")
Back to Journals » Clinical Ophthalmology » Volume 18
Assessment of Preoperative Risk Factors for Post-LASIK Ectasia Development [Response to Letter]
Authors El-Naggar MT , Elkitkat RS , Ziada HED, Esporcatte LPG, Ambrósio R Jr
Received 14 March 2024
Accepted for publication 1 April 2024
Published 8 April 2024 Volume 2024:18 Pages 1045—1047
Mohamed Tarek El-Naggar,1 Rania Serag Elkitkat,2–5 Hossam El-din Ziada,6 Louise Pellegrino Gomes Esporcatte,7–9 Renato Ambrósio Jr7–11
1Refractive Surgery Unit, Ophthalmology Department, Research Institute of Ophthalmology, Giza, Egypt; 2Ophthalmology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 3Watany Eye Hospital, Cairo, Egypt; 4Watany Research and Development Center, Cairo, Egypt; 5Ophthalmology Department, Modern University for Technology and Information, Cairo, Egypt; 6Cornea and Refractive Surgery Unit, Ophthalmology Department, Faculty of Medicine, AL-Azhar University, Cairo, Egypt; 7Rio de Janeiro Corneal Tomography and Biomechanics Study Group, Rio de Janeiro, Brazil; 8Instituto de Olhos Renato Ambrósio, Rio de Janeiro, Brazil; 9Department of Ophthalmology, Federal University of São Paulo, São Paulo, Brazil; 10Brazilian Study Group of Artificial Intelligence and Corneal Analysis - BrAIN, Rio de Janeiro& Maceió, Brazil; 11Department of Ophthalmology, Federal University of the State of Rio de Janeiro (UNIRIO), Rio de Janeiro, Brazil
Correspondence: Mohamed Tarek El-Naggar, Email [email protected]
View the original paper by Prof. Dr. El-Naggar and colleagues
This is in response to the Letter to the Editor
Dear editor
First, we thank Dr. Navarro-Naranjo and his colleagues for their collaboration and interest in our ectasia study.1 In their letter, they mentioned some inaccuracies reported in our study related to the calculation of the NICE. We must respectfully disagree as we present Table 1, which includes the clinical data from the parameters considered in the NICE index. These data support the published NICE results in which 62.5% of the eyes (15 out of 24) presented with a score higher than 5.1 Based on their criteria, these scores would contraindicate for LASIK.2 Interestingly, the remaining nine eyes had a score of 4. While reducing the cut-off would make the sensitivity of 100%, this would also impact the specificity of the criteria.
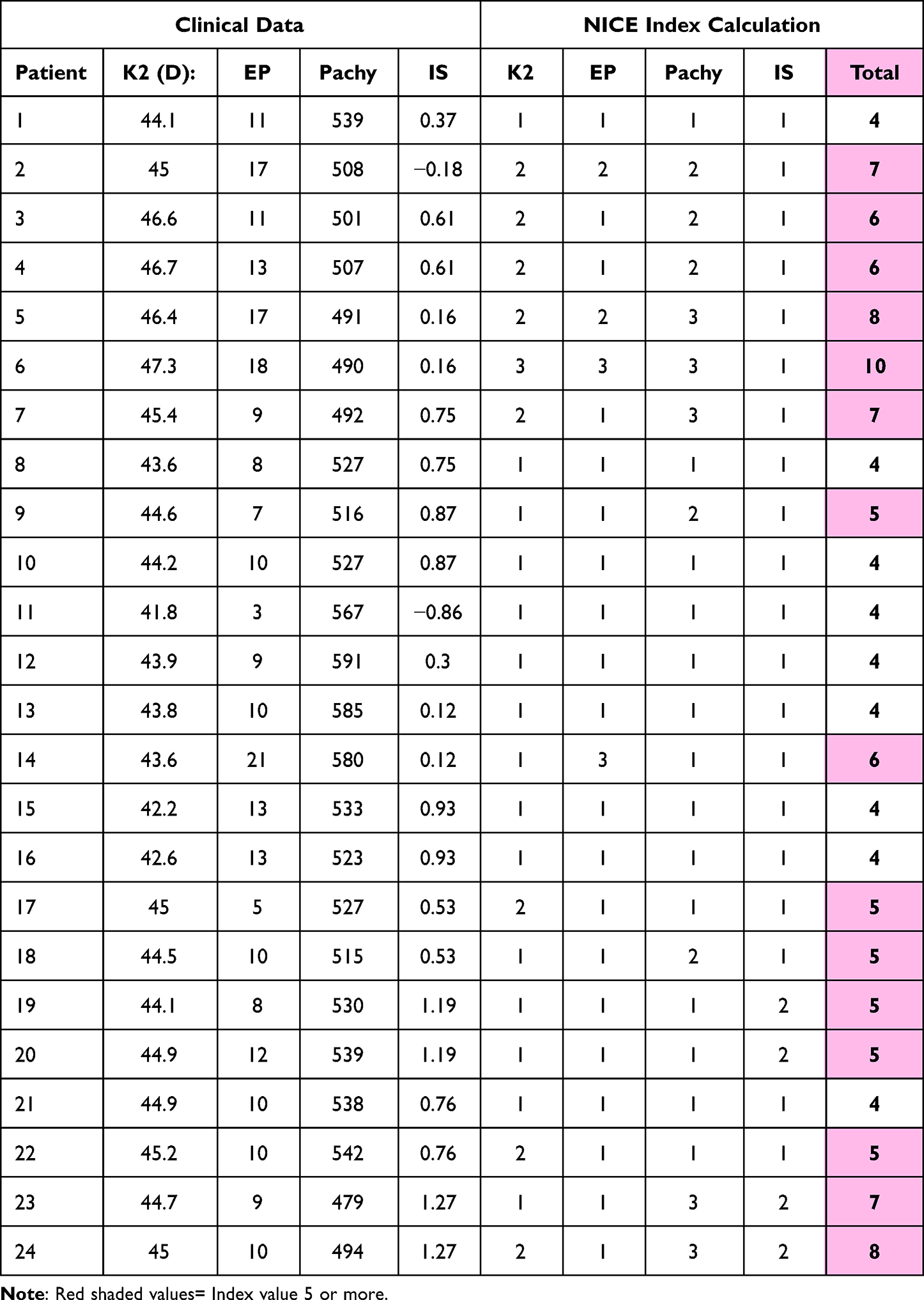 |
Table 1 NICE Clinical Parameters and Calculation |
