")
Back to Journals » Clinical Interventions in Aging » Volume 18
Whether Assisted Intramedullary Nail Implantation Without Traction Table is as Safe and Effective as Using Traction Table of Older Intertrochanteric Fracture Patients?
Authors Li DY, Liu CG, Zhang K
Received 29 November 2022
Accepted for publication 4 March 2023
Published 10 March 2023 Volume 2023:18 Pages 387—395
DOI https://doi.org/10.2147/CIA.S399608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Dong-Yang Li,1,2 Chun-Gui Liu,1,2 Kun Zhang1
1Department of Orthopedic Trauma, Honghui Hospital, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 2Xi’an Medical University, Xi’an, People’s Republic of China
Correspondence: Kun Zhang, Email [email protected]
Purpose: Despite promising clinical outcome proposals, there has been relatively little published regarding the use of traction table-assisted intramedullary nail implantation for intertrochanteric fractures. The purpose of this study is to further summarize and evaluate published clinical studies comparing the clinical outcomes of using traction table and without traction table in the management of intertrochanteric fracture.
Methods: A comprehensive literature search using PubMed, Cochrane Library, and Embase was systematically performed to evaluate all studies included in the literature up to May 2022. The search terms included “intertrochanteric fractures”, “hip fractures”, and “traction table” with Boolean operators “AND” and “OR”. The following information was extracted and summarized: demographic information, setup time, surgical time, amount of bleeding, fluoroscopy exposure time, reduction quality, and Harris Hip Score (HHS).
Results: A total of eight clinical controlled studies involving 620 patients were eligible for the review. The mean age at the time of injury was 75.3 years (traction table group 75.7 years, non-traction table group 74.9 years). The most common assisted intramedullary nail implantation method of non-traction table group included lateral decubitus position (4 studies), traction repositor, (3 studies) and manual traction (1 studies). Included studies results all support that there was no difference between the two groups in terms of reduction quality and Harris Hip Score, and the non-traction table group had an advantage in terms of setup time. However, there were still disputes in terms of surgical time, amount of bleeding and fluoroscopy exposure time.
Conclusion: For patients with intertrochanteric fractures, assisting intramedullary nail implantation without traction table is as safe and effective as using traction table and doing so without a traction table may be more advantageous in terms of setup time.
Keywords: intertrochanteric fractures, traction table, closed reduction, internal fixation, systematic review
Introduction
As the aging population and longer life expectancy rapidly increase. Intertrochanteric fractures due to osteoporosis are increasingly common.1–3 While the treatment of intertrochanteric fractures has shown encouraging results with current technology and implants, the percentage of 20% of patients still fail the treatment.4,5 The management of intertrochanteric fractures remains a major challenge for orthopedic surgeons.
As the first choice for treatment of intertrochanteric fractures, compared with plates and screws, intramedullary devices have better biomechanical advantages, and minimal soft tissue injury.6–8 It has been well established that no matter what kind of devices are used, intraoperative traction reduction is an important part of successful surgery.9,10 In order to obtain better reduction quality, the currently preferred treatment method of intramedullary nailing for the treatment of intertrochanteric fractures is to take the supine position on the orthopedic surgery traction table.11,12
Traction tables are commonly used to treat lesions around the hip joint (fracture fixation, hip arthroscopy, and minimally invasive arthroplasty)) to achieve and maintain reduction.13,14 Previous studies have reported many advantages of the traction table, including ease of surgical manipulation and imaging procedures, and can be done with fewer assistants or by the surgeon alone. Traction tables have gained wide acceptance and have shown good clinical outcomes. However, the reported possible complications remain numerous, including neurological injuries, soft tissue contusions, pressure ulcers, compartment syndrome, crush syndrome, and vascular injuries.15–17 Therefore, the exact indication for the use of a traction table still deserves further evaluation, Furthermore, traction tables have certain requirements for hospital surgical equipment, which limits the application and development of hospitals with limited resources.
