")
Back to Journals » Pragmatic and Observational Research » Volume 13
Variation in Demographic and Clinical Characteristics of Patients with COPD Receiving Care in US Primary Care: Data from the Advancing the Patient EXperience (APEX) in COPD Registry
Authors Fox C, Pace W , Brandt E, Carter V, Chang KL, Edwards C, Evans A, Gaona G, Han MK, Kaplan A , Kent R, Kocks JWH , Kruszyk M, Le Lievre Chantal , LiVoti TM, Mahle C, Make B , Ratigan A, Shaikh A , Skolnik N, Stanley B , Yawn BP, Price DB
Received 5 October 2021
Accepted for publication 15 April 2022
Published 29 April 2022 Volume 2022:13 Pages 17—31
DOI https://doi.org/10.2147/POR.S342736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Christoph R Meier
Chester Fox,1,2 Wilson Pace,1,3 Elias Brandt,1 Victoria Carter,4,5 Ku-Lang Chang,6 Chelsea Edwards,7 Alexander Evans,4 Gabriela Gaona,1 MeiLan K Han,8 Alan Kaplan,5,9,10 Rachel Kent,1 Janwillem WH Kocks,5,11– 13 Maja Kruszyk,5,7 Le Lievre Chantal,5,7 Tessa LiVoti,4,5 Cathy Mahle,14 Barry Make,15 Amanda Ratigan,1 Asif Shaikh,14 Neil Skolnik,16,17 Brooklyn Stanley,4 Barbara P Yawn,17 David B Price4,5,18
1DARTNet Institute, Aurora, CO, USA; 2University at Buffalo, Buffalo, NY, USA; 3University of Colorado, Denver, CO, USA; 4Optimum Patient Care, Cambridge, UK; 5Observational and Pragmatic Research Institute, Singapore; 6University of Florida College of Medicine, Gainesville, FL, USA; 7Optimum Patient Care, Brisbane, Queensland, Australia; 8University of Michigan, Ann Arbor, MI, USA; 9Family Physician Airways Group of Canada, Stouffville, Ontario, Canada; 10University of Toronto, Toronto, Canada; 11General Practitioners Research Institute, Groningen, the Netherlands; 12Groningen Research Institute Asthma and COPD (GRIAC), University of Groningen, University Medical Center Groningen, Groningen, the Netherlands; 13Department of Pulmonology, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands; 14Boehringer Ingelheim, Ridgefield, CT, USA; 15Department of Medicine, NJH, Denver, CO, USA; 16Abington Jefferson Health, Jenkintown, PA, USA; 17University of Minnesota, Minneapolis, MN, USA; 18Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Aberdeen, UK
Correspondence: David B Price, Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Polwarth Building, Foresterhill, Aberdeen, AB25 2ZD, UK, Tel +65 3105 1489, Email [email protected]
Introduction: Little is known about the variability in chronic obstructive pulmonary disease (COPD) management and how it may be affected by patient characteristics across different healthcare systems in the US. This study aims to describe demographic and clinical characteristics of people with COPD and compare management across five primary care medical groups in the US.
Methods: This is a retrospective observational registry study utilizing electronic health records stored in the Advancing the Patient Experience (APEX) COPD registry. The APEX registry contains data from five US healthcare organizations located in Texas, Ohio, Colorado, New York, and North Carolina. Data on demographic and clinical characteristics of primary care patients with COPD between December 2019 and January 2020 were extracted and compared.
Results: A total of 17,192 patients with COPD were included in analysis: Texas (n = 811), Ohio (n = 8722), Colorado (n = 472), New York (n = 1149) and North Carolina (n = 6038). The majority of patients at each location were female (> 54%) and overweight/obese (> 60%). Inter-location variabilities were noted in terms of age, race/ethnicity, exacerbation frequency, treatment pattern, and prevalence of comorbid conditions. Patients from the Colorado site experienced the lowest number of exacerbations per year while those from the New York site reported the highest number. Hypertension was the most common co-morbidity at 4 of 5 sites with the highest prevalence in New York. Depression was the most common co-morbidity in Ohio. Treatment patterns also varied by site; Colorado had the highest proportion of patients not on any treatment. ICS/LABA was the most commonly prescribed treatment except in Ohio, where ICS/LABA/LAMA was most common.
Conclusions and Relevance: Our data show heterogeneity in demographic, clinical, and treatment characteristics of patients diagnosed with COPD who are managed in primary care across different healthcare organizations in the US.
Keywords: quality of care, observational study, research database, patient-reported outcomes
Plain Language Summary
Why was the study done?
A clearer picture is needed on the variation in patient characteristics across the US as they may affect the quality of management of patients with chronic obstructive pulmonary disease (COPD). We conducted this study to describe and compare the demographic and clinical characteristics of patients with COPD across five primary care healthcare groups in the US.
What did the researchers do and find?
Electronic health record data from the APEX (Advancing the Patient Experience) COPD registry were extracted and variations in patient characteristics across five healthcare organizations located in Texas, Ohio, Colorado, New York, and North Carolina were compared.
We observed variances in the age and race/ethnicity distribution of COPD patients across different healthcare organizations in the US Variances in clinical characteristics such as prescription of treatment, presence of co-morbid diseases, and frequency of COPD exacerbations were also observed.
What do these results mean?
Factors that contribute to clinical care disparities need to be identified and understood to develop approaches to help standardize and improve COPD clinical care across US healthcare.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by a progressive respiratory airflow obstruction that affects normal breathing and is not fully reversible.1 It remains one of the leading causes of death both globally1,2 and within the US,3,4 and imposes significant clinical morbidity and lifestyle and socioeconomic burden on those affected by the condition.5–7
Despite its high prevalence and disease burden, COPD is still underdiagnosed, especially within the primary care setting.8,9 This may be in part due to the lack of availability and underutilization of spirometry which is required to formally diagnose COPD.1,8,10,11 Due to the slow progression of COPD, its early symptoms are often unrecognized by both patients and clinicians, despite substantial deterioration in health status.12 Consequently, COPD is often only first diagnosed when the disease is at an advanced stage.13 Early treatment is important for potentially slowing disease progression14 and for reducing disease burden.15 The majority of COPD patients in the US are managed in primary care settings.16 As such, primary care clinicians play a key role in COPD treatment and management.
Guidelines for the treatment and management of COPD for patients in the US have been provided by bodies such as the COPD Foundation,17,18 the American College of Physicians,19 the American College of Chest Physicians,19,20 the American Thoracic Society,19 and the US Department of Veteran Affairs.21 In addition to this, the Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Diseases (GOLD)1 provides key recommendations for diagnosis and care. These recommendations outline best practices, most of which are regularly updated in accordance with current research. However, awareness and adherence to these guidelines in primary care remain suboptimal.11
Treatment and disease management can be influenced by patient demographics and clinical characteristics, stemming from both patients and clinicians, which may vary widely between states, cities, and neighborhoods. This may be amplified due to healthcare quality disparity between different healthcare systems.22,23 A clearer picture of this variation is important for identifying underlying factors impacting care in different communities. A better understanding of the variability across healthcare organizations may improve the ability to assess variations of care across the US due to disease heterogeneity versus system related variations. Such information may help to suggest where care could be standardized and where it may need to be varied to meet patient specific disease requirements. However, to date, the variation of US primary care-based patient demographics and clinical care of people with COPD is not well described.
