")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 15
Use of Intramuscular Ephedrine Sulfate During Kidney Transplantation
Authors Patel GP , Smith SA, Romej M, McAdoo B, Wilson EA
Received 8 May 2023
Accepted for publication 21 June 2023
Published 24 June 2023 Volume 2023:15 Pages 57—61
DOI https://doi.org/10.2147/CPAA.S418124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Gaurav P Patel, Susan A Smith, Michelle Romej, Billynda McAdoo, Elizabeth A Wilson
Department of Anesthesiology, Emory University School of Medicine, Atlanta, GA, 30322, USA
Correspondence: Gaurav P Patel, Department of Anesthesiology, Emory University School of Medicine, 1364 Clifton Road, NE, Atlanta, GA, 30322, USA, Tel +1 404-778-3900, Email [email protected]
Abstract: Hypotension during kidney transplantation can be common. Vasopressor use during these procedures is often avoided, with a fear of decreasing renal perfusion in the transplanted kidney. However, adequate perfusion for the rest of the body is also necessary, and given that these patients often have underlying hypertension or other comorbid conditions, an appropriate mean arterial pressure (MAP) has to be maintained. Intramuscular injections of ephedrine have been studied in the anesthesiology literature in a variety of case types, and it is seen as a safe and effective method to boost MAP. We present a case series of three patients who underwent renal transplantation and who received an intramuscular injection of ephedrine for hypotension control. The medication worked well for increasing blood pressures without apparent side effects. All three patients were followed for more than one year, and all patients had good graft function at the end of that time period. This series shows that while further research is necessary in this arena, intramuscular ephedrine may have a place in the management of persistent hypotension in the operating room during kidney transplantation.
Keywords: kidney transplant, hypotension, general anesthesia, intramuscular ephedrine, perfusion pressure
Introduction
During kidney transplantation, it is vital to optimize renal perfusion pressure to the allograft to facilitate recovery of renal function postoperatively. The use of vasopressor medications during kidney transplantation is controversial. There are some data suggesting that vasopressor use during the transplant surgery to maintain blood pressure may lead to delayed graft function (DGF), likely secondary to a paradoxical decrease in renal blood flow during transplant.1,2 DGF is associated with decreased patient survival, issues with long-term graft function, and possible acute rejection.3,4 Other studies have shown minimal long-term, post-operative effects with the use of intra- or postoperative vasopressor use.5 Given that perioperative fluid management in renal transplantation is difficult to manage,4 the anesthesiologist’s armamentarium to manage intraoperative hypotension is limited. There is a need to explore other options from a vasopressor standpoint to ensure that the anesthesiologist is able to maintain appropriate perfusion pressure to the whole body.
A single intramuscular (IM) ephedrine injection has been used in a variety of scenarios to mitigate hypotension successfully.6,7 While intravenous doses of ephedrine are often used, repeated use can lead to tachyphylaxis.7 IM ephedrine avoids this issue and can often lead to more predictable serum levels.6 Unfortunately, IM ephedrine use has not yet been validated in kidney transplantation. We present a series of 3 patients in which the intraoperative use of IM ephedrine successfully maintained goal mean arterial pressure (MAP) without adverse outcomes – up to at least one year post-transplantation. Of note, no prisoners were involved here as patients, and patients were neither coerced nor paid. This case series is in compliance with the Helsinki Congress and the Declaration of Istanbul. All patients included have given written consent for their case details to be included, and Institutional Review Board approval was waived given that this is a case series of 3 patients.
All donor organs for the case series below were from patients with confirmed brain death – consent for procurement was given by next-of-kin, and this informed consent was given voluntarily and under free will as is required by the United Network for Organ Sharing.
Cases
Case 1
A 53-year-old male with hemodialysis (HD) dependent end-stage renal disease (ESRD) due to long-standing hypertension and diabetes mellitus type 1 underwent a deceased donor renal transplant (DDRT). Baseline blood pressures for this patient ran 16-180/80-95 (MAP 107–123) for the last several months prior to surgery. He was maintained on amlodipine, metoprolol, and lisinopril for his blood pressure. The evening before transplantation, the patient received hemodialysis (HD) via a left arm arteriovenous (AV) fistula. After arrival to the operating room, the patient had an uncomplicated intravenous (IV) induction of general anesthesia with standard American Society of Anesthesiologists (ASA) monitors. An endotracheal tube was easily placed, and two large bore IV lines were obtained. Blood pressure was monitored every 5 minutes by a non-invasive blood pressure on the right arm. Anesthesia was maintained with sevoflurane, fentanyl, and rocuronium for paralysis. After incision, the patient became hypotensive with MAPs below 60, presumably secondary to volatile anesthetic induced vasodilation. The anesthesiologist subsequently performed to volume resuscitation with two liters of crystalloid without any improvement in his MAP. Small doses of phenylephrine (50–100 mcg) were utilized to temporarily maintain MAPs in the 80s. A 25 mg dose of IM ephedrine was then administered in the right deltoid. Within the next 30 minutes, hemodynamics appeared to improve and the blood pressure slowly trended upwards with sustained MAPs in the 80s for the remainder of the case. The patient’s heart rate increased mildly from a baseline in the mid-60s to the 70s. In the recovery room, the patient’s MAPs remained in 80–90s, within appropriate range of his baseline (Figure 1).