To avoid traction table-related complications and dependence on the traction table, some researchers have used the lateral decubitus position and traction repositor to assist in the implantation of intramedullary nails.18–20 According to published articles, the lateral decubitus position and traction repositor are advantageous, but whether their use is as safe and efficient as the traction table is still unknown.
The aim of this study was to further summarize and evaluate published clinical studies comparing the clinical outcomes of using traction table and without traction table in the management of intertrochanteric fracture.
Methods and Materials
To conduct a comprehensive study of the evidence, we performed a systematic review of the literature. The review was conducted by searching the following databases: PubMed, Cochrane Library, and Embase. For the maximum range of potentially relevant literature, screening with keywords, including “intertrochanteric fractures”, “hip fractures”, and “traction table” with Boolean operators “AND” and “OR” was performed. The search period was from database creation to May 2022. All titles and abstracts were reviewed for relevance. Those considered consistent to the stated purposes of this review were read in full text and had their information extracted. At least two investigators evaluated each article. If there was a disagreement between the reviewers, then discrepancies were resolved by a third reviewer. Our search strategy is shown in Figure 1.
 |
Figure 1 Flowchart of included studies. |
The inclusion criteria were as follows: 1) clinical control studies comparing the clinical outcomes of using traction table and without traction table in the management of intertrochanteric fracture; 2) a minimum means radiological and clinical follow-up period of 6 months; 3) postoperative surgical data, and functional and radiological outcome data are available.
The exclusion criteria were biomechanical studies, computational and finite element analyses, and other nonclinical applications. Moreover, case reports and gray literature were also excluded.
From the included studies, we extracted and analyzed the following data: demographic information, setup time, surgical time, amount of bleeding, fluoroscopy exposure time, reduction quality, and HHS. Continuous variable data were reported as mean and standard deviations from the mean. Categorical variable data were reported as frequency with percentages. The primary outcomes were surgical time, reduction quality, and HHS. The secondary outcomes were setup time, amount of bleeding, fluoroscopy exposure time. Most of the literature applied different evaluation criteria, or the data reports were incomplete. We could not conduct a meta-analysis because of high heterogeneity. We only conducted a descriptive analysis of these date.
Results
In total, eight clinical studies, including three randomized controlled trials (RCTs) and five case–control studies, were eligible for our research and met the inclusion criteria. Of these eight studies, four studies comparing the radiographic and clinical outcomes of traction table versus lateral decubitus in the treatment of intertrochanteric fractures.21–24 Three studies compared the clinical outcomes of intertrochanteric fractures treated with traction repositors (without a traction table) with those treated using a traction table.25–27 One study compared the final outcomes of a traction table versus manual traction for the treatment of unstable intertrochanteric fractures.4 The general information of the included studies is illustrated in Table 1. A total of 620 patients were included at the baseline; at study completion, only 603 patients were included in the data analysis (295 patients treated with a traction table and 308 without a traction table). The mean age at the time of injury was 75.3 years (traction table group 75.7 years, non-traction table group 74.9 years).
 |
Table 1 Baseline Information of the Included Studies |
Primary Outcomes
Surgical Time
Surgical time was the important outcome analyzed in this systematic review. Seven of the eight studies reported surgical time. In the non-traction table group, three studies reported the use of the lateral decubitus position,22–24 three studies reported the use of a traction repositor,25–27 and one study reported the use of manual traction.4 As enumerated in Table 2, four studies reported that surgical time was shorter in the non-traction table group than in the traction table group. No difference was found in three studies.
