")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
We Ask and Listen: A Group-Wide Retrospective Survey on Satisfaction with Digital Medication Software
Authors Herrmann S , Giesel-Gerstmeier J, Demuth A, Fenske D
Received 7 November 2023
Accepted for publication 9 February 2024
Published 2 March 2024 Volume 2024:17 Pages 923—936
DOI https://doi.org/10.2147/JMDH.S446896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Saskia Herrmann,1,2 Jana Giesel-Gerstmeier,1 Annika Demuth,1 Dominic Fenske1
1Hospital Pharmacy, Helios Kliniken Gmbh, Berlin, Berlin, Germany; 2Department of Pharmaceutical/Medicinal Chemistry, Institute of Pharmacy, Friedrich Schiller University Jena, Jena, Thuringia, Germany
Correspondence: Dominic Fenske, Krankenhausapotheke, Helios Klinikum Erfurt, Nordhäuser Straße 74, 99089, Erfurt, Thuringia, Germany, Tel +49 361 781 71100, Fax +49 361 781 71105, Email [email protected]
Purpose: Computerized physician order entry (CPOE) and clinical decision support systems (CDSS) are used internationally since the 1980s. These systems reduce costs, enhance drug therapy safety, and improve quality of care. A few years ago, there was a growing effort to digitize the healthcare sector in Germany. Implementing such systems like CPOE-CDSS requires training for effective adoption and, more important, acceptance by the users. Potential improvements for the software and implementation process can be derived from the users’ perspective. The implementation process is globally relevant and applicable across professions due to the constant advancement of digitalization. The study assessed the implementation of medication software and overall satisfaction.
Methods: In an anonymous voluntary online survey, physicians and nursing staff were asked about their satisfaction with the new CPOE-CDSS. The survey comprised single-choice queries on a Likert scale, categorizing into general information, digital medication administration, drug safety, and software introduction. In addition multiple-choice questions are mentioned. Data analysis was performed using Microsoft Office Excel 2016 and GraphPad PRISM 9.5.0.
Results: Nurses and physicians’ satisfaction with the new software increased with usage hours. The software’s performance and loading times have clearly had a negative impact, which leads to a low satisfaction of only 20% among physicians and 17% among nurses. 53% of nurses find the program’s training period unsuitable for their daily use, while 57% of physicians approve the training’s scope for their professional group. Both professions agree that drug-related problems are easier to detect using CPOE-CDSS, with 76% of nurses and 75% of physicians agreeing. The study provides unbiased feedback on software implementation.
Conclusion: In conclusion, digitizing healthcare requires managing change, effective training, and addressing software functionality concerns to ensure improved medication safety and streamlined processes. Interfaces, performance optimization, and training remain crucial for software acceptance and effectiveness.
Keywords: computerized physician order entry, clinical decision support system, change management, feedback, electronic prescribing
Introduction
Former German Chancellor Merkel, during her press conference with ex-president Obama in 2013, remarked, “The Internet is new territory, uncharted territory to all of us”.1 On social media, Angela Merkel was widely criticised and vilified for this statement. A decade later, healthcare digitisation still evokes strong reactions. In Germany, increased efforts to digitise healthcare have been ongoing since 2015.2 The use of computerized physician order entry (CPOE) and clinical decision support systems (CDSS) in hospitals dates back to the 1980s.3,4 Research in 1994 and 1996 indicated their potential to reduce therapy costs, enhance antibiotic stewardship, and mitigate antibiotic resistance.4,5 In addition, a recent review shows that mortality can be reduced.6 This is corroborated by a study conducted in Thailand, which demonstrates that physician’s prescribing behaviour have improved. This results in fewer prescriptions of potential inappropriate medication in elderly.7 Although CPOE is more time-consuming for physicians than paper-based prescribing, it reduces risks like transmission errors by nursing staff.3,8–10 The costs of prescribed drugs, including antibiotics, can be reduced.5,7,11 However, there is a lack of data on the costs of implementation. Comprehensive cost-benefit analyses that factor in aspect like physician time are still lacking.12 Several studies have demonstrated improved drug therapy safety when using CPOE-CDSS in combination with unit dose dispensing systems and the collaboration of hospital pharmacists.13–17 Firstly, fewer prescription errors occur, specifically, prescribing drugs despite allergies, interactions or double prescriptions.18,19 Secondly, the combination can aid the treatment team in adhering to evidence-based guidelines, identifying contraindications, and optimizing therapy while considering other patient parameters such as laboratory values, age, gender, and diagnosis.20,21 Along with the enhanced quality of care provided by the CPOE-CDSS, performance also plays a vital role.22,23 Various factors that affect the response time of the software should be tested during development to ensure optimal performance.24 The increased implementation of the 6-R rule promotes the factor of increased drug safety.19 This rule outlines that the right drug must be given to the right patient at the right time, right dosage and right route of administration, followed by right documentation of drug administration afterward.25
Human resistance to change is well-documented, even when new procedures promise to enhance daily life.26,27 Nevertheless, when changes occur, employees undergo a cycle of acceptance described by Kübler-Ross.28 The length of each phase in the cycle varies for each individual, though group dynamics still exert an influence.27,28 Successful change management involves selection of new processes/programs, team formation, training for key users, communication to future users, and gradual integration.29 Live operation support and routine operation consolidation are crucial, followed by evaluation for improvement.30
For the implementation of CPOE-CDSS at Helios Kliniken GmbH, specialist key users were trained, comprising pharmacists at regional and local levels. These pharmacists trained at least one person from each ward and occupational group among the nursing staff and physicians as key users. Further, the information was then disseminated in a cascade manner to end users within the wards. The objective is to connect the maximum care providers to the new software within 8–10 months, basic and standard care providers within 6–10 months, and specialist clinics within a quarter. From 2017 to 2023, 68 of 83 clinics (82% company-wide) were successfully connected.
