")
Back to Journals » Psychology Research and Behavior Management » Volume 17
Association of Non-Suicidal Self-Injury with Tryptophan Hydroxylase 2 Gene Polymorphism and Negative Life Events Among Adolescents with Depression in Northern China
Authors Liu W , Li G, Zhu M, Yang L
Received 4 March 2024
Accepted for publication 11 July 2024
Published 1 August 2024 Volume 2024:17 Pages 2875—2883
DOI https://doi.org/10.2147/PRBM.S462835
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bao-Liang Zhong
Wenliang Liu, Gongying Li, Mengya Zhu, Lin Yang
Department of Psychological, Huai’an No. 3 People’s Hospital, Huaian, People’s Republic of China
Correspondence: Gongying Li, Department of Psychological, Huai’an No. 3 People’s Hospital, No. 272, Huaihai West Road, Huaian, 223001, People’s Republic of China, Tel +86-517-83285124, Email [email protected]
Objective: To investigate the association between single nucleotide polymorphisms (SNPs) of tryptophan hydroxylase 2 (TPH2) (rs11178997, rs11178998, and rs120074175) and negative life events in adolescent depression with Non-suicidal self-injury (NSSI).
Methods: Genomic DNA was extracted from 197 adolescents with depression (participants group, including NSSI group and non-NSSI group), as well as from 100 healthy controls (control group), in northern China. PCR technology was utilized to amplify DNA fragments and detect genotypes in both groups. The Adolescent Life Event Scale (ASLEC) was employed to conduct a questionnaire survey among the participants and control groups. Differences in allele and genotype frequency distribution between the two groups were analyzed using the X^2 test, while generalized multifactor dimensionality reduction (GMDR) was used to analyze gene-environment interactions.
Results: Significant differences were observed in ASLEC scores between the control group and both the NSSI group and non-NSSI group (P< 0.05). Additionally, significant differences were found in the interpersonal relationship factor and punishment factor between the NSSI group and non-NSSI group (P < 0.05). Moreover, a significant difference was identified in SNP genotype of rs11178997 between the depression group (NSSI group + non-NSSI group) and control group (P< 0.05). GMDR analysis revealed an interaction among rs11178997, rs11178998, and ASLEC.
Conclusion: Adolescents with depression, particularly females, may exhibit a tendency to employ NSSI as an emotional coping mechanism when confronted with greater family and interpersonal challenges. The AT genotype of TPH2 gene locus rs11178997 is more prevalent among adolescents with depression. Furthermore, the occurrence of NSSI may be associated with an interaction involving polymorphic sites rs11178997 and rs11178998 along with life events.
Keywords: adolescent depression, non-suicidal self-injury, tryptophan hydroxylase 2, gene polymorphism, life events in adolescence
Introduction
In recent times, there has been a noticeable increase in the occurrence of depression among younger individuals, resulting in a rise in the number of adolescents suffering from depression and experiencing strong thoughts of suicide. This often leads to acts of self-harm and suicidal behavior.1 Apart from the typical clinical symptoms observed in adults with depression, adolescent depression also exhibits distinct characteristics such as non-suicidal self-injury (NSSI). NSSI refers to purposeful and direct harm inflicted on one’s body surface without any intention of ending one’s life.2 Unfortunately, this behavior remains largely unrecognized by society. Common methods employed for self-injury include cutting, pricking, biting, scalding oneself, banging one’s head against walls, and carving patterns into the skin.3 Currently, NSSI poses a significant threat to the mental well-being of adolescents.4 Studies have reported that among adolescents diagnosed with mental disorders like depression, up to 60% have engaged in previous instances of self-harm with a recurrence rate as high as 50%.5 Depression manifests itself through various manifestations; however its causes and underlying mechanisms remain uncertain. A harmonic brain-body communication is fundamental to individual wellbeing and is the basis of human cognition and behavior. Over the past two decades, researchers in both clinical and non-clinical settings have increasingly focused on studying the interaction between brain and body functions. It is evident that dysfunctions in the brain-body axis are present in numerous psychiatric, neurological, and neurodegenerative disorders. The current consensus within the medical community is that depression is a complex condition influenced by multiple genetic and environmental factors.6 Similarly, the etiology and pathogenic mechanism of NSSI remain unresolved, and various theoretical models have been proposed by scholars, including functional models, developmental pathological models, and integrative models. These models suggest that the etiology and pathogenic mechanism of NSSI are closely related to genetic and environmental factors, such as the 5-HT-related polymorphic gene, negative life events, and individual’s growth experience.7–9 In order to investigate potential risk factors associated with NSSI in adolescents diagnosed with depression, we conducted a study that included both depressed adolescents and healthy controls. The group of depressed adolescents was further divided based on the presence or absence of NSSI behaviors. We determined the genotypes of tryptophan hydroxylase 2 (TPH2) polymorphisms (rs11178997, rs11178998, rs120074175) in each subgroup and also assessed adolescent life events using the Adolescent Life Events Scale (ASLEC). We used the generalized multifactor dimensionality reduction (GMDR) method to analyze the influence of gene-environment interactions on adolescent depression and NSSI behavior.