The APEX (Advancing the Patient Experience) in COPD patient registry (https://www.apexcopd.org/) was established as the first primary-care health system-based registry in the US to collect both retrospective and prospective electronic health record (EHR) data supplemented with patient-reported information/outcomes (PRIO) data from patients with COPD.24 This study aims to investigate the variation in demographic and clinical characteristics of patients diagnosed with COPD across different primary care healthcare organizations in the US using the APEX COPD registry.
Methods
Design
This is a retrospective, observational registry study utilizing electronic health records from the APEX COPD Registry. The APEX COPD Registry consists of longitudinal primary care data from 5 healthcare organizations located in Texas, Ohio, Colorado, New York, and North Carolina, encompassing a total of 31 primary care clinics. Data stored in the APEX COPD Registry range from August 2001 to September 2020.
Patient Population
Patients were included if they had diagnostic codes for COPD (including chronic bronchitis, emphysema, α1-antitrypsin deficiency [AATD], and mixed COPD/asthma) and were aged ≥35 years at the time of COPD diagnosis (Supplementary Table 1). As spirometry is poorly recorded in many primary care EHR records, no COPD-confirming result ie FEV1/FVC ratio of >70%, was required. Additionally, patients were included if they had active/current COPD as of September 2020, defined as having an appointment in the last two years and either: 1) had a COPD code in the last year or 2) had a prescription for a COPD inhaler in the last two years together with a COPD diagnosis, or 3) had active patient-reported symptoms of COPD. Active symptoms included the reporting of an exacerbation within the previous year, with an exacerbation as defined in the study variables section. Patients were excluded if they were: 1) participating in a clinical trial for COPD drugs at the time of enrolment, 2) had an active cancer diagnosis in the last 3 years (excluding non-melanoma skin cancers), and/or 3) were receiving hospice care. All available data from eligible patients were extracted for this study.
Study Variables
Demographic, clinical, and PRIO variables collected in the APEX COPD Registry were developed by a panel of international experts via a modified Delphi consensus process. Briefly, a panel of experts voted from a list of variables to be included. At the end of each round of voting, the remaining variables were summarized and presented to the panel for another round of voting, until the end of the third round.
The variables summarized in the current study include data on patient demographics (age, sex, race/ethnicity, BMI), smoking status/history, COPD exacerbations, co-morbidities, and treatment. The full list and description of variables are available in Supplementary Table 2. Additional PRIO variables collected include information on the quality of life (COPD Assessment Test [CAT]), breathlessness (Modified Medical Research Council Dyspnea Scale [mMRC]), COPD exacerbations and hospitalizations, and smoking status/history. Patient GOLD groups were calculated using mMRC, CAT, and exacerbation history. The full list and description of PRIO variables collected are also available in Supplementary Table 3.
EHR-recorded and patient-reported COPD exacerbations are defined separately. EHR-recorded COPD exacerbations were defined according to a hierarchical algorithm as the occurrence of the following events:25
- Recorded COPD exacerbation codes (Supplementary Table 4).
- COPD, acute bronchitis, LRTI, other lower respiratory code or influenza code with prescribed oral corticosteroid (OCS) and/or respiratory specific antibiotic.
- Uncoded exacerbation with prescribed OCS and/or respiratory specific antibiotic (without other reason).
Patient-reported COPD exacerbations are received from patient questionnaires.
Data Collection
Aggregated baseline demographic and clinical EHR data were collected from June 2019 to September 2020. Longitudinal patient data extended to earlier years at each site: January 2002 (Texas), January 2010 (Ohio), March 2007 (Ohio), August 2001 (New York), and July 2009 (N. Carolina). EHR data were extracted remotely by the DARTNet Institute, a non-profit organization that hosts data sets of health information for quality improvement and research (http://www.dartnet.info/).
EHR data was standardized using the Observational Medical Outcomes Partnership (OMOP) common data model (v6), allowing for the analysis of data from disparate sources. To ensure anonymity, all patients were assigned a unique Registry ID using a one-way hashing algorithm prior to storage in the database.
PRIO data were collected by paper questionnaires or PEERS (a HIPAA compliant, browser-based study management, and PRIO data collection system) between Dec 2019 and November 2020. These data were integrated into the OMOP DARTNet database and reconciled with respective patient EHR data. Paired PRIO data were stored as a single data set per patient and assigned a unique registry ID using a one-way hashing algorithm.
EHR and PRIO data quality were enhanced through a series of programmed data quality checks that automatically detect out-of-range or anomalous data. The APEX COPD databases are hosted in the US on an Amazon Web Service (AWS) firewall-firewall-protected server. This server is part of the HIPAA 1996 compliant DARTNet server environment maintained by AWS. OPC Global acts as data custodians, but each site/patient continues to own the patient-level data contributed.
Statistical Analysis
Stata version 14 (College Station, TX, US) and R version 3.6 (Vienna, Austria) were used to conduct all statistical analyses and data handling. Descriptive statistics were computed for all demographic, clinical, and PRIO variables. All available (non-missing) data were summarized. Categorical variables were presented as number (%) and numerical variables as mean (standard deviation).
Results
Patient Population
A total of 17,192 patients were identified to be eligible for analysis from the APEX COPD Registry from healthcare organizations located in Texas (n=811), Ohio (n=8722), Colorado (n=472), New York (n=1149), and North Carolina (n=6038). Supplementary PRIO data was available from 63, 565, 62, 79, and 585 patients respectively from Texas, Ohio, Colorado, New York, and North Carolina.
Baseline Characteristics
Sex distribution was similar at each site with a slight female majority (>54%) (Table 1). The 65–74 years age-group had the highest proportion of patients in Texas (36.3%), Colorado (28.4%), and North Carolina (34.2%). Meanwhile, in Ohio and New York, the age-group with the highest proportion of patients was the 55–64 years group (35.7% and 38.6% respectively). BMI distribution was also similar across sites with 62–73% of patients being overweight or obese (BMI ≥25). Colorado had the lowest proportion of overweight to obese patients and the lowest mean BMI (mean (SD) = 27.9 [7.2]). Racial and ethnicity distribution was highly variable. Patients from Colorado (94.8%) and North Carolina (83.7%) were predominantly Caucasian. Ohio also had a majority (58.9%) Caucasian patients but also a sizable proportion of African American patients (31.9%). Texas had 45.9% Hispanic patients while New York consisted of mostly African American patients. The majority (83.7–100.0%) of patients were current or ex-smokers, except in Texas where 54.0% had never smoked. EHR recorded prescription of pharmacological intervention for smoking cessation was rare, with approximately half the number of current smokers across all sites having received intervention, the lowest being in in New York (7.7%) which has the highest proportion of current smokers (71.5%). The distribution of baseline characteristics for patients who provided supplementary PRIO data is presented in Supplementary Table 5.
