")
Back to Journals » Open Access Surgery » Volume 17
A 5-Year Retrospective Study of Gastrointestinal Atresia in a Tertiary Care Hospital in Mogadishu, Somalia
Authors Mohamed SS , Küçük A, Sheikh OA , SARAÇ A, Adam MK, Ibrahim IG , Osman MM , Ali NA, Mohamud AA
Received 3 January 2024
Accepted for publication 2 August 2024
Published 22 August 2024 Volume 2024:17 Pages 123—129
DOI https://doi.org/10.2147/OAS.S457913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Shukri Said Mohamed,1 Adem Küçük,2 Omar Adam Sheikh,3 Ahmet SARAÇ,4 Mesut Kayse Adam,1 Ismail Gedi Ibrahim,5 Marian Muse Osman,6 Naima Abukar Ali,7 Abdirahman Ahmed Mohamud8
1Department of Pediatric Surgery, Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 2Düzce Atatürk Devlet Hastanesi, Düzce, Turkey; 3Faculty of Medicine, Department of Basic Medical Science, Somali National University, Mogadishu, Somalia; 4Department of Pediatric Surgery, Samsun Training and Research Hospital, Samsung, Turkey; 5Department of Radiology, Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 6Department of Public Health, Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 7Department of Pediatric, Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 8Department of General Surgery, Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia
Correspondence: Shukri Said Mohamed, Email [email protected]
Background: Birth defects of the digestive system are a phenotypically and etiologically different category common birth defects caused by various causes during fetal development.
Objective: The study’s goal was to evaluate patient demographics, related abnormalities, atresia location, operational management, postoperative care, and results of patients with gastrointestinal atresia and compare them with other research.
Methods: A 5-year retrospective study in cases with gastrointestinal atresia at a tertiary hospital in Mogadishu, Somalia, was carried out by the pediatric surgery department from January 2017 to January 2022.
Results: A165 cases were operated due to gastrointestinal atresia in five-year period., 105 were male (63.6%) and 60 were female (36.4%), giving the male to female ratio of 1.75:1. According to the age group of the study population, the majority of cases (48.5%) were aged less than 1 month. The esophageal atresia, duodenal atresia, high jejunal atresia, jejunoileal atresia, and colon atresia, anorectal malformations were 9.7%, 9.1%, 0.6%, 7.3%, 73.3%, respectively; the anorectal malformations has resulted in the majority of cases (73.3%). 20 % of cases had no follow-up, while 80% arrived as planned. 52.1% got well and had no complications and some developed different complications like peristomal skin irritation (14%), rectal and urethral fistula (4.8%), rectal prolapse (1.8%), rectal stenosis (2.4%), rectal adhesions (1.2%), esophageal stricture (1.2%), wound infection (3.6%), anastomosis dehiscence (0.6%), abdominal distension (0.6%), recto-perineal fistula (1.2%), urethral damage and urinary retention (0.6%). Mortality for this study was 24.8% (41 patients).
Conclusion: Children with gastrointestinal atresia present late in the course of their illness, with substantial morbidity and death due to poor economic conditions, poor nutrition, surgical problems, and likely related anomalies, rather than surgical morbidity alone.
Keywords: birth defects, fetal development, digestive system, intestinal obstruction
Introduction
Gastrointestinal atresia is caused by a group of abnormalities that can occur anywhere in the digestive tract, from the esophagus to the colon. Prenatal imaging may be able to reveal the underlying cause in some cases. More often than not, the patient presents in an emergency situation and requires a combination of a detailed medical history and physical examination, along with correlative imaging, to provide an accurate diagnosis.1
The most common esophageal abnormality is esophageal atresia (EA), which is defined as a discontinuity with or without an aberrant connection between the esophagus and the trachea (tracheoesophageal fistula) (TEF).2 Small intestinal atresia (SIA) is a birth defect characterized by abnormal closure, discontinuity, or narrowing of the duodenum, jejunum, or ileum.3,4 When recanalization, which occurs at the end of the second month of the colon’s embryonic stage, fails, duodenal atresia develops. Vascular accidents that result in an obstruction of the blood supply to the small intestine induce atresia or stenosis of the jejunum or ileum (jejunoileal atresia, JIA).4 Intestinal atresia is favored by vomiting bile immediately after childbirth. Because the obstruction occurs beyond the opening of the Ampulla of Vater in the second half of the duodenum, the majority of cases of duodenal atresia result in bilious vomiting. Abdominal distension is nonexistent or minor in cases of duodenal atresia. On the other hand, in situations of jejunal and ileal atresia, it is a major feature.3 Anorectal malformations (ARMs) comprise a wide range of anomalies involving the anus and distal rectum, as well as the urogenital tract, and are most usually caused by aberrant anorectal septum development. The anus is frequently imperforated, and the distal bowel terminates either blindly or through a fistulous junction with the urogenital tract or the perineum.5
As we know of no previous research on this topic in Somalia, this study was designed to collect and analyse data from cases of gastrointestinal atresia or stenosis at any level from this institution, primarily to highlight the patterns and differences among the various gastrointestinal atresia.
