")
Back to Journals » Infection and Drug Resistance » Volume 17
Alterations of Gut Microbiota in Pyogenic Liver Abscess Patients with and without Type 2 Diabetes Mellitus
Authors Liu S, Ge X, Xu X, Zhang K, Lu X
Received 23 December 2023
Accepted for publication 8 May 2024
Published 29 May 2024 Volume 2024:17 Pages 2149—2158
DOI https://doi.org/10.2147/IDR.S456423
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Sandip Patil
Shanshan Liu,1,2 Xiaomeng Ge,3 Xizhan Xu,4 Kang Zhang,1 Xinxin Lu1
1Department of Laboratory Medicine, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Infection Management, The Affiliated Lianyungang Hospital of Xuzhou Medical University, The First People’s Hospital of Lianyungang, Jiangsu, People’s Republic of China; 3Microbial Resources and Big Data Center, Institute of Microbiology, Chinese Academy of Sciences, Beijing, People’s Republic of China; 4Beijing Institute of Ophthalmology, Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Xinxin Lu, Department of Laboratory Medicine, Beijing Tongren Hospital, Capital Medical University, No. 1, Dongjiaomin Lane, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86-13911682566, Fax +8610-65125617, Email [email protected]
Purpose: The clinical manifestations of pyogenic liver abscess (PLA) vary between patients with and without diabetes mellitus (DM). However, the relationship between PLA and the gut microbiome remains unknown. This study analyzed the composition of gut microbiota in PLA patients with and without DM and healthy controls (HCs) with the goal of identifying potential reasons for the observed variations in clinical manifestations.
Patients and Methods: Using 16S ribosomal RNA(16S rRNA) gene sequencing, we analyzed the compositions of gut microbiota in 32 PLA patients with DM, 32 PLA patients without DM, and 29 matched HCs.
Results: In PLA patients with DM, the D-dimer level, fibrinogen degradation products, and thrombin time were significantly higher compared to the PLA patients without DM (P < 0.05). The abundance and diversity of intestinal flora were reduced in both groups of PLA patients compared with the HCs (P < 0.05). Specifically, the PLA patients with DM showed significant decreases in the relative abundances of Bacteroides, Blautia, Prevotella9, and Faecalibacterium, whereas Enterococcus and Escherichia-Shigella were relatively more abundant (P < 0.05). Compared to PLA patients without DM, those with DM had lower relative abundances of Lactobacillus and Klebsiella (P < 0.05) and showed different bacterial flora, including Anaerosporobacter and Megamonas.
Conclusion: PLA patients with DM exhibited more severe clinical manifestations of PLA compared to patients without DM. It is important to monitor blood coagulation in PLA patients with DM to prevent the development of thrombotic diseases. Additionally, PLA patients with DM exhibit distinct differences in the composition and diversity of their intestinal flora compared to both PLA patients without DM and HCs.
Keywords: Gut microbiota, Pyogenic liver abscess, type 2 diabetes mellitus, 16S rRNA sequencing
Introduction
Pyogenic liver abscess (PLA) is an infectious disease caused by pyogenic bacteria that invade the liver through various routes and form solitary or multiple collections of pus within the liver.1,2 In recent years, there has been a noticeable rise in the incidence rate of PLA in adults in China and Korea.3–5 The incidence of liver abscesses is also on the rise among children in the United States.6 Patients with PLA do not typically present with specific symptoms. However, if the infection is not effectively managed, it can progress to disseminated infection, sepsis, and potentially death, especially in individuals with type 2 diabetes mellitus (T2DM).5,7,8 PLA patients with DM tend to experience more severe symptoms compared to PLA patients without DM.9,10 Over 140 million Chinese adults were estimated to have diabetes in 2021, and this number is projected to increase to over 174 million by 2045.11 Therefore, effective strategies for PLA prevention and treatment are urgently needed.
The gut microbiota plays a significant role in host metabolism, protection against microbial invasion, and nutrient absorption, thereby exerting a profound effect on human health and disease.12,13 Gut microbiota dysbiosis can be linked to the pathogeneses of chronic liver diseases such as chronic hepatitis B and C, liver cirrhosis, and hepatocellular carcinoma.14–16 Alterations in the diversity of the gut microbiota have been observed in animal models of liver abscess.17–19 Changes in the composition of pus (pus collection were as described in a previous study) microbiota are associated with the development of PLA in patients with DM.20,21 In addition, there are variations in the gut microbiota among individuals from different geographic regions.22 Hence, we hypothesized that the PLA patients with and without DM show differences in the composition of the gut microbiome. In this study, we analyzed the differences in clinical characteristics between the T2DM+PLA group and the PLA group. Additionally, we utilized 16S rRNA amplicon sequencing to analyze the gut microbiota of PLA patients with DM, PLA patients without DM, and healthy controls (HCs) to better understand the role of gut microbiota in the occurrence of PLA. The ultimate goal is to prevent hospitalization, reduce financial burden, and avoid potential life-threatening complications.
Material and Methods
Study Population
The study was approved by the Medical Ethics Committee of The First People’s Hospital of Lianyungang (number KY-20181213001), and all participants provided informed consent.