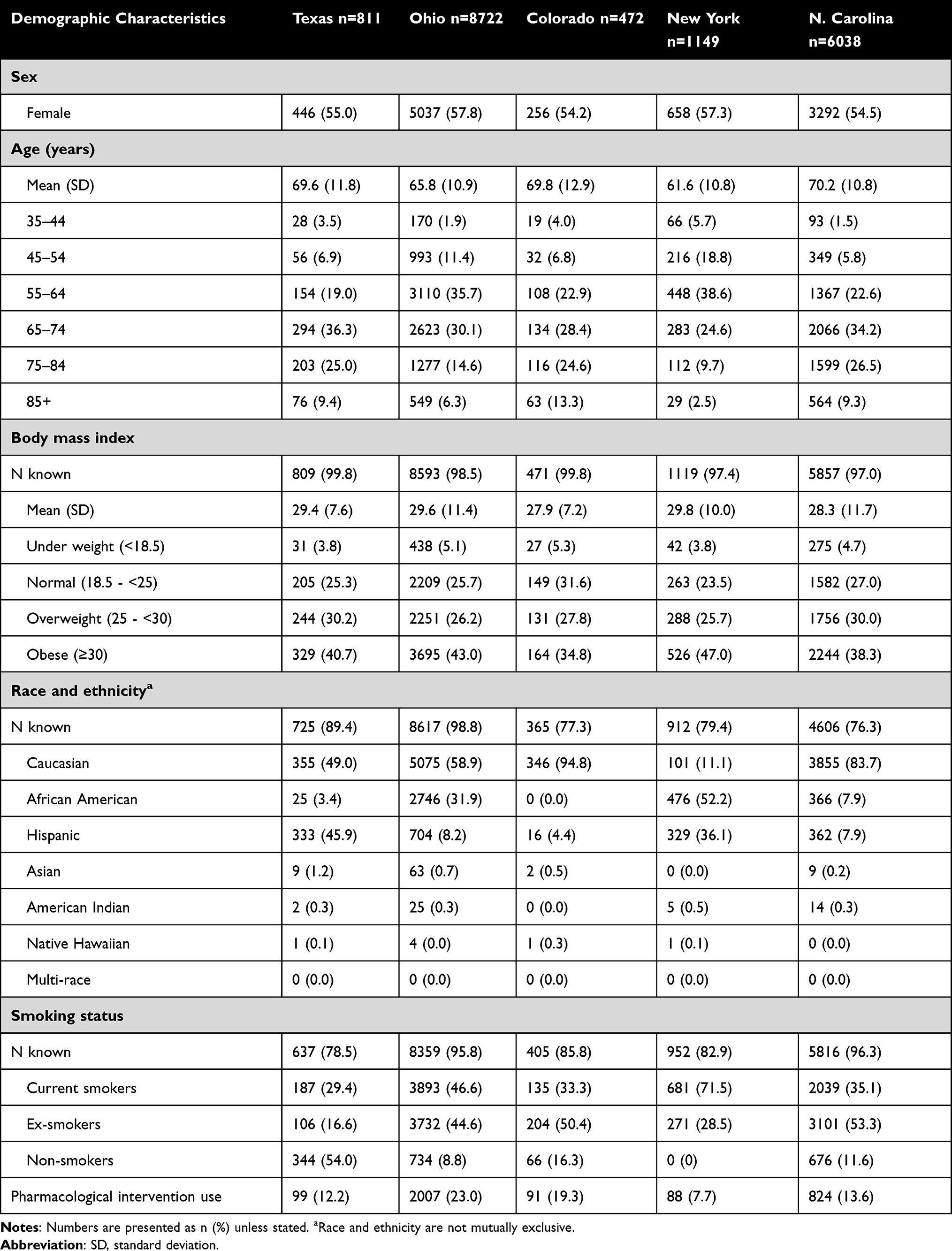 |
Table 1 Demographic Characteristics of COPD Patients in the APEX COPD Registry |
Clinical Characteristics
Overall, 34.7% to 42.2% of patients experienced an exacerbation in the previous year (Table 2). Colorado had the fewest number of exacerbations with the highest proportion of no exacerbation (65.3%) and the smallest proportion of 3+ exacerbations (1.5%). Patients from Colorado also experienced the lowest average number of exacerbations (mean [SD] = 0.5 [0.7]) while New York and Ohio experienced the highest (mean [SD] = 0.9 [1.6] and 0.9 [1.5] respectively).
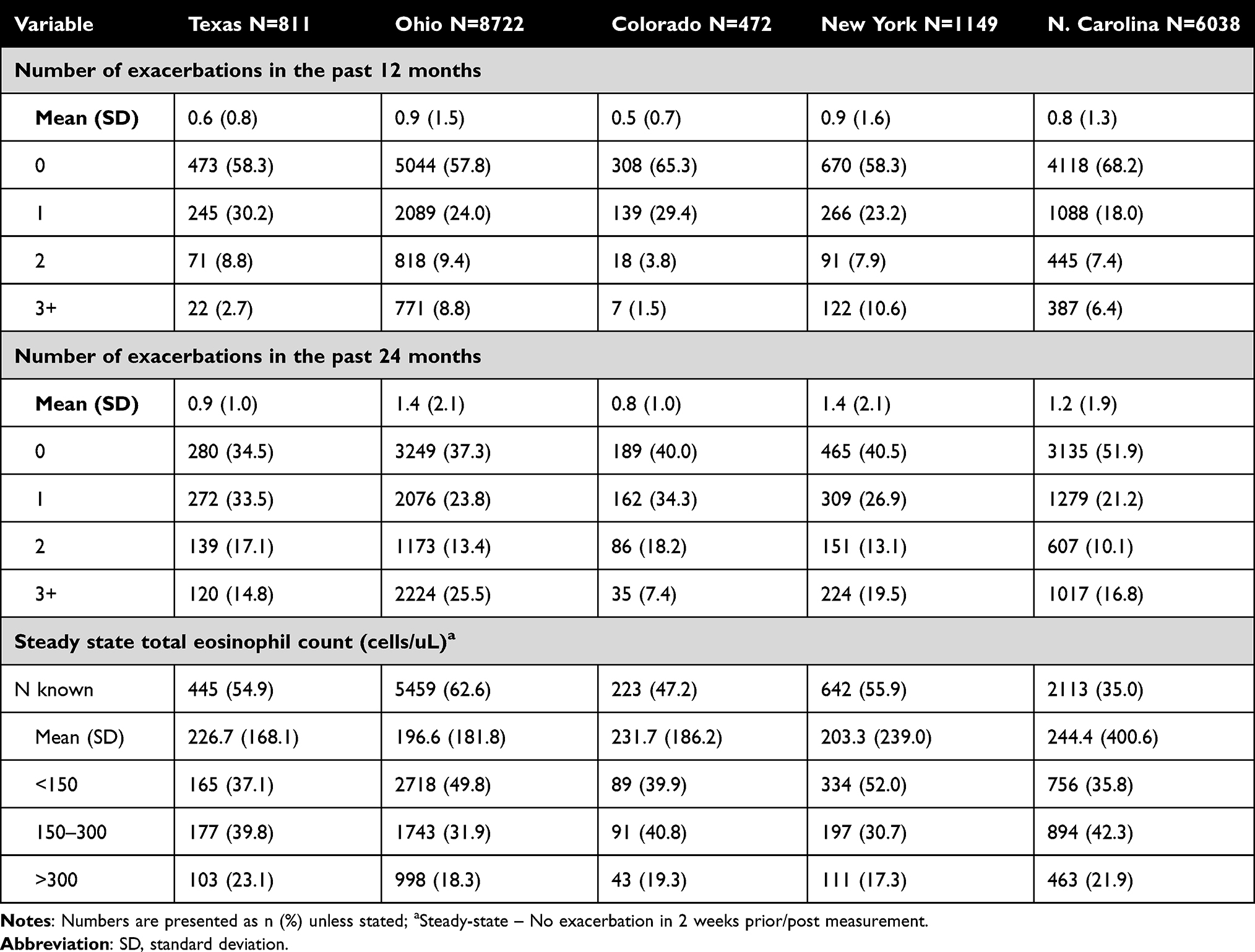 |
Table 2 Disease Monitoring Characteristics of COPD Patient from the APEX COPD Registry |
Steady-state (no exacerbation in the 2 weeks pre- and post-measurement) total eosinophil count varied across the sites. Patients from Ohio had the lowest mean steady-state total eosinophil count (mean [SD] = 196.6 [181.8]) while North Carolina had a much higher total eosinophil count (mean [SD] = 244.4 [400.6]). (Table 2). The proportion of patients with >300 cells/µL total eosinophil count, the cut-off for the greatest benefit for ICS treatment, was highest in Texas (23.1%) followed by North Carolina (21.9%). Results for exacerbations and total eosinophil count in patients who provided supplementary PRIO data are presented in Supplementary Table 6.
