")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Cigarette Smoking, and Blood Monocyte Count Correlate with Chronic Lung Injuries and Mortality
Authors Sangani RG , Deepak V , Anwar J , Patel Z, Ghio AJ
Received 22 November 2022
Accepted for publication 27 March 2023
Published 1 April 2023 Volume 2023:18 Pages 431—446
DOI https://doi.org/10.2147/COPD.S397667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Rahul G Sangani,1 Vishal Deepak,1 Javeria Anwar,1 Zalak Patel,2 Andrew J Ghio3
1Section of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, West Virginia University, Morgantown, WV, USA; 2Department of Radiology, West Virginia University, Morgantown, WV, USA; 3US EPA, Chapel Hill, NC, USA
Correspondence: Rahul G Sangani, Section of Pulmonary, Critical Care, and Sleep Medicine, West Virginia University School of Medicine, 1 Medical Center Dr, PO BOX 9166, Morgantown, WV, 26506, USA, Tel +1 304 293-4661 option #2, Fax +1 304-293-3724, Email [email protected]
Background: Cigarette smoking (CS)-related monocytosis contributes to the development of chronic lung injuries via complex mechanisms. We aim to determine correlations between measures of CS and monocytes, their capacities to predict chronic lung diseases, and their associations with mortality.
Methods: A single-center retrospective study of patients undergoing surgical resection for suspected lung nodules/masses was performed. CS was quantified as cigarettes smoked per day (CPD), duration of smoking, composite pack years (CPY), current smoking status, and smoking cessation years. A multivariate logistic regression analysis was performed.
Results: Of 382 eligible patients, 88% were ever smokers. In this group, 45% were current smokers with mean CPD of 27.2± 40.0. CPY and duration of smoking showed positive linear correlations with percentage monocyte count. Physiologically, CPY was associated with progressive obstruction, hyperinflation, and reduced diffusion capacity (DLCO). Across the quartiles of smoking, there was an accumulation of radiologic and histologic abnormalities. Anthracosis and emphysema were associated with CPD, while lung cancer, respiratory bronchiolitis (RB), emphysema, and honeycombing were statistically related to duration of smoking. Analysis using consecutive CPY showed associations with lung cancer (≥ 10 and < 30), fibrosis (≥ 20 and < 40), RB (≥ 50), anthracosis and emphysema (≥ 10 and onwards). Percentage monocytes correlated with organizing pneumonia (OP), fibrosis, and emphysema. The greater CPY increased mortality across the groups. Significant predictors of mortality included percentage monocyte, anemia, GERD, and reduced DLCO.
Conclusion: Indices of CS and greater monocyte numbers were associated with endpoints of chronic lung disease suggesting a participation in pathogenesis. Application of these easily available metrics may support a chronology of CS-induced chronic lung injuries. While a relative lesser amount of smoking can be associated with lung cancer and fibrosis, greater CPY increases the risk for emphysema. Monocytosis predicted lung fibrosis and mortality. Duration of smoking may serve as a better marker of monocytosis and associated chronic lung diseases.
Keywords: smoking, monocyte, pulmonary fibrosis, lung cancer, mortality, emphysema
Introduction
Smoking-related disease remains the most preventable cause of death.1 While epidemiological studies have established etiological roles for cigarette smoking (CS) in lung cancer and emphysema in a dose-dependent manner, it is also a well-established risk factor for idiopathic pulmonary fibrosis (IPF) and precursor lesions of interstitial lung abnormalities (ILAs).2–5 The presentation of these smoking-related pulmonary injuries is variable with prevalence rates approximating 6.25% for lung cancer (1 in 16 for lifetime probability), 40% for COPD, 0.0005–0.002% for IPF, and 8% for ILAs.6,7
Studies have defined a dose-dependent response between smoking and peripheral monocytosis; these have included the contrasting impacts of current smoking status and smoking cessation.8–10 Accordingly, circulating blood monocyte counts have been associated with lung cancer, COPD, IPF, and ILAs.11–17 Monocytes are a heterogenous population of myeloid cells with well-characterized subsets to maintain tissue integrity and functions of innate and adaptive immunity.18 Classical CD14++CD16− monocytes represent a transient cell population, which contributes to early inflammatory response, whereas non-classical CD14DIMCD16+ monocytes (5–8% of blood monocytes) expand markedly following infection or other inflammatory stimuli.19–21 Along with monocytes, role of alveolar macrophages (AM) as effector cells for the CS-induced immune response have been highlighted.21,22 When encountering stimuli, AM generally can assume two polarized states based on differential cytokines production: M1 or “classically activated” pro-inflammatory phenotype vs M2 or “alternatively activated” anti-inflammatory phenotype.13 Recent evidence has examined the plasticity of AM and their phenotypic polarization existing as a spectrum, largely modified based on local environment.23 CS promotes chronic inflammation, recruitment of immune cell in lungs including non-classical blood monocytes,24,25 initiation of monocyte-to-macrophage program and maturation of macrophages.26–29 In addition to CS, aging affects blood monocytosis and aging induced immunosenescence is associated with development and advancement of chronic respiratory diseases of COPD and pulmonary fibrosis.30–32 Although, the blood monocyte count has shown utility in predicting disease outcome and progression, its role in the natural history of chronic lung diseases remains inconclusive.33 Animal studies have supported a relationship between respiratory disease, CS exposure and monocyte.34 However, equivalent associations are lacking in clinical settings.
An excessive burden of co-existing malignant and non-malignant lung injuries in the Appalachian region reflects the United States’ highest smoking rates.35 This heavily smoking population provided an opportunity to examine the associations between CS, monocytes, and smoking-related lung diseases. Objectives of this study were to describe the associations between: 1) smoking and hematological parameters including monocyte counts, 2) CS, monocyte counts, and radiologic and histologic indices of lung injury, and, lastly, 3) CS, monocyte counts, and mortality.
Materials and Methods
Study Design
After obtaining the approval of the institutional review board, a single-center, retrospective, cohort study was conducted at West Virginia University Hospital (WVUH). Patients who underwent surgical resection for suspicious lung nodules/masses during the study period (January 1, 2017 to December 31, 2020) were identified. Those with a poor-quality CT scan of the chest and/or inadequate lung tissue for histopathology were excluded from the study. Patients were identified as never and ever smokers and the latter were divided into quartiles of smoking pack years (PY).
Data Collection
Self-reported cigarette smoking by patients was reported as never and ever (ex- and current) smokers. For ever-smokers, prolonged cumulative exposure and daily exposure were recorded as composite pack years (CPY; 1 pack-year was 20 cigarettes or the equivalent smoked daily for 1 year) and number of cigarettes smoked per day (CPD), respectively. For ex-smokers, years since quitting smoking was recorded. For each patient, there was a pre-surgical complete blood count (CBC) profile obtained which included total white blood cell (WBC, x109/L), absolute monocyte count (x109/L), percentage monocyte count, hemoglobin (g/dL), hematocrit (%), red blood cell volume (million/mm3), mean corpuscular volume (MCV, fL), mean corpuscular hemoglobin concentration (MCHC, g/dL), and mean corpuscular hemoglobin (MCH) (pg/cell). In addition, charts were reviewed to collect demographics, comorbidities, exposure history (coal, silica, asbestos and others), baseline supplemental oxygen use, and pulmonary function test (PFT) findings. An analysis of radiographic findings (emphysema subtypes, interstitial lung abnormalities (ILAs), and interstitial lung disease (ILD) patterns, traction bronchiectasis (TB), honeycombing (HC)) and histologic abnormalities (anthracosis, peribronchiolar metaplasia (PBM), respiratory bronchiolitis (RB), desquamative interstitial pneumonia (DIP), fibrosis, organizing pneumonia, emphysema, and lung cancer morphology) of the cohort have been previously reported.35 Pulmonary hypertension status was also noted as indicated by the radiographic marker of pulmonary artery to aorta (PA/Ao) ratio >0.9.