CDSS is categorised as class IIa medical devices in accordance with the European Medical Device Regulation (MDR), necessitating post-market monitoring to identify preventative and corrective measures, including opportunities to improve usage (Chapter VII, Section I, Art. 83 MDR).31
In 2016 Koskela et al provided initial impressions of the implementation of a CDSS from a user perspective. They conducted interviews with individual physicians and nurses on clinical topics related to the CDSS, and the respondents expressed satisfaction but also suggested areas for improvement.32 However, the study did not focus on the technical aspects of the software or the training and immediate introduction on the wards. The implementation and use of CPOE-CDSS in hospitals worldwide has already demonstrated its effectiveness in a clinical context on several occasions (eg improve antibiotic use, reducing costs, reducing medication errors).4–6,13–17 However, data on end user satisfaction, including physicians and nursing staff, with such software is still lacking. Since the introduction of CPOE-CDSS to the Helios hospital group, the pharmaceutical key users have from time to time received complaints from doctors and nursing staff about the software’s functionality. In order to contextualise these statements and gather a picture of the users mood and due to missing data, our survey entitled, “The e-medication has demonstrated its effectiveness! Has it worked for you as well?” was conducted across all Helios hospital sites. The data collected serves a dual purpose: first to improve the software and second to refine the implementation process at the remaining Helios sites. Additionally, the data is of great interest for software introduction, especially in relation to subsequent training courses worldwide.
Materials and Methods
Pre-Test of the Survey
The pharmacy designed the questionnaire to record user satisfaction with unit dose care and CPOE-CDSS in Erfurt. The questionnaire’s further development, which related only to CPOE-CDSS, took place in cooperation with IT. The questionnaire underwent a pre-test in the Helios hospitals Erfurt and Gotha. To this end, the questionnaire was first discussed with physicians and nurses from Erfurt and adapted based on their feedback. The survey was then distributed via LimeSurvey to all physicians and nursing staff at the Helios Klinikum Erfurt. In addition to questions about CPOE-CDSS, the Erfurt survey also included questions about the introduction of unit dose care. As unit dose care had only been introduced in two clinics at that time, the questions on unit dose care were removed for a company-wide survey and the questions on CPOE-CDSS were further expanded. This version was discussed with physicians and nurses from the Helios Klinikum Gotha. As a result, questions that were considered difficult to understand were reworded. In addition, multiple-choice answers were included and open-ended questions were added to obtain a broader range of opinions. This questionnaire was then distributed to all physicians and nurses of the hospital in Gotha via LimeSurvey. In addition to the open and multiple choice questions, the majority of the survey consisted of a bipolar Likert scale.
Main Survey
The questionnaire used for the Group-wide survey is based on the pre-test conducted at Helios Klinikum Gotha. It is submitted to the group works council for final approval after the removal of questions that could identify respondents, such as gender and age, as well as well as open questions where respondents can express further opinions. The analysis can only be conducted if the group size is greater than five participants, even if the results are used within the clinic. Once all necessary changes were made, the Group Works Council approved the survey.
The final survey comprised of single-choice queries utilizing a bipolar Likert scale, supplemented by multiple-choice questions for a more comprehensive view of opinions. The survey is categorised into general information, digital medication administration, drug therapy safety, and software introduction by the hospital pharmacy and IT (Supplementary Questionnaire 1).
The voluntary and anonymous survey was conducted in all hospitals with CPOE-CDSS from June 2022 to December 2022. The survey instrument has been newly designed based on the pre-test. It is an internal survey platform used exclusively for this survey. The survey link was featured in the intranet from all company locations at the onset of the survey. The pharmacy’s local key users were requested to notify the physicians and nursing staff at their respective sites and remind them periodically to participate. The study included all physicians and nursing staff who work with CPOE-CDSS in the company. Table 1 displays the characteristics of the physicians and nurses who were invited to participate in the survey.
 |
Table 1 Characteristics of All Physicians and Nurses Employed by Helios to Whom the Survey Was Addressed |
Data and Statistical Evaluation
The survey results were presented in Microsoft Office Excel 2016, and further data analysis and statistic was conducted using Microsoft Office Excel 2016 and GraphPad PRISM 9.5.0. The scale of the questions ranges from “do not agree at all” = 1, “agree rather less” = 2, “agree rather” = 3 to “agree completely” = 4. It should be noted that, despite the conversion to numerical values, this is a subjective and not an objective perception. It is therefore not a nominal scale, which must be taken into account with regard to the statistical tests. This categorisation was created on the basis of Lee et al33 The statements “agree completey” and “agree rather” were categorised as “satisfied”. The results on satisfaction with CPOE-CDSS are presented in three different ways: as a bar/column chart, a mesh diagram or a heat map. All responses classified as satisfied were analysed for the mesh diagram. For each question, the number of satisfied respondents was divided by the number of all respondents and the resulting percentage was plotted on the grid to provide comparability across professional groups. The bar graphs reflect the individual response options. Again, the frequency of each response was determined and then plotted as a percentage. The satisfied participants are on the right side of the graph in the positive area, the left side describes the participants who did not give an answer and all the dissatisfied participants. The heat map describes the overall satisfaction. The mean of the response scale was calculated for each block of questions.