Co-Morbidities
Co-morbidities were common across all sites (Table 3). Hypertension was the most common co-morbidity at all sites (75.0–87.9%), except in Colorado where depression was more common (86.9%). A much higher rate of asthma (61.6%) and heart failure (72.3%) were observed in New York compared to the other sites (<41% and <26% respectively). In contrast, obstructive sleep apnea was much less common in New York (7.8%) than in other sites (>27%). Pneumonia in the last 24 months was observed in 11.6–16.9% of patients within Texas, Ohio, and Colorado. Almost none (1.5%) in North Carolina and none in New York had recorded pneumonia. The prevalence of co-morbidities in patients who provided supplementary PRIO data is presented in Supplementary Table 7.
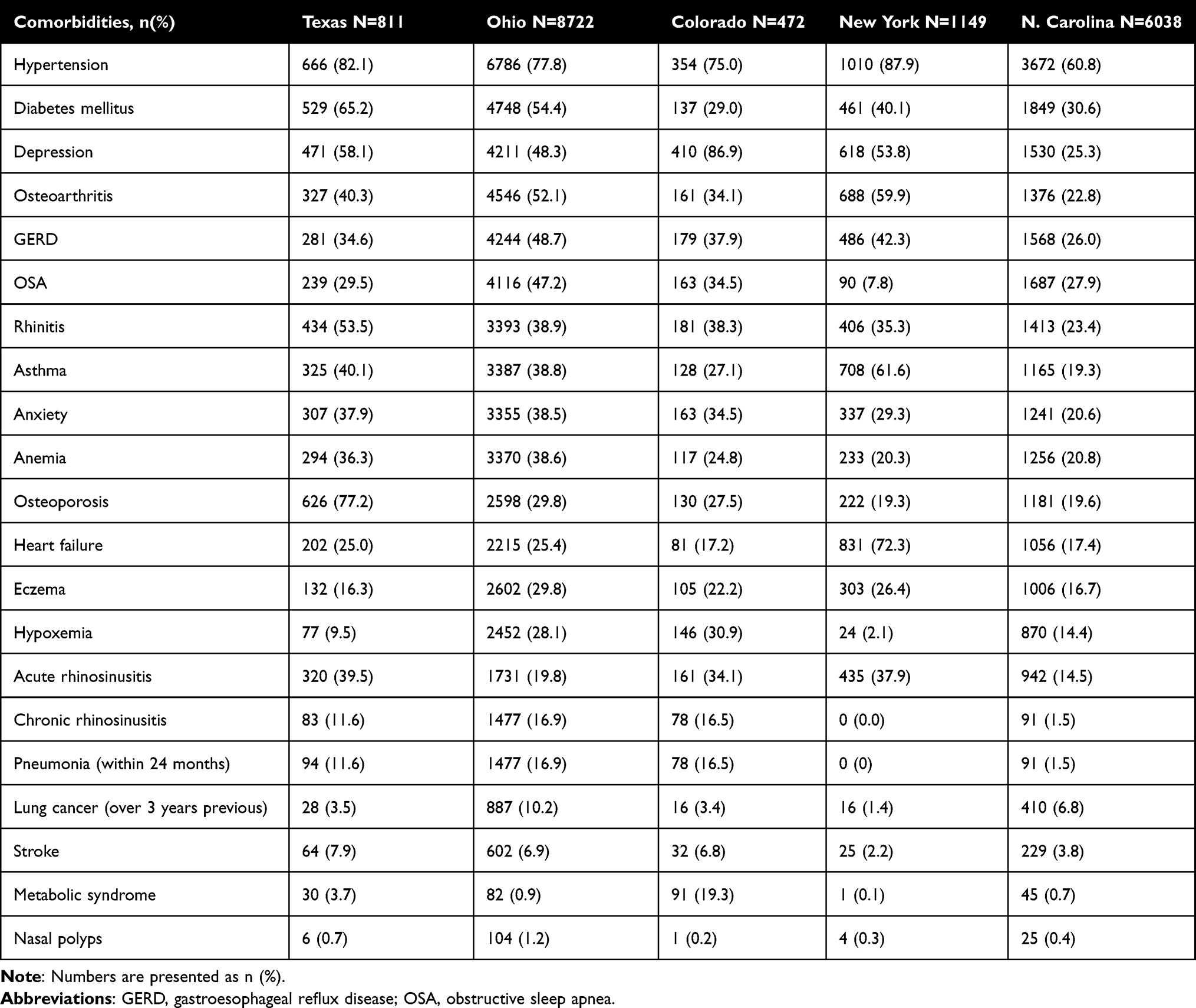 |
Table 3 Differential Diagnosis and Comorbidities of COPD Patients from the APEX COPD Registry |
Treatment
Only a small proportion of patients (<9%) were not on any therapy for COPD except in Colorado (28.4%) (Table 4). A minority (4.9–14.9%) were given only short-acting bronchodilator therapy across all 5 sites. Among controller therapies given, with or without short-acting bronchodilator inhalers, inhaled corticosteroid (ICS) with long-acting beta-agonist (LABA) was the most common treatment combination (26.1–45.6%), except in Ohio where triple therapy with ICS, LABA, and Long-acting muscarinic antagonist (LAMA) was more common (32.9%). Triple therapy was given in roughly 1 in 5 patients at other sites except in Colorado with only 4.7% of patients receiving triple therapy. Prescribing of ICS monotherapy was most common in Colorado (12.9%) but was much less common at other sites (1.4–5.7%). Vaccination rates were similar across all sites with 19.3–34.7% and 56.8–78.0% of patients having received influenza vaccine within the past 12 months and pneumococcal vaccines within the past 10 years respectively. Vaccination data were not available from the New York site. Treatment and vaccination data for patients who provided supplementary PRIO data are presented in Supplementary Table 8.