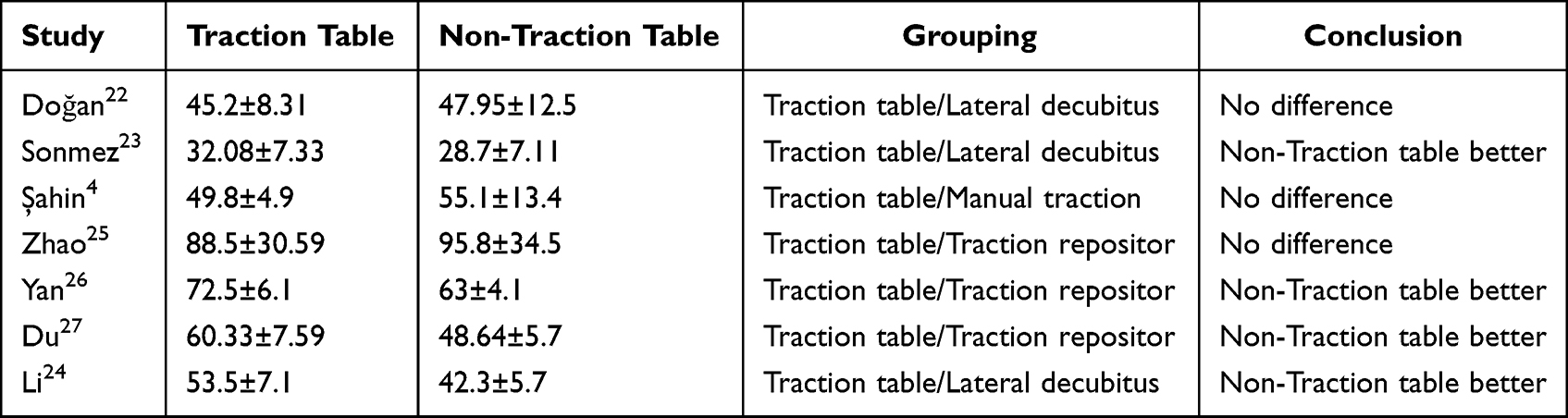 |
Table 2 Mean Surgical Time in Min (Mean ± SD) |
Reduction Quality
Reduction quality was the most important primary outcome of this study. We extracted and analyzed the relevant data of five studies. Two studies used the Baumgaertner system to evaluate reduction quality.22,23,28 Two studies evaluated reduction quality according to the criteria of Schipper.4,25,29 One study assessed reduction quality using the Garden alignment index.,26,30 as enumerated in Table 3. While different authors used different criteria, the conclusions they reached were consistent.
 |
Table 3 Reduction Quality |
Harris Hip Score
Function, as the most important prognostic criterion, was our primary outcome. A total of 6 articles reported the HHS of patients at different times. Five articles recorded specific scores, as enumerated in Table 4. All studies found no difference between the two groups. In Yan’s study, with at least one year of follow-up, the HHS in the non-traction table group was excellent in 10 patients (17.9%), good in 36 (64.3%), fair in 8 (14.3%), and poor in 2 (3.6%). Similar results were obtained with the traction table group, which were excellent in 8 patients (20.5%), good in 24 (61.5%), fair in 6 (15.4%), and poor in 1 (2.6%). 26
 |
Table 4 Mean Harris Hip Score (Mean ± SD) |
Secondary Outcomes
Setup Time
The period from the transfer of patients from the anesthesia group to the surgery group until the skin incision was defined as the setup time. Four of the eight studies reported the setup time as we defined it. As enumerated in Table 5, there was a significant difference between the groups in all the studies. The non-traction table group has a clear advantage in terms of setup time.
 |
Table 5 Mean Setup Time in Min (Mean ± SD) |
Amount of Bleeding
Six of the eight studies reported the amount of bleeding. The amount of bleeding reported by different studies varied greatly, which may be mainly due to the different types of implants used in the different studies or differences in surgical proficiency. As enumerated in Table 6, most studies concluded that there was no difference in the amount of bleeding between the traction table group and the non-traction table group.