Objectives
The goal of this study was to determine the demographic pattern of gastrointestinal atresia as well as related anomalies, atresia location, operational management, postoperative care, and patient outcomes in Somalia. Our management strategy was examined, and the results were compared to other studies in the literature.
Methods
The 5-year document of patients with gastrointestinal atresia (oesophageal atresia, duodenal atresia, high jejunal atresia, jejunoileal atresia, and colon atresia, anorectal malformations) had been managed at a Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital in Mogadishu, Somalia, Department of the Pediatric Surgery between January 2017 and January 2022, and was reviewed retrospectively. For those patients, we used cross-sectional studies and structured data were analysed. Age, gender, type of atresia, related anomalies, type of operation, post-operative problems, and follow-up were all recorded. Statistical analysis was performed on the available data. All patients admitted to the Pediatric Surgery Department and undergoing operations in the hospital were included in the study; those who were operated on in another hospital and then referred to our hospital were excluded. Also, there were 4 cases who died before the operation due to sepsis and aspiration, these cases were included from this study.
This study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of the Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital before the commencement of this study (05.07.2021; decision number 370, MSTH/6639). Informed consent was obtained from the patient’s parents during the hospitalisation and they signed the consent form.
Results
During the 5-year period, 165 cases with gastrointestinal atresia were operated. 105 were male (63.6%) and 60 were female (36.4%), giving the male to female ratio of 1.75/1. 80 cases (48.5%) were aged <1 month, 21 cases (12.1%) were aged between 1 &6 months, 41 cases (24.8%) were aged between 6 &12 months, and 23 cases (13.9%) were aged >1 year. According to the case counts, anorectal malformations was reported in 121 cases (73.3%), oesophageal atresia was reported in 16 cases (9.7%), duodenal atresia was reported in 15 cases (9.1%), jejunoileal atresia was reported in 12 cases (7.3%), and high jejunal atresia was reported in 1 case (0.6%:respectively Table 1).
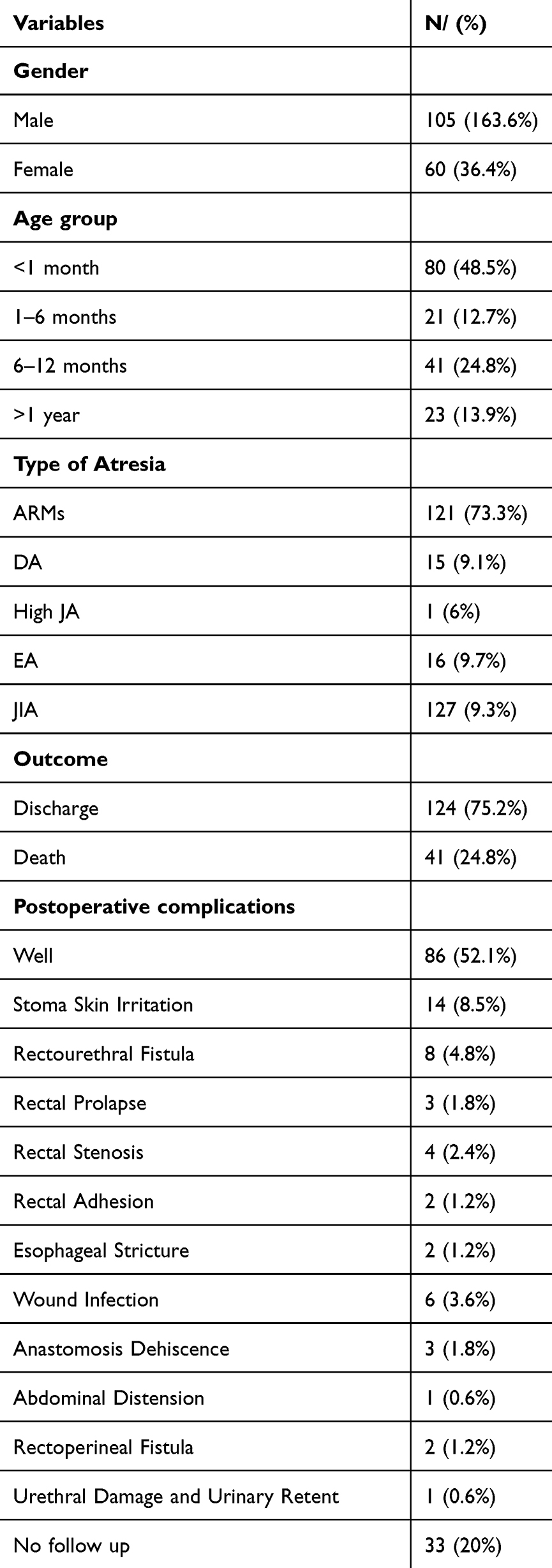 |
Table 1 This Table Shows the Demographic Features, Type of Atresia, Outcome and Postoperative Complication of Gastrointestinal Atresia |