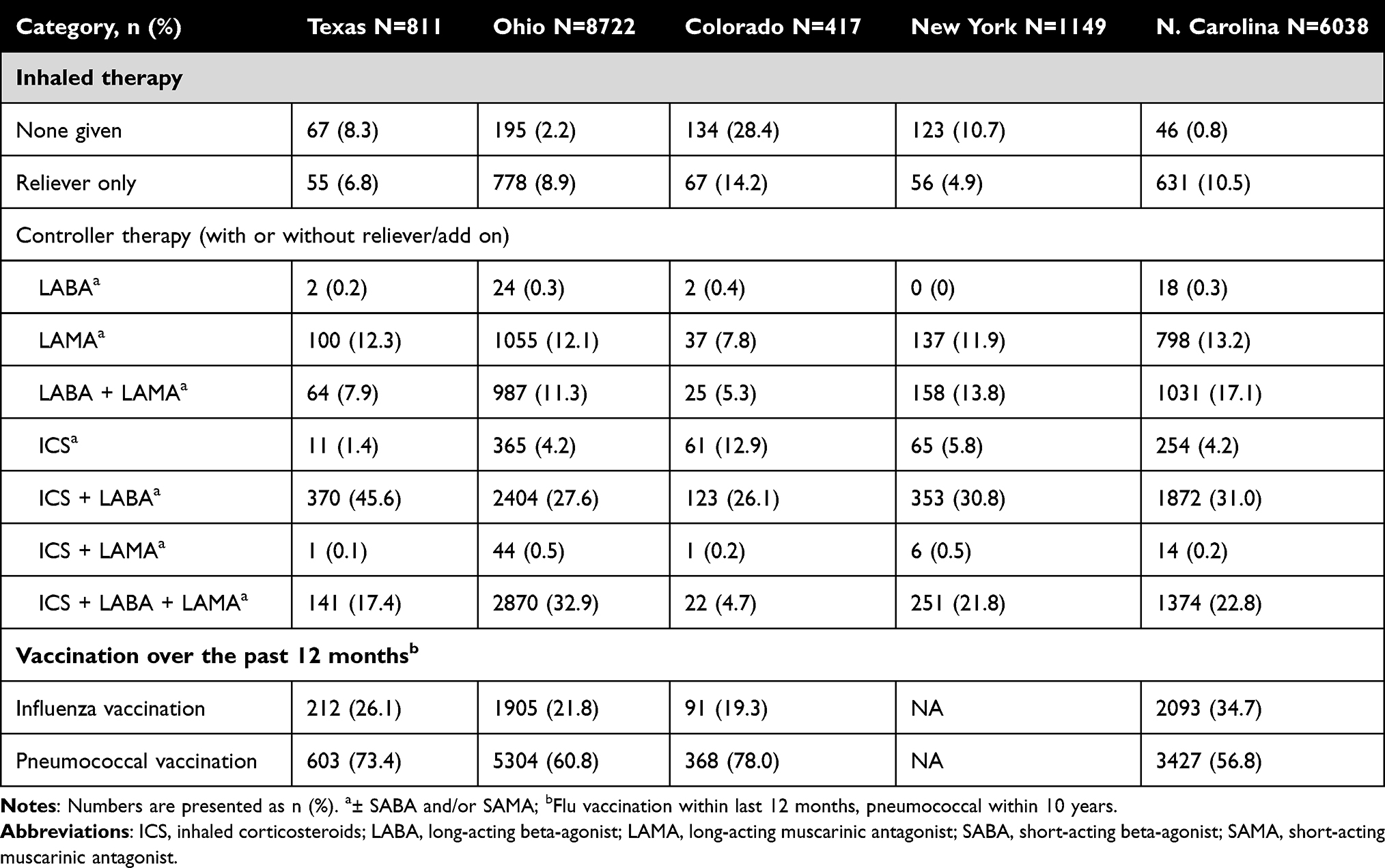 |
Table 4 Treatment Patterns of COPD Patients in the Last 24 Months from the APEX COPD Registry |
Patient-Reported Information/Outcomes (PRIO)
Among the 1354 patients who provided additional PRIO data, the majority (68–74%) reported a CAT score of 10–30. (Table 5). Texas had the highest proportion of patients who reported Grade 0 or 1 mMRC-rated breathlessness (66.2%) and patients who were categorized as GOLD group A (21.0%). New York reported the highest proportion of mMRC at >2 (54.6%); however, Colorado reported the highest proportion of patients at the highest level 4 (11.9%).
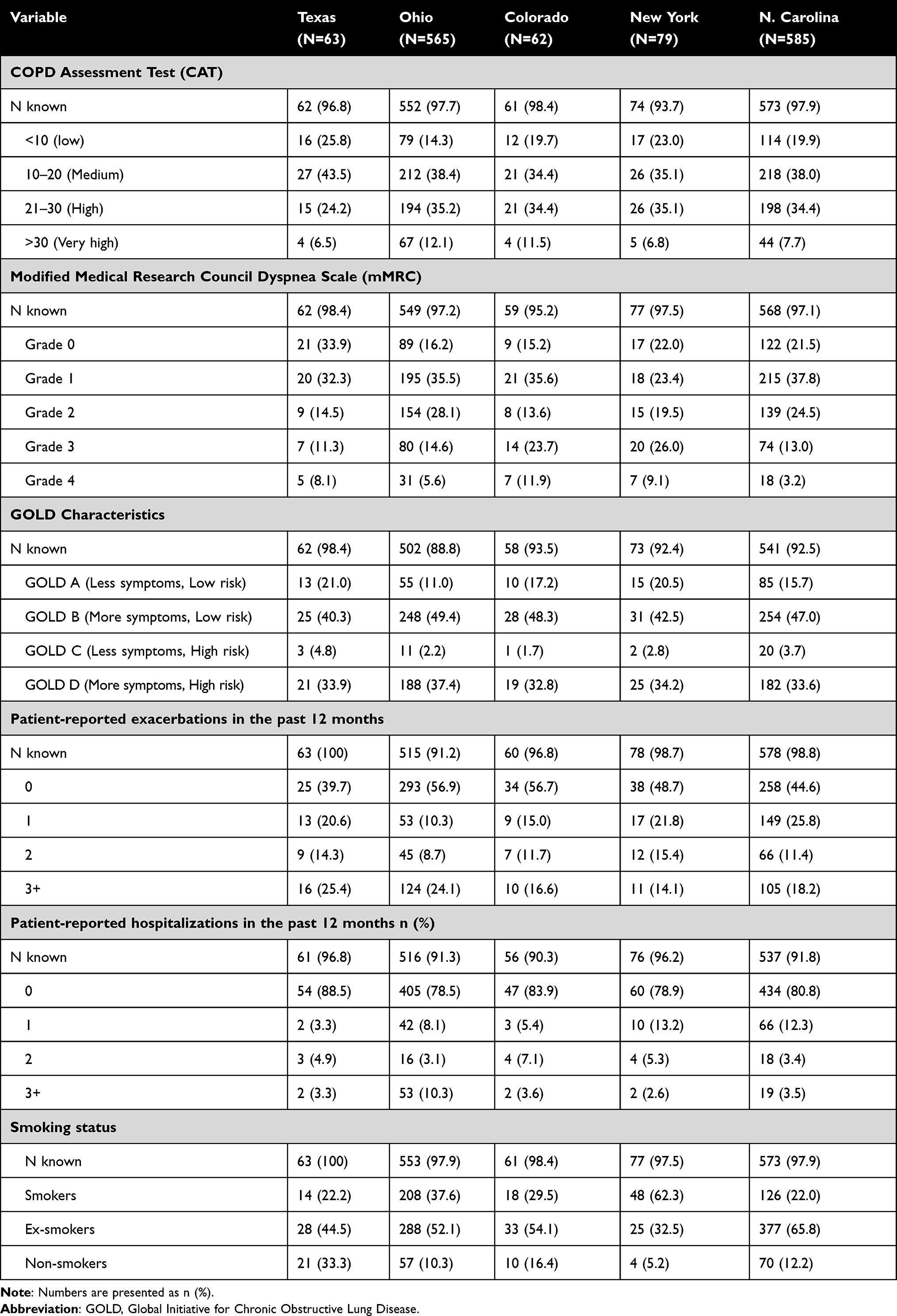 |
Table 5 Additional Patient Reported Information/Outcome Data from the APEX COPD Registry |
In Ohio and Colorado, 57% of the patients reported no exacerbation in the past 12 months. In contrast, >60% of patients from the Texas site reported having at least one exacerbation in the previous year. Texas also had the highest proportion of patients reporting 3 or more exacerbations (25.4%), compared to the lowest in New York (14.1%). Most patients reported not being hospitalized in the past 12 months (78.5–88.5%) despite more than 10% of patients in Ohio reported having had 3 or more hospitalizations.