Kolmogorov–Smirnov test was used to assess normality of the data. The Mann–Whitney U-test and the Kolmogorov–Smirnov test were employed to examine for statistically significant distinctions. The choice between the two tests depended on whether the data was normally distributed or not. The internal reliability of the Likert-scales was determined through Cronbach’s alpha. The study tested three subject blocks: digital medication administration, drug therapy safety, and software introduction by the hospital pharmacy and IT. Each block comprises multiple questions, or items. To ensure consistency within each block, we evaluated the number of items, average variance, and average total variance between the items as well as the amount of questionnaires filled out. Values above 0.8 indicate good internal consistency (Table 2).
 |
Table 2 Values of Cronbach’s Alpha for the Three-Part Questionnaire |
Ethics Approval and Consent to Participate
The research conducted is a survey of clinic staff, carried out within the context of the European Medical Device Regulation, with a focus on ensuring the quality of medical devices used (Chapter VII, Section I, Art. 83 MDR). Participants were informed of the voluntary and anonymous nature of their participation through a declaration of consent, which includes information on data processing. Authorization for this study was obtained from the Group Works Council, with data protection measures in place. As this study does not involve diagnostic or therapeutic procedures on patients, no ethical approval is required.
Results
Implementation of medication software is a major change in nurses’ and physicians’ daily routines. This study aimed to identify potential problems with the new software and provide an overview of clinicians’ satisfaction.
General Data
The population surveyed is characterised in Table 1. Unfortunately, it is not possible to provide a complete characterization of participants by age and gender as this information was not recorded due to Group Works Council agreement. The purpose is to protect employees’ privacy and prevent them from making assumptions about individuals after our survey, in accordance with the data protection law. The descriptive statistics are therefore limited to the type of hospital, the period of software use, and the department in which the physicians and nurses work.
Of the medical staff, 389 from 32 sites completed the survey and 561 nurses from 38 sites. The sites were categorised as maximum care provider, basic care provider and specialist clinics. Approximately 80% of both professions work in similar parts in maximum and basic care provider, with a further 20% in specialist hospitals (Figure 1a and b). The majority of both professions work in internal medicine departments (13% of physicians and 6.4% of nurses), where CPOE-CDSS is regularly used (Supplementary Tables 1 and 2). Among physicians, 22% (n = 342) reported previous exposure to e-medication, compared to 17% (n = 475) of nurses. Half of the participants had used the newly introduced software for a period of four to twelve months (physicians 53%, n = 389; nurses 50%, n = 561, Figure 1c). Cronbach’s alpha was used to assess the internal consistency of question blocks aimed at physicians and nurses (Table 2). The computed Cronbach alpha is at least 0.87, suggesting that the questions are highly related.
 |
Figure 1 The pie chart shows the distribution of participants into types of care provider subdivided into physicians (a) and nurses (b). A total of 389 physicians answered the question in which clinic they work. This shows about 38% work in maximum care provider (148 physicians), 39% in specialist clinic (151 physicians) and 23% in basic care provider (90 physicians). A similar picture emerges for nurses with 561 participants. 41% work in maximum care provider (232 nurses), 41% in specialist clinic (214 nurses) and 21% work in basic care provider (115 nurses). Also shown is the period of use of the CPOE-CDSS in months separated into physicians and nurses (c). Nearly 50% uses the software between four to 12 months (207 physicians out of 389 and 280 nurses out of 561). 74 nurses and 65 physicians are using the software less than 3 months. (a) and (b): black = maximum care provider, grey = basic care provider, light grey = specialist clinic. (c): white with black dots = physicians; grey with diagonal stripes = nurses. |
The majority of participants use ID MEDICS as a CPOE-CDSS, so the results most likely reflect satisfaction with ID MEDICS (Further programmes at Helios: ID DIACOS PHARMA in CGM MEDICO, ORBIS Medication, iMedOne Medikation; Supplementary Table 3).
Digital Medication Management: Transitioning to the New e-Medication Software
The majority of both professions expressed confidence in their ability to use the new software (physicians 73%, n = 342; nurses 85%, n = 475). More than half of the participants agree that the prescribing software provides a superior overview of patients’ medication (56% of physicians, n = 389; 64% of nurses, n = 561) and enables a better display of available drugs listed by the hospital (74% of physicians, n = 342; 56% of nurses, n = 475). Most participants (53% physicians, n = 388; 51% nurses, n = 560) also agree that medication documentation has improved. Some participants report fewer delays in the medication process (47% of physicians, n = 386; 42% of nurses, n = 552). Only 35% of physicians (n = 388) perceive the software as helpful in the prescription process, whereas 41% of nurses (n = 473) find it useful in simplifying the daily medication process. This is confirmed by the respondents who are clearly dissatisfied with the “acceptable loading time” (satisfaction physicians 20%, n = 342; nurses 17%, n = 475) and “time relief” (satisfaction physicians 23%, n = 342; nurses 31%, n = 558; Figure 2).
 |
Figure 2 The mesh diagram is a representation of the positive feedback (statements: agree completely, agree rather) from the participants on the topic of satisfaction with the software. The dashed line within the mesh diagram marks 50%, light grey with dots symbolises physicians and black with triangle represents nurses. |
In addition, both professional groups had the opportunity to answer multiple choice questions about processes delayed before and after CPOE-CDSS implementation. It is evident that the use of CPOE-CDSS in drug research has reduced the delay in the prescribing process for physicians. The perception of delay before the introduction of CPOE-CDSS was 16%, which decreased to 8% after its introduction. Similar results were observed among the nursing staff, with a decrease from 12% to 6%. Furthermore, the implementation of CPOE-CDSS has significantly reduced the need for reworking due to changes in previously provided medicines, with a decrease from 13% to 1%. The remaining parameters are either at comparable levels or have worsened due to the new software (Figure 3a and b).