 |
Table 6 Mean Amount of Bleeding in Ml (Mean ± SD) |
Fluoroscopy Exposure Time
Five of the eight studies reported fluoroscopy exposure, three of the studies reported the fluoroscopy exposure time4,22,23 and two studies reported the frequency of fluoroscopy exposure.24,27 As enumerated in Table 7, Although studies are similar, reports have reached different conclusions, fluoroscopy time remaining the same,4 decreasing,23,24,27 or increasing.22 Fluoroscopy exposure time may vary depending on surgical technique or fracture types.
 |
Table 7 Mean Fluoroscopy Exposure Time or Times in Sec (Mean ± SD) |
Discussion
The traction table, lateral decubitus position, and traction repositor can be used to assist reduction and implant intramedullary nails for intertrochanteric hip fractures. Fixation of these fractures with intramedullary nails is generally considered to be best performed on a traction table The traction table has the advantages of a large axial traction force, which is conducive to correcting limb shortening and maintaining fracture reduction. However, it also has other shortcomings, such as the use of traction table during the treatment is inconvenient to readjust the reduction of fracture end during the operation. For obese patients, the operation must be ensured by enlarging the surgical incision, and some elderly and frail patients are difficult to tolerate lying on the traction table.31,32 Lateral decubitus position and traction repositor techniques can avoid these shortcomings, so it has attracted more and more attention.
Is nonuse of a traction table-assisted intramedullary nailing of intertrochanteric fractures as safe and effective as a traction table-assisted intramedullary nailing? Our study included eight papers published between 2016 and 2021 that evaluated the radiographic and clinical outcomes of 620 patients with intertrochanteric fractures. The major findings of this systematic review are as follows: 1) no significant differences in the reduction quality or the HHS were observed between the two groups; 2) nonuse of a traction table is advantageous in terms of setup time compared to the use of a traction table; and 3) in terms of surgical time, the amount of bleeding and fluoroscopy exposure time remain controversial.
Intertrochanteric fractures are especially common in elderly patients, and decreasing the setup time and surgical time is an important step in the surgical treatment of high-risk elderly patients. Prolonged anesthesia in elderly patients with additional comorbidities can contribute to increased mortality.33,34 We compiled the setup time data of all the studies. The results showed that the non-traction table group could significantly reduce the operation setup time compared with the traction table group. Setup time includes placing the patient on the traction table or surgical table, adjusting the patient’s position and sterile covering until the skin is incised. For patients treated with a traction table-assisted intramedullary nailing, the reduction phase and use of fluoroscopy during the reduction were included within the setup time, and the reduction of patients without a traction table-assisted treatment is completed during the operation.35 Therefore, theoretically, patients with a traction table-assisted intramedullary nailing always need more setup time for surgery, while patients without a traction table-assisted treatment will lose some surgical time due to the fracture reduction needs to be completed during surgery.4 However, this theory did not translate to surgical data, and we found Compared with the traction table group, the non-traction table group significantly reduced the operation preparation time, but did not prolong the operation time.
Additional fluoroscopic exposure can cause serious health problems for both the surgical team and the patient, and reducing fluoroscopic exposure time is a topic of concern for surgeons.36 Some studies reported the amount of fluoroscopy as time, and some studies reported it as “shoots”.4,22,23,27 It is difficult to interpret and comparison of the previous studies’ outcomes due to such a discrepancy One study showed that the duration of fluoroscopy exposure in the non-traction table group was prolonged because it was more difficult to achieve reduction and obtain lateral views without the use of a traction table.22 However, most studies have shown no difference between the two groups or that the non-traction table group had an advantage over the traction table group.4,23,24,27 It is worth noting that there is a strong correlation between the amount of fluoroscopy and the degree of comminution of the fracture, and fluoroscopy exposure time may vary depending on skill of the surgical team. In view of the above controversies, we believe that this issue deserves further study. In the operation of hip fractures in the elderly, the amount of bleeding is of great significance to the incidence of complications and mortality.37 We compiled the amount of bleeding data of all the studies and obtained encouraging results that showed that a traction table was not superior to a non-traction table in terms of the amount of bleeding.