The diagnostic criteria for PLA included the following: 1) clinical manifestations such as fever, chills, nausea, discomfort in the liver area, fatigue, and tenderness or percussion pain in the liver area; 2) confirmation of liver abscess through imaging examinations such as abdominal Doppler ultrasound, CT, or MRI; 3) positive results from clinical bacteriological examination or effective antimicrobial drug treatment; and 4) confirmation of purulent infection caused by bacteria through percutaneous liver puncture or surgical treatment. To be considered for inclusion, participants had to meet criteria 1 and 2 as well as any one or both of criteria 3 and 4. Diabetes was diagnosed according to the American Diabetes Association criteria.23
A cohort of 93 subjects, including 32 PLA patients with DM (T2DM+PLA group) patients, 32 PLA patients without DM (PLA group), and 29 age- and sex-matched HCs (Health Control group), were recruited from The First People’s Hospital of Lianyungang in Jiangsu Province, China, between February 2021 and January 2022.
Patient data, including basic demographic information, clinical manifestations, underlying diseases, laboratory test results, and imaging examination results, were obtained from medical records, laboratory information systems, and the Picture Achieving and Communication System at our institution.
Sample Collection and DNA Extraction
Fecal samples were freshly collected from both the PLA groups and the HC group for the analysis of intestinal flora. The samples were processed in the laboratory within 4 h after collection and then stored at −80°C until analysis. DNA was extracted from fecal samples (0.5 g) using the QIAamp PowerFecal DNA kit (QIAGEN, Germany) according to the manufacturer’s protocols.
Polymerase Chain Reaction (PCR) and 16S rRNA Amplicon Sequencing
The V3-4 region of the bacterial 16S rRNA gene was amplified by PCR (95°C for 3 min followed by 25 cycles at 95°C for 30s, 55°C for 30s, and 72°C for 30s and a final extension at 72°C for 5 min) using the primers 341F 5′-CCTACGGGNBGCASCAG-3′ and 805R 5′-GACTACNVGGGTATCTAATCC-3′. PCR cleanup was conducted using AMPure XP beads to purify the 16S V3 and V4 amplicon away from the free primers and primer dimer species. The purified product was amplified by PCR (95°C for 3 min followed by eight cycles at 95°C for 30s, 55°C for 30s, and 72°C for 30s and a final extension at 72°C for 5 min) using primers where barcode is an eight-base sequence unique to each sample. The amplicons were subsequently purified by AMPure XP beads to clean up the final library before quantification. Finally, the purified amplicons were pooled in equimolar amounts and paired-end sequenced (2×250) on an Illumina MiSeq platform according to the standard protocols.
Bioinformatics Analysis
Fast Length Adjustment of Short reads (FLASH) was used to merge paired-end reads from next-generation sequencing. Low-quality reads were filtered, and chimera reads were removed. The number of reads for each sample was normalized by random subtraction based on the smallest sample size. Operational taxonomic units (OTUs) were aligned using the UCLUST algorithm with a 97% identity and taxonomically classified using the SILVA 16S rRNA database (v128). The alpha and beta diversities were generated using Quantitative Insights Into Microbial Ecology (QIIME) and calculated based on weighted and unweighted UniFrac distance matrices. We used linear discriminant analysis effect size (LEfSe) method to identify species with statistically significant differences in abundance among the groups.
Statistical Analysis
Normal measurement data were presented as mean ± standard deviation, and statistical comparisons were conducted using the independent t-test. Non-normally distribution data were represented by M (P25, P75), and comparisons were performed using the Mann–Whitney U-test. Statistical analysis and graphing were performed using SPSS 27.0 and GraphPad Prism9 software. A P-value less than 0.05 was considered statistically significant.
Results
Patient Clinical Characteristics
This study included 32 patients each in the T2DM+PLA group and the PLA group. Detailed characteristics of the patients are given in Table 1. The average age of the patients was 56.2 years, and the patients included 43 males (63.19%) and 21 females (32.81%). There were no significant differences in age, gender, or symptoms and signs between these two groups. The rate of hypertension was significantly higher in the T2DM+PLA group (χ2 = 4.267, P = 0.039), while the rate of previous hepatobiliary surgery was significantly higher in patients with PLA (χ2 = 0.7819, P = 0.005). Significant differences were observed in the D-dimer level, content of fibrinogen degradation products (FDP), and thrombin time (TT) between the T2DM+PLA group and the PLA group whereas no significant differences were found in the contents of PCT, C-reactive protein, and alkaline phosphatase, which showed significant increases in the two PLA groups. In terms of treatment, most patients with T2DM+PLA received antibiotics and underwent percutaneous drainage (χ2 = 6.335, P = 0.012). Regarding prognosis, patients with T2DM+PLA experienced a longer duration of hospitalization and drainage tube placement time than patients with PLA (P < 0.05).