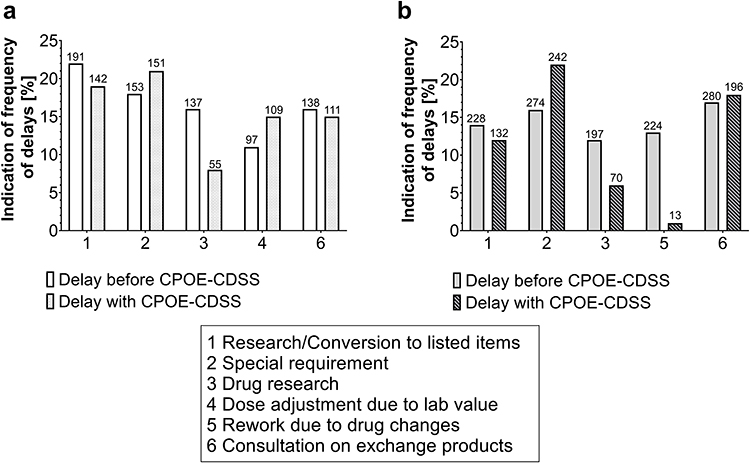 |
Figure 3 Illustration of the delays to the medication process before and after the introduction of the CPOE-CDSS from the perspective of physicians (a) and nurses (b) as column chart. The scale indicates the percentage frequency, the numbers above the columns are the absolute frequency of the answers. The left column of the grouping shows the frequency in delays before the introduction of CPOE-CDSS, the right columns show the frequency of delay from the same process after the introduction of the new software. The processes are numbered consecutively and can be found in the text box below the diagrams. White = delays in the prescription process from physicians perspective before CPOE-CDSS, white with black dots = delays in the prescription process from physicians perspective with CPOE-CDSS, light grey = delays in the prescription process from nurses perspective before CPOE-CDSS, grey with diagonal stripes = delays in the prescription process from nurses perspective with CPOE-CDSS. |
Software Training Courses
In addition to the aforementioned factors, the implementation process for end users also holds great importance. Only the availability of the pharmacy and IT department were rated positively by respondents, with 54% of physicians (n = 342) and 55% of nurses (n = 474) expressing satisfaction. However, only 40% of physicians (n = 342) and 41% of nurses (n = 475) were satisfied with live support. The transition process was not perceived as smooth, with only 36% of physicians (n = 387) and 42% of nurses (n = 558) satisfied. Half of the nurses (n = 561) felt that the training provided was sufficient, but only 47% (n = 475) felt that it met their needs. According to 47% (n = 388) of physicians, the training is adequate. Additionally, 57% (n = 342) state that it is tailored to the requirements of physicians (Figure 4a). There is a unique area of application for physicians in addition to the requests: prescription schemes. The development of these schemes by pharmacists has a satisfaction rate of 43% (n = 342). Nevertheless, the prescription plans facilitate daily practice (54% agreement, n = 341; Figure 4b).
 |
Figure 4 The mesh diagram (a) is a representation of the positive feedback (statements: agree completely, agree rather) from physicians and nurses of the implementation from the new software. The dashed line within the mesh diagram marks 50%, light grey with dots symbolises physicians and black with triangle represents nurses satisfaction. Physicians were also asked about their approval about prescriptions schemes (b), which is illustrated in a bar chart. The upper bar shows the opinion on “prescription schemes simplify daily work”, the lower one about the creation of prescription schemes. Both are divided in the categories agree completely (black with white dots), agree rather (dark grey with white dots), agree rather less (grey with black dots), do not agree at all (light grey with black dots) and not specified (white with black dots). For better visualisation, the rejection categories and the escape category are found in the negative part, the approval categories in the positive part. The 50% are represented by a dotted line. |
Drug Safety
Improving drug therapy safety via the CDSS is the primary aim. Notably, 46% of physicians felt that initial alerts were adequate despite negative visual effects, while only 37% did not agree. The “not specified” category accounted for 17% (n = 342; Figure 5a) of the negative responses. A majority of nurses (53%, n = 473) agree that the new software does not assist with the 6-R rule. In this case, 51% of nurses think there is no improvement in drug safety, while only 43% see progress (n=531, Figure 5b). Physicians were asked to what extent they change therapy in response to warnings. The data demonstrate that 64% of physicians make alterations to therapy (n=385), while only 5% never do (Figure 5c).
 |
Figure 5 Response frequencies of physicians (dotted bars, (a) and nursing (bars with diagonal stripes, (b) on the topic of drug therapy safety as well as the response frequencies of physicians on the topic of therapy adjustment after warnings (c). Negative numbers indicate rejection or not specified in a and b, positive numbers indicate agreement, white with black dots/black stripes = not specified, light grey with black dots/black stripes = do not agree at all, grey with dots/stripes = agree rather less, dark grey with white dots/lines = agree rather, black with white dots/stripes = agree completely; the dotted line marks 50%. The adjustment of therapy is presented as column chart, the colours get lighter with less adjustment after initial warning of the CPOE-CDSS by physicians. To the right of the columns are the absolute response frequencies. |
Overall Satisfaction
The selected comparisons include history of e-medication use (category 2), duration of software use (category 3–5) and type of clinic (category 6–8). Values above 2.5 indicate satisfaction with the respective question category. Values between 1 and 4 can be reached by the graded response options (see Methods - Statistical analysis). Drug safety received high satisfaction ratings (all values > 2.5) in all comparison categories. Among physicians, only those who have previously used a similar program expressed satisfaction with Digital Medication Management (2.6) and the software’s introduction (2.6, Figure 6a).