High-quality reduction is critical for attaining the ideal position of the implant and achieving a good clinical outcome.8,38 For patients in the non-traction table group, the surgeon can adjust the reduction at each stage of the procedure, the quality of the reduction can be more precisely controlled. For the patients in the traction table group, the adjustment of the reduction was completed during the setup time at the beginning of the operation, and it was difficult to finely adjust the reduction during the operation, as the fine adjustment is made with a nonsterile device.21 All of the studies we included found no difference between the two groups in reduction quality, and the good and acceptable rates of the two groups were basically the same (the traction table group was 95.1% and the non-traction table group was 95.3%). Tip-apex distance (TAD) and cervicodiaphyseal angle (CDA) are widely accepted parameters used to evaluate whether the reduction and positioning of the cephalic element in both positioning methods were equivalent. TAD is the distance of subchondral bone in the central portion of the femoral head to the end of the cephalicpin of the nail, shorter than 25 mm are ideal.39 CDA values between 130◦ and 135◦were considered as normal.40 In the studies we included, a total of 4 articles reported these two parameter indicators. All studies concluded that there was no difference in TAD between the two groups. The CDA is still controversial (3 studies reported that the CDA of traction table group is significantly smaller than that of non-traction Table 1 study found no difference between the two groups.). In conclusion, the time spent to achieve better reduction may lead to a slightly longer surgical time and increased use of fluoroscopy, but better reduction also leads to better outcomes. The results of all the studies also showed that there was no significant difference in the HHS between the two groups, which fully showed that implanting intramedullary nails for a femoral intertrochanteric fracture without the assistance of a traction table did not affect postoperative rehabilitation. However, it is important to note that the different intramedullary nail designs might be a confounder while comparing different parameters as surgical time, fluoroscopy time and blood loss.
The available data support the effectiveness of the lateral decubitus position and traction repositor, which seems to be reproducible and safe when compared with conventional traction table techniques. Finally, the traction repositor is more cost-effective than the traction table, which makes it an ideal substitute for the traction table in primary hospitals.
Limitations
First, this review was limited by the clinical and methodological heterogeneity of included studies and inconsistent outcome reporting. Variability in baseline data, intervention data, and outcome data did not permit the quantitative synthesis of data into a meta-analysis. Second, the relatively few included studies ultimately made it difficult to provide a comprehensive and accurate review. Third, the complication rate is an important indicator in the evaluation of surgical efficacy. Unfortunately, we did not analyze complication rate. Duo to the limitations of included studies, we were not able to obtain data of complication rate. Fourth, our paper indicating that implantation without a traction table is safe and reliable was intended to provide clinicians with an overview; however, it does not provide exhaustive detail about any one surgical technique to guide administration or training in any specific surgical technique. Clinicians need to refer directly to the cited article and more widely in the published literature for this information.
Conclusion
Regarding proximal femoral intramedullary nailing for elderly intertrochanteric fractures, treatment without a traction table is equally as safe and reliable as treatment with a traction table, and it may be more advantageous in terms of setup time.
Abbreviations
HHS, Harris Hip Score; RCT, randomized controlled trial; TFN, trochanteric fixation nail; PFN, proximal femoral nail; PFNA, proximal femoral nail antirotation; MD, mean difference; CI, confidence interval.
Data Sharing Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Ethical Approval
The study was waived by the Ethics Committee of the Honghui Hospital, Xi’an Jiaotong University.
Consent
The work described has not been previously published; it is not under consideration for publication elsewhere; and its publication has been approved by all the co-authors.
Acknowledgments
Professor Bin-Fei Zhang and Ai-Yong Cui, Xi’an Jiaotong University Affiliated Honghui Hospital, provided important advice.
Funding
There is no funding to report.