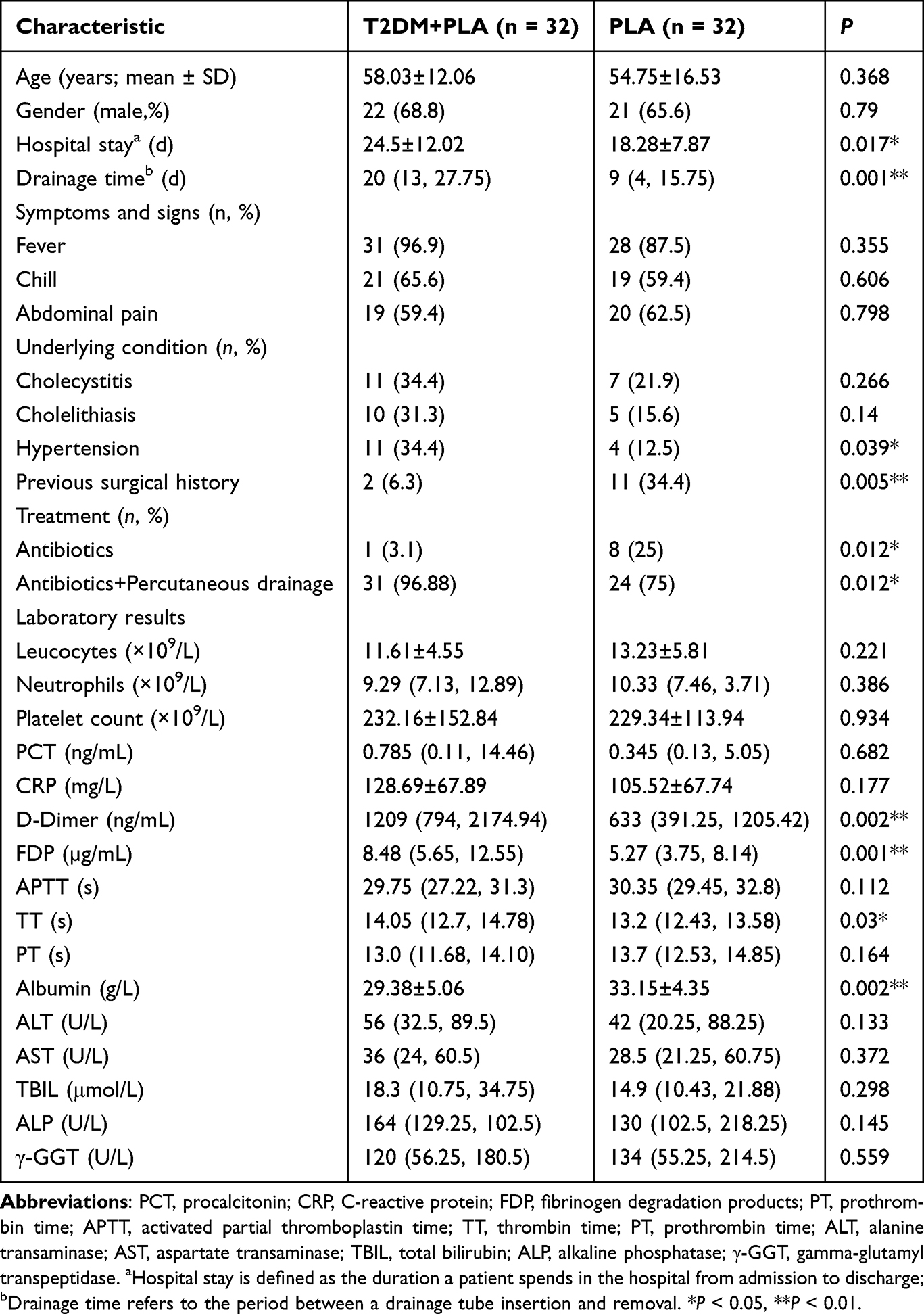 |
Table 1 Clinical Characteristics and Laboratory Results of the Study Population |
PLA Decreases Microbial Diversity Both with and without DM
The characteristics of the gut microbiome in the three groups were analyzed based on the 16S rRNA gene sequencing of 93 fecal samples. The α-diversity reflects the abundance and diversity of gut microbes. The gut microbial richness was determined based on the number of observed species, and the Chao1 diversity index and gut microbial diversity were measured by the Shannon and Simpson diversity indexes. The richness and diversity of gut microbiota were significantly lower in the T2DM+PLA and PLA groups than in the HCs (P < 0.01; Figures 1A–D). When comparing to the PLA group, there was a decrease in both the richness and diversity of the gut microbiome in T2DM+PLA group. However, the differences were not significant. The β-diversity reflects the composition of gut microbiota. Principal coordinate analysis of the weighted UniFrac distance indicated a non-significant difference in fecal microbiota between the T2DM+PLA and PLA groups. Compared with the PLA group, the fecal microbiota of the T2DM+PLA was more different from the HC group (ANOSIM, P < 0.01; Figure 1E). The gut microbiota of the PLA group showed considerable dispersion, indicating significant variations in the composition of the gut microbiota among individuals (Figure 1E).