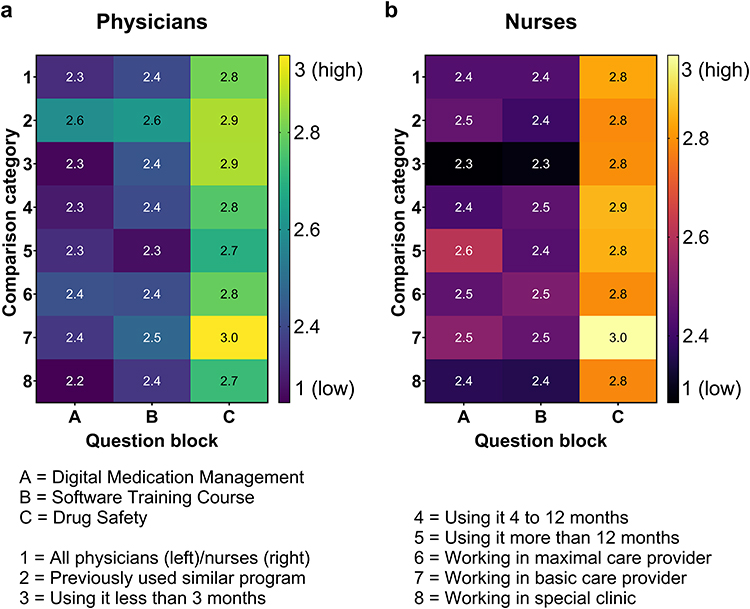 |
Figure 6 The heat map displays satisfaction levels in categories 1–8, divided into question blocks (A–C). Values above 2.5 indicate satisfaction and are represented by light colours (blue-green to yellow in a; pink to yellow in (b). Darker colours indicate lower satisfaction levels with the CPOE-CDSS or its implementation. 1 = All physicians (left, (a)/nurses (right, (b); 2 = Previously used similar program; 3 = Using CPOE-CDSS less than 3 months; 4 = Using CPOE-CDSS 4 to 12 months; 5 = Using CPOE-CDSS more than 12 months; 6 = Working in maximal care provider; 7 = Working in basic care provider; 8 = Working in special clinic. A = satisfaction with digital medication management; B = satisfaction with software training course; C = satisfaction with drug safety. |
Satisfaction with drug safety in nurses, however, is evident with values above 2.5. Furthermore, nursing staff who have used the software for more than 6 months report higher satisfaction with Digital Medication Management compared to other categories, with a value of 2.6. In the Digital Medication Management questionnaire block (2.5), the nursing staff of a basic care provider demonstrated neutrality, while the nursing staff of a maximum care provider showed neutrality in relation to the Software Training Course (2.5, Figure 6b). The survey results indicate that both physicians and nursing staff are dissatisfied with Digital Medication Management and Software Training Course, as shown by values below 2.5 (Figure 6a and b).
Discussion
Due to precise monitoring of the implementation of the CPOE-CDSS, personal evaluations of the programme have already been conveyed to the key users, verbally and through e-mails. The survey was carried out to provide an unbiased assessment of these viewpoints and to guarantee quality with regard to MDR.
Overall, the professional groups are content with the software’s features. However, they do not experience any ease from the supporting functions of the CPOE-CDSS because of the extended loading times (see Figure 2). In terms of software management, “acceptable loading times” is the least tolerable factor. Over 30 years ago, Card et al demonstrated that fast loading times are crucial, and that loading times exceeding 10 seconds result in a loss of user attention.34 This issue remains as relevant as ever in today’s fast-paced world.35 User satisfaction decreases with each passing second, and in healthcare sector, rapid access to medication is essential in an emergency.35,36 Reports of this issue had been increasing before the survey. Therefore, it was crucial to collect user feedback to identify possible software enhancements. After presenting the results to the hospital group, the task force for performance was established. They will analyse and measure loading times depending on release changes, and are constantly working on improving infrastructure.
However, individuals who have prior experience with e-medication are more satisfied with the program in comparison to those who have used it for less than three months. This may be due to the fact that users are more familiar with the programme and it has become part of their routine.37
On top of everything, comments of the pre-test (data not shown) already point out the absence of interfaces to the chemotherapy software, intensive care unit, patients’ laboratory values, ordering software on the wards, and the faulty scanning of the national medication plan. The disruptions in media are also indicated by the multiple-choice questions (Figure 3). In line with the comments Figure 3 shows a worsening with regard to therapy adjustment due to lab values. To increase drug management, developers are committed to ensuring uninterrupted patient care. In addition to patient safety factors, the ordering process also plays a role in the context of media disruptions. In the past, wards had to fax special requirements in requests for drugs that were not in stock to the pharmacy. This not only increased paper consumption but also complicated the nursing staff’s daily work. Due to the results of our survey, special requirements can now be submitted through the digital ordering software, in addition to regular ward orders. In this light, an interface between the CPOE-CDSS and the ordering software is under development to automatically generate order proposals after receiving a clinician’s request. This means that the ordering system and CPOE-CDSS can be seamlessly linked. Interfaces such as these, particularly those related to patient safety, play a crucial role in the ongoing development of CPOE-CDSS.38 The integration of laboratory values into a CPOE-CDSS is still considered a novelty, as previous studies have shown.39,40 The benefits of such an interface have been demonstrated.41 For example, dose adjustment based on renal values. This also contributes to the development of interfaces to other systems, such as chemotherapy software or software in intensive care units.
The dissatisfaction rates among physicians and nurses regarding the changeover process are concerning, with 62% and 54% respectively (see Figure 4a). Users’ satisfaction with the ease of access to pharmacy and IT services in case of issues is a positive aspect to emphasise. This shows that the new issues raised are both pharmaceutical and technical in nature and that interprofessional collaboration is of great benefit to the user.42,43 This collaboration is relevant because digitalisation is enriching everyday clinical and pharmaceutical life in all areas. Furthermore, while physicians found the training materials to be relevant, nurses were less satisfied (see Figure 4a, 57% vs 47%). Initially, product management favoured comprehensive training covering all functions, regardless of the system’s future application or user group, in order to supplement knowledge. Because of our survey and verbal feedback, the nursing staff’s training was modified to their specific needs. Training focuses only on essential functions, and follow-up sessions are provided with each new release and functionality to enhance knowledge. Medical staff have requested on-site explanation of the nursing staff training for support. This demonstrates the usefulness of conducting a survey to learn and adapt processes. New employees at all 80 Helios sites can also benefit from the adjustments made. The survey showed limited enthusiasm for the on-site support by local pharmacy key users. This may be because different hospital sites have different key users, making the results not fully applicable. Due to the intra-individual differences of the key users, various points must be taken into account when evaluating this item. On the one hand, there are different key users, which means that interpersonal problems play a role in answering the question, and on the other hand, there may have been short-term changes to the schedule due to staff shortages. It is therefore not possible to provide a completely objective assessment of real-life operational support and it remains a matter of conjecture as to why the results of the question are rather inconsistent.