Pathologic Evaluation
Retrospective review of consensus histopathologic findings was conducted for the study cohort. At least one tissue section (typically 3–6 sections) for total 382 lung specimens were examined by two pathologists at WVUH. These assessments were performed primarily for suspicious lung nodule or mass, however, the additional non-malignant findings suggestive of emphysema and variety of ILD patterns were reported from the lung tissue un-involved with the tumor. The possible under-reporting of these findings cannot be excluded. Case definition for these findings and detailed methods have been previously described.35
Statistical Analysis
Descriptive statistics included means, medians, and standard deviations to summarize continuous variables and frequency distributions were used to describe categorical variables. Chi-square or Fisher exact tests were used to detect differences in categorical variables between the groups, while means of continuous variables were compared using one-way ANOVA. Tukey’s honest significant difference (HSD) calculator was employed to determine the difference between the individual groups for continuous variables. The Pearson correlation coefficient was used to measure the strength of a linear association between two continuous variables. Logistic regression analysis was used to determine associations of smoking behavior, monocyte and various histologic findings and to predict mortality of the cohort. Two-tailed tests of significance were employed.
Results
Of 392 patients, 382 met the inclusion criteria with sufficient radiology and lung tissue available for evaluation. Forty-six/382 (12%) patients were never smokers (Figure 1). For ever-smokers, 45.4% were current smokers with a mean CPD of 27.2±40.0 for a mean duration of 39.2± 12.7 years; there was a median PY of 45.0 (with an interquartile range (IQR) of 30.5) in the same group. The ever-smokers were divided into groups of quartiles based on their CPY (Figure 1). Each quartile (Q) of ever-smokers comprised of approximately one-fifth of the study cohort (Figure 1). Among the ever-smokers, mean composite pack years smoked increased linearly across the groups (17.2±8.1, 36.5±5.2, 50.8±5.5, and 93.1±31.3 in Q1–4, respectively, p=0). A similar linear trend was observed in means of CPD (14.7±6.5, 21.5±5.1, 23.3±6.0, and 40.2±7.5 in Q1–4, respectively, p=0) and duration of smoking (27.7±15.2, 35.3±7.4, 45.7±9.2, and 47.0±7.5 in Q1–4, respectively, p=0). For ex-smokers, mean years since quit declined across the groups (21.6±18.1, 13.0±11.6, 8.5±10.0, and 7.08±7.4 in Q1–4, respectively, p=0), while there was a higher proportion of current smokers across the groups (32.9%, 44.9%, 48.3%, and 54.8% in Q1–4, respectively, p=0.04) (Figure 2A).
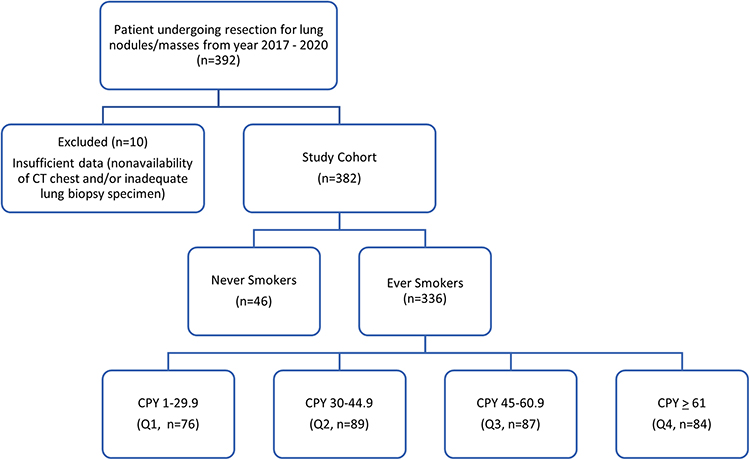 |
Figure 1 Flow chart demonstrating selection of study subjects. Abbreviation: CPY, composite pack year. |
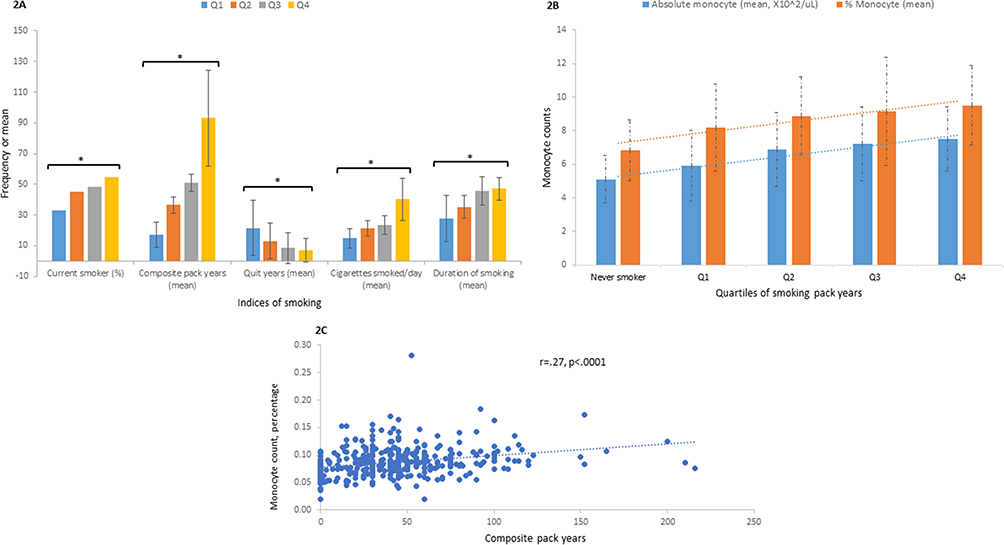 |
Figure 2 Cigarette smoking increased monocytes in the peripheral blood. Different indices of smoking in the study cohort are provided according to quartiles of pack years (A). One-way ANOVA and Tukey’s honest significant difference (HSD) calculator was used to identify significant difference between the groups. Mean values of composite pack years increased across the groups with significant difference existed between all groups. Quit years decreased significantly for groups Q1-Q2, Q1-Q3, and Q1-Q4. Mean number of cigarettes smoked per day increased significantly between groups Q1-Q2, Q1-Q3, Q1-Q4, Q2-Q4, and Q3-Q4. Lastly, mean duration of smoking (years) increased significantly between groups Q1-Q2, Q1-Q3, Q1-Q4, Q2-Q3, and Q2-Q4. Mean absolute monocyte count (x102/µL) increased significantly across the groups: NS- Q2, NS- Q3, NS-Q4, Q1-Q2, Q2-Q3, and Q1- Q4 (B). Similar significance was maintained across groups for percentage monocyte count: NS- Q1, NS-Q2, NS-Q3, NS-Q4, and Q1-Q4. The correlation between percentage monocytes and composite pack years was significant (C). *Statistically significant (p<0.05). Abbreviation: Q1 to 4, quartile 1 to 4. |
The cohort was elderly with a mean age of 66.0±10.1 years, and there were no significant differences in ages between the groups of smokers. Q4 had a higher proportion of males and body mass index (BMI) declined significantly with increasing CPY (Table 1). Comorbid COPD, peripheral artery disease (PAD), coronary artery disease (CAD), and baseline hypoxemia were more common in heavy smokers, while hypothyroidism was more frequent among never smokers (Table 1). Exposure to coal, silica and asbestos were not different between the groups (Table 1). Hematological parameters including total WBC count, hemoglobin, hematocrit, MCV, MCHC, and MCH were not significantly different between the groups, however, compared to never smokers, Q4 group showed significantly reduced RBC volume and increased MCV (Table 1). Means of absolute monocyte (5.1±1.4, 5.9±2.1, 6.9±2.2, 7.2±2.2, and 7.5±1.9, x102/µL, respectively, p=0) and percentage monocyte (6.8±1.8, 8.2±2.6, 8.9±2.3, 9.1±3.2, and 9.5±2.4, respectively, p=0) increased significantly across the groups from never smokers to Q4 (Figure 2B). There was a positive linear correlation between CPY and percentage monocyte (r=0.27, p<0.0001, Figure 2C). In contrast, age did not correlate with percentage monocyte count (r=0.043, p=0.435).