Discussion
Summary of Findings
This study demonstrates the extent of the inter-site heterogeneity in both the demographic, clinical, and treatment characteristics, as well as patient-reported outcomes of COPD in patients with COPD managed in different healthcare organizations across 5 states in the US The study also provides an up-to-date refresh of COPD population demographics and clinical characteristics in varying situations within US primary care at a specific cross-sectional point, which can be utilized by future studies.
Slight variations in age and BMI were observed across the states, however, a wider variation was observed in patient ethnicity. Ethnicity has been suggested to play a role in the development and severity of COPD,26 and may also impact access and quality of healthcare.3 Data on the distribution of demographic characteristics may be useful for tailoring health policies according to the needs of individual sites.
Tobacco smoking remains a top risk factor for COPD and its co-morbidities.27 Smoking cessation is a key intervention for the improvement of COPD and the GOLD recommendations strongly support treatment of tobacco dependence.1 Counselling and pharmacological intervention are effective in helping patients to cease smoking.28–31 The low uptake of documented prescription pharmacological intervention to assist smoking cessation across all sites suggests a care gap that could be readily addressed. One possible approach is by promoting comprehensive and accessible insurance coverage for smoking cessation interventions.32 Interestingly, the Texas site recorded low smoking rate which may be due to smoking data not being entirely present within primary care EHR or stored separately within the system.
Both EHR-recorded and patient-reported exacerbations were collected and analyzed in this study. Regardless of the inter-site variation, we observed a higher number of patient-reported exacerbations compared to EHR-recorded exacerbations across all sites. The difference between EHR-recorded and patient-reported prevalence of exacerbation ranged from 1% in Ohio up to 24% in North Carolina. This may indicate COPD exacerbations for which the patients did not seek appointments with primary care, either self-managing or attending urgent care or other sites outside of the usual EHR system, and was thus unrecorded. Underreporting of COPD exacerbations has been observed in previous studies and is likely to be common.33,34 Since the frequency of exacerbations is important in determining appropriate pharmacotherapy, support for enhanced patient interactions with their primary care site appears to be important. Tools such as COPD Action Plans may facilitate better interactions for COPD exacerbation identification and management.35
Blood eosinophil levels are associated with a patient’s response to ICS therapy.1 In this study, the steady state total eosinophil counts varied by site. However, only half or fewer of the patients at each site had eosinophil count data. In addition, the current observation does not suggest any clear pattern between eosinophil count and ICS prescription, either as monotherapy or in combination, across the locations. This may indicate an opportunity for improved treatment selection based on appropriate biomarkers, specifically on recommendations for eosinophil measurement to direct treatment decisions.
Variation in the maintenance therapy prescribing patterns was present and might indicate differential uptake of the GOLD recommendation. Colorado had the highest proportion without maintenance treatment and also the lowest rates of EHR-derived and patient-reported exacerbations relative to the other sites. This may suggest that individuals in Colorado are being diagnosed at an early stage of COPD. This warrants further investigation as diagnosis of COPD is often delayed across the US.34
Influenza and pneumococcal vaccination are recommended for all patients with COPD.1 The varying and suboptimal uptake of vaccination may represent another opportunity for optimization of patient management.
Strengths and Limitations
This study was conducted from a registry of 17,000 primary care patients in the US across 5 healthcare organizations that collected a predefined set of data with an analysis protocol. Standardization of data collected across the sites also facilitated unbiased comparison. The study’s list of variables was selected through voting by a panel of experts, ensuring that clinically relevant variables are extracted and compared. Data within the registry was also enhanced with PRIO data from over 1000 patients, providing additional insight into the burden of COPD on patients’ lives beyond that reported in EHR data.
There are several limitations to the current study. The data in this study was originally stored for routine patient care instead of research purposes. Consequently, there is missing and incomplete data within the registry; in particular, vaccination data are not stored on-site in New York but are instead stored within a statewide database which was not accessible by the APEX team. Therefore, vaccination within New York could not be included in the current study.
Due to the nature of the study, the COPD status of patients within the registry are not directly confirmed. COPD diagnosis code was used as selection criteria instead of confirmation by spirometry. This was decided as spirometry is often not completed during diagnosis, or poorly recorded in primary care EHR.36 Therefore, no COPD-confirming result, ie FEV1/FVC ratio of >70%, was required. Additionally, due to the lack of consensus in asthma/COPD definition, lack of accuracy in diagnosis within EHR especially in the absence of confirmatory spirometry, and the ambition to gather the most representable COPD population for observation, patients with asthma-COPD overlap were included. Patients were excluded however if they were classified as an active asthma patient (visit with an asthma code within the previous 2 years).
The current study is also limited to providing descriptive analyses of the variation across healthcare systems based on all available patient EHR. Follow-up data collection and analyses would need to be conducted to generate a more solid conclusion on the reasons behind these differences between healthcare systems and their impact on COPD patient outcomes.
The difference of treatment pattern in this study also do not take into account the differences in patient characteristics within each site. Deeper analyses into the differences in appropriateness of COPD therapy relative to the GOLD recommendation across the sites are also warranted.
Conclusion
This study shows the heterogeneity in the demographic and clinical characteristics and treatment of patients diagnosed with COPD who are managed in primary care in the US These differences could stem from both real inter-location differences in the patient and disease characteristics, but may also be due to differences in uptake of guideline recommendations. Data from this study is hoped to facilitate further investigations of the differences to enable improvement and standardization of the quality of care in primary care for patients with COPD across the US.
Abbreviations
AATD, Alpha-1 anti-trypsin deficiency; APEX, advancing the patient experience; CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease; EHR, electronic health record; GOLD: Global Initiative for Chronic Obstructive Lung Disease; GERD, gastroesophageal reflux disease; ICS, inhaled corticosteroids; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist; LRTI, lower respiratory tract infection; MMRC, Modified Medical Research Council; OSA, obstructive sleep apnoea; OCS, oral corticosteroid; PRIO, patient reported information/outcomes; SABA, short-acting beta-agonist; SAMA, short-acting muscarinic antagonist; SD, standard deviation.
Data Sharing Statement
The dataset supporting the conclusions of this article was derived from the APEX COPD Registry. Anonymized Data Ethics Protocols and Transparency committee (ADEPT0520), the American Academy of Family Physicians and the APEX Steering Committee. Central ethics (Institutional Review Board, IRB) approval was obtained from the American Academy of Family Physicians for most sites (AAFP; IRB reference number: 19-349). The authors do not have permission to give public access to the study dataset; researchers may request access to APEX Registry data for their own purposes via the APEX COPD website (https://www.apexcopd.org/) or via the enquiries email [email protected].
