")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
A Case of Squamous Cell Carcinoma Arising in Disseminated Superficial Porokeratosis
Authors Zheng HE , Wang Y , Wu S, Zhu MF
Received 16 February 2024
Accepted for publication 18 May 2024
Published 29 May 2024 Volume 2024:17 Pages 1259—1263
DOI https://doi.org/10.2147/CCID.S463569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jeffrey Weinberg
Hui-E Zheng, Yun Wang, Shuhui Wu, Ming-Fang Zhu
Department of Dermatology, The Second Affiliated Hospital of Hunan University of Chinese Medicine, Changsha, People’s Republic of China
Correspondence: Ming-Fang Zhu, Department of Dermatology, The Second Affiliated Hospital of Hunan University of Chinese Medicine, 233 Cai E North Road, Kaifu District, Changsha, People’s Republic of China, Tel +86-13907317358, Fax +86-731-84917727, Email [email protected]
Abstract: Porokeratosis (PK), characterized by keratotic lesions with an atrophic center and a prominent peripheral ridge, with a typical histological hallmark, namely, the cornoid lamella, has two forms: disseminated and localized. While PK often converts into squamous cell carcinoma (SCC), conversion from disseminated superficial porokeratosis (DSP) alone is rarely reported except for one case in which DSP and LP coexisted and converted to SCC. Here, we report the case of a patient with SCC converted from DSP alone, presenting with coin-sized macules on the bottom right of his waist that developed into an ulcer at the center. The patient underwent radiation therapy, which effectively treated the SCC but did not resolve the PK. This article highlights regular follow-up and undergo comprehensive diagnosis, both of which are beneficial to enable early detection and management of DSP that has converted to into SCC; in addition, standardized medical treatment may help improve the treatment therapeutic effect of in similar diseases.
Keywords: disseminated superficial porokeratosis, porokeratosis, squamous cell carcinoma
Introduction
Porokeratosis (PK) is a rare, genetically chronic progressive skin disease characterized by dike-like verrucous bulges at the edges, atrophy in the center, and histological manifestations involving cornoid lamella.1 PK can be classified as porokeratosis of Mibelli (PM), disseminated superficial actinic porokeratosis (DSAP), disseminated superficial porokeratosis (DSP), porokeratosis palmaris et plantaris disseminate (PPPD) and Linear Porokeratosis (LP), etc.2 Porokeratosis often develops into cancer: studies show that 6.9% to 30% of cases will develop into non-melanoma skin cancer (NMSC),3 including basal cell carcinoma, Merkel cell carcinoma and squamous cell carcinoma, with SCC having the highest risk ratio among the three types.4 According to reports, among the many clinical subtypes of PK, the top three canceration rates of SCC are for LP at 19%, PM at 7.6%, and DSAP at 3.4%.4 Compared with other subtypes of PK, there is currently only one reported case of the transformation of DSP into SCC, and it is due to coexistence with LP;5,6 in contrast, in DSP alone, canceration is rare, which may be related to DSP’s relatively rare incidence.7
In the present report, we describe the case of a 61-year-old male patient with a history of DSP of approximately 20 years and a relevant family medical history who was finally diagnosed with squamous cell carcinoma (SCC) under the premise of no coexistence of multiple PK variants and no history of prolonged sun exposure.
Case Report
A 61-year-old male presented with a 20-year history of multiple annular brown macule lesions surrounded by elevated borders all over the body. Twenty years ago, he had undergone total surgical resection at a local hospital, but the diagnosis was not available to us. Although the patient’s condition had improved following total surgical resection, the symptoms suddenly recurred and worsened, despite the absence of sun exposure, 10 years previously. During this period, he did not seek professional medical treatment until one year prior to presentation at our clinic, and was diagnosed with DSP at the time. Because the patient’s symptoms did not improve significantly after treatment with oral acitretin (20 mg/day) and topical vitamin E cream, the patient did not follow medical advice to continue regular treatment. Over the course of the next six months, the patient experienced gradual swelling, thickening, and plaque formation on a rash located on the bottom right of his waist. Subsequently, the area turned into an ulcer, which was accompanied by mild pain. The patient attempted self-treatment with topical medications; however, no significant improvement was observed. Consequently, the patient sought further treatment at our department. The patient denied history of any other chronic disease and sunburn, but admitted during consultation that his uncle had similar diseases.