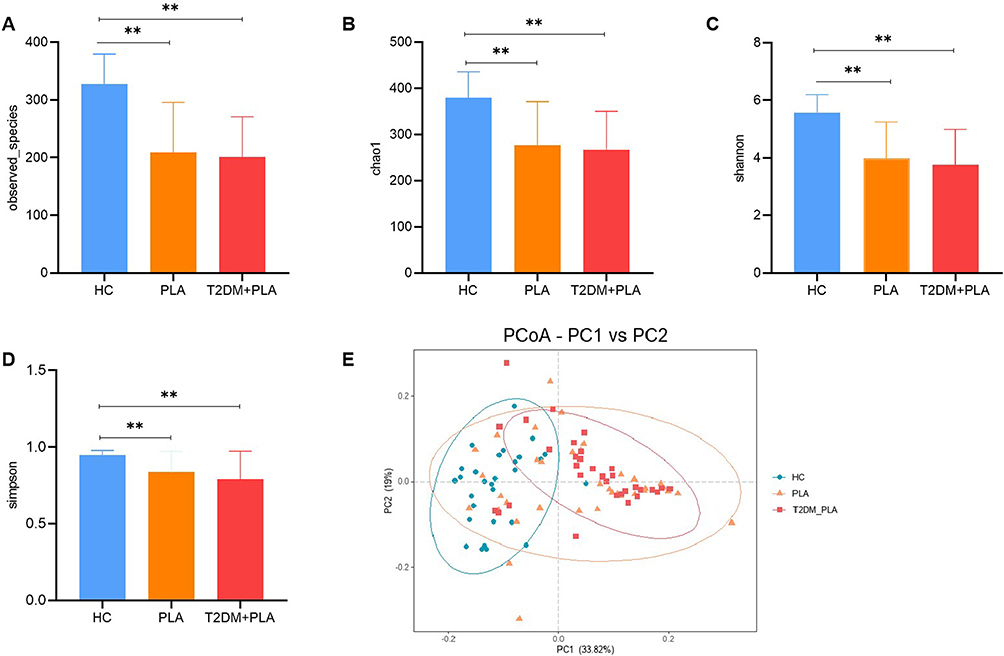 |
Figure 1 Differences in fecal microbial diversity and community structures in patients with T2DM+PLA (n = 32), patients with PLA (n = 32), and HCs (n = 29). (A) Observed species; (B) Chao1 diversity index; (C) Simpson diversity index; (D) Shannon diversity index; and (E) β-diversity assessed by principal coordinate analysis of the weighted UniFrac distance. The horizontal and vertical axes in (E) represent the first and second principal coordinates in the principal coordinate analysis. **P < 0.01. |
The Bacteria Differ Among the Three Groups
We assessed the differences in the relative abundances of bacteria at the phylum and genus levels among the three groups. At the phylum level, the relative abundance of Bacteroidetes, which contains many beneficial commensal organisms, was lower in the T2DM+PLA and PLA groups compared with the HCs. Conversely, the relative abundance of Proteobacteria was significantly higher in the T2DM+PLA and PLA groups (P < 0.05). When comparing the T2DM+PLA group with the PLA group, the relative abundance of Bacteroidetes decreased in the T2DM+PLA group, but this difference was not significant (Figures 2A and 2C, P=0.11, Z=1.60). At the genus level, the relative abundances of Blautia and Prevotella9 were significantly decreased in the two PLA groups compared with the HCs (P < 0.05). Conversely, the relative abundances of Enterococcus and Escherichia-Shigella were significantly higher in the two PLA groups compared with the HCs (P < 0.05). The relative abundances of Bacteroides and Faecalibacterium were significantly decreased in the T2DM+PLA group compared with the HCs (P < 0.05). Similarly, compared with the PLA group, the relative abundances of Lactobacillus and Klebsiella were significantly reduced in the T2DM+PLA group (Figure 2B and Table 2).
 |
Table 2 Comparison of the Relative Abundances of Gut Microbiota at the Genus Level Among the Three Groups |
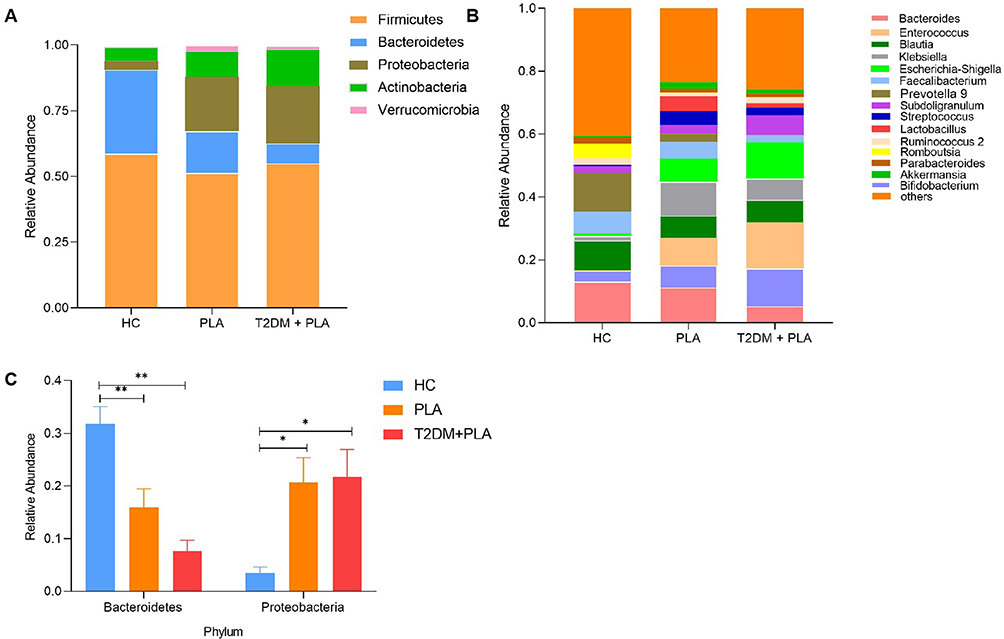 |
Figure 2 The major gut bacterial phyla and genera in the three groups. (A) Bacterial phylum level among three groups. (B) Bacterial genus level among three groups. (C) Comparison of the relative abundances of gut microbiota at the phylum level. The P-values were calculated by Mann–Whitney U-test. *P < 0.05, **P < 0.01. |
Differences in Fecal Microbiota Among the Groups