Materials and Methods
Research Subjects
The study subjects were 197 Han Chinese adolescent patients with depression who were admitted to the Psychiatric Department of Huai’an Third People’s Hospital in Jiangsu Province from 2022 to 2023. The patients were divided into the NSSI group and the non-NSSI group by using the random number table method. Based on the definition of NSSI and measures of NSSI used in prior studies, we assessed NSSI using a question that asked “In the past year did you deliberately hurt yourself but not intend to kill yourself (for example, cut or hit yourself on purpose or take an overdose)?”. Respondents who answered “yes” were classified as having NSSI. The control group was comprised of healthy Han individuals who underwent physical examinations at the hospital, matched with the case group in terms of age and gender. All participants provided informed consent after a comprehensive understanding of the study objectives. This study complies with the principles of the Helsinki Declaration and has been approved by the Ethics Committee of Huai’an Third People’s Hospital, with approval number Huai’an 2020–007.
Inclusion criteria: Each patient in the case group received a diagnosis from two psychiatrists with intermediate professional titles or above, according to diagnostic criteria outlined in International Classification of Diseases, 10th edition (ICD-10). In addition, they met specific requirements including: (1) Hamilton Depression Scale (HAMD) score above moderate level (>21 points); (2) no history major physical illnesses prior to enrollment; (3) aged between 12 and 18 years old; and (4) signed informed consent along with their guardian. Healthy control group: Individuals included in this group had no history major physical illnesses prior to enrollment; HAMD score below <8 points before enrollment; aged between 12 and 18 years old; and signed informed consent along with their guardian.
Exclusion criteria: Patients diagnosed with bipolar depression or other mental disorders were excluded from this study. Additionally, those suffering from severe or unstable physical diseases as well as those unable to cooperate were also excluded.
Methods
Survey Tools
Questionnaire: The researchers who received standardized training conducted investigations on all research subjects. Self-designed general questionnaire: The content was divided into two parts, namely general demographic data and patient characteristics, including gender, age, nationality, education level, place of residence, family history, etc. Adolescent Life Events Scale (ASLEC),10 compiled by Liu Xianchen et al, was adapted to assess the frequency and intensity of stressful life events in adolescents, particularly middle school and college students. This scale has a simple structure and is easy to administer. After testing 1473 middle school students for reliability and validity purposes, it demonstrated good psychometric properties. The scale comprises 27 negative life events that may elicit psychological reactions in adolescents. The evaluation period was determined based on the study’s objectives and could span the last 3 months, 6 months, 9 months or 12 months. For each event response option within the specified time frame; if an event did not occur during this period only a “√” should be marked in the corresponding column indicating its absence; if it did occur then participants were asked to rate their psychological feelings at the time of occurrence using a five-point Likert scale ranging from no effect (1), mild (2), moderate (3), severe (4) to extremely severe (5). Completing the scale typically takes approximately five minutes. Statistical indicators encompass event frequency and stress levels. In the absence of any events, it is recorded as having no impact. The cumulative score for each event represents the total amount of stress experienced. For further analysis, these scores can be categorized into six factors: interpersonal relationships, academic pressure, disciplinary actions, loss experiences, health adaptation, and other factors. Different factor scores indicate varying degrees of psychological stress in different environments. All test subjects’ scores are sorted from low to high and averaged into four grades for GMDR analysis. The Hamilton Depression Scale (HAMD), developed by Hamilton, is a widely used clinical assessment tool for measuring depressive states in adults with symptoms of depression. It provides a comprehensive evaluation of disease severity and treatment effectiveness and is considered a classic and recognized rating scale for depression assessment purposes. This scale has three versions: 17-item, 21-item, and 24-item; we will focus on the 24-item version here. Criteria for evaluation are as follows: A total score exceeding 35 points may indicate severe depression; more than 20 points may suggest mild or moderate depression; if the score falls below 8 points, there are no depressive symptoms present.
