef.org/sdgs/goal-3-good-health-wellbeing/.
2. Casey SE, Gallagher MC, Dumas EF, Kakesa J, Katsongo JM, Muselemu JB. Meeting the demand of women affected by ongoing crisis: increasing contraceptive prevalence in North and South Kivu, Democratic Republic of the Congo. PLoS One. 2019;14(7):e0219990. doi:10.1371/journal.pone.0219990
3. Tran NT, Gaffield ME, Seuc A, et al. Effectiveness of a package of postpartum family planning interventions on the uptake of contraceptive methods until twelve months postpartum in Burkina Faso and the Democratic Republic of Congo: the YAM DAABO study protocol. BMC Health Serv Res. 2018;18(1):439. doi:10.1186/s12913-018-3199-2
4. Democratic Republic of the Congo | demographic Dividend. Available from: https://demographicdividend.org/democratic-republic-of-The-congo/.
5. Track20; 2022. Available from: https://track20.org/DR_Congo.
6. Kwete D, Binanga A, Mukaba T, et al. Family planning in the democratic republic of the Congo: encouraging momentum, formidable challenges. Glob Health Sci Pract. 2018;6(1):40–54. doi:10.9745/GHSP-D-17-00346
7. Mathe JK, Kasonia KK, Maliro AK. Barriers to adoption of family planning among women in eastern democratic Republic of Congo. Afr J Reprod Health. 2011;15(1). doi:10.4314/ajrh.v15i1.67859
8. Muanda MF, Ndongo GP, Messina LJ, Bertrand JT. Barriers to modern contraceptive use in rural areas in DRC. Cult Health Sex. 2017;19(9):1011–1023. doi:10.1080/13691058.2017.1286690
9. Mwaikambo L, Speizer IS, Schurmann A, Morgan G, Fikree F. What works in family planning interventions: a systematic review of the evidence. Stud Fam Plann. 2011;42(2):67–82.
10. Bapolisi WA, Bisimwa G, Merten S. Barriers to family planning use in the Eastern Democratic Republic of the Congo: an application of the theory of planned behaviour using a longitudinal survey. BMJ Open. 2023;13(2):e061564. doi:10.1136/bmjopen-2022-061564
11. MOMENTUM Safe Surgery in Family Planning and Obstetrics. EngenderHealt; 2024. Available from: https://www.engenderhealth.org/program/momentum-safe-surgery-in-family-planning-and-obstetrics.
12. The Democratic Republic of the Congo. USAID Momentum: A Global Partnership for Health and Resilience; 2023. Available from: https://usaidmomentum.org/where-we-work/drc/.
13. Community-based contraception distribution in the DRC. Abt Associates. Available from: https://www.abtassociates.com/who-we-are/news/feature-stories/community-based-contraception-distribution-in-The-drc.
14. Rogers D, Snyder LB, Rego M. The impact of mass media-delivered family planning campaigns in low- and middle-income countries: a meta-analysis of advertising and entertainment-education format effects. Stud Fam Plann. 2021;52(4):439–465. doi:10.1111/sifp.12175
15. Tilahun T, Coene G, Temmerman M, Degomme O. Couple based family planning education: changes in male involvement and contraceptive use among married couples in Jimma Zone, Ethiopia. BMC Public Health. 2015;15(1):682. doi:10.1186/s12889-015-2057-y
16. Osuafor GN, Akokuwebe ME, Idemudia ES. Male involvement in family planning decisions in Malawi and Tanzania: what are the determinants? Int J Environ Res Public Health. 2023;20(6):5053. doi:10.3390/ijerph20065053
17. Silverman JG, Boyce SC, Dehingia N, et al. Reproductive coercion in Uttar Pradesh, India: prevalence and associations with partner violence and reproductive health. SSM - Popul Health. 2019;9:100484. doi:10.1016/j.ssmph.2019.100484
18. Tounkara MS, Ingabire R, Comeau DL, et al. A mixed-methods study of factors influencing postpartum intrauterine device uptake after family planning counseling among women in Kigali, Rwanda. PLoS One. 2022;17(11):e0276193. doi:10.1371/journal.pone.0276193
19. Ibrahimi S, Steinberg JR. Spousal violence and contraceptive use among married afghan women in a nationally representative sample. Int J Environ Res Public Health. 2022;19(16):9783. doi:10.3390/ijerph19169783
20. Moulton JE, Corona MIV, Vaughan C, Bohren MA. Women’s perceptions and experiences of reproductive coercion and abuse: a qualitative evidence synthesis. PLoS One. 2021;16(12):e0261551. doi:10.1371/journal.pone.0261551
21. Limaye RJ, Sara AB Assessing the Effects of a Storytelling Initiative; 2017.
22. Snyder LB. Health communication campaigns and their impact on behavior. J Nutr Educ Behav. 2007;39(2 Supplement):S32–S40. doi:10.1016/j.jneb.2006.09.004
23. Pazol K, Zapata LB, Tregear SJ, Mautone-Smith N, Gavin LE. Impact of contraceptive education on contraceptive knowledge and decision making. Am J Prev Med. 2015;49(2 0 1):S46–S56. doi:10.1016/j.amepre.2015.03.031
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.