To identify differences in key biomarkers among the groups, we conducted LEfSe analysis to characterize differences in species among the groups. A total of 77 genera showed significant differences between the HC group and the PLA group. Out of these, 60 genera were found in the HC group, and 17 genera were found in the PLA group (Figures 3A and B). Eighty-four genera displayed significant differences between the HC group and the T2DM+PLA group, with 63 genera in the HC group and 21 genera in the T2DM+PLA group (Figures 3C and D). When comparing the two PLA groups, significant differences were observed in 9 genera. In the PLA group, the gut microbiome was dominated by Lactobacillus, LachnospiraceaeNC2004group, Eubacterium_eligensgroup, Lachnospira, Eisenbergiella, Coprococcus2, and Romboutsia; in contrast, in the T2DM+PLA group, the microbiome was dominated by the Anaerosporobacter and Megamonas (Figures 3E and F).
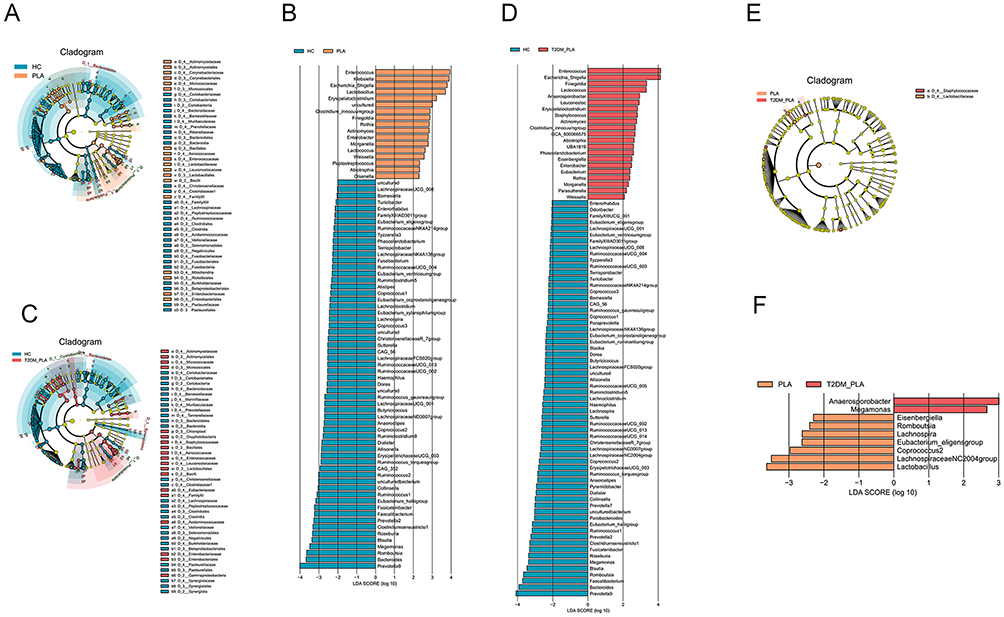 |
Figure 3 Relative abundances of different species in the three groups identified by LEfSe analysis. The length of the column represents the influence of significantly different species in relative abundance (linear discriminant analysis score > 2). The significantly different species are shown in the cladogram. Each circle represents phylogenetic level from the phylum to genus moving from inside to outside. The diameter of each circle is proportional to the taxon abundance, The PLA, T2DM+PLA, and HC groups are indicated in Orange, red, and blue, respectively. (A and B) PLA and HC; (C and D) T2DM+PLA and HC; and (E and F) PLA and T2DM+PLA. |
Discussion
We detected inflammatory mediators, liver function indices, and coagulation indicators in this study. In the present study, PLA patients with DM had longer hospital stays and drainage times compared with PLA patients without DM, consistent with previous findings.20 In the present study, PLA patients with DM had notably elevated levels of D-dimer and FDP compared with PLA patients without DM.Lee et al reported that PLA patients with DM caused by Klebsiella pneumoniae displayed platelet hyperreactivity.24 Furthermore, individuals with liver abscess were found to be susceptible to hepatic venous thrombophlebitis,25 which can lead to cerebral venous thrombosis26 and pulmonary embolism.27 The resolution of venous thrombosis is closely linked to the resolution of PLA.28 The mechanism by which DM contributes to higher blood coagulation indexes in PLA patients requires further study. Both the present study and past findings highlight the importance of monitoring the coagulation status of PLA patients and implementing timely intervention measures to prevent the development of thrombotic diseases.