DNA Extraction and Genotyping
DNA extraction: After obtaining informed consent from the participants, 10mL of peripheral venous blood was collected and stored at −80°C. Subsequently, the human genomic DNA extraction kit (TianGen DP304) was employed for the extraction process. (2) PrimerExpress3.0 software was used for design, and the primer sequences were shown in Table 1. (3) The PCR amplification protocol for the TaqMan assays involved an initial denaturation step at a temperature of 95°C for a duration of 5 minutes, followed by 40 cycles consisting of denaturation at 95°C for 10 seconds and annealing/extension at a temperature of 60°C for a duration of 30 seconds. Finally, there was an elongation step at a temperature of 72°C lasting for 5 minutes. The TaqMan assays were performed using an ABI7900 Fast Real-Time PCR System manufactured by Applied Biosystems. Fluorescence data files obtained from each plate were analyzed using automated software (SDS version 2.1; Applied Biosystems).
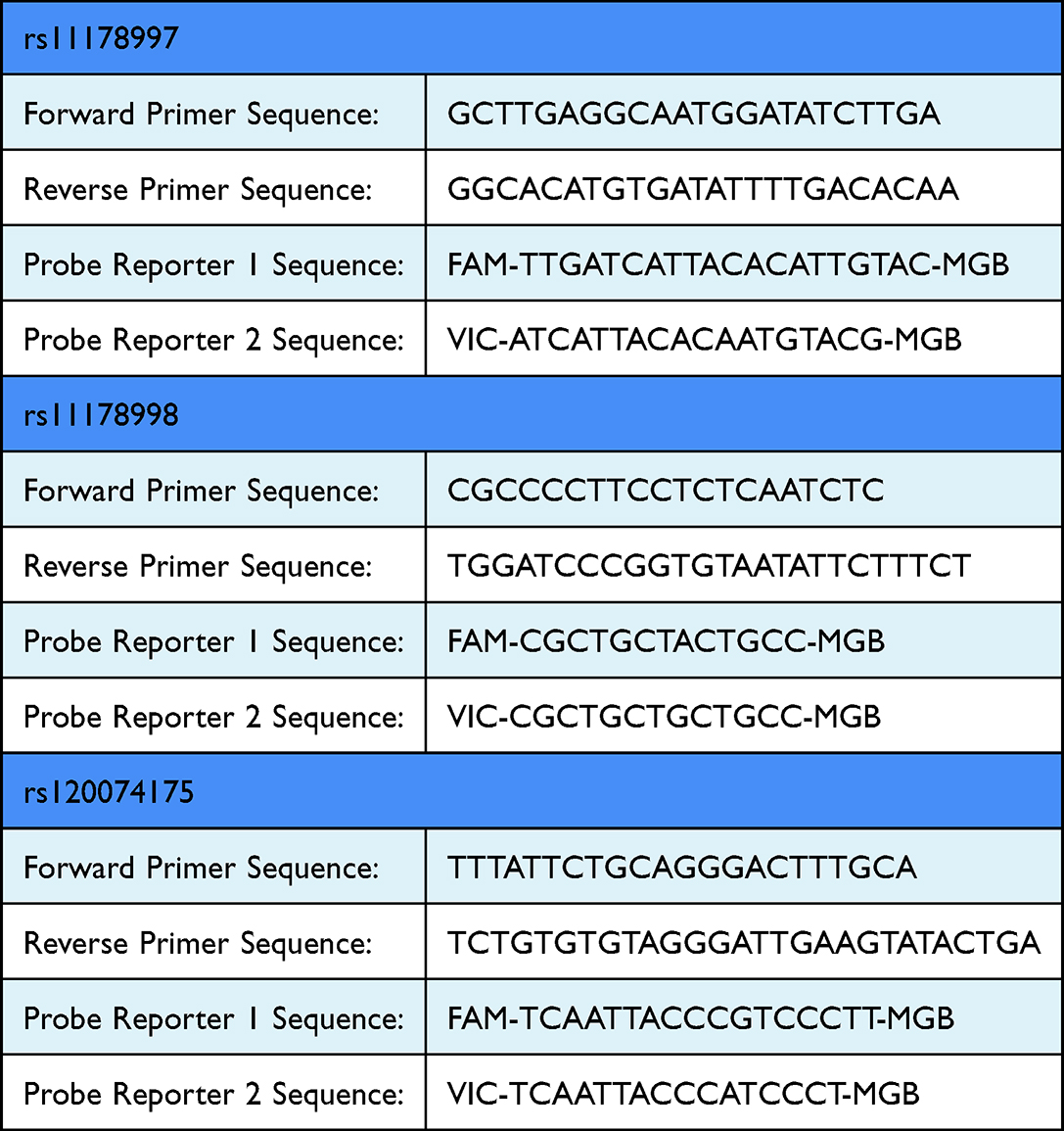 |
Table 1 The Primers Sequence for TPH2 SNPs |
Statistical Methods
The obtained data were inputted into the computer and subjected to statistical analysis using SPSS23.0 software. For comparison of measurement data between the two groups, a two independent sample t-test was conducted for normally distributed variables, with results presented as mean±standard deviation (±SD). In cases where the data did not follow a normal distribution, a rank sum test of two independent samples was performed. One-way analysis of variance (ANOVA) was employed for comparing measurement data among multiple groups when homogeneity of variances or transformed variances were met; otherwise, Kruskal–Wallis H nonparametric test (H-test) was used if heterogeneity persisted even after transformation. Pairwise comparisons of means were conducted using LSD method if homogeneity tests passed, while Games-Howell method was utilized in case homogeneity tests failed. Paired design t-test was applied to compare within-subject differences before and after treatment. X2 test was employed to analyze differences in genotype and allele frequency distributions at gene SNP loci between the two groups. A significance level of P < 0.05 indicated statistical significance. GMDR analysis assessed the influence of gene-environment interaction