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. Guzon-Illescas O, Perez Fernandez E, Crespi Villarias N, et al. Mortality after osteoporotic Hip fracture: incidence, trends, and associated factors. J Orthop Surg Res. 2019;14:203.
2. Uliana CS, Abagge M, Malafaia O, Kalil Filho FA, Cunha LAM. Fraturas transtrocantéricas – avaliac¸ã o dos dados da admissão à alta hospitalar. Rev Bras Ortop. 2014;49(2):121–128. doi:10.1016/j.rbo.2014.01.006
3. Kregor PJ, Obremskey WT, Kreder HJ, Swiontkowski MF. Unstable pertrochanteric femoral fractures. J Orthop Trauma. 2014;28(Suppl 8):S25–S28. doi:10.1097/BOT.0000000000000187
4. Şahin E, Songür M, Kalem M, et al. Traction table versus manual traction in the intramedullary nailing of unstable intertrochanteric fractures: a prospective randomized trial. Injury. 2016;47(7):1547–1554. doi:10.1016/j.injury.2016.04.012
5. Knobe M, Gradl G, Ladenburger A, Tarkin IS, Pape HC. Unstable intertrochanteric femur fractures: is there a consensus on definition and treatment in Germany? Clin Orthop Relat Res. 2013;471:2831–2840. doi:10.1007/s11999-013-2834-9
6. Roberts KC, Brox WT. AAOS Clinical Practice Guideline: management of Hip Fractures in the Elderly [published correction appears in J Am Acad Orthop Surg. 2015 Apr;23(4):266]. J Am Acad Orthop Surg. 2015;23(2):138–140. doi:10.5435/JAAOS-D-14-00433
7. Ertürk C, Ça˘gman B, Altay MA. The use of Ender nail in in- tertrochanteric fractures supported with external fixation. Ulus Travma Acil Cerrahi Derg. 2011;17(5):407–412. [PMID: 22090325]. doi:10.5505/tjtes.2011.48716
8. Ma HH, Chiang CC, Lin CC, Wang CS. The influence of proximal femur canal size on reduction of intertrochanteric fracture with cephalomedullary nail. Orthop Traumatol Surg Res. 2021;107(6):103006. doi:10.1016/j.otsr.2021.103006
9. Ahrengart L, Törnkvist H, Fornander P, et al. A randomized study of the compression Hip screw and Gamma nail in 426 fractures. Clin Orthop Relat Res. 2002;401:209–222. doi:10.1097/00003086-200208000-00024
10. Palm H, Krasheninnikoff M, Holck K, et al. A new algorithm for Hip fracture surgery. Reoperation rate reduced from 18 % to 12 % in 2000 consecutive patients followed for 1 year. Acta Orthop. 2012;83(1):26–30. doi:10.3109/17453674.2011.652887
11. Sadowski C, Lübbeke A, Saudan M, Riand N, Stern R, Hoffmeyer P. Treatment of reverse oblique and transverse intertrochanteric fractures with use of an intramedullary nail or a 95 degrees screw-plate: a prospective, randomized study. J Bone Joint Surg Am. 2002;84(3):372–381. doi:10.2106/00004623-200203000-00007
12. Swart E, Makhni EC, Macaulay W, Rosenwasser MP, Bozic KJ. Cost-effectiveness analysis of fixation options for intertrochanteric Hip fractures. J Bone Joint Surg Am. 2014;96(19):1612–1620. doi:10.2106/JBJS.M.00603
13. Stephen DJ, Kreder HJ, Schemitsch EH, Conlan LB, Wild L, McKee MD. Femoral intramedullary nailing: comparison of fracture-table and manual traction. a prospective, randomized study. J Bone Joint Surg Am. 2002;84(9):1514–1521. doi:10.2106/00004623-200209000-00002
14. Flierl MA, Stahel PF, Hak DJ, Morgan SJ, Smith WR. Traction table-related complications in orthopaedic surgery. J Am Acad Orthop Surg. 2010;18(11):668–675. doi:10.5435/00124635-201011000-00004
15. Chan PT, Schondorf R, Brock GB. Erectile dysfunction induced by orthopedic trauma managed with a fracture table: a case report and review of the literature. J Trauma. 1999;47(1):183–185. doi:10.1097/00005373-199907000-00040