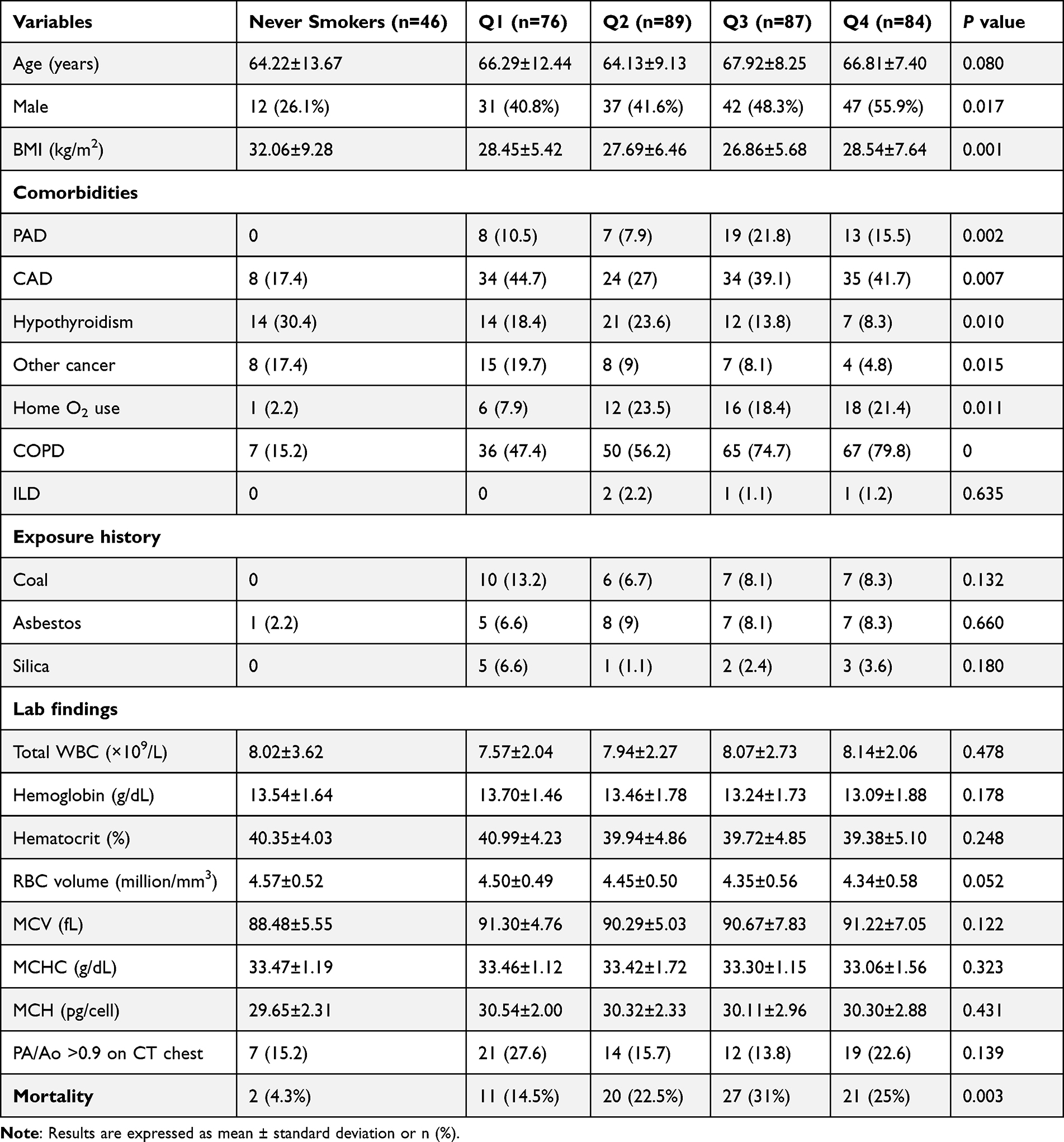 |
Table 1 Characteristics of Groups by Smoking Pack Years (Quartiles) |
The prevalence of radiologic and histologic abnormalities increased drastically across the groups of never smokers to Q4 (Figure 3A and B). The proportion of any radiologic emphysema (13% vs 78.9% vs 96.6% vs 98.8% vs 98.8%, respectively, p=0), centrilobular (CL) emphysema (10.9% vs 72.4%, 86.5% vs 86.2% vs 94.1%, respectively, p=0), paraseptal (PS) emphysema (2.2% vs 23.7% vs 41.6% vs 36.8% vs.46.4%, respectively, p<0.001) and ILD patterns (0 vs 11.8% vs 20.2% vs 21.8% vs 29.8%, respectively, p<0.001) were significantly higher in smokers compared to never smokers. Approximately one-third of patients had any ILA patterns across the groups without significant differences between them. Mixed CL-ground glass opacity (GGO) and subpleural reticular pattern of ILA showed statistical significance for higher CPY (10.9%, 17.1%, 10.1%, 26.4%, and 17.9%, respectively, p=0.044). Rates of isolated TB or HC changes were not different. Proportions of patients with any histologic emphysema (28.7% vs 61.8% vs 78.6% vs 86.2% vs 89.3%, respectively, p=0), fibrosis (13% vs 13.2% vs 41.6% vs 25.3% vs 32.1%, respectively, p<0.001), DIP (0 vs 2.6% vs 6.7% vs 13.8% vs 4.8%, respectively, p=0.009) and anthracosis (34.8% vs 54% vs 60% vs 70.1% vs 77.4%, respectively, p<0.001) were significantly different between the groups. While RB-ILD trended towards significance (0, 11.8%, 11.2%, 23%, and 16.7%, respectively, p=0.051), PBM, OP and HC changes were not different between the groups. Representative CT chest and histopathology findings of a patient from Q4 group are shown in Figures 4 and 5, respectively. Morphology of resected nodule/mass was significantly different across the groups for subtypes of squamous cell carcinoma (4.3% vs 22.4% vs 19.1% vs 39.1% vs 42.8%, respectively, p<0.001), neuro-endocrine cancer (2.2% vs 11.8% vs 5.6% vs 2.3% vs 3.6%, respectively, p<0.001), atypical adenomatous hyperplasia (AAH, 10.9% vs 7.9% vs 3.4% vs 0 vs 4.8%, respectively, p=0.032), and benign pathology (17.4% vs 7.9% vs 5.6% vs 4.5% vs 2.3%, respectively, p=0.016), whereas adenocarcinoma (45.6% vs 55.3% vs 53.9% vs 37.9% vs 38.1%, respectively, p=0.055) trended towards significance (Figure 6). Rates for subtypes of small cell carcinoma, large cell carcinoma and metastatic disease did not differ between the groups.