Ethics Approval
Patient EHR data were shared in accordance with the local regulatory/ethics requirements. Informed consent was obtained from patients via an online portal to allow data sharing for ethically approved research purposes as well as recruitment for future studies. Patients were permitted to opt out of data sharing. This study was designed, implemented, and reported in accordance with the European Network Centres for Pharmacoepidemiology and Pharmacovigilance (study reference number: EUPAS29401); http://www.encepp.eu/encepp/viewResource.htm?id=29348 and performed in compliance with all applicable local laws and regulations. Governance was provided by Optimum Patient Care (OPC) Global, the Respiratory Effectiveness Group, the Anonymized Data Ethics Protocols and Transparency Committee (ADEPT0520), the American Academy of Family Physicians, and the APEX Steering Committee. Central ethics (Institutional Review Board, IRB) approval was obtained from the American Academy of Family Physicians for most sites (AAFP; IRB reference number: 19-349). Secondary ethics approval was obtained for 1 site which has their own ethics approval board.
Acknowledgments
Medical writing support was provided by Dr. Antony Hardjojo of Jaya Medical Writing Pte Ltd, Singapore. Writing, editorial support, and/or formatting assistance in the development of this manuscript was provided by Andrea Teh, BSc (Hons) and Shilpa Suresh, MSc of the Observational and Pragmatic Research Institute, Singapore. We wish to acknowledge Kidane Gebremariam for his contribution to protocol development. BIPI was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Author Contributions
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. All authors took part in drafting, revising or critically reviewing the article. All authors gave final approval of the version to be published. All authors have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work. All authors have given approval for the submission of this article. The authors received no direct compensation related to the development of the manuscript.
Funding
APEX COPD is established and maintained by Optimum Patient Care (OPC) Global Limited; and research was conducted by the Observational & Pragmatic Research Institute Pte Ltd (OPRI). The establishment of the APEX registry was co-funded by OPC Global and Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI). OPC Global retains intellectual property rights to the APEX registry.
Disclosure
Chester Fox declares no conflict of interest. Wilson Pace is on the advisory board for Mylan; stock from Eli Lilly, Novo Nordisk, Pfizer, Novartis, Johnson & Johnson, Stryker, Amgen, Gilead, and Sanofi.
Elias Brandt, Gabriela Gaona, and Rachel Kent are employees of the DARTNet Institute. Amanda Ratigan is a consultant to Boehringer-Ingelheim, but at the time of this disclosure had received no funding directly or through any organization she works for from Boehringer-Ingelheim.
Victoria Carter, Alexander Evans, Maja Kruszyk, Chantal Le Lievre, and Brooklyn Stanley are employees of Optimum Patient Care, a co-founder of the APEX COPD initiative.
Chelsea Edwards was an employee of Optimum Patient Care Australia at the time that this study was conducted.
Ku-Lang Chang declares no conflict of interest.
MeiLan K Han reports personal fees from GlaxoSmithKline, AstraZeneca, Boehringer Ingelheim, Cipla, Chiesi, Novartis, Pulmonx, Teva, Verona, Merck, Mylan, Sanofi, DevPro, Aerogen, Polarian, Regeneron, United Therapeutics, UpToDate, Altesa Biopharma, Medscape and Integrity. She has received either in kind research support or funds paid to the institution from the NIH, Novartis, Sunovion, Nuvaira, Sanofi, AstraZeneca, Boehringer Ingelheim, Gala Therapeutics, Biodesix, the COPD Foundation and the American Lung Association. She has participated in Data Safety Monitoring Boards for Novartis and Medtronic with funds paid to the institution. She has received stock options from Meissa Vaccines and Altesa Biopharma.
Alan Kaplan is a member of the advisory board of, or speakers bureau for, AstraZeneca, Behring, Boehringer Ingelheim, Covis, Cipla, Grifols, GlaxoSmithKline, Merck Frosst, Novo Nordisk, Novartis, Pfizer, Purdue, Sanofi, Teva, and Trudel.
Janwillem Kocks reports grants, personal fees and non-financial support from AstraZeneca, grants, personal fees and non-financial support from Boehringer Ingelheim, grants and personal fees from Chiesi Pharmaceuticals, grants, personal fees and non-financial support from GSK, grants and non-financial support from Mundi Pharma, grants and personal fees from TEVA, grants and personal fees from Novartis, personal fees from MSD, personal fees from COVIS Pharma, grants from Valneva outside the submitted work; and Janwillem Kocks holds <5% shares of Lothar Medtec GmbH and 72.5% of shares in the General Practitioners Research Institute.
Tessa Li Voti was an employee of Optimum Patient Care at the time this study was conducted.
Cathy Mahle and Asif Shaikh are employees of Boehringer Ingelheim, a co-founder of the APEX COPD initiative.
Barry Make reports funding from the NHLBI for the COPDGene study; grants and medical advisory boards from Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca, and Sunovion; personal fees for DSMB from Spiration and Shire/Baxalta; CME personal fees from WebMD, National Jewish Health, American College of Chest Physicians, Projects in Knowledge, Hybrid Communications, SPIRE Learning, Ultimate Medical Academy, Catamount Medical, Eastern Pulmonary Society, Catamount Medical Communications Medscape, Eastern VA Medical Center, Academy Continued Healthcare Learning, and Mt. Sinai Medical Center; royalites from Up-To-Date; medical advisory boards from Novartis, Phillips, Third Pole, Science 24/7, and Verona; grants from Pearl; outside the submitted work.
Neil Skolnik is on advisory boards for AstraZeneca, Teva, Lilly, Boehringer Ingelheim, Sanofi, Janssen Pharmaceuticals, Intarcia, Mylan, and GlaxoSmithKline; Payment for lectures/speaking engagements from AstraZeneca and Boehringer Ingelheim; Research Support from Sanofi, AstraZeneca, Boehringer Ingelheim, and GlaxoSmithKline.
Barbara P Yawn has served on COPD-related advisory boards for GlaxoSmithKline, AstraZeneca, Novartis, and Boehringer Ingelheim, Teva, receives consultancy fees from ndd Medical Technology and received COPD-related investigator-initiated research funds from GlaxoSmithKline, Boehringer Ingelheim, AstraZeneca, and Novartis.
David Price has advisory board membership with AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, Thermo Fisher; consultancy agreements with Airway Vista Secretariat, AstraZeneca, Boehringer Ingelheim, Chiesi, EPG Communication Holdings Ltd, FIECON Ltd, Fieldwork International, GlaxoSmithKline, Mylan, Mundipharma, Novartis, OM Pharma SA, PeerVoice, Phadia AB, Spirosure Inc, Strategic North Limited, Synapse Research Management Partners S.L., Talos Health Solutions, Theravance and WebMD Global LLC; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Theravance, British Lung Foundation, and UK National Health Service; payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mylan, Mundipharma, Novartis, Regeneron Pharmaceuticals and Sanofi Genzyme; payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Mundipharma, Mylan, Novartis, Thermo Fisher; stock/stock options from AKL Research and Development Ltd which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK) and 92.61% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); 5% shareholding in Timestamp which develops adherence monitoring technology; is peer reviewer for grant committees of the UK Efficacy and Mechanism Evaluation programme, and Health Technology Assessment; and was an expert witness for GlaxoSmithKline.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2021 report. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
2. World Health Organization. Burden of COPD. Available from: https://www.who.int/respiratory/copd/burden/en/.
3. National Center for Health Statistics. Health, United States. In: Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. Hyattsville (MD): National Center for Health Statistics (US); 2016.
4. Centers for Disease Control and Prevention. Leading causes of death. Available from: https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm.