Additionally, the initial adjustment to a new system can be challenging, requiring a period of rebuilding familiar routines, which is in line with literature.28,37 Implementing the new system at the wards, as seen at the University Hospital of Leverkusen, meant first integrating new admissions into the new process to allow the old and new system to run parallel. Switching from the previous routine to CPOE-CDSS was evaluated as unfavourable, regardless whether a CPOE-CDSS has already been used or not (see Figure 6). At a software user meeting (internal software data, data not shown), University Hospital of Leverkusen reported receiving feedback from users that using both processes (paper-based health record and CPOE-CDSS) simultaneously caused more confusion, and that a full transition of all patients at once would be preferable. Users at Helios Kliniken GmbH may also agree this sentiment. It is not possible to convert all health records to the new system overnight. The changeover process in Leverkusen took 30 months, according to their own information. In contrast Helios Kliniken GmbH aims to connect its clinics faster, as described above in the introduction. However, users may find this transition too rapid, which can cause further dissatisfaction. Although satisfaction with the speed of the changeover process was not part of the questionnaire, it can still be assumed that personal preferences may play a role in the process.27,28 Further investigations could explore this point.
The prescription schemes are a special feature of the software. The medical staff are generally content with the operation of prescription schemes, including those drafted by pharmaceutical key users (see Figure 4b). Such schemes facilitate speedy initiation of infusions, given that the involved prescription can be intricate, necessitating customisation of the carrier solution and infusion pace, which makes prompt ordering impractical in everyday clinical settings. Therefore, templates have been developed for adjusting medication dosages based on laboratory parameters. These templates can even store complex dosages, such as glucocorticoid therapies with up- and down-titration, eliminating the need for physicians to adjust dosages for every patient. At Helios, the prescription schemes are used in particular to make the anti-infective therapy of patients as safe as possible, also in view of the fact that the use of antibiotics was already reduced around 30 years ago thanks to CDSS.4,5 The templates enable direct adaptation of anti-infective therapy to kidney values, without the need for complicated adjustments to the anti-infective agent, carrier solution, or running speed. Each template title includes the dosage and the corresponding kidney values.
Particularly positive is the improvement in drug safety, which received a high level of satisfaction from both professional groups, bolstering existing literature (see also Figure 6).4,515–17 This is why there has been increasing development in this area, supported by politicians. Physicians consider the initial messages generated by the software regarding dose adjustments, interactions, and multiple prescriptions as rather unsuitable
The issue of over-alerts is acknowledged and requires further attention.44 An immediate remedy is not feasible considering the stored database. Basic information regarding drugs authorized in Germany can be found there (e g divisibility of tablets, dosage form). Nevertheless, they actively use this function to manage patients’ therapies. Furthermore, it includes a drug safety check, which assesses drugs for any potential interactions, individual drug risks (such as allergies), double medication, or any other potential risks. The topic of over alert is currently subject of further research.45 The question remains as to whether the adjustment rate stated by the physicians (Figure 5c) corresponds to reality. According to our survey, 64% of physicians claim to follow at least 50% of the warning messages provided by the software. However, there may be discrepancies between hospitals that use unit dose dispensing systems and those where nursing staff still administer medication. In hospitals with unit dose dispensing systems, clinical pharmacists verify medication and provide information on clinically relevant medication errors. A study conducted across Germany has demonstrated that more than 80% of the information provided by clinical pharmacists is accepted by physicians, which is supported by international literature.46
To support the 6-R rule in nursing, closed loop medication management should enable scanning patients’ wristband and drugs supplied by unit dose dispensing systems As shown in Figure 5b, nursing is not satisfied with the item “Support of the 6R rule” by CPOE-CDSS. This is because the interfaces still need to be fully implemented. Currently, nursing does not have the option to scan medication and patient wristbands. Yet the pre-test has already shown that unit dose dispensing systems lead to better patient care (data not shown). In the survey, unit dose dispensing systems are not significant as they have only been used at five locations so far. It is worth noting that CPOE-CDSS has made it easier for nursing staff to handle the issue of “Rework due to drug changes” (refer to Figure 3b). The changes in medication are now more easily identifiable.
Finally, it cannot be ruled out that only a certain group of people took part in the survey (eg only younger users, computer-savvy participants). However, the pre-test results in Erfurt suggest that a representative cross-section of the population participated. Additionally, the survey aims to present personal opinions objectively, despite the highly emotional nature of the topic for users. It is possible that participants may express dissatisfaction, which could diminish the significance of positive opinions.
Conclusion
For the first time, our survey provides a comprehensive, current overview of the use of a CPOE-CDSS in everyday clinical practice. It is important to note that, despite current shortcomings of the CPOE-CDSS, it is still a successful software tool in achieving their key objective: drug safety. The weaknesses of CPOE-CDSS are primarily due to the digital environment, including lack of interfaces with other clinical programs and slow loading times. The software developers should prioritise responding to the needs of end users. Providing good training and satisfactory on-site support from pharmaceutical key users, as well as follow-up training, is essential for user acceptance. The study provides a scientific analysis to identify opportunities for improvement in a number of areas, as well as meeting the requirements of the MDR. Previous studies have already proven that the use of CPOE-CDSS increases patient safety and the prescription schemes offer further opportunities for improvement. In addition, compared to paper-based health records, interactions and overdoses can now be accessed quickly and easily. This aspect was highly valued by users in our survey.