We agree that a subjective classification may change the criteria of some cases. Nevertheless, while any refractive surgeon should master the interpretation of color-coded curvature maps, the limitations of such subjective classification are relevant. In a previous study that evaluated the subjective classification from 11 experient examiners on 25 cases, high inter-observer variability was observed in the subjective classifications using the same scale. Moreover, the study also found significant intra-observer variability, with eight of the eleven examiners presenting statistically different categories from the maps presented with the Klyce/Smolek 1.5D absolute scale and the 0.5D Holladay (classic Eye Sys red-to-blue) normative scale.3 Differences in calculating the NICE index are expected, considering the subjective classifications.
We agree with Navarro-Naranjo et al in their letter that multimodal diagnostics, beyond front surface topography and 3-D tomography, is essential to augment the safety and efficiency of refractive surgery.4 Corneal biomechanical assessment, integrated with tomography with artificial intelligence, aims to characterize the corneal predisposition or susceptibility to biomechanical decompensation.4,5 This concept goes beyond, but not over, the detection of mild or subclinical (fruste) cases of keratoconus. The BrAIN (Brazilian Artificial Intelligence Networking in Medicine) ectasia software combines with AI the intrinsic predisposition and the extrinsic impact of the corneal procedure to objectively characterize ectasia risk (https://brain.med.br/).
Disclosure
The authors report no conflicts of interest in this communication.
References
1. El-Naggar M, Elkitkat R, Ziada H, Pellegrino L, Ambrosio R. Assessment of preoperative risk factors for post-lasik ectasia. Clin Ophthalmol. 2023;17:3705–3715. doi:10.2147/OPTH.S425479
2. Navarro PI, Torres Y, Bareño J Indice acumulativo de riesgo para tamizaje de candidatos a cirugia corneal refractiva con excimer laser. Editorial Académica Española EAE; 2016. Available from: www.morebooks.de.
3. Ramos IC, Correa R, Guerra FP, et al. Variability of subjective classifications of corneal topography maps from LASIK candidates. J Refract Surg. 2013;29(11):770–775. PMID: 23980708. doi:10.3928/1081597X-20130823-01
4. Ambrósio R, Salomão MQ, Barros L, et al. Multimodal diagnostics for keratoconus and ectatic corneal diseases: a paradigm shift. Eye Vis. 2023;10(1):45. doi:10.1186/s40662-023-00363-0 PMID: 37919821; PMCID: PMC10623885.
5. Ambrósio R, Machado AP, Leão E, et al. Optimized artificial intelligence for enhanced ectasia detection using scheimpflug-based corneal tomography and biomechanical data. Am J Ophthalmol. 2023;251:126–142. PMID: 36549584. doi:10.1016/j.ajo.2022.12.016
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.