 |
Figure 3 Increasing prevalence of radiologic and histologic findings with increasing intensity of smoking. The proportion of patients with radiologic evidence of any emphysema, centrilobular (CL) emphysema, paraseptal (PS) emphysema, ILD pattern, and mixed centrilobular-ground glass opacity (CL-GGO) and subpleural reticular (SPR)-interstitial lung abnormality (ILA) pattern increased across the groups, p<0.05 (A). Histological findings of emphysema, fibrosis, desquamative interstitial pneumonia (DIP) and anthracosis varied significantly, p<0.05 (B). Abbreviation: Q1 to 4, quartile 1 to 4. |
 |
Figure 4 Radiographic findings in a 67-year-old-male active smoker patient with 100 CPY smoking history. Axial presurgical CT chest images showed advanced centrilobular (yellow arrowhead), paraseptal (yellow arrow) and bullous emphysema (asterisk) (A). (B) represented bibasilar subpleural reticular changes with traction bronchiolectasis (solid red arrow) and traction bronchiectasis (dotted yellow arrow). |
 |
Figure 5 Histopathologic findings in a 67-year-old-male active smoker patient with 100 CPY smoking history who underwent right lower lobectomy for suspicious nodule. Photomicrographs of lung specimen showed (a) invasive squamous cell carcinoma with keratin pearls (black arrows) [50X], (b) interstitial fibrosis (black arrow) and anthracotic pigment deposition (green arrow) [100X], (c) respiratory bronchiolitis with macrophages contain finely granular brown pigments (black arrow) [100X], and (d) interstitial fibrosis (black arrow), accumulation of macrophages in the airspace (green arrow) and associated architectural distortion [50X]. |
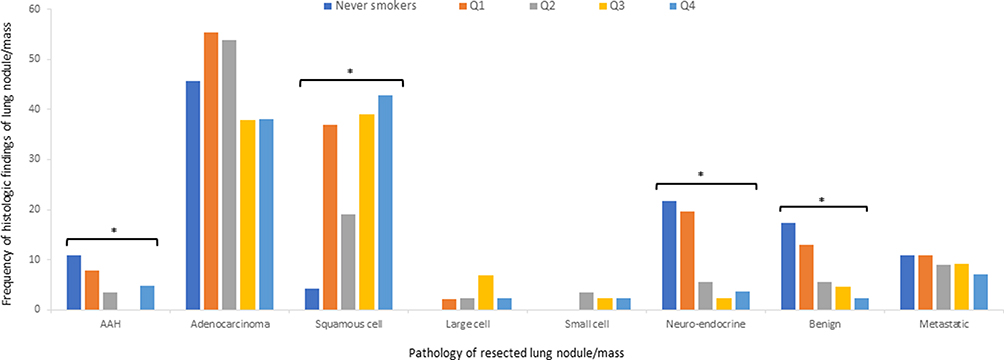 |
Figure 6 Pathology of resected lung nodule/mass in never smokers and quartiles of smoking pack years. While adenocarcinoma trended towards significance, rates of squamous cell cancer increased, and frequencies of atypical adenomatous hyperplasia, neuro-endocrine cancer and benign pathology decreased between the groups. *Statistically significant (p<0.05). Abbreviation: Q1 to 4, quartile 1 to 4. |
Compared to never-smokers, increasing CPY showed reduced means for percentage predicted forced expiratory volume in one second (FEV1, 94.8±19.3 vs 80.7±21.9 vs 76.6±19.4 vs 71.2±20.1 vs 68.9±20.0, respectively, p=0), percentage predicted forced vital capacity (FVC, 92.8±26.1 vs 88.4±17.2 vs 85.6±17.8 vs 82.5±15.8 vs 82.1±19.0, respectively, p=0.008), and FEV1/FVC (78.4±8.3 vs 69.1±12.6 vs 68.5±10.4 vs 65.1±11.5 vs 64.9±12.6, respectively, p=0; Figure 7A), whereas means for percentage predicted residual volume (RV, 115.0±38.1 vs 138.6±66.8 vs 135.6±35.5 vs 149.0±51.2 vs 147.9±48.4, respectively, p=0.006) and RV/total lung capacity (TLC, 108.6±21.7 vs 122.8±26.5 vs 125.6±23.4 vs 131.1±30.7 vs 132.3±24.5, respectively, p<0.001) ratio were greater (Figure 7B). There was a significant decline for percentage predicted diffusing capacity for carbon monoxide (DLCO, 93.3±22.7 vs 71.1±22.2 vs 68.7±18.2 vs 62.5±16.3 vs 61.7±19.6, respectively, p=0; Figure 7C). Lastly, there was linear decline of FEV1/FVC ratio, percentage predicted DLCO in relation to greater CPY and percent monocyte count for the cohort (Figure 7D).
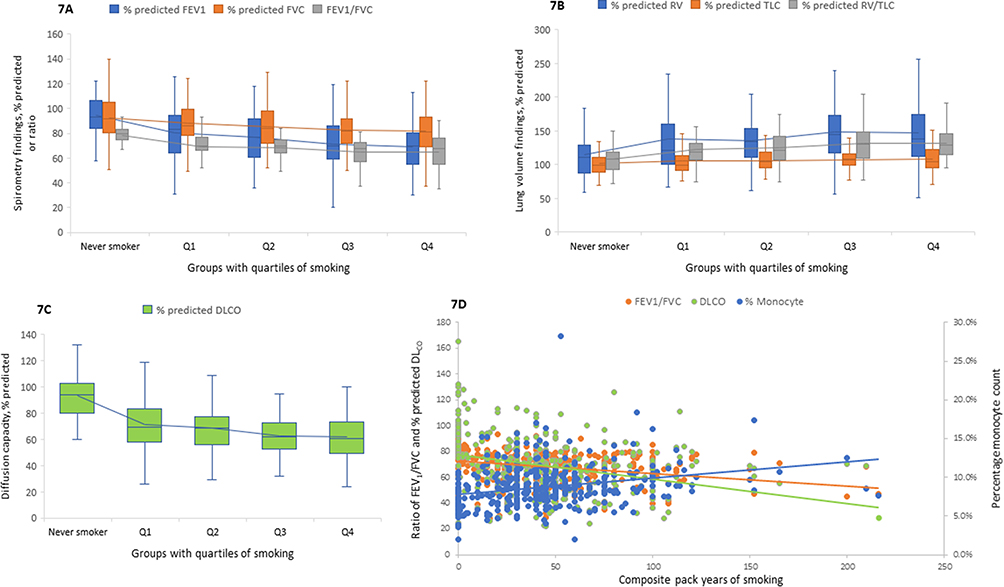 |
Figure 7 Box plots for the various PFT measures in never smokers (NS) and quartiles of CPY (A–C). All measures showed a relationship with smoking except for TLC (p<0.05). Percentage predicted FEV1 and FVC as well as ratio FEV1/FVC declined with smoking (A). For FEV1, there were significant differences between NS and all quartiles, Q1-Q3, and Q1-Q4. For FVC, significant differences were demonstrated between NS-Q3 and NS-Q4 whereas for the FEV1/FVC ratio, comparisons between NS and all quartiles were significant. Percentage predicted RV and TV/TLC increased across all groups (B). For predicted RV, significant differences were demonstrated for NS-Q3 and NS-Q4. For predicted RV/TLC, significance was evident in comparisons between NS-Q2, NS-Q3, and NS-Q4. Percentage predicted DLCO decreased in quartiles of CPY (C). Significant differences were observed between NS-Q1, NS-Q2, NS-Q3, NS-Q4, and Q1-Q4. There was a linear negative correlation between either CPY or percentage monocyte count and PFT measures of ratio FEV1/FVC (r=−0.28, p<0.0001, and r=−0.19, p=0.0001, respectively) and percentage predicted DLCO (r=−0.31, p<0.0001, and r=−0.13, p=0.01, respectively) (D). Abbreviations: DLCO, diffusing capacity for carbon monoxide; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; Q1 to 4, quartile 1 to 4; RV, residual volume; TLC, total lung capacity. |
A linear dose–response relationship was demonstrated across the spectrum of radiologic abnormalities of no disease (n=35, 9.2%), ILA only (n=24, 6.3%), emphysema only (n=107, 28%), ILA+ emphysema (n=145, 37.9%), and ILD+ emphysema (n=71, 18.6%) for both indices of cigarette smoking and monocytes (absolute count and percentage) (Figure 8). While a statistically significant reduced prevalence of never smokers (71% vs 66.7% vs 3.7% vs 4.1% vs 0, respectively, p=0) and quit years (mean of 32.9±16.6 vs 16.3±15.9 vs 9.4±10.6 vs 8.9±13.7 vs 4.4±7.8, respectively, p=0) were seen, the proportion of patients who were current smokers (9% vs 0% vs 48.6% vs 40.7% vs 53.5%, respectively, p<0.001) and mean CPY of smoking (3.0±6.9 vs 6.2±14.5 vs 47.2±25.4 vs 50.9±33.9 vs 58.5±31.4, respectively, p=0) increased consistently across the groups (Figure 8A). From no disease to accumulation of radiologic injuries, there was a linear rise in the means of absolute monocyte count (4.9±1.5 vs 5.1±1.2 vs 6.6±2.3 vs 7.0±1.8 vs 7.7±2.3, x102/uL, respectively, p=0) and percentage monocyte (5.8±1.3 vs 7.2±1.6 vs 8.5±3.1 vs 9.1±1.9 vs 10.2±3.1, respectively, p=0; Figure 8B). Distribution of histologic findings across these groups of radiologic abnormalities showed a significant rise in proportion of patients with lung cancer, PBM, anthracosis, RB-ILD, DIP, fibrosis, emphysema and HC (Figure S1).