In this study, we identified specific signatures of the fecal microbiota in PLA patients with DM, PLA patients without DM, and matched HCs. We found significant differences in the microbiota composition along with decreases in both the diversity and abundance of gut microbiota in PLA patients compared to the HCs. These findings are consistent with previous studies demonstrated decreases in gut microbiota diversity in animal models of liver abscess17,19 and lower microbial diversity in Hepatitis C Virus(HCV) patients compared to HCs.29 Based on these findings, we speculate that the richness and diversity of the gut microbiome play a role in the pathogenesis of patients with PLA. However, further studies are needed to investigate the specific mechanisms involved.
The gut microbial composition was examined at different phylogenetic levels. At the phylum level, Proteobacteria were more abundant than Bacteroidetes in both PLA groups compared with the HCs. At the genus level, the relative abundances of the Blautia and Prevotella9 genera were lower in the PLA groups than in the HC group. These genera are responsible for producing short-chain fatty acids and participating in immune response by regulating phagocytosis and chemokines.30,31 Patients with liver cirrhosis have lower levels of Bacteroidetes and higher levels of Proteobacteria compared to healthy people.15,32 The abundance of the Prevotella genus was also reduced in patients with severe fever associated with thrombocytopenia syndrome.33 Wang et al found that the level of Prevotella was the same in patients with non-alcoholic fatty liver disease as in healthy individuals.34 Thus, the alterations in gut microbiota associated with different diseases have unique characteristics. In the present study, we observed an increase in the abundance of Enterococcus and Escherichia-Shigella in the PLA patients compared with the HCs. The presence of Escherichia-Shigella could potentially impair hepatic lipid metabolism, produce lipopolysaccharides, and contribute to liver injury related to intra-abdominal hypertension.35,36 Differences in gut microbial may be one reason why PLA patients with DM have more serious clinical manifestations than those without DM.
The abundances of the genera Lactobacillus and Klebsiella were decreased in the T2DM+PLA group compared with PLA group. The microbiota in T2DM patients is primarily characterized by a reduction in Roseburia intestinalis and Faecalibacterium prausnitzii along with moderate dysbiosis, a proinflammatory environment, and increased intestinal permeability.37 The interaction between the changes in bacterial flora in T2DM and PLA requires further study. The pathogenic bacterium Klebsiella pneumoniae is commonly found in PLA patients with DM.10,38 Zhang et al demonstrated that Klebsiella pneumoniae liver abscesses are mixed abscesses infected by Klebsiella pneumoniae along with other bacteria.39 Guo et al reported that the relative abundance of Klebsiella in the pus cavity of PLA patients with DM was higher than that in PLA patients without DM.20 This might reflect an increase in the relative abundance of Klebsiella pneumoniae within the Klebsiella genus; alternatively, bacterial interactions might lead to the enhanced virulence of Klebsiella pneumoniae. In an animal model, Klebsiella pneumoniae strains were able to cross the intestinal barrier and pass through the portal vein to the liver.40 Therefore, it is possible that the gut microbial imbalance damaged the intestinal barrier and increased intestinal permeability. As a result, pathogens entered the portal vein and liver, leading to a decrease in Klebsiella. Interestingly, changes in the composition of the intestinal flora have been shown to significantly affect the levels of metabolites in the host.41,42 To understand the underlying mechanism, further investigation using targeted metabolomics is necessary.
Several different probiotic strains, particularly those belonging to Lactobacillus and Bifidobacterium, have been shown to improve parameters related to T2DM.37 Future studies could explore the potential of beneficial bacteria to prevent or delay the progression of PLA in patients with DM through precision medicine. This study identified relevant biomarkers of these diseases, which may play a role in the diagnosis of these diseases.
This study has some limitations. First, it was a single-center study with a limited sample size, and the results are preliminary. Further research is needed to validate the findings in a more diverse population. Second, additional investigation is required to identify the specific mechanisms that connect PLA with changes in the gut microbiota.
Conclusion
In summary, we found that PLA patients with DM exhibited more severe clinical symptoms than those without DM. We also observed significant alterations in the gut microbiota of PLA patients with DM compared with both PLA patients without DM and the HCs. Compared with the HCs, the intestinal microbiomes of PLA patients with DM showed reduced diversity and noticeable changes in composition. These findings establish a theoretical basis for the prevention and treatment of PLA.
Data Sharing Statement
The datasets utilized and/or analyzed during the present study can be obtained from the corresponding author.
Ethics Approval
The research followed the principles of the Declaration of Helsinki. The Ethics Committee of The First People’s Hospital of Lianyungang granted approval for this study. The patients/participants provided written informed consent to participate in this study.