The time age of presentation is different for every type of atresia. In <1 month, 42 cases of anorectal malformations, 11 cases of duodenal atresia, 11 cases of jejunoileal atresia, and 16 cases of oesophageal atresia were presented. Between 1 and 6 months, 16 cases of anal atresia, 3 cases of duodenal atresia, 1 case of high jejunal atresia, and 1 case of jejunoileal atresia were presented. Otherwise, 40 cases of anal atresia and 1 case of duodenal atresia were represented between 6 and 12 months. Only 23 cases of anorectal malformations came late, at the age of <1 year.
Approximately 89 cases of anorectal malformations had no associated anomalies, while 19 cases had a congenital heart defect diagnosed on echocardiogram and physical examination, and 6 cases had a renal anomaly. There are individual cases of anal atresia with associated individual anomalies like Down syndrome, microcephaly, limb anomaly, hypospadias, spina bifida, and absence of internal female organs. In contrast, one case of duodenal atresia and one case of high jejunal atresia had a congenital heart defect and a renal anomaly, respectively. Most of the oesophageal atresia (7 cases) had congenital heart disease.
Surgical records were reviewed for all patients with gastrointestinal atresia. Patients with anal atresia underwent different management procedures like divided sigmoid colostomies (47 cases), posterosagittal anorectoplasty (PSARP) (31 cases), anterosagittal anorectoplasty (ASARP) (25 cases), abdominoperineal pull-through (1 case), and colostomy closure (3 cases). On the other hand, duodenal atresia, ileal atresia, and oesophageal atresia were done with duodenoduodenostomy (15 cases), ileoileostomy (12 cases), and primary oesophageal anastomosis (12 cases) procedures, respectively. There are 4 cases who developed septicemia, aspiration, and those who died before the operation.
20% of cases had no follow up while 80% were coming on schedule within the five years after operation. 52.1% got well and had no complications, and others had different complications like peristomal skin irritation (14%), rectourethral fistula (4.8%), rectal prolapse (1.8%), rectal stenosis (2.4%), rectal adhesion (1.2%), oesophageal stricture (1.2%), wound infection (3.6%), anastomosis dehiscence (0.6%), abdominal distension (0.6%), rectoperineal fistula (1.2%), urethral damage and urinary retention (0.6%). The overall mortality rate for this series was 24.8% (41 patients). For anorectal malformations, 17.3% death were reported (21 patients). For duodenal atresia, 6 deaths were reported (40% of patients), compared to 4 deaths for jejunoileal atresia (33.3% of patients) and 56.2% of esophageal atresia (9 patients). In addition, one patient with high jejunal atresia died after the operation because of severe malnutrition due to short bowel syndrome.