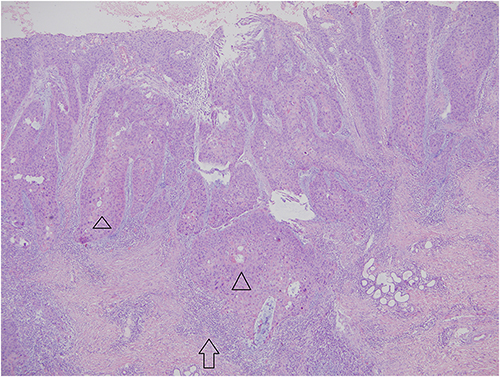
Dermatological examination revealed scattered brown macules with annular keratotic rims, varying from pin cap to broad bean. Some of these brown macules merged to form an annular configuration with raised edges resembling dikes, well-demarcated borders, and a slightly atrophic center. Coin-sized macules were observed at the bottom right of his waist, which developed into an ulcer at the center. The bottom of the ulcer was unevenly infiltrative and there were a few shallow erosions in the surrounding rash. The ulcer felt hard to the touch (Figure 1). Histological examination revealed that the brown macules exhibited hyperkeratosis with columnar parakeratosis (as indicated by the red arrow in the Figure 2). Dyskeratotic cells were observed in the epidermis beneath the parakeratosis column. Additionally, mild hyperplasia and hypertrophy of the spinous layer and slight lymphocyte infiltration in the superficial dermis were observed (Figure 2). Biopsy of the lesion within the plaque revealed irregular epidermal proliferation with obvious cell atypia which mainly comprised squamous cells (as shown by the black triangle in the Figure 3) with pathological karyokinesis (as indicated by the green arrow in the Figure 4). Biopsy of the dermis revealed infiltrative growth of cell clumps and inflammatory cell infiltration (as indicated by the black arrow in the Figure 3), and a new diagnosis of DSP and SCC was confirmed. Following radiotherapy, the patient ceased to experience SCC, but PK remained untreated.
 |
Figure 1 Clinical manifestations of the patient. There is a coin-sized macules at the bottom right of his waist, which developed into an ulcer at the center. The bottom of the ulcer was uneven and infiltrative, with a few shallow erosions in the surrounding rash. The ulcer was hard on touch. |




 |
Figure 4 Atypia of tumor cells with pathological karyokinesis is evident. (HE x 400). Pathological karyokinesis: |

Prior to the study, the patient provided written consent for examination and biopsy after being informed about the procedure.
Discussion
PK, which is characterized by keratotic lesions with an atrophic center and a prominent peripheral ridge with a typical histologic hallmark, namely, the cornoid lamella, may present as single or multiple lesions and can be divided into disseminated or localized forms.8,9 DSP, an extremely rare subtype of PK, can present with skin lesions in both sun-protected and sun-exposed sites, and occasionally in the oral mucosa and genitalia. It is associated with immunodeficiency and may develop sporadically during childhood.8
Studies have found that PK is more likely to develop into malignant lesions; this process is related to the following risk factors: larger limb lesions, long disease course, older age, sun exposure, and immunosuppression.1 Additionally, SCC rarely develops in unaffected skin— it typically arises in the presence of specific skin conditions and is influenced by factors such as patient age, disease duration, and history of sun exposure. To date, SCC secondary to DSP coexisting with other subtypes of porokeratosis has been confirmed, for example, Murata et al reported5 a Japanese patient with superficial disseminated porokeratosis. Obvious linear lesions were also observed on the left side of the DSP- affected area. Coincidentally, all the tumors developed linear lesions on the left side of the body. However, to our knowledge, SCC secondary to DSP alone is rare, and this report provides the first case. Unexpectedly, the ulcer of the case is located in a relatively hidden area, and the patient stressed that there was no history of prolonged sun exposure. Therefore, it is speculated that the patient’s age and the course of DSP may be important factors in the conversion of DSP to SCC. Furthermore, it is important to consider that both DSP and SCC have strong links to genetic factors.10 The patient also acknowledged a similar medical history in the family, suggesting that genetic factors may also play a role in the progression of DSP to SCC.