Acknowledgments
We express our gratitude to the enrolled patients for their cooperation in our study and acknowledge the professionalism and compassion displayed by all the workers involved in the study. Additionally, we would like to extend our thanks to the State Key Laboratory of Microbial Resources, Institute of Microbiology for providing assistance with the 16S rRNA analysis of samples and data analysis. The authors thank AiMi Academic Services (www.aimieditor.com) for English language editing and review services.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the National Key R&D Program of the Ministry of Science and Technology of China (Approval No. 2019YFC1200702).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Tsai FC, Huang Y-T, Chang L-Y, et al. Pyogenic liver abscess as endemic disease, Taiwan. Emerg Infect Dis. 2008;14(10):1592–1600. doi:10.3201/eid1410.071254
2. Luo M, Yang -X-X, Tan B, et al. Distribution of common pathogens in patients with pyogenic liver abscess in China: a meta-analysis. Eur J Clin Microbiol Infect Dis. 2016;35(10):1557–1565. doi:10.1007/s10096-016-2712-y
3. Yu HX, Lin G-S, Zhang J-F, et al. Clinical characteristics of 606 patients with community-acquired pyogenic liver abscess: A Six-Year Research in Yantai. Infect Drug Resist. 2022;15:7067–7075. doi:10.2147/IDR.S372360
4. Zhang S, Zhang X, Wu Q, et al. Clinical, microbiological, and molecular epidemiological characteristics of Klebsiella pneumoniae-induced pyogenic liver abscess in southeastern China. Antimicrob Resist Infect Control. 2019;8:166. doi:10.1186/s13756-019-0615-2
5. Yoo JJ, Lee TK, Kyoung D-S, et al. A population-based study of pyogenic liver abscess in Korea: Incidence, mortality and temporal trends during 2007–2017. Liver Int. 2021;41(11):2747–2758. doi:10.1111/liv.15034
6. Thavamani A, Umapathi KK, Khatana J, et al. Incidence Trends, Comorbidities, and Outcomes of Pyogenic Liver Abscess Among Children: a Nationwide Population-based Analysis. J Pediatr Gastroenterol Nutr. 2020;71(1):106–111. doi:10.1097/MPG.0000000000002700
7. Yin D, Ji C, Zhang S, et al. Clinical characteristics and management of 1572 patients with pyogenic liver abscess: a 12-year retrospective study. Liver Int. 2021;41(4):810–818. doi:10.1111/liv.14760
8. Cui J, Liu Y, Li J. The New Changes of Epidemiology, Etiology, and Clinical Characteristics of Pyogenic Liver Abscesses: a Retrospective Study in a Hospital in Northern China. Infect Drug Resist. 2023;16:4013–4023. doi:10.2147/IDR.S416860
9. Lee IR, Sng E, Lee K-O, et al. Comparison of diabetic and non-diabetic human leukocytic responses to different capsule types of Klebsiella pneumoniae responsible for causing pyogenic liver abscess. Front Cell Infect Microbiol. 2017;7:401. doi:10.3389/fcimb.2017.00401
10. Li W, Chen H, Wu S, et al. A comparison of pyogenic liver abscess in patients with or without diabetes: A retrospective study of 246 cases. BMC Gastroenterol. 2018;18(1):144. doi:10.1186/s12876-018-0875-y
11. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
12. Amoroso C, Perillo F, Strati F, et al. The role of gut microbiota biomodulators on mucosal immunity and intestinal inflammation. Cells. 2020;9(5). doi:10.3390/cells9051234
13. Ansaldo E, Farley TK, Belkaid Y. Control of Immunity by the Microbiota. Annu Rev Immunol. 2021;39:449–479. doi:10.1146/annurev-immunol-093019-112348
14. Iida N, Mizukoshi E, Yamashita T, et al. Overuse of antianaerobic drug is associated with poor postchemotherapy prognosis of patients with hepatocellular carcinoma. Int, J, Cancer. 2019;145(10):2701–2711. doi:10.1002/ijc.32339
15. Milosevic I, Vujovic A, Barac A, et al. Gut-Liver Axis, Gut Microbiota, and Its Modulation in the Management of Liver Diseases: A Review of the Literature. Int J Mol Sci. 2019;20(2):395. doi:10.3390/ijms20020395
16. Anand S, Mande SS. Host-microbiome interactions: gut-Liver axis and its connection with other organs. NPJ Biofilms Microbiomes. 2022;8(1):89.
17. Zheng Y, Ding Y, Xu M, et al. Gut Microbiota Contributes to Host Defense Against Klebsiella pneumoniae-Induced Liver Abscess. J Inflamm Res. 2021;14:5215–5225. doi:10.2147/JIR.S334581
18. Chen N, Ling Z-X, Jin -T-T, et al. Altered Profiles of Gut Microbiota in Klebsiella pneumoniae-Induced Pyogenic Liver Abscess. Curr Microbiol. 2018;75(7):952–959. doi:10.1007/s00284-018-1471-7
19. Zheng Y. Deoxycholic Acid and Lithocholic Acid Alleviate Liver Injury and Inflammation in Mice with Klebsiella pneumoniae-Induced Liver Abscess and Bacteremia. J Inflamm Res. 2021;14:777–789. doi:10.2147/JIR.S298495
20. Guo Y, Wang H, Liu Z, et al. Comprehensive analysis of the microbiome and metabolome in pus from pyogenic liver abscess patients with and without diabetes mellitus. Front Microbiol. 2023;14:1211835. doi:10.3389/fmicb.2023.1211835
21. Song YG, Shim SG, Kim KM, et al. Profiling of the bacteria responsible for pyogenic liver abscess by 16S rRNA gene pyrosequencing. J Microbiol. 2014;52(6):504–509. doi:10.1007/s12275-014-4241-7
22. He Y, Wu W, Zheng H-M, et al. Regional variation limits applications of healthy gut microbiome reference ranges and disease models. Nat Med. 2018;24(10):1532–1535. doi:10.1038/s41591-018-0164-x
23. American Diabetes A. 2. Classification and Diagnosis of Diabetes: Standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S13–S28.