Discussion
The most prevalent cause of intestinal obstruction is intestinal atresia. Mortality in high income countries (HICs) such as the Netherlands, United States, and Canada has dropped dramatically, from 35–50% to 4.6–11%.6,7 Poor outcomes and mortality rates as high as 28–50% have been reported in different series from Nigeria and Nepal in low- and middle-income countries (LMICs). Similarly, to our study, the mortality of gastrointestinal atresia during the study period is high at 24.8%.6 The improvement in survival of neonates with gastrointestinal system atresia is largely due to advances in surgical technique and, more crucially, prompt access to surgical services, the availability of intensive care, and the widespread use of parenteral nutrition.6
In the presence of chromosomal abnormalities, gastrointestinal problems develop more frequently than expected. Children with esophageal atresia/tracheoesophageal fistula have been found to have Trisomies 13, 18, and 21. These studies also have several related anomalies, such as cardiac anomaly, renal abnormality, and Trisomy 21. The patients with major anomalies had the highest mortality rate within the first year of birth. Individuals with isolated EA, on the other hand, had a better prognosis, with survival rates comparable to those reported in a smaller cohort of EA patients1,8 The significant decline in mortality rates for children with multiple anomalies is most likely due to advancements in surgical and anesthesiologic methods, particularly for cardiac problems, as well as recent advances in neonatal medical treatment. Live-born patients with accompanying abnormalities may have a greater mortality rate.9 In our study, 0.6% of our patients whose morphological findings were compatible with Down syndrome or other trisomies, genetic tests could not be performed. 75.2% of the 165 individuals with gastrointestinal atresia survived, but 16.3% of was death because they had severe congenital heart disease. Nearly to our study, male to female ratio of 1.75/1.
The most prevalent cause of neonatal intestinal obstruction was intestinal atresia. The ileum (43.2%), jejunum (31%), duodenum (20.9%), and colon (20.9%) are the most prevalent sites.9 In contrast to our study, anorectal malformations were the most prevalent site of atresia (73.3%), oesophageal atresia was (9.7%), duodenal atresia was 9.1%, jejunoileal atresia was (7.3%), and high jejunal atresia was 0.6%. In most cases, the diagnosis of gastrointestinal system atresia is made prenatally or immediately after birth, and surgical correction is required during the first few days of life. Despite the fact that the cause of EA is mostly unknown,2,4 postoperative children with severe jejunal atresia have a high incidence of sluggishness, peristalsis, early enteral feeding problems, and difficulty recovering intestinal function after the operation. Intestine plication is a procedure for reducing the circumference of the proximal bowel wall to a normal diameter by folding the antimesenteric section.7
Anorectal malformations (ARMs) comprise a wide range of anomalies involving the anus and distal rectum, as well as the urogenital tract, and are most usually caused by aberrant anorectal septum development. The anus is frequently imperforated, and the distal bowel terminates either blindly or through a fistulous junction with the urogenital tract or the perineum. Up to 70% of cases have associated birth defects, with the spine and urinary tract being most commonly affected. ARMs are now characterized based on the existence and position of fistulous connections, and gender can be used to distinguish between different types of arms. Surgical treatment includes a perineal approach to posterior sagittal anorectoplasty, first described by deVries and Pena.5 Furthermore, females with (80%) are more likely than males (33–40%) to have rectoperineal fistulas.10–12 Clinical signs alone can make it difficult to distinguish atresia from other causes of vomiting. Before surgery, GI radiography and endoscopy are the best ways to diagnose the obstruction.13,14 Abdominal distension, vomiting, dehydration, intestinal perforation, acute or subacute intestinal obstruction, sepsis, and respiratory distress are among the early complications, while megarectum, megacolon (requiring a decompressing colostomy), constipation, and failure to thrive are among the late complications, so it’s important to think about the implications for patients who are undergoing a multistaged procedure in ARMs. Although a colostomy prevents some complications, these patients require numerous procedures, each with its own set of risks.15,16 Stoma-related skin irritation is a common consequence. Peristomal skin irritation affects 3% to 42% of people, with symptoms ranging from mild dermatitis to full-thickness skin necrosis and ulceration.17 The delay in the onset of anorectal malformations are common, and it can lead to significant consequences.15,16 In the neonatal era, a single-stage method of repair has already been shown to be both safe and feasible in ARMs.10,18–20 We revealed that delayed re-pair is the most common occurrence among a group of institutions with colorectal specialist clinics. Rectoperineal and rectovestibular fistulas have generally positive short-term and long-term outcomes. The vast majority of our cases with rectovestibular fistulas (75%) were treated in a delayed fashion.