 |
Figure 8 Relationship between indices of smoking, blood monocyte count and groups of radiologic abnormalities. For mean years since quitting smoking, there were significant differences between no disease and emphysema only, no disease and ILA+emphysema, and no disease and ILD+emphysema (A). For mean composite pack years of smoking, significant comparisons included no disease and emphysema only, no disease and ILA+emphysema, no disease and ILD+emphysema, ILA and emphysema, ILA and ILA+emphysema, and ILA and ILD+emphysema (A). There were significant increases in both absolute monocyte (x102/µL) and percentage monocyte count associated with radiologic injuries, p<0.05 (B). Significant differences in absolute monocyte count were observed between no disease and emphysema, no disease and ILA+emphysema, no disease and ILD+emphysema, ILA and emphysema, ILA and ILA+emphysema, ILA and ILD+emphysema, and emphysema and ILD+emphysema. With percentage monocyte count significance was evident in comparisons between no disease and emphysema, no disease and ILA+emphysema, no disease and ILD+emphysema, ILA and ILA+emphysema, ILA and ILD+emphysema, emphysema and ILA+emphysema, emphysema and ILD+emphysema. *Statistically significant (p<0.05). Abbreviations: ILA, interstitial lung abnormality; ILD, interstitial lung disease. |
Smoking habits of the cohort were significantly different between men (n=169, 44.2%) and women (n=213, 55.8%). Male patients were more likely to be ever-smoker (90.5% vs 83.5%, respectively, p=0.012), smoked higher average daily cigarettes (27.2±13.9 vs 23.3±11.2, respectively, p=0.005) for a longer duration (37.1±16.2 vs 32.7±18.2, respectively, p=0.010), and had excessive resultant CPY exposure (51.5±38.1 vs. 38.1±29.7, respectively, p<0.001). Men were older (67.5±9.5 vs 64.8±10.4, respectively, p=0.008) and underweight (BMI of 27.6±5.5 vs 29.0±7.8 kg/m2, respectively, p=0.042) compared to women. The distribution of comorbid conditions showed a higher prevalence of CAD (42.6% vs.29.6%, respectively, p=0.007), atrial fibrillation (18.3% vs 10.3%, p=0.025), chronic liver disease (8.2% vs.0.9%, respectively, p<0.001) and non-pulmonary malignancy (14.2% vs 8.4%, respectively, p=0.046) among men, whereas women had a higher prevalence of mood disorders (21.9% vs 39.9%, respectively, p<0.001), and hypothyroidism (10.0% vs 23.5%, respectively, p<0.001). Occupational exposures (coal, silica, asbestos and others) were significantly greater among males compared to females (56.2% vs 8.4%, respectively, p<0.0001). Pre-surgical absolute and percentage blood monocyte count were increased in male patients compared to females (7.1±2.3 vs 6.4±1.9 x102/µL, respectively, p=0.001, and 9.4±2.8 vs 8.2±2.4, respectively, p<0.001). The peripheral blood monocyte count correlated positively with male gender (r=0.16, p=0.001). Reflecting the greater smoking history, men had more frequent radiographic evidence of any emphysema (89.9% vs 79.3%, respectively, p=0.003) and CL emphysema (82.8% vs 70.9%, respectively, p=0.004). Radiologic ILA or ILD patterns were not different between the genders. Except for the finding of anthracosis (68.6% vs 55.9%, respectively, p=0.009), the prevalence of other histologic chronic lung findings was not different between the genders. While males had a higher frequency of squamous cell cancer (33.7% vs 19.7%, respectively, p=0.001), females had more adenocarcinoma (38.5% vs 52.1%, respectively, p=0.010) and neuro-endocrine cancer (3.5% vs 9.4%, respectively, p=0.038). Males had significantly reduced ratio FEV1/FVC (64.7±1.5 vs 70.9±11.8, respectively, p<0.001) compared to females but lung volumes or diffusion capacity did not differ. A distribution of entire cohort for the groups of never smokers and quartiles of CPY smoking is presented by gender in Table S1.
A logistic regression model consisting of current smoking status, sequential CPYs, percentage monocyte count and percentage predicted DLCO<70 was developed to predict the histologic findings (Table S2). Significant odds ratio for increasing CPY (≥10 or ≥20 or ≥30 or ≥40 or ≥50) and other variables (from model#4, Table S2) were used to suggest a chronology of histologic injuries (Figure 9). CPY≥10 or ≥20 predicted lung cancer early in the course. Anthracosis was prevalent across all CPY of smoking and was associated with percentage monocyte count. While OP pattern only correlated with percentage monocyte, histologic fibrosis showed an association with percentage monocyte and CPY ≥20 or ≥30. RB was significantly predicted by current smoking status, CPY ≥50 and percentage predicted DLCO<70. Lastly, emphysema showed a significant association with all CPYs and other variables of the model. Alternatively, employing current smoking status, CPD, duration of smoking (years), years since smoking cessation and percentage monocyte count in a logistic regression analysis, the following associations were identified: current smoking with RB, CPD with anthracosis and emphysema, duration of smoking with lung cancer, RB-, emphysema and HC, smoking quit years with PBM, and percentage monocyte with OP, fibrosis, emphysema (Table 2).