Abbreviations
CPOE, computerized physician order entry; CDSS, clinical decision support systems; MDR, Medical Device Regulations.
Data Sharing Statement
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request.
Acknowledgments
We thank our colleagues who provided insight and expertise that greatly assisted the research and also for their comments on an earlier version of the manuscript. We thank our reviewers for their insights.
Funding
The authors have no relevant funding to disclose for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Office of the Press Secretary. Remarks by President Obama and German Chancellor Merkel in Joint Press Conference. Available from: https://obamawhitehouse.archives.gov/the-press-office/2013/06/19/remarks-president-obama-and-german-chancellor-merkel-joint-press-confere.
2. Bundesgesundheitsministerium. Digitalisierung im Gesundheitswesen. Available from: https://www.bundesgesundheitsministerium.de/themen/digitalisierung/digitalisierung-im-gesundheitswesen.html.
3. Berger RG, Kichak JP. Computerized physician order entry: helpful or harmful? J Am Med Inform Assoc. 2004;11(2):100–103. doi:10.1197/jamia.M1411
4. Pestotnik SL, Classen DC, Evans RS, Burke JP. Implementing antibiotic practice guidelines through computer-assisted decision support: clinical and financial outcomes. Ann Intern Med. 1996;124(10):884–890. doi:10.7326/0003-4819-124-10-199605150-00004
5. Evans RS, Classen DC, Pestotnik SL, Lundsgaarde HP, Burke JP. Improving empiric antibiotic selection using computer decision support. Arch Intern Med. 1994;154(8):878–884.
6. Curtis CE, Al Bahar F, Marriott JF. The effectiveness of computerised decision support on antibiotic use in hospitals: a systematic review. PLoS One. 2017;12(8):e0183062. doi:10.1371/journal.pone.0183062
7. Nguyen -T-T, Hollands W, Zaiken K. Optimization of medication point-of-prescribing alerts at a multi-site, ambulatory care organization to aid clinical care and reduce healthcare cost. J Pharm Pract. 2023;36(4):845–852. doi:10.1177/08971900221079022
8. Barron WM, Reed RL, Forsythe S, et al. Implementing computerized provider order entry with an existing clinical information system. J Qual Patient Safe. 2006;32(9):506–516. doi:10.1016/s1553-7250(06)32066-1
9. McDonald CJ, Overhage JM, Mamlin BW, Dexter PD, Tierney WM. Physicians, information technology, and health care systems: a journey, not a destination. J Am Med Inform Assoc. 2004;11(2):121–124. doi:10.1197/jamia.M1488
10. Pesel G, Ricci G, Gibelli F, Sirignano A. Electronic unified therapy record as a clinical risk management tool in the Italian healthcare system. Front Public Health. 2022;10:919543. doi:10.3389/fpubh.2022.919543
11. McMullin ST, Lonergan TP, Rynearson CS. Twelve-month drug cost savings related to use of an electronic prescribing system with integrated decision support in primary care. J Manag Care Pharm. 2005;11(4):322–332. doi:10.18553/jmcp.2005.11.4.322
12. Donovan T, Abell B, Fernando M, McPhail SM, Carter HE. Implementation costs of hospital-based computerised decision support systems: a systematic review. Implement Sci. 2023;18(1):7. doi:10.1186/s13012-023-01261-8
13. H-N T, Shan T-H, Y-C W, et al. Reducing medication errors by adopting automatic dispensing cabinets in critical care units. J Med Syst. 2023;47(1):52. doi:10.1007/s10916-023-01953-0
14. Wylegała K, Religioni U, Czech M. The impact of hospital pharmacy operation on the quality of patient care. Int J Environ Res Public Health. 2023;20(5). doi:10.3390/ijerph20054137
15. Kaushal R, Shojania KG, Bates DW. Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review. Arch Intern Med. 2003;163(12):1409–1416. doi:10.1001/archinte.163.12.1409
16. Foo GTT, Tan CH, Hing WC, Wu TS. Identifying and quantifying weaknesses in the closed loop medication management system in reducing medication errors using a direct observational approach at an academic medical centre. J Pharm Pract Res. 2017;47(3):212–220. doi:10.1002/jppr.1235
17. Franklin BD, O’Grady K, Donyai P, Jacklin A, Barber N. The impact of a closed-loop electronic prescribing and administration system on prescribing errors, administration errors and staff time: a before-and-after study. Qual Saf Health Care. 2007;16(4):279–284. doi:10.1136/qshc.2006.019497
18. Pontefract SK, Hodson J, Slee A, et al. Impact of a commercial order entry system on prescribing errors amenable to computerised decision support in the hospital setting: a prospective pre-post study. BMJ Qual Saf. 2018;27(9):725–736. doi:10.1093/jamia/ocw119
19. Armstrong I, Cox MA. Horus meets Nightingale in the modern age: how nursing communicates with pharmacy in HCIT era. Stud Health Technol Inform. 2006;122:585–586.
20. Eisend S, Lemmer L, Melzer S, et al. Leitlinie: anforderungen an eine Unit-Dose Versorgung in der Krankenhausapotheke. Available from: https://www.adka.de/index.php?eID=dumpFile&t=f&f=3717&token=4313d5da192351f6d0b6db8b4a2a90589c09b460.