on self-injury behavior in adolescent depression patients. GMDR is a new statistical analysis software developed in recent years, in which factor refers to the variables in the interaction study, and dimension refers to the number of multi-factor combinations. This method is mainly used in health statistics, epidemiology, and genetics, and it models disease susceptibility classification in a way that studies the interaction between genes and environment, filling the limitation of logistic regression in handling high-order interactions.
Results
Comparison of General Data
The general demographic information of the subjects is as follows: Among the 197 patients with depression, there were 106 in the NSSI group and 91 in the non-NSSI group. In the NSSI group, there were 23 males (21.7%) and 83 females (78.3%), aged between 12 and 18 years, with an average age of 14.2 years. In the non-NSSI group, there were 38 males (41.8%) and 53 females (58.2%), aged between 12 and 18 years, with an average age of 14.2 years. The control group consisted of 29 males (29%) and 71 females (71%), aged between 13–18 years, with an average age of 14 0.3 years. There was no statistically significant difference in age among the three groups (p > 0 0.05). Regarding gender distribution, no statistically significant difference was observed between the control group and both NSSI and non-NSSI groups (p > 0 0.05), but a statistically significant difference existed between NSSIandnon-NSSlgroups (p < 0 0.05). Please refer to Table 2.
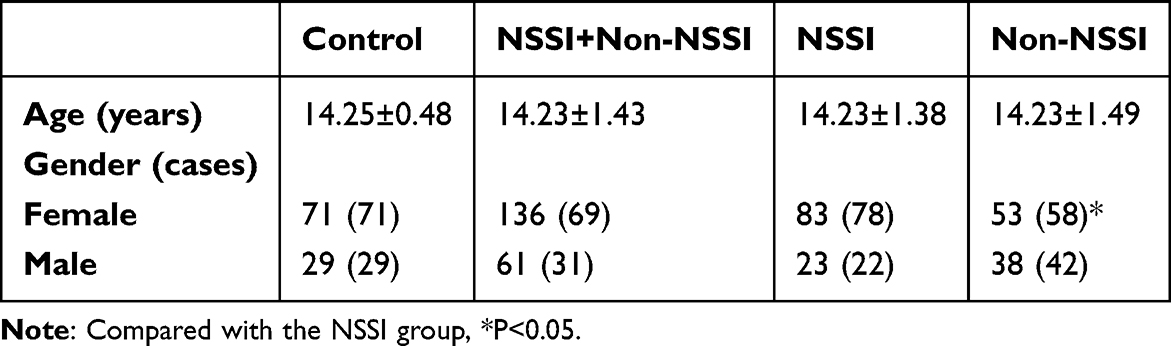 |
Table 2 Comparative Analysis of General Information |
Assessment of ASLEC
The ASLEC assessment revealed significant statistical differences (P < 0.05) in the total score between the control group and the case group, as well as between the NSSI group and the non-NSSI group. However, no statistical difference was observed in the loss factor during factor analysis (P > 0.05). There was also no statistical difference in the total score between the NSSI group and the non-NSSI group (P > 0.05), nor in factors such as learning pressure, loss, health adaptation, and others during factor analysis (P > 0.05). Nevertheless, there were statistically significant differences observed in factors related to interpersonal relationships and punishment (P < 0.05). Please refer to Table 3 for details.