 |
Table 2 Logistic Regression Analysis Showing Associations (as or, 95% CI) Between Smoking, Monocyte and Lung Injuries |
 |
Figure 9 Significant predictors for histologic lung injuries. Based on a logistic regression model consisting of current smoking status, successive CPY, percentage monocyte count, and percentage predicted DLCO<70, the odds ratio of significant predictors of histologic lung injuries were displayed. Lung cancer was associated with CPY≥10 or ≥20. Anthracosis showed association with all CPY smoked and percentage monocyte count. While organizing pneumonia (OP) was only associated with percentage monocyte count, fibrosis was associated with moderate smoking exposure and percentage monocyte count. Respiratory bronchiolitis showed correlations with current smoking, CPY≥50, and percentage predicted DLCO<70. Lastly, all variables of the models predicted emphysema: current smoking, CPY (≥10 and onwards), percentage monocyte count, and percentage predicted DLCO<70. Abbreviations: CPY, composite pack year; DLCO, diffusion capacity for carbon monoxide. |
Lastly, mortality increased across the groups with greater CPY (Table 1). Multiple variables were associated with poor prognosis on univariate analysis including older age, higher comorbidity burden, PFT limitations (airflow obstruction, hyperinflation, and reduced diffusion capacity), greater monocyte count, anemia, presence of radiologic emphysema, ILD patterns, isolated HC, and histologic lung cancer, anthracosis and HC changes (Table S3). After adjustment, a multivariate logistic regression model was developed to report the predictors of mortality (Table 3). Percentage monocyte count (OR 1.28 per each unit rise, 95% CI[1.14–1.44], p<0.001), anemia (OR 1.95, 95% CI[1.07–3.56], p=0.029), GERD (OR 1.77, 95% CI[1.02–3.06]), and percentage predicted DLCO<70 (OR 3.17, 95% CI[1.60–6.29], p=<.001) were associated with mortality. While isolated HC on CT chest trended towards significance, CPY, duration of smoking, CPD, and lung cancer were not associated with mortality. Percentage monocyte count and CPY revealed positive correlation with mortality (r=0.29, p<0.00001 and r=0.16, p=0.0017, respectively). In contrast, hemoglobin (g/dL) had weak negative correlation with mortality of the cohort (r=−0.14, p=0.0062).
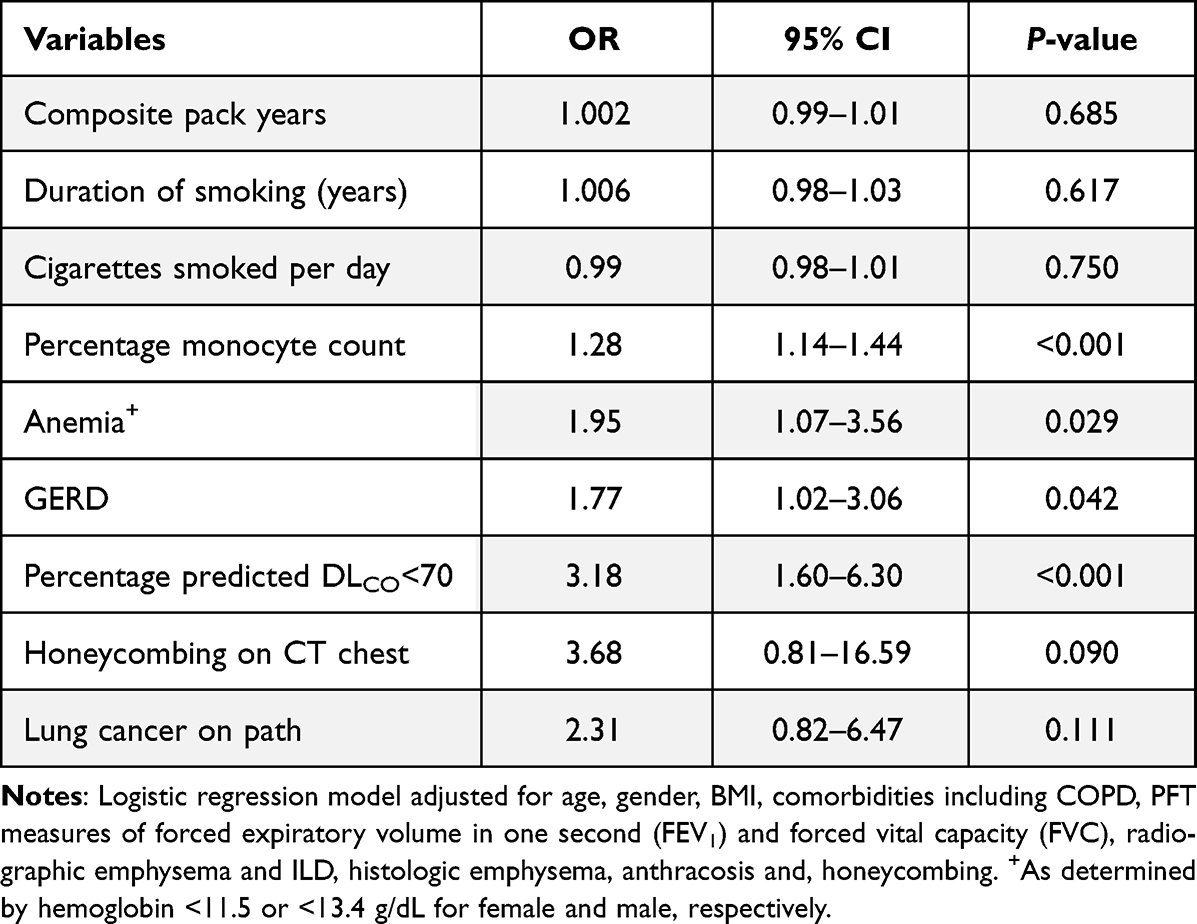 |
Table 3 Predictors of Mortality for the Cohort |
Discussion
The study cohort undergoing surgical resection for suspicious lung nodules/masses showed a distinctive smoking profile (45% current smokers, 88% ever-smoker and average 1.5 packs smoked per day for mean of 40 years) which continues to challenge the central Appalachian region.36,37 One-fourth of the cohort (Q4 group) demonstrated enormous cumulative smoke exposure (approx. 2 ppd for 47 years) and fewer quit years for ex-smokers. Hematologic assessment revealed a dose-dependent, linear correlation between CPY and peripheral monocytosis, independent of the age of cohort. This is similar to a recent cross-sectional study of smokers (r=0.308).38 Stimulating effects of chronic smoking on the bone marrow have been shown to increase 1) the size of the mitotic and postmitotic pools of leukocytes and 2) the transition out of the postmitotic pool.39 A higher plasma level of granulocyte-colony stimulating factor in smokers increases myelopoiesis and circulating monocytosis.24 Air pollution (eg traffic-related air pollution and PM10) and diesel exhaust are among other particle-related exposures, which can also impact a monocytosis.40–42 Components of particles which mediate the elevation in monocytes can include metals and endotoxin.43,44 There is abundant investigation which has demonstrated an extravasation of circulating monocytes into lungs which contributes to the numbers of alveolar macrophages (AM) after further differentiation in response to inflammation.45–47 As sentinel cells, AM are responsible for initiating and resolving immune response to inhaled particles and pathogens. CS has been shown to dysregulate AM functions by influencing its recruitment, phenotype, immune function, and homeostatic roles.23
Considering an involvement of cumulative CS exposure (ie, CPY) and monocytes in lung injury, easily available metrics were employed in a logistic regression model. While plotting odds ratios in relation to successive CPY, a timeframe for the development of lung cancer (PY ≥10 and <30) and fibrosis (PY ≥20 and <40) was suggested. Anthracosis was evident as early as PY ≥10 and steadily maintained during higher exposures. Approximately two-thirds of histologic specimens from the cohort (62%) showed anthracosis and this finding was directly proportional to CPY. Historic tissue-based investigations have shown anthracosis as a result of particle exposures (eg coal and non-coal) with greater concentrations associated fibrosis and limitation of functional capacity of lungs.48 Current smokers with CPY exposure of 20–29 were noted to have similar lung cancer risk as compared to low dose CT scan of chest (LDCT) eligible former smokers (PY≥30).49 Recognizing this burden, recent update on lung cancer screening guidelines have appropriately lowered the requirement of PY to be ≥20.50 Smoking-related fibrosis has been reported in historic autopsy studies and prospective cohort studies.51,52 Our model showed that the active smoking allowed an associated ILD process to become clinically apparent with reduced diffusion capacity. Findings also suggest that the monocytes can be a determinant of these fibrotic injuries. This is comparable to the results of investigation which supports an involvement of monocyte-derived macrophages in the development of lung fibrosis.33,47,53,54 Lastly, emphysema (irreversible cell death) can manifest histologically during early years of smoking (CPY≥10 and onwards) but it became the most prominent feature as CPY increased being associated with all predictors in the model (CPY, current smoking status, percentage monocyte, and DLCO<70). Collaborative evidence was observed when the study cohort was divided as per the accumulation of radiographic abnormalities (ILA, emphysema, and ILD). An additive impact of greater CPY and monocytosis was present across these groups with accumulation of multiple histologic findings. Physiologically, the deleterious impact of CS in the cohort was evident with airflow limitation, hyperinflation and reduction in diffusion capacity, which is comparable to prior observations in a study population.55 Smoking-related monocytosis was associated with a negative effect on lung function.56,57 This chronology of events may suggest a perspective for clinicians to determine the minimum required dose of smoking (in CPY) for the emergence of chronic lung disease. With continued cigarette smoking, diverse patterns of disease can coexist obscuring individual processes.35