21. Yu FB, Menachemi N, Berner ES, Allison JJ, Weissman NW, Houston TK. Full implementation of computerized physician order entry and medication-related quality outcomes: a study of 3364 hospitals. Am J Med Qual. 2009;24(4):278–286. doi:10.1177/1062860609333626
22. Bates DW, Kuperman GJ, Wang S, et al. Ten commandments for effective clinical decision support: making the practice of evidence-based medicine a reality. J Am Med Inform Assoc. 2003;10(6):523–530. doi:10.1197/jamia.M1370
23. Bonhag W, Olschner S, Feindt D, Schubert U. Wie schnell ist “schnell” bei Business-Software?: analyse zur Performance bei der Nutzung von Business-Software. Mensch Computer. 2015;22–32. doi:10.1515/9783110443882-004
24. Pargaonkar S A comprehensive review of performance testing methodologies and best practices: software quality engineering; 2024.
25. Dietmaier O, Schmidt S, Laux G. Pflegewissen Psychopharmaka. Berlin, Heidelberg: Springer; 2019.
26. Rehman N, Mahmood A, Ibtasam M, Murtaza SA, Iqbal N, Molnár E. The psychology of resistance to change: the antidotal effect of organizational justice, support and leader-member exchange. Front Psychol. 2021;12:678952. doi:10.3389/fpsyg.2021.678952
27. Hehn S, Cornelissen NI, Braun C. Kulturwandel in Organisationen. Berlin, Heidelberg: Springer; 2016.
28. Meiler MM. Emotionales Change Management. Berlin, Heidelberg: Springer; 2020.
29. van de Wetering R. IT-Enabled clinical decision support: an empirical study on antecedents and mechanisms. J Healthc Eng. 2018;2018:6945498. doi:10.1155/2018/6945498
30. Hochuli Freund U, Gebert J, Sprenger R, Amez-Droz P, Hübscher R, Grumbinaite I. Wie Entwicklungs- und Implementierungsprozesse gelingen können: skizze eines integrativen Phasenmodells. Organ Super Coach. 2022;1–20. doi:10.1007/s11613-022-00799-8
31. ID Information und Dokumentation im Gesundheitswesen GmbH & Co. KGaA. eMedikation: arzneimitteltherapiesicherheit verbessern mit dem Closed Loop Medication Management. Available from: https://www.id-berlin.de/produkte/emedikation/.
32. Koskela T, Sandström S, Mäkinen J, Liira H. User perspectives on an electronic decision-support tool performing comprehensive medication reviews - a focus group study with physicians and nurses. BMC Med. Inf. Decis. Making. 2016;16(1):1–9. doi:10.1186/s12911-016-0245-z
33. Lee F, Teich JM, Spurr C, Bates DW. Implementation of physician order entry: user satisfaction and self-reported usage patterns. J Am Med Inform Assoc. 1996;3:42–55.
34. Card SK, Robertson GG, Mackinlay JD. The information visualizer, an information workspace. Proceed SIGCHI Confer Hu Fact Comp Sys. 1991;3:181–186.
35. Kumari R Response Time Testing – what it is & How to Measure it? Available from: https://testsigma.com/blog/response-time-testing/.
36. gematik GmbH. Notfalldaten: einfach da, wenn es darauf ankommt. Available from: https://www.gematik.de/anwendungen/notfalldaten.
37. Jimenez G, Spinazze P, Matchar D, et al. Digital health competencies for primary healthcare professionals: a scoping review. Int J Med Inform. 2020;143:104260. doi:10.1016/j.ijmedinf.2020.104260
38. Gawer A. Digital platforms’ boundaries: the interplay of firm scope, platform sides, and digital interfaces. Long Range Planning. 2021. doi:10.1016/j.lrp.2020.102045
39. Verdoorn S, Kwint HF, Hoogland P, Gussekloo J, Bouvy ML. Drug-related problems identified during medication review before and after the introduction of a clinical decision support system. J Clin Pharm Ther. 2018;43(2):224–231. doi:10.1111/jcpt.12637
40. Sutton RT, Pincock D, Baumgart DC, Sadowski DC, Fedorak RN, Kroeker KI. An overview of clinical decision support systems: benefits, risks, and strategies for success. NPJ Digit Med. 2020;3:17. doi:10.1038/s41746-020-0221-y
41. Ibáñez-Garcia S, Rodriguez-Gonzalez C, Escudero-Vilaplana V, et al. Development and evaluation of a clinical decision support system to improve medication safety. Appl Clin Inform. 2019;10(3):513–520. doi:10.1055/s-0039-1693426
42. Zielińska-Tomczak Ł, Cerbin-Koczorowska M, Przymuszała P, Marciniak R. How to effectively promote interprofessional collaboration? – a qualitative study on physicians’ and pharmacists’ perspectives driven by the theory of planned behavior. BMC Health Serv Res. 2021;21(1):1–13. doi:10.1186/s12913-021-06903-5
43. Ismail S, Osman M, Abulezz R, Alhamdan H, Quadri KHM. Pharmacists as interprofessional collaborators and leaders through clinical pathways. Pharmacy. 2018;6(1). doi:10.3390/pharmacy6010024
44. van Doormaal JE, Rommers MK, Kosterink JGW, Teepe-Twiss IM, Haaijer-Ruskamp FM, Mol PGM. Comparison of methods for identifying patients at risk of medication-related harm. Qual Saf Health Care. 2010;19(6):e26. doi:10.1136/qshc.2009.033324
45. Chen C-Y, Chen Y-L, Scholl J, Yang H-C, Li Y-CJ. Ability of machine-learning based clinical decision support system to reduce alert fatigue, wrong-drug errors, and alert users about look alike, sound alike medication. Comput Methods Programs Biomed. 2024;243:107869. doi:10.1016/j.cmpb.2023.107869
46. Langebrake C, Hohmann C, Lezius S, et al. Clinical pharmacists’ interventions across German hospitals: results from a repetitive cross-sectional study. Int J Clin Pharm. 2021:1–8. doi:10.1007/s11096-021-01313-3
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.