5. Ford ES, Murphy LB, Khavjou O, Giles WH, Holt JB, Croft JB. Total and state-specific medical and absenteeism costs of COPD among adults aged ≥ 18 years in the United States for 2010 and projections through 2020. Chest. 2015;147(1):31–45. doi:10.1378/chest.14-0972
6. May SM, Li JT. Burden of chronic obstructive pulmonary disease: healthcare costs and beyond. Allergy Asthma Proc. 2015;36(1):4–10. doi:10.2500/aap.2015.36.3812
7. Huybrechts KF, Bateman BT, Pawar A, et al. Maternal and fetal outcomes following exposure to duloxetine in pregnancy: Cohort Study. BMJ;2020. m237. doi:10.1136/bmj.m237
8. Hill K, Goldstein RS, Guyatt GH, et al. Prevalence and underdiagnosis of chronic obstructive pulmonary disease among patients at risk in primary care. Can Med Assoc J. 2010;182(7):673–678. doi:10.1503/cmaj.091784
9. Tinkelman DG, Price D, Nordyke RJ, Halbert RJ. COPD screening efforts in primary care: what is the yield? Prim Care Respir J. 2007;16(1):41–48. doi:10.3132/pcrj.2007.00009
10. Johns DP, Walters JAE, Walters EH. Diagnosis and early detection of COPD using spirometry. J Thorac Dis. 2014;6(11):1557–1569. doi:10.3978/j.issn.2072-1439.2014.08.18
11. Albitar HAH, Iyer VN. Adherence to Global Initiative for Chronic Obstructive Lung Disease guidelines in the real world: current understanding, barriers, and solutions. Curr Opin Pulm Med. 2020;26(2):149–154. doi:10.1097/MCP.0000000000000655
12. van Schayck CP, Chavannes NH. Detection of asthma and chronic obstructive pulmonary disease in primary care. Eur Respir J. 2003;21(Supplement 39):16S–22S. doi:10.1183/09031936.03.00040403
13. Jones RCM, Price D, Ryan D, et al. Opportunities to diagnose chronic obstructive pulmonary disease in routine care in the UK: a retrospective study of a clinical cohort. Lancet Respir Med. 2014;2(4):267–276. doi:10.1016/S2213-2600(14)70008-6
14. Calverley PM. COPD: early detection and intervention. Chest. 2000;117(5 Suppl 2):365s–371s. doi:10.1378/chest.117.5_suppl_2.365S
15. Larsson K, Janson C, Ställberg B, et al. Impact of COPD diagnosis timing on clinical and economic outcomes: the Arctic Observational Cohort Study. Int J Chron Obstruct Pulmon Dis. 2019;14:995–1008. doi:10.2147/COPD.S195382
16. Ferrone M, Masciantonio MG, Malus N, et al. The impact of integrated disease management in high-risk COPD patients in primary care. NPJ Prim Care Respir Med. 2019;29(1):8. doi:10.1038/s41533-019-0119-9
17. Rennard S, Thomashow B, Crapo J, et al. Introducing the COPD Foundation Guide for Diagnosis and Management of COPD, recommendations of the COPD Foundation. COPD. 2013;10(3):378–389. doi:10.3109/15412555.2013.801309
18. Yawn BB, Thomashaw B, Mannino DM, et al. The 2017 update to the COPD Foundation COPD pocket consultant guide. COPD. 2017;4(3):177–185. doi:10.15326/jcopdf.4.3.2017.0136
19. Qaseem A, Wilt TJ, Weinberger SE, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155(3):179–191. doi:10.7326/0003-4819-155-3-201108020-00008
20. Criner GJ, Bourbeau J, Diekemper RL, et al. Prevention of acute exacerbations of COPD: American College of Chest Physicians and Canadian Thoracic Society Guideline. Chest. 2015;147(4):894–942. doi:10.1378/chest.14-1676
21. Department of Defense, D. of V. A. VA/DoD. Clinical practice guideline for the management of Chronic Obstructive Pulmonary Disease; 2014. Available from: https://www.healthquality.va.gov/guidelines/CD/copd/VADoDCOPDCPG.pdf.
22. Ridic G, Gleason S, Ridic O. Comparisons of health care systems in the United States, Germany and Canada. Mater Sociomed. 2012;24(2):112–120. doi:10.5455/msm.2012.24.112-120
23. Agency for Healthcare Research and Quality. 2018 national healthcare quality and disparities report. Available from: https://www.ahrq.gov/research/findings/nhqrdr/nhqdr18/index.html.
24. Edwards CL, Kaplan AG, Yawn BP, et al. Development of the advancing the patient experience in COPD registry: a Modified Delphi Study. COPD. 2021;8(1):135–151. doi:10.15326/jcopdf.2020.0154
25. Halpin DMG, de Jong HJI, Carter V, Skinner D, Price D. Distribution, temporal stability and appropriateness of therapy of patients with COPD in the UK in relation to GOLD 2019. EClinicalMedicine. 2019;14:32–41. doi:10.1016/j.eclinm.2019.07.003
26. Gilkes A, Ashworth M, Schofield P, et al. Does COPD risk vary by ethnicity? A retrospective cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2016;11:739–746. doi:10.2147/COPD.S96391
27. Chatila WM, Thomashow BM, Minai OA, Criner GJ, Make BJ. Comorbidities in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):549–555. doi:10.1513/pats.200709-148ET
28. Wagena EJ, Knipschild PG, Huibers MJH, Wouters EFM, van Schayck CP. Efficacy of bupropion and nortriptyline for smoking cessation among people at risk for or with Chronic Obstructive Pulmonary Disease. Arch Intern Med. 2005;165(19):2286–2292. doi:10.1001/archinte.165.19.2286
29. Tønnesen P. Smoking cessation and COPD. Eur Respir Rev. 2013;22(127):37. doi:10.1183/09059180.00007212
30. Hoogendoorn M, Feenstra TL, Hoogenveen RT, Rutten-van Mölken MPMH. Long-term effectiveness and cost-effectiveness of smoking cessation interventions in patients with COPD. Thorax. 2010;65(8):711. doi:10.1136/thx.2009.131631
31. Lemmens V, Oenema A, Knut IK, Brug J. Effectiveness of smoking cessation interventions among adults: a systematic review of reviews. Eur J Cancer Prev. 2008;17(6):535–544. doi:10.1097/CEJ.0b013e3282f75e48
32. Centers for Disease Control and Prevention. Coverage for Tobacco use cessation treatments. Content last reviewed on June 2, 2021. Available from: https://www.cdc.gov/tobacco/quit_smoking/cessation/coverage/index.htm.
33. Mohan A, Sethi S. The reliability and validity of patient-reported chronic obstructive pulmonary disease exacerbations. Curr Opin Pulm Med. 2014;20(2):146–152. doi:10.1097/MCP.0000000000000032
34. Mackay AJ, Kostikas K, Murray L, et al. Patient-reported outcomes for the detection, quantification, and evaluation of Chronic Obstructive Pulmonary Disease exacerbations. Am J Respir Crit Care Med. 2018;198(6):730–738. doi:10.1164/rccm.201712-2482CI
35. American Lung Association. My COPD action plan. Available from: https://www.lung.org/getmedia/c7657648-a30f-4465-af92-fc762411922e/fy20-ala-copd-action-plan.pdf.
36. Wells CD, Joo MJ. COPD and asthma: diagnostic accuracy requires spirometry. J Fam Pract. 2019;68(2):76–81.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.