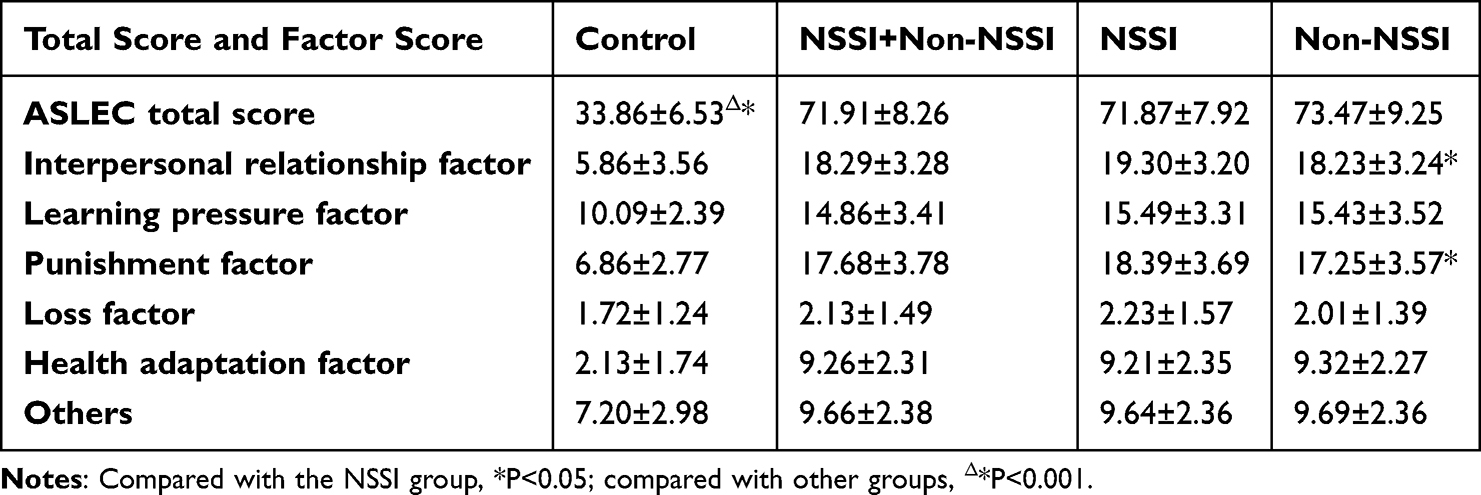 |
Table 3 Scores of Adolescent Life Events Scale |
Comparison of Genotypes and Allele Frequency Distributions of Three SNP Loci
The genetic distribution frequencies of the research subjects adhere to the Hardy-Weinberg equilibrium law and exhibit representative characteristics of the population. Regarding SNP loci genotypes, a statistically significant difference was observed in the rs11178997 locus genotype between the case group (self-injury group + non-self-injury group) and the control group (P < 0.05). Within each individual group, no statistically significant differences were found in the SNP genotypes of the three loci (rs11178997, rs11178998, rs120074175) between the self-injury group and the control group, between the non-self-injury group and the control group, or between the self-injury group and non-self-injury groups (P>0.05). When comparing allele frequency distributions among all three groups, no statistically significant differences were observed (P>0.05). Please refer to Table 4.
 |
Table 4 Genotype and Allele Frequency Distribution [Number of Cases (%)] |
GMDR Analysis of TPH2 Gene Locus and Adolescent Life Events
GMDR was used to analyze the interaction between TPH2 gene and adolescent life events and the risk of NSSI. The third-order model was the optimal model, and there was an interaction between rs11178997, rs11178998 and adolescent life events, with a cross-validation consistency of 10/10 and a sample test accuracy of 0.7446. See Table 5.