16. Wiltfong RE, Taylor BC, Steensen RN. Lower extremity bypass graft occlusion after intramedullary fixation of intertrochanteric Hip fracture on a fracture table. Orthopedics. 2011;34(5):395. doi:10.3928/01477447-20110317-27
17. Callanan I, Choudhry V, Smith H. Perineal sloughing as a result of pressure necrosis from the traction post during prolonged bilateral femoral nailing. Injury. 1994;25(7):472. doi:10.1016/0020-1383(94
18. Aguirre-Rodríguez VH, Inzunza-Enríquez G, Bibiano-Escalante O, Martínez-Ruiz FJ, Valero-González FS. Osteosíntesis de cadera con clavo centromedular: posición en decúbito lateral, sin mesa de fracturas [Hip osteosynthesis with IM nail: lateral decubitus without fracture table]. Acta Ortop Mex. 2016;30(6):279–283.
19. Turgut A, Kalenderer Ö, Günaydın B, Önvural B, Karapınar L, Ağuş H. Fixation of intertrochanteric femur fractures using Proximal Femoral Nail Antirotation (PFNA) in the lateral decubitus position without a traction table. Acta Orthop Traumatol Turc. 2014;48(5):513–520. doi:10.3944/AOTT.2014.14.0098
20. Chen W, Zhang T, Wang J, Liu B, Hou Z, Zhang Y. Minimally invasive treatment of displaced femoral shaft fractures with a rapid reductor and intramedullary nail fixation. Int Orthop. 2016;40(1):167–172. doi:10.1007/s00264-015-2829-0
21. Souza EF, Hungria JO, Rezende LR, Bellan DG, Borracini JA. Comparative study between lateral decubitus and traction table for treatment of pertrochanteric fractures with cephalomedullary nails. Rev Bras Ortop. 2016;52(1):24–28. doi:10.1016/j.rboe.2016.04.009
22. Doğan N, Ertürk C, Gülabi D. Is proximal femoral nailing of unstable intertrochanteric fractures in the lateral decubitus position without a traction table as safe and effective as on a traction table? Injury. 2022;53(2):555–560. doi:10.1016/j.injury.2021.11.017
23. Sonmez MM, Camur S, Erturer E, Ugurlar M, Kara A, Ozturk I. Strategies for Proximal Femoral Nailing of Unstable Intertrochanteric Fractures: lateral Decubitus Position or Traction Table. J Am Acad Orthop Surg. 2017;25(3):e37–e44. doi:10.5435/JAAOS-D-15-00691
24. Li M, Chen J, Ma Y, Li Z, Qin J. Comparison of proximal femoral nail anti-rotation operation in traction bed supine position and non-traction bed lateral position in treatment of intertrochanteric fracture of femur. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020;34(1):32–36. doi:10.7507/1002-1892.201905076
25. Zhao K, Zhang J, Li J, et al. Treatment of Unstable Intertrochanteric Fractures with Proximal Femoral Nailing Antirotation: traction Table or Double Reverse Traction Repositor. J Invest Surg. 2021;34(11):1178–1184. doi:10.1080/08941939.2020.1786610
26. Yan M, Kuang L, Ni J, et al. Use of a Double Reverse Traction Repositor versus a Traction Table for the Treatment of Intertrochanteric Femur Fractures: a Comparative Study. Orthop Surg. 2021;13(4):1254–1261. doi:10.1111/os.12956
27. Du G, Wang Z, Yang S, et al. A comparative study on effectiveness of closed reduction and internal fixation of intertrochanteric fracture assisted with skeletal tractor and traction table. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020;34(4):469–474. doi:10.7507/1002-1892.201908120
28. Baumgaertner MR, Curtin SL, Lindskog DM. Intramedullary versus extramedullary fixation for the treatment of intertrochanteric Hip fractures. Clin Orthop Relat Res. 1998;348:87–94.