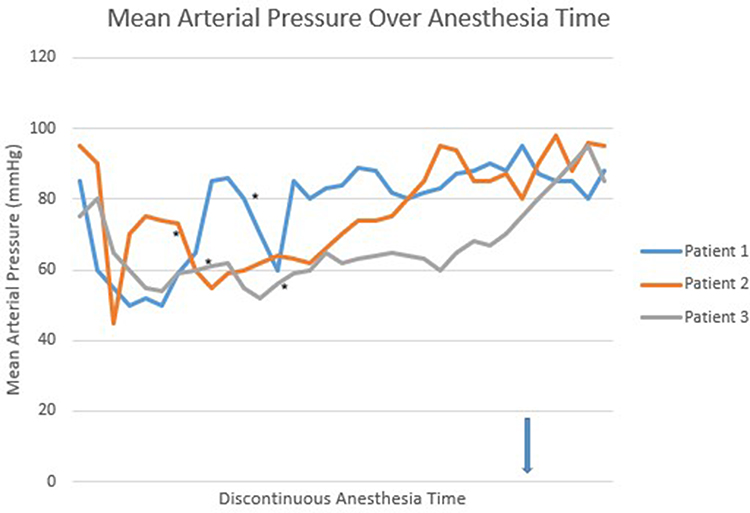 |
Figure 1 Mean arterial pressure presented over anesthesia time. Notes: This chart shows the change in mean arterial pressure (MAP) over anesthesia time. The * denotes doses of intramuscular (IM) ephedrine. Patient 3 had two separate doses of IM ephedrine. This image clearly shows the gradual increases in MAPs over time in these 3 patients after doses of IM ephedrine were administered. The arrow denotes the start of MAP readings in the recovery room. |
Follow-up of this patient’s chart demonstrates appropriate graft function and patient survival at over one year post-transplant.
Case 2
A 67-year-old female with ESRD secondary to diabetes type II underwent a DDRT. She received HD on the morning of her transplant via a dialysis catheter in the left internal jugular vein. Baseline blood pressures were MAPs 90s–100s on a home anti-hypertensive regimen of amlodipine 5mg daily. Baseline heart rate was in the 70s-80s. General endotracheal anesthesia via intravenous induction was performed. Standard ASA monitors were used. Upon induction, the patient’s blood pressure decreased to a MAP of 45, which improved with doses of IV phenylephrine (variable) and IV ephedrine (variable) with resultant MAPs of 75 and above. After incision and during the surgical procedure, the blood pressure gradually decreased again with MAPs in the 50s, unresponsive to volume resuscitation with two liters of lactated ringers and 500mL of Albumin 5%. An IM injection of 25mg ephedrine was subsequently administered in the left deltoid. Within 20 minutes, the blood pressure and heart rate steadily increased. For the remainder of the surgery, MAPs remained between 75 and 90, with heart rates in the mid-80s. In the recovery room, the patient maintained MAPs in the 90s (Figure 1).
Follow-up of this patient’s chart shows appropriate graft function and patient survival at one year.
Case 3
A 33-year-old male with ESRD secondary to polycystic kidney disease, maintained on peritoneal dialysis, underwent a DDRT at our institution. He had no other cardiopulmonary issues. Blood pressure during clinic visits was relatively normotensive, with MAP 75–90 in our system. He was not on any blood pressure medications. Baseline heart rates were 65–85. The patient was taken to the operating room, and anesthesia was induced. A balanced, general endotracheal anesthetic was maintained with sevoflurane, fentanyl and rocuronium. Blood pressure gradually decreased over time to a MAP of 50, and fluid resuscitation with 2 liters crystalloid solution and 500mL of albumin 5% did not appreciably increase the MAPs. An IM dose of 25 mg ephedrine was administered in the right deltoid muscle. Blood pressure slowly increased to a MAP of 55 but did not increase further than this. An additional 25mg of IM ephedrine was administered. MAPs increased into the 60s over the next 30 minutes. Heart rate did increase into the 90s. In the recovery room, the patient’s MAP remained in the 85–95 range (Figure 1). Heart rate did remain elevated in the 90s–100s.