According to our postoperative complications are peristomal skin irritation (14%), rectourethral fistula (4.8%), rectal prolapse (1.8%), rectal stenosis (2.4%), rectal adhesion (1.2%), oesophageal stricture (1.2%), wound infection (3.6%), anastomosis dehiscence (0.6%), abdominal distension (0.6%), rectoperineal fistula (1.2%), urethral damage and urinary retention (0.6%).
Overall, compared to developed countries, there are challenges in the management of gastrointestinal atresia in Somalia. There are many resource-limited settings, insufficient specialized medical facilities, and the expertise required to diagnose and treat gastrointestinal atresias effectively. Access to pediatric surgeons and pediatric gastroenterologists, who are essential for managing such conditions, may be severely limited. Families in resource-limited settings may struggle to afford the costs associated with the diagnosis, treatment, and follow-up care of gastrointestinal atresias. This financial burden can lead to delays in seeking medical attention or incomplete treatment, which can adversely affect patient outcomes.
There were certain limitations to our research. To begin with, the database only covered a five-year span of birth registration (2017–2021), implying that our study used data from a relatively short period of time. Additionally, since this study’s infant data was not connected to maternal data, it was impossible to account for or control for confounding factors such as perinatal health.
Limitation
This article included a limited number of patients; asingle-center, retrospective study. Therefore, prospective research is recommended.
Conclusion
Despite advances in surgical management and care in HICs, this study represents one of the largest series of gastrointestinal atresia in an LMIC and reports a disproportionately high volume of diagnosed gastrointestinal atresia with persistently low survival, as in many LMICs. Unfortunately, the high mortality rate for children born with gastrointestinal atresia is most likely due to a lack of effective neonatal and prenatal care. To enhance outcomes, this study underscores the urgent need for improvements in neonatal care facilities, qualified workers, and resources. There has been no previous research in Somalia that we are aware of, so it is thought that this study will form the basis for future epidemiological investigations on gastrointestinal system disorders in our country.
Abbreviations
DA, duodenal atresia; JA, jejunal atresia; EA, esophageal atresia; JIA, jejunoileal atresia; ARMs, anorectal malformations; PSARP, posteriorsagittal anorectoplasty; ASARP, anterosagittal anorectoplasty; HICs, high-income countries; LMICs, low- and middle-income countries.
Acknowledgments
We would like to thank all the participants and Mogadishu Somali Turkey Education and Research Hospital for their valuable contributions to the study, also I would Thank to Professor Dr Ayşenur Celayir, MD for all contributions, corrections and critical reviews. The abstract of this paper was presented at the Ulusal Çocuk Cerrahisi Kongresi as a poster presentation/conference talk with interim findings. The poster’s abstract was published in ‘Poster Abstracts’ in Türkiye Çocuk Cerrahisi journal [https://m.bildirim.org/bld/cocukcer2022/7042].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lupo PJ, Isenburg JL, Salemi JL, et al. Population-based birth defects data in the United States, 2010–2014: A focus on gastrointestinal defects. Birth Defects Res. 2017;109(18):1504–1514. doi:10.1002/bdr2.1145
2. Nassar N, Leoncini E, Amar E, et al. Prevalence of esophageal atresia among 18 international birth defects surveillance programs. Birth Defects Res Part A, Clin Mol Teratol. 2012;94(11):893–899. doi:10.1002/bdra.23067