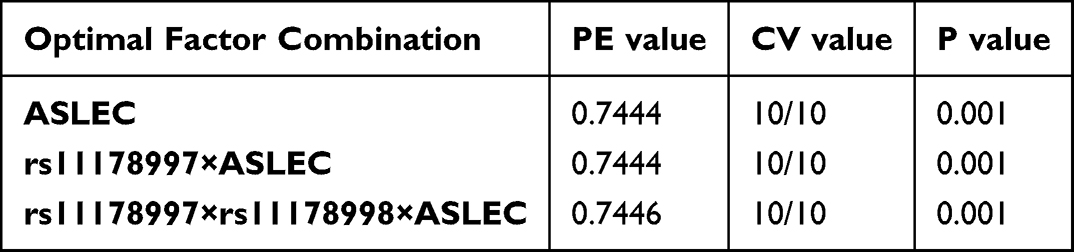 |
Table 5 GMDR Model of Gene-Environment Interaction |
Discussion
Adolescent depression exhibits distinct clinical characteristics compared to adult depression, with a higher prevalence of NSSI observed in adolescents. Numerous studies have consistently demonstrated this pattern, indicating that the occurrence of NSSI peaks during mid-adolescence (around 15–16 years old) and declines during late adolescence (around 18 years old).11,12 The etiology and mechanism underlying NSSI remain unclear. Some studies have suggested an association between negative life events such as social bullying, exposure to family violence, parental criticism, indifference, and abuse with NSSI.5,13,14 Our study results (Table 3) reveal that adolescent patients who experience more significant adolescent life events are more likely to engage in NSSI. Specific factor analysis highlights the prominence of poor family environment, inadequate education, and difficulties in family and interpersonal relationships among these patients – findings consistent with previous research. However, it is important to note that subjective perceptions of life events by adolescents may introduce bias into study outcomes since the same event can be interpreted differently by individuals. Therefore, for depressed adolescent patients, mere consideration of life events may not sufficiently explain the occurrence of NSSI. Furthermore, NSSI is regarded as an effective strategy for regulating negative emotions. Gender differences in the incidence of NSSI have been reported in various studies. In our study (Table 2), we found a higher prevalence of NSSI among female patients compared to male patients – aligning with findings from a case-control study conducted in Wuhan.15 These findings suggest that female patients are more inclined to employ emotional regulation strategies in managing depression and anxiety, potentially serving as the psychological regulatory mechanism underlying the higher prevalence of NSSI among depressed adolescent females compared to males.
It has been reported that NSSI is a biological manifestation of depression, which is associated with susceptibility genes for depression, particularly those encoding proteins involved in the production, metabolism, uptake, and receptors of serotonin (5-HT).16,17 Tryptophan hydroxylase 2 (TPH2), predominantly expressed in the brain and neurons, plays a crucial role in regulating 5-HT synthesis through its enzymatic activity and content. The exon region of TPH2 harbors multiple single nucleotide polymorphisms (SNPs), including rs7305115 and rs4570625, which have been implicated in antidepressant response.18 Studies conducted in Poland suggest an association between interactions of TPH2 and TPH1 gene polymorphisms with depression.19 A meta-analysis conducted internationally revealed that various coding and non-coding SNPs within TPH2 (rs4570625, rs11178997, rs11178998, rs10748185, rs1843809, rs4290270, and rs17110747) were linked to one or more psychiatric disorders. Notably, Tph2 polymorphism exhibited the strongest association with mood disorders, suicidal behavior/attempts, and schizophrenia.20 In Table 4, we conducted genetic testing on three polymorphic loci (rs11178997, rs11178998, rs120074175) of the depression susceptibility gene TPH2 and observed a statistically significant difference in the rs11178997 genotype between the depression group (including both self-injury and non-self-injury groups) and the control group. However, no statistically significant differences were found in SNP genotypes or allele frequencies of the three loci (rs11178997, rs11178998, rs120074175) between either the self-injury group or non-self-injury group compared to the control group. These results indicate that adolescent patients with depression have a higher frequency of AT genotype for the rs11178997 allele compared to healthy controls. Furthermore, our study did not find any association between these three TPH2 loci and NSSI, suggesting that single gene locus polymorphisms may not directly contribute to NSSI development. This could be due to NSSI being an adaptive strategy employed by adolescent patients to cope with life events rather than solely a biological symptom of depression. Due to the complexity and multifaceted nature of depression, its causes and pathogenesis are complex, and our understanding of it is only a small part of the entire picture. However, our current research has also achieved some positive results by understanding depression and NSSI from the perspective of the interaction between genes and environment, and we are hopeful that further in-depth research will lead to a more comprehensive understanding of depression.