Addressing the controversy of smoking exposure assessment in clinical studies, smoking intensity (as CPD) and duration were alternatively employed to determine associations with histologic and radiologic lung abnormalities.58,59 While smoking intensity showed relationships with anthracosis and emphysema, the duration of smoking was associated with multiple lung injuries (cancer, RB-ILD, emphysema and HC). There was little difference in using smoking intensity or duration in the association of percentage monocyte and lung pathology (ie, OP, fibrosis, and emphysema). The duration of smoking mirrors the CPY in its linear relationship with monocyte, whereas CPD did not (r=0.26, p<0.00001 vs r=0.11, p=0.031, respectively). These observations suggest that the duration of smoking was a greater driver of peripheral monocytosis and could serve as a better marker of CS-induced lung damage. Recent investigation suggests that duration can have a higher impact on the development of smoking-related diseases.60
Sexual dimorphism of blood monocyte counts has been reported under physiological conditions with elevated blood monocyte counts among men in all stages of life.61 There was statistically significant smoking burden among men compared to women, which may have contributed towards conglomeration findings of monocytosis, comorbid CAD, radiographic emphysema, and obstructive ventilatory impairment on spirometry. Despite lower cumulative smoke exposure, proportion of females with histologic non-malignant lung injuries (except anthracosis) did not differ from males, which points towards increased susceptibility of women for smoking-associated lung damage at younger age.62 Excess occupational exposures in men could have accounted for greater anthracotic lung deposits than women.48 Lastly, women had significantly higher prevalence of adenocarcinoma as reported in large population-based cohort study.63
Patients who died were less likely to be never smokers, had excessive CPY exposure with greater duration of smoking, however, none of smoking behavior parameters predicted mortality. Absolute monocyte count for patients who did not survive was higher compared to for those who did survive with each rise of percentage monocyte increasing the odds of mortality by 1.28 times. Similarly, peripheral monocytosis has been associated with poor prognosis in diverse lung disease processes including COPD, IPF and lung cancer.16,17,64–67 Monocyte levels were also associated with disease progression in IPF and its precursor lesions of ILAs.11,12 Consequently, monocyte count can function as an inexpensive prognostic biomarker in a smoking population.
Previous investigations have noted an impact of smoking on anemia, erythrocytosis, and increased MCV in healthy subjects.9,68 Diverse mechanisms are involved in the development of anemia in smokers.69 In our study cohort, excessive PY of smoking lead to increased MCV with contraction in RBC volume. A high percentage of patients with lung malignancies in the cohort might have contributed to a reduced rate of effective RBC production and therefore, reduced RBC volume.70 Anemic patients were twice as likely to die in our cohort. Anemia has been similarly linked with poor survival in COPD, fibrotic lung diseases, and lung cancer.71–73 Additionally, reduced diffusion capacity predicted mortality in our cohort which is a recognized prognostic marker for COPD and IPF.74,75
This study has several limitations. Being retrospective in its approach, misclassification of smoking groups is possible. Smoking status could not be validated using biomarkers (eg, measurement of cotinine in blood or carbon monoxide in exhaled air). Underreporting of smoking habits is a common finding due to lower response rates on national surveys and stigmatization of smoking.76 Lastly, the study focused on a cohort of smokers with a lung nodule/mass on presentation and this may limit its generalization. Prior investigations have studied the conflicting correlation between the histologic grades of emphysema and intensity of smoking.77–79 Future large cohort studies can better define the relationship between the histologic and physiologic classification of emphysema (eg Global Initiative for Chronic Obstructive Lung Disease – GOLD) and the smoking indices. Conversely, our study offers strengths in the consecutively enrolled patients who underwent resection and permitting comprehensive assessment of smoking behavior, hematology, PFT (94% of patients), and radiologic and histologic abnormalities.
Conclusion
Our evaluation identified a significant dose–response relationship between smoking behavior, monocytes, and an accumulation of radiologic and histologic lung injuries. There was a linear correlation (positive) between CPY, duration of smoking and peripheral monocytosis. Their impact was evident physiologically as excessive CS exposure caused progressive obstruction, hyperinflation and reduction in diffusion capacity. Despite the heterogenous nature of lung injuries from cigarette smoking, our results highlight a probable chronology of lung pathology. Lung cancer and fibrosis manifested early during smoking. With ongoing CS exposure, monocytes may contribute towards the progression of lung injury with emphysema being the leading histologic finding. Compared to intensity of daily smoking, duration of smoking reflected better correlation with monocyte and associated lung damage. Finally, peripheral monocytosis, anemia and decreased diffusion capacity predicted poor outcomes. These findings highlight the potential guidance to clinicians for the application of timely smoking cessation.
Abbreviations
AM, alveolar macrophage; BMI, body mass index; CAD, coronary artery disease; CBC, complete blood count; CL, centrilobular; CS, cigarette smoking; COPD, chronic obstructive pulmonary disease; CPD, cigarettes smoked per day; CPY, composite pack years; DIP, desquamative interstitial pneumonia; DLCO, diffusing capacity for carbon monoxide; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; GGO, ground glass opacity; HC, honeycombing; HSD, honest significant difference; ILAs, interstitial lung abnormalities; ILD, interstitial lung disease; IPF, idiopathic pulmonary fibrosis; IQR, interquartile range; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; OP, organizing pneumonia; PAD, peripheral artery disease; PBM, peribronchiolar metaplasia; PFT, pulmonary function test; PS, paraseptal; PY, pack years; Q1 to 4, quartile 1 to 4; RBC, red blood cell; RB-ILD, respiratory bronchiolitis-ILD; RV, residual volume; TB, traction bronchiectasis; TLC, total lung capacity; WBC, white blood cell.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Statements
Ethics committee: the study protocol was approved by the Institutional Review Board of West Virginia University (ID 2010131995). The written informed consent was waived by the IRB considering its qualification for exempt research category 4: “secondary research”. The identifiable private information was recorded by the investigators in such a manner that the identity of the human subjects could not readily be ascertained directly or through identifiers linked to the subjects, the investigator did not contact the subjects, and the investigator did not re-identify subjects. The data related to study was collected confidentially to maintain HIPAA compliance. All ethical standards were adhered in accordance with the Declaration of Helsinki.