Follow-up of the patient’s chart showed appropriate graft function after one year.
Discussion
Hypotension during kidney transplantation can be common due to intravascular volume depletion and peripheral vasodilation from general anesthesia. Benken et al found that close to 40% of their patients receiving a kidney transplant required continuous vasopressor infusions intraoperatively.1 Maintaining appropriate perfusion pressures by maintaining MAP is essential, as allograft perfusion is vitally important to graft function.1 In the non-anesthetized, non-transplanted patient, low MAP can be negated by renal autoregulation to minimize renal injury. However, in the anesthetized patient and a patient with a denervated, transplanted kidney, compensatory autoregulation can be deranged. Of note, the afferent arterioles in the transplanted kidney have an increased responsiveness to vasopressor agents and reduced vasodilation from nitric oxide.8 The clinical significance of these changes in the transplanted kidney is not well understood. Some studies show that the alpha-adrenergic activity of catecholamine vasopressors and other vasopressors such as phenylephrine may not affect long-term outcomes. Kristopher et al showed that while the use of intraoperative phenylephrine in these patients may lead to a slower postoperative normalization of the creatinine than those who did not receive phenylephrine, creatinine at discharge showed no difference.5 Hence, there may be a brief “shock” to the transplanted kidney, but this likely has no long-term consequence for graft survival. Other studies also mimic this noted effect.9 The intraoperative use of dopamine has also been studied for potential renal protective effects but remains controversial.4,10,11
The anesthesiologist is charged with maintaining appropriate renal perfusion but also appropriate perfusion of the rest of the body during the surgical procedure. Managing appropriate hemodynamics can be difficult in transplantation procedures and hypotension, even temporarily, has demonstrated detrimental long-term outcomes, from both cardiopulmonary and neurologic standpoints.12–14 As such, appropriate vasopressor therapy along with adequate fluid management is essential in these patients.
IM ephedrine has been studied, particularly in neuraxial anesthetics, for the mitigation of hypotension. Ephedrine acts as a non-specific sympathomimetic, causing an increase in heart rate, cardiac output, and systemic vascular resistance.6 Its mechanism includes both direct and indirect effects.6,7,15 Classically, ephedrine is given as intermittent, bolus doses intravenously in response to low blood pressure. Park et al note that this can lead to waxing and waning serum drug levels, leading to unpredictable results.6 Ephedrine cannot be used as an intravenous infusion. Several studies have shown, nevertheless, that a single IM dose of ephedrine can likely lead to a more stable, steady state concentration of drug than bolus dosing.6,7,16 Other studies have shown that an IM dose of ephedrine may cause less perturbation of vascular resistance,7 and specifically for ephedrine, the pharmacokinetics of IM injection allow for a relatively reliable onset and offset.6 Furthermore, hypertension and tachycardia, often thought of as side effects of ephedrine administration, have not been commonly seen.6,17,18 The efficacy and safety of IM ephedrine based on multiple studies appear to have been recognized.6,7,15–18
There are several limitations of this case series. This report describes only three patients, and follow-up was only for a little over a year. A randomized, controlled trial would be ideal to assess the acute and long-term effects of IM ephedrine. Furthermore, the appropriate dosing of IM ephedrine would need to be elucidated, as doses varied above. The effect of IM ephedrine on renal vasculature as compared to other studied vasopressor infusions also remains unknown. The decreased effects on vascular resistance by ephedrine noted above were described in a global fashion and did not specifically address a denervated kidney or renal vascular tone in general. While the grafts did well in our cases, further studies and more long-term evaluation of graft survival in comparison to graft survival with other vasopressor use may be another possible avenue to explore.
Even given these limitations, IM ephedrine may be a potential addition to the anesthesiologist’s vasopressor arsenal for kidney transplantation. Maintaining appropriate perfusion to all end organs, including the new kidney, is essential during intraoperative management. We believe that these cases certainly open the door for further study in this area.