Currently, the investigation of gene-environment interaction (G×E) has emerged as a prominent area of research in exploring risk factors associated with depression. Given that certain gene loci exhibit functionality solely under environmental influences, studying gene-environment interactions aids in comprehending how genetic variations and environmental factors interact to contribute to the development of depression.21 Previous studies have indicated an upregulation of TPH2 expression and increased conversion of 5-HT in the brains of depressive suicidal patients and untreated depressive patients, respectively. The elevated expression levels may be attributed to genetic factors, early life experiences, adverse events during adulthood, or their interplay.22 A study on gene-environment interaction conducted among individuals from the Han population residing in northern China revealed a significant G×E interaction between negative life events and variants (rs4570625, rs11178997, rs120074175) within the TPH2 allele.23 Furthermore, a meta-analysis conducted abroad failed to establish a significant correlation between TPH2 and childhood trauma in depressed patients, suggesting that future studies on gene-environment interactions should consider expanding the sample size and conducting more comprehensive evaluations of environmental exposures.24 In our study (Table 5), we discovered a statistically significant interaction between rs11178997, rs11178998, and adolescent life events. This finding partially elucidates why the polymorphism of a single gene locus alone does not lead to NSSI but requires an appropriate environment. However, the limitation of our study is the small sample size and the lack of genome-wide association analysis. The next step should be to further expand the sample size and examine more polymorphic sites, as well as comprehensively and dynamically assess the environmental exposure factors and the relationship between them and NSSI.
Conclusion
Adolescent patients with depression, particularly females, may exhibit a propensity towards engaging in NSSI as a coping mechanism for managing emotions when confronted with increased familial and interpersonal challenges. The AT genotype of the TPH2 gene locus rs11178997 is found to be more prevalent among adolescent patients with depression. Furthermore, there appears to be an association between the interaction of rs11178997 and rs11178998 polymorphic sites and negative life events in relation to NSSI. Depression is a complex and multifaceted disorder, and our study offers insights into both depression and NSSI. However, due to the limitations of the sample size and methodology, we recommend conducting more high-quality longitudinal studies to validate the results of this study.
Data Sharing Statement
All datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics and Consent Statements
The study complies with the Declaration of Helsinki, and all participants were informed and gave their informed consent by signing an informed consent form.
Funding
This study was supported by Huai’an natural science research program (HAB202044).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Luo W, Zhong BL, Chiu HF. Prevalence of depressive symptoms among Chinese university students amid the COVID-19 pandemic: a systematic review and meta-analysis. Epidemiol Psych Sci. 2021;30:e31. doi:10.1017/S2045796021000202
2. Zhong BL, Xu YM, Zhu JH, et al. Non-suicidal self-injury in Chinese heroin-dependent patients receiving methadone maintenance treatment: prevalence and associated factors. Drug Alcohol Depend. 2018;189:161–165. doi:10.1016/j.drugalcdep.2018.05.006
3. Zetterqvist M, Zhu J, Qian R. The DSM-5 diagnosis of nonsuicidal self-injury disorder: a review of the empirical literature. Child Adolesc Psychiatr Ment Health. 2015;9(1):31. doi:10.1186/s13034-015-0062-7
4. Brown RC, Plener PL. Non-suicidal Self-Injury in Adolescence. Curr Psychiatry Rep. 2017;19(3):20. doi:10.1007/s11920-017-0767-9
5. Kaess M, Parzer P, Mattern M, et al. Adverse childhood experiences and their impact on frequency, severity, and the individual function of nonsuicidal self-injury in youth. Psychiatry Res. 2013;206(2–3):265–272. doi:10.1016/j.psychres.2012.10.012