24. Lee CH, Chuah S-K, Tai W-C, et al. Platelet reactivity in diabetic patients with invasive Klebsiella pneumoniae liver abscess syndrome</em>. Infect Drug Resist. 2018;11:1669–1676. doi:10.2147/IDR.S174913
25. Liu C, Guo J. Hypervirulent Klebsiella pneumoniae (hypermucoviscous and aerobactin positive) infection over 6 years in the elderly in China: antimicrobial resistance patterns, molecular epidemiology and risk factor. Ann Clin Microbiol Antimicrob. 2019;18(1):4. doi:10.1186/s12941-018-0302-9
26. Zhou L, Wang C, Bian J, et al. Cerebral venous sinus thrombosis in a patient with Klebsiella pneumoniae primary liver abscess: a case report. BMC Neurol. 2022;22(1). doi:10.1186/s12883-022-02806-y
27. Wang Y, Wang H, Liu Z, et al. The Incidence of Septic Pulmonary Embolism in Patients with Klebsiella pneumoniae Liver Abscess: a Systematic Review and Meta-analysis. Gastroenterol Res Pract. 2022;2022:3777122. doi:10.1155/2022/3777122
28. Molton JS, Chee YL, Hennedige TP, et al. Impact of Regional Vein Thrombosis in Patients with Klebsiella pneumoniae Liver Abscess. PLoS One. 2015;10(10):e0140129. doi:10.1371/journal.pone.0140129
29. Preveden T, Scarpellini E, Milić N, et al. Gut microbiota changes and chronic hepatitis C virus infection. Expert Rev Gastroenterol Hepatol. 2017;11(9):813–819. doi:10.1080/17474124.2017.1343663
30. Ratajczak W, Rył A, Mizerski A, et al. Immunomodulatory potential of gut microbiome-derived short-chain fatty acids (SCFAs). Acta Biochim Pol. 2019;66(1):1–12. doi:10.18388/abp.2018_2648
31. Ney LM, Wipplinger M, Grossmann M, et al. Short chain fatty acids: key regulators of the local and systemic immune response in inflammatory diseases and infections. Open Biol. 2023;13(3):230014. doi:10.1098/rsob.230014
32. Qin N, Yang F, Li A, et al. Alterations of the human gut microbiome in liver cirrhosis. Nature. 2014;513(7516):59–64. doi:10.1038/nature13568
33. Xu H, Wei Y, Ma H, et al. Alterations of Gut Microbiome in the Patients With Severe Fever With Thrombocytopenia Syndrome. Front Microbiol. 2018;9:2315. doi:10.3389/fmicb.2018.02315
34. Wang B, Jiang X, Cao M, et al. Altered fecal microbiota correlates with liver biochemistry in nonobese patients with non-alcoholic fatty liver Disease. Sci Rep. 2016;6:32002. doi:10.1038/srep32002
35. Zhao Z, Guo Z, Yin Z, et al. Gut Microbiota Was Involved in the Process of Liver Injury During Intra-Abdominal Hypertension. Front Physiol. 2021;12:790182. doi:10.3389/fphys.2021.790182
36. Liu J. Ethanol and liver: recent insights into the mechanisms of ethanol-induced fatty liver. World J Gastroenterol. 2014;20(40):14672–14685. doi:10.3748/wjg.v20.i40.14672
37. Salgaco MK, Oliveira LGS, Costa GN, et al. Relationship between gut microbiota, probiotics, and type 2 diabetes mellitus. Appl Microbiol Biotechnol. 2019;103(23–24):9229–9238. doi:10.1007/s00253-019-10156-y
38. Chiang TY, Huang Y-N, Weng Y-C, et al. The influence of early adoption of nonenhanced computed tomography on management of patients with pyogenic liver abscess. JGH Open. 2023;7(6):419–423. doi:10.1002/jgh3.12913
39. Zhang Z, Wang H, Guo Y, et al. Metagenome Analysis of the Bacterial Characteristics in Invasive Klebsiella Pneumoniae Liver Abscesses. Front Cell Infect Microbiol. 2022;12:812542. doi:10.3389/fcimb.2022.812542
40. Tu YC, Lu M-C, Chiang M-K, et al. Genetic Requirements for Klebsiella pneumoniae -Induced Liver Abscess in an Oral Infection Model. Infect Immun. 2009;77(7):2657–2671. doi:10.1128/IAI.01523-08
41. Shin Y, Han S, Kwon J, et al. Roles of Short-Chain Fatty Acids in Inflammatory Bowel Disease. Nutrients. 2023;15(20):4466. doi:10.3390/nu15204466
42. Lange O, Proczko-Stepaniak M, Mika A. Short-chain fatty acids-a product of the microbiome and its participation in two-way communication on the microbiome-host mammal line. Curr Obes Rep. 2023;12(2):108–126. doi:10.1007/s13679-023-00503-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.