Disclosure
The authors report no conflicts of interest. This article did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
1. Benken J, Lichvar A, Benedetti E, et al. Perioperative vasopressors are associated with delayed graft function in kidney transplant recipients in a primarily Black and Hispanic cohort. Prog Transplant. 2022:15269248221087433. PMID: 35477338. doi:10.1177/15269248221087433
2. Aulakh NK, Garg K, Bose A, Aulakh BS, Chahal HS, Aulakh GS. Influence of hemodynamics and intra-operative hydration on biochemical outcome of renal transplant recipients. J Anaesthesiol Clin Pharmacol. 2015;31(2):174–179. PMID: 25948896; PMCID: PMC4411829. doi:10.4103/0970-9185.155144
3. Yarlagadda SG, Coca SG, Formica RN Jr, Poggio ED, Parikh CR. Association between delayed graft function and allograft and patient survival: a systematic review and meta-analysis. Nephrol Dial Transplant. 2009;24(3):1039–1047. PMID: 19103734. doi:10.1093/ndt/gfn667
4. Calixto Fernandes MH, Schricker T, Magder S, Hatzakorzian R. Perioperative fluid management in kidney transplantation: a black box. Crit Care. 2018;22(1):14. PMID: 29368625; PMCID: PMC5784708. doi:10.1186/s13054-017-1928-2
5. Day KM, Beckman RM, Machan JT, Morrissey PE. Efficacy and safety of phenylephrine in the management of low systolic blood pressure after renal transplantation. J Am Coll Surg. 2014;218(6):1207–1213. PMID: 24768292. doi:10.1016/j.jamcollsurg.2014.01.058
6. Park JH, Shim JK, Hong H, Lim HK. The efficacy of intramuscular ephedrine in preventing hemodynamic perturbations in patients with spinal anesthesia and dexmedetomidine sedation. Int J Med Sci. 2020;17(15):2285–2291. PMID: 32922193; PMCID: PMC7484642. doi:10.7150/ijms.48772
7. Sternlo JE, Rettrup A, Sandin R. Prophylactic i.m. ephedrine in bupivacaine spinal anaesthesia. Br J Anaesth. 1995;74(5):517–520. PMID: 7772424. doi:10.1093/bja/74.5.517
8. Morita K, Seki T, Nonomura K, Koyanagi T, Yoshioka M, Saito H. Changes in renal blood flow in response to sympathomimetics in the rat transplanted and denervated kidney. Int J Urol. 1999;6(1):24–32. PMID: 10221861. doi:10.1046/j.1442-2042.1999.06117.x
9. Pahari H, Rizzari M, Safwan M, et al. Effect of donor vasopressor requirements on recipient outcomes for intestinal and multi-visceral grafts - is it overrated? Transplantation. 2017;101(6S2):S17. doi:10.1097/01.tp.0000521299.96555.8b
10. Gingell-Littlejohn M, Koh H, Aitken E, et al. Below-target postoperative arterial blood pressure but not central venous pressure is associated with delayed graft function. Transplant Proc. 2013;45(1):46–50. PMID: 23267785. doi:10.1016/j.transproceed.2012.03.058
11. Othman MM, Ismael AZ, Hammouda GE. The impact of timing of maximal crystalloid hydration on early graft function during kidney transplantation. Anesth Analg. 2010;110(5):1440–1446. PMID: 20418304. doi:10.1213/ANE.0b013e3181d82ca8
12. Running K, Weinberg D, Trudo W, Sullivan CL, Patel GP. Intraoperative use of angiotensin II for severe vasodilatory shock during liver transplantation: a case report. A a Pract. 2021;15(2):e01402. PMID: 33577171. doi:10.1213/XAA.0000000000001402
13. Weinberg D, Running K, Kalarickal PL, Patel GP. Use of intravenous hydroxocobalamin for vasoplegic syndrome in simultaneous liver-kidney transplant: a case report. Transplant Proc. 2021;53(4):1300–1302. PMID: 33246585. doi:10.1016/j.transproceed.2020.09.019
14. Nycz BT, Chalhoub A, Patel GP, Dean CE, Papangelou A. Hemispheric asymmetry on the electroencephalogram during general anesthesia responsive to blood pressure manipulations. Neurol Int. 2022;14(4):1018–1023. PMID: 36548186; PMCID: PMC9782369. doi:10.3390/neurolint14040081
15. Goertz AW, Hübner C, Seefelder C, et al. The effect of ephedrine bolus administration on left ventricular loading and systolic performance during high thoracic epidural anesthesia combined with general anesthesia. Anesth Analg. 1994;78(1):101–105. PMID: 8267145. doi:10.1213/00000539-199401000-00018
16. Jin JF, Zhu LL, Chen M, et al. The optimal choice of medication administration route regarding intravenous, intramuscular, and subcutaneous injection. Patient Prefer Adherence. 2015;9:923–942. PMID: 26170642; PMCID: PMC4494621. doi:10.2147/PPA.S87271
17. Hemmingsen C, Poulsen JA, Risbo A. Prophylactic ephedrine during spinal anaesthesia: double-blind study in patients in ASA groups I-III. Br J Anaesth. 1989;63(3):340–342. PMID: 2803892. doi:10.1093/bja/63.3.340
18. Ayorinde BT, Buczkowski P, Brown J, Shah J, Buggy DJ. Evaluation of pre-emptive intramuscular phenylephrine and ephedrine for reduction of spinal anaesthesia-induced hypotension during Caesarean section. Br J Anaesth. 2001;86(3):372–376. PMID: 11573527. doi:10.1093/bja/86.3.372
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.