6. Zhong BL, Ruan YF, Xu YM, et al. Prevalence and recognition of depressive disorders among Chinese older adults receiving primary care: a multi-center cross-sectional study. J Affect Disord. 2019;260:26–31. doi:10.1016/j.jad.2019.09.011
7. Hankin BL, Barrocas AL, Young JF, et al. 5-HTTLPR x interpersonal stress interaction and nonsuicidal self injury in general community sample of youth. Psychiatry Res. 2015;225(3):609–612. doi:10.1016/j.psychres.2014.11.037
8. Yates TM, Carlson EA, Egeland B. A prospective study of child maltreatment and self-injurious behavior in a community sample. Dev Psychopathol. 2008;20(2):651–671. doi:10.1017/S0954579408000321
9. Muehlenkamp JJ, Kerr PL, Bradley AR, et al. Abuse subtypes and nonsuicidal self-injury: preliminary evidence of complex emotion regulation patterns. J Nerv Ment Dis. 2010;198(4):258–263. doi:10.1097/NMD.0b013e3181d612ab
10. Chen H, Jia CX, Liu XC. Research progress on the evaluation and application of the Adolescent Life Event Scale. Chin J Public Health. 2016;32(8):1116–1119. doi:10.11847/zgggws2016-32-08-28
11. Moran P, Coffey C, Romaniuk H, et al. The natural history of self-harm from adolescence to young adulthood: a population-based cohort study. Lancet. 2012;379(9812):236–243. doi:10.1016/S0140-6736(11)61141-0
12. Plener P, Schumacher T, Munz L, et al. The longitudinal course of non-suicidal self- injury and deliberate self-harm: a systematic review of the literature. Borderline Personal Disord Emot Dysregul. 2015;2(1):2. doi:10.1186/s40479-014-0024-3
13. Brunstein Klomek A, Snir A, Apter A, et al. Association between victimization by bullying and direct self injurious behavior among adolescence in Europe: a ten-country study. Eur Child Adolesc Psychiatry. 2016;25(11):1183–1193. doi:10.1007/s00787-016-0840-7
14. Tschan T, Schmid M, In-Albon T. Parenting behavior in families of female adolescents with nonsuicidal self-injury in comparison to a clinical and a nonclinical control group. Child Adolesc Psychiatr Ment Health. 2015;9(1):17. doi:10.1186/s13034-015-0051-x
15. Zhu J, Qian R, Zhong H, et al. Factors influencing the addiction characteristics of non-suicidal self-injurious behaviors in adolescents: a case-control study. Front Psychiatry. 2022;13:1033242. doi:10.3389/fpsyt.2022.1033242
16. Albert PR, Le Francois B, Millar AM. Transcriptional dysregulation of 5-HTlA autoreceptors in mental illness. Mol Brmn. 2011;4(1):21. doi:10.1186/1756-6606-4-21
17. Yao K-K, Dong Q-L, Ye L-X. Research progress on adolescent depression and gene polymorphism. Chin J Contemp Pediatr. 2023;25(3):328–332. doi:10.7499/j.issn.1008-8830.2208178
18. Pregelj P. Single nucleotide polymorphisms and suicidal behaviour. Psychiatry Danub. 2012;24(1):61–64.
19. Paulina W, Piotr C, Ewelina S, et al. Association between single nucleotide polymorphisms of TPH1 and TPH2 genes, and depressive disorders. J Cell Mol Med. 2018;22(3):1778–1791. doi:10.1111/jcmm.13459
20. Ottenhof KW, Sild M, Lévesque ML, et al. TPH2 polymorphisms across the spectrum of psychiatric morbidity: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2018;92:29–42. doi:10.1016/j.neubiorev.2018.05.018
21. Assary E, Vincent JP, Keers R, et al. Gene-environment interaction and psychiatric disorders: review and future directions. Semin Cell Dev Biol. 2018;77:133–143. doi:10.1016/j.semcdb.2017.10.016
22. Hale MW, Shekhar A, Lowry CA, et al. Development by environment interactions controlling tryptophan hydroxylase expression. J Chem Neuroanat. 2011;41(4):219–226. doi:10.1016/j.jchemneu.2011.05.002
23. Ma J, Xiao H, Yang Y, et al. Interaction of tryptophan hydroxylase 2 gene and life events in susceptibility to major depression in a Chinese Han population. J Affective Disorders. 2015;188(1):304–309. doi:10.1016/j.jad.2015.07.041
24. Vander Auwera S, Peyrot WJ, Milaneschi Y, et al. Genome-wide gene-environment interaction in depression: a systematic evaluation of candidate genes. Am J Med Genet B Neuropsychiatr Genet. 2018;177(1):40–49. doi:10.1002/ajmg.b.32593
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.