Currently, although there is no standardized treatment plan for porokeratosis due to a lack of randomized controlled trials, symptoms of PK can be improved through the following treatments, including 5-fluorouracil, imiquimod cream, topical or systemic retinoids, topical vitamin D derivatives, topical steroids, lasers, dermabrasion, and surgical intervention.1 Moreover, the disseminated form of PK requires regular follow-up to prevent cancer and enable early intervention. Although this case had a 20-year history of relevant skin lesions, he was not diagnosed with DSP until 1 year ago, reflecting the importance of early diagnosis of this disease. Dermoscopy is a non-invasive dermatological examination technology that can observe skin structures under the epidermis, dermis-epidermis junction, and upper dermis that are usually invisible to the naked eye, Das and his team pointed out that11 dermoscopy is one of the important diagnostic tools for PK, which can make the diagnosis of PK more clear. All of these prompt that the inclusion of more valuable diagnostic tool like dermoscopy during follow-up can help detect the transformation of PK into cancer in advance and promptly alert doctors to propose intervention plans.7
Once porokeratosis becomes cancerous, surgical resection, radiotherapy, chemotherapy, and other methods are usually adopted. Surgical excision or destruction is generally recommended after localized skin lesions become malignant.5,12 After surgery, it is necessary to pay attention to local moisturizing skin care or sun protection. After cancer developed in this case, the patient first chose to self-medicated before sought professional medical help. Finally, the patient ceased to experience SCC, although PK remained untreated. This may be a consequence of the patient’s self-medication, which caused the best opportunity for surgery of the ulcer to be missed, radiotherapy as an option.
In summary, this study highlights that individuals susceptible to DSP with a family history should ensure that they attend regular follow-up and undergo comprehensive diagnosis, both of which enable early detection and management of DSP that has converted into SCC. In addition, standardized medical treatment may help improve the therapeutic effect in similar diseases.
Ethics Statement
Publications of the images were included after obtaining the patients’ consent.
Consent Statement
Informed consent was obtained from the patient for publication of this case. Institutional approval was not required to publish the case details.
Funding
This study was funded by the National Natural Science Foundation of China (grant number 82174375).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Aitkens L, Byrne J, Jennings-Dover C, Potter KA. A case of squamous cell carcinoma arising in a giant porokeratosis previously diagnosed as psoriasis. Dermatol Reports. 2023;15(2):9634. doi:10.4081/dr.2023.9634
2. Zhang F, Bai W, Sun S, Li N, Zhang X. Squamous cell carcinoma arising from giant porokeratosis and rare postoperative recurrence and metastasis: a case report. Medicine. 2020;99(2):e18697. doi:10.1097/MD.0000000000018697
3. Ahmed A, Hivnor C. A case of genital porokeratosis and review of literature. Indian J Dermatol. 2015;60(2):217. doi:10.4103/0019-5154.152587
4. Inci R, Zagoras T, Kantere D, et al. Porokeratosis is one of the most common genodermatoses and is associated with an increased risk of keratinocyte cancer and melanoma. J Eur Acad Dermatol Venereol. 2023;37(2):420–427. doi:10.1111/jdv.18587
5. Abbott-Frey AM, Coromilas AJ, Niedt GW, Lewin JM. Recurrent squamous cell carcinoma arising within a linear porokeratosis. J Drugs Dermatol. 2020;19(2):205–206. doi:10.36849/JDD.2020.4640
6. Murata Y, Kumano K, Takai T. Type 2 segmental manifestation of disseminated superficial porokeratosis showing a systematized pattern of involvement and pronounced cancer proneness. Eur J Dermatol. 2001;11(3):191–194.
7. Vargas-Mora P, Morgado-Carrasco D, Fustà-Novell X. Porokeratosis: a review of its pathophysiology, clinical manifestations, diagnosis, and treatment. Actas Dermosifiliogr. 2020. 111(7):545–560. English, Spanish. PMID: 32401728. doi:10.1016/j.ad.2020.03.005
8. Ramakrishnan R, Vignesh TA, Durai P, Narasimhan M. A rare case of disseminated superficial porokeratosis-Case report. J Family Med Prim Care. 2022;11(3):1195–1197. doi:10.4103/jfmpc.jfmpc_1232_21
9. Cannavó SP, Borgia F, Adamo B, Guarneri B. Simultaneous development and parallel course of disseminated superficial porokeratosis and ovarian cancer: coincidental association or true paraneoplastic syndrome. J Am Acad Dermatol. 2008;58(4):657–660. doi:10.1016/j.jaad.2007.12.030
10. Zambrano-Román M, Padilla-Gutiérrez JR, Valle Y, et al. PTCH1 Gene Variants, mRNA expression, and bioinformatics insights in Mexican cutaneous squamous cell carcinoma patients. Biology. 2024;13(3):191. doi:10.3390/biology13030191
11. Das A, Vasudevan B, Talwar A. Porokeratosis: an enigma beginning to unravel. Indian J Dermatol Venereol Leprol. 2022;88(3):291–299. doi:10.25259/IJDVL_806_20
12. Lee HR, Han TY, Son SJ, Lee JH. Squamous cell carcinoma developing within lesions of disseminated superficial actinic porokeratosis. Ann Dermatol. 2011;23(4):536–538. doi:10.5021/ad.2011.23.4.536
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.