3. Maheshwari M, Tanwani R, Patel M, Joshi A, Jain R, Praneeth E. Intestinal Obstruction in Pediatric Age Group: a Clinico- Pathological Study. Ann Int Med Dent Res. 2016;2(6):28–30. doi:10.21276/aimdr.2016.2.6.sg8
4. Best KE, Tennant PW, Addor MC, et al. Epidemiology of small intestinal atresia in Europe: a register-based study. Arc Dis Childhood-Fetal and Neonatal. 2012;97:353–358. doi:10.1136/fetalneonatal-2011-300631
5. Stanescu AL, Liszewski MC, Lee EY, Phillips GS. Neonatal Gastrointestinal Emergencies: step-by-Step Approach. Radiol Clin North Am. 2017;55(4):717–739. doi:10.1016/j.rcl.2017.02.010
6. Cairo S, Kakembo N, Kisa P, et al. Disparity in access and outcomes for emergency neonatal surgery: intestinal atresia in Kampala, Uganda. Pediatr Surg Int. 2017;33(8):907–915. doi:10.1007/s00383-017-4120-5
7. Yang S, Wang M, Shen S. Bowel plication in neonatal high jejunal atresia. Medicine. 2019;98(19). doi:10.1097/MD.0000000000015459
8. Cassina M, Ruol M, Pertile R, et al. Prevalence, characteristics, and survival of children with esophageal atresia: a 32-year population-based study including 1,417,724 consecutive newborns. Birth Defects Res Part a - Clin Mol Teratol. 2016;106(7):542–548. doi:10.1002/bdra.23493
9. Vargas MG, Miguel-Sardaneta ML, Rosas-Téllez M, Pereira-Reyes D, Justo-Janeiro JM. Neonatal intestinal obstruction syndrome. Pediatr Annals. 2018;47(5):220–225. doi:10.3928/19382359-20180425-02
10. Kumar B, Kandpal DK, Sharma SB, Agrawal LD, Jhamariya VN. Single-stage repair of vestibular and perineal fistulae without colostomy. J Pediatr Surg. 2008;43(10):1848–1852. doi:10.1016/j.jpedsurg.2008.03.047
11. Cassina M, Leon FF, Ruol M, et al. Prevalence, and survival of patients with anorectal malformations: a population-based study. J Pediatr Surg. 2019;54(10):1998–2003. doi:10.1016/j.jpedsurg.2019.03.004
12. Jonker JE, Trzpis M, Broens PM. Underdiagnosis of mild congenital anorectal malformations. J Pediatr Surg. 2017;186:101–104. doi:10.1016/j.jpeds.2017.03.054.)
13. Chen HD, Jiang H, Kan A, et al. Intestinal obstruction due to dual gastrointestinal atresia in infants: diagnosis and management of 3 cases. BMC Gastroenterol. 2014;14(1):1–5. doi:10.1186/1471-230X-14-108
14. Gupta AK, Guglani B. Imaging of congenital anomalies of the gastrointestinal tract. Ind J Pediatr. 2005;72(5):403–414.
15. Divya G, Kundal VK, Debnath PR, et al. Delayed presentation of anorectal malformations in a tertiary care hospital in India. Pediatr Surg Int. 2021;37(4):451–456. doi:10.1007/s00383-020-04843-5
16. Tofft L, Salö M, Arnbjörnsson E, Stenström P. Wound dehiscence after posterior sagittal anorectoplasty in children with anorectal malformations. Bio Med Res Int. 2018;11.
17. Bafford AC, Irani JL. Management and complications of stomas. Surg Clin. 93(1):145–166. doi:10.1016/j.suc.2012.09.015
18. Marenco CW, Rice-Townsend S, Rollins M, et al. 30-day postoperative outcomes of neonatal versus delayed anoplasty for perineal and vestibular fistulas. J Pediatr Surg. 2021;56(8):1454–1458. doi:10.1016/j.jpedsurg.2021.04.023
19. Kuijper CF, Aronson DC. Anterior or posterior sagittal anorectoplasty without colostomy for low-type anorectal malformation: How to get a better outcome. J Pediatr Surg. 2010;45(7):1505–1508. doi:10.1016/j.jpedsurg.2010.02.042
20. Elrouby A, Waheeb S, Koraitim A. Anterior sagittal anorectoplasty as a technique for the repair of female anorectal malformations: a twenty-two-years-single-center experience. J Pediatr Surg. 2020;55(3):393–396. doi:10.1016/j.jpedsurg.2019.04.008
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.