29. Schipper IB, Steyerberg EW, Castelein RM, et al. Treatment of unstable trochanteric fractures. Randomised comparison of the gamma nail and the proximal femoral nail. J Bone Joint Surg Br. 2004;86(1):86–94. doi:10.1302/0301-620X.86B1.14455
30. Lenich A, Vester H, Nerlich M, Mayr E, Stöckle U, Füchtmeier B. Clinical comparison of the second and third generation of intramedullary devices for trochanteric fractures of the Hip--Blade vs screw. Injury. 2010;41(12):1292–1296. doi:10.1016/j.injury.2010.07.499
31. Aguirre-Rodríguez VH, Inzunza-Enríquez G, Bibiano-Escalante O, Martínez-Ruiz FJ, Valero-González FS. Osteosíntesis de cadera con clavo centromedular: posición en decúbito lateral, sin mesa de fracturas [Hip osteosynthesis with IM nail: lateral decubitus without fracture table]. Acta Ortop Mex. 2016;30(6):279.
32. Turgut A, Kalenderer Ö, Günaydın B, Önvural B, Karapınar L, Ağuş H. Fixation of intertrochanteric femur fractures using Proximal Femoral Nail Antirotation (PFNA) in the lateral decubitus position without a traction table. Acta Orthop Traumatol Turc. 2014;48(5):513–520. doi:10.3944/AOTT.2014.14.0098
33. Jaffer AK, Barsoum WK, Krebs V, Hurbanek JG, Morra N, Brotman DJ. Duration of anesthesia and venous thromboembolism after Hip and knee arthroplasty. Mayo Clin Proc. 2005;80(6):732–738. doi:10.1016/S0025-6196(11)61526-7
34. Byrne AM, Morris S, McCarthy T, Quinlan W, O’byrne JM. Outcome following deep wound contamination in cemented arthroplasty. Int Orthop. 2007;31(1):27–31. doi:10.1007/s00264-006-0121-z
35. Xue L, Zha L, Chen Q, et al. Randomized controlled trials of proximal femoral nail antirotation in lateral decubitus and supine position on treatment of intertrochanteric fractures. ScientificWorldJournal. 2013;2013:276015. doi:10.1155/2013/276015
36. Gausden EB, Christ AB, Zeldin R, Lane JM, McCarthy MM. Tracking Cumulative Radiation Exposure in Orthopaedic Surgeons and Residents: what Dose Are We Getting? J Bone Joint Surg Am. 2017;99(15):1324–1329. doi:10.2106/JBJS.16.01557
37. Zhang JQ, Xue FS, Meng FM, Liu GP. Is basal haemoglobin level really a prognostic factor for early death of elderly patients undergoing Hip fracture surgery? Injury. 2015;46(10):2079–2080. doi:10.1016/j.injury.2015.05.012
38. Bilsel K, Erdil M, Gulabi D, Elmadag M, Cengiz O, Sen C. Factors affecting mortality after Hip fracture surgery: a retrospective analysis of 578 patients. Eur J Orthop Surg Traumatol. 2013;23(8):895–900. doi:10.1007/s00590-012-1104-y
39. Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the Hip. J Bone Joint Surg Am. 1995;77(7):1058–1064. doi:10.2106/00004623-199507000-00012
40. Giordano V, Dias MC, Santos GF, Cabral S, Amaral NP, Albuquerque RP. Estudo radiográfico da extremidade proximal do fêmur para avaliac¸ ão do risco de fratura osteoporótica. Rev Bras Ortop. 2007;42(4):88–96.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.