Acknowledgments
Authors sincerely thank Esra Alshaikhnassir, MD, from the Department of Pathology, West Virginia University for the photomicrographs representing lung histology findings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare they have no financial or non-financial competing interests in this work.
References
1. CDC. Health effects of cigarette smoking; 2022. Available from: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/index.htm#references.
2. Baumgartner KB, Samet JM, Stidley CA, Colby TV, Waldron JA. Cigarette smoking: a risk factor for idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 1997;155(1):242–248. doi:10.1164/ajrccm.155.1.9001319
3. Bilello KS, Murin S, Matthay RA. Epidemiology, etiology, and prevention of lung cancer. Clin Chest Med. 2002;23(1):1–25. doi:10.1016/s0272-5231(03)00057-1
4. Forey BA, Thornton AJ, Lee PN. Systematic review with meta-analysis of the epidemiological evidence relating smoking to COPD, chronic bronchitis and emphysema. BMC Pulm Med. 2011;11:36. doi:10.1186/1471-2466-11-36
5. Lederer DJ, Enright PL, Kawut SM, et al. Cigarette smoking is associated with subclinical parenchymal lung disease: the multi-ethnic study of atherosclerosis (Mesa)-lung study. Am J Respir Crit Care Med. 2009;180(5):407–414. doi:10.1164/rccm.200812-1966OC
6. Beghe B, Cerri S, Fabbri LM, Marchioni A. COPD, pulmonary fibrosis and ILAs in aging smokers: the paradox of striking different responses to the major risk factors. Int J Mol Sci. 2021;22(17). doi:10.3390/ijms22179292
7. Ridge CA, McErlean AM, Ginsberg MS. Epidemiology of lung cancer. Semin Intervent Radiol. 2013;30(2):93–98. doi:10.1055/s-0033-1342949
8. Bergmann S, Siekmeier R, Mix C, Jaross W. Even moderate cigarette smoking influences the pattern of circulating monocytes and the concentration of sICAM-1. Respir Physiol. 1998;114(3):269–275. doi:10.1016/s0034-5687(98)00098-x
9. Pedersen KM, Colak Y, Ellervik C, Hasselbalch HC, Bojesen SE, Nordestgaard BG. Smoking and increased white and red blood cells. Arterioscler Thromb Vasc Biol. 2019;39(5):965–977. doi:10.1161/ATVBAHA.118.312338
10. Smith CJ, Kluck LA, Ruan GJ, et al. Leukocytosis and tobacco use: an observational study of asymptomatic leukocytosis. Am J Med. 2021;134(1):e31–e35. doi:10.1016/j.amjmed.2020.06.014
11. Achaiah A, Lyon P, Fraser E, et al. Increased monocyte level is a risk factor for radiological progression in patients with early fibrotic interstitial lung abnormality. ERJ Open Res. 2022;8(3). doi:10.1183/23120541.00226-2022
12. Achaiah A, Rathnapala A, Pereira A, et al. Monocyte and neutrophil levels are potentially linked to progression to IPF for patients with indeterminate UIP CT pattern. BMJ Open Respir Res. 2021;8(1). doi:10.1136/bmjresp-2021-000899
13. Cornwell WD, Kim V, Fan X, et al. Activation and polarization of circulating monocytes in severe chronic obstructive pulmonary disease. BMC Pulm Med. 2018;18(1):101. doi:10.1186/s12890-018-0664-y
14. Kapellos TS, Bonaguro L, Gemund I, et al. Human monocyte subsets and phenotypes in major chronic inflammatory diseases. Front Immunol. 2019;10:2035. doi:10.3389/fimmu.2019.02035
15. Kim JS, Axelsson GT, Moll M, et al. Associations of monocyte count and other immune cell types with interstitial lung abnormalities. Am J Respir Crit Care Med. 2022;205(7):795–805. doi:10.1164/rccm.202108-1967OC
16. Kreuter M, Lee JS, Tzouvelekis A, et al. Monocyte count as a prognostic biomarker in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2021;204(1):74–81. doi:10.1164/rccm.202003-0669OC
17. Scott MKD, Quinn K, Li Q, et al. Increased monocyte count as a cellular biomarker for poor outcomes in fibrotic diseases: a retrospective, multicentre cohort study. Lancet Respir Med. 2019;7(6):497–508. doi:10.1016/S2213-2600(18)30508-3
18. Guilliams M, Mildner A, Yona S. Developmental and functional heterogeneity of monocytes. Immunity. 2018;49(4):595–613. doi:10.1016/j.immuni.2018.10.005
19. Fingerle G, Pforte A, Passlick B, Blumenstein M, Strobel M, Ziegler-Heitbrock HW. The novel subset of CD14+/CD16+ blood monocytes is expanded in sepsis patients. Blood. 1993;82(10):3170–3176.
20. Nockher WA, Scherberich JE. Expanded CD14+ CD16+ monocyte subpopulation in patients with acute and chronic infections undergoing hemodialysis. Infect Immun. 1998;66(6):2782–2790. doi:10.1128/IAI.66.6.2782-2790.1998
21. Ziegler-Heitbrock L. Blood monocytes and their subsets: established features and open questions. Front Immunol. 2015;6:423. doi:10.3389/fimmu.2015.00423
22. Mosser DM, Edwards JP. Exploring the full spectrum of macrophage activation. Nat Rev Immunol. 2008;8(12):958–969. doi:10.1038/nri2448
23. Lugg ST, Scott A, Parekh D, Naidu B, Thickett DR. Cigarette smoke exposure and alveolar macrophages: mechanisms for lung disease. Thorax. 2022;77(1):94–101. doi:10.1136/thoraxjnl-2020-216296
24. Elisia I, Lam V, Cho B, et al. The effect of smoking on chronic inflammation, immune function and blood cell composition. Sci Rep. 2020;10(1):19480. doi:10.1038/s41598-020-76556-7
25. Strzelak A, Ratajczak A, Adamiec A, Feleszko W. Tobacco Smoke induces and alters immune responses in the lung triggering inflammation, allergy, asthma and other lung diseases: a mechanistic review. Int J Environ Res Public Health. 2018;15(5). doi:10.3390/ijerph15051033
26. Auffray C, Sieweke MH, Geissmann F. Blood monocytes: development, heterogeneity, and relationship with dendritic cells. Annu Rev Immunol. 2009;27:669–692. doi:10.1146/annurev.immunol.021908.132557
27. Geissmann F, Jung S, Littman DR. Blood monocytes consist of two principal subsets with distinct migratory properties. Immunity. 2003;19(1):71–82.
28. Hoogsteden HC, van Dongen JJ, van Hal PT, Delahaye M, Hop W, Hilvering C. Phenotype of blood monocytes and alveolar macrophages in interstitial lung disease. Chest. 1989;95(3):574–577. doi:10.1378/chest.95.3.574
29. Tacke F, Randolph GJ. Migratory fate and differentiation of blood monocyte subsets. Immunobiology. 2006;211(6–8):609–618. doi:10.1016/j.imbio.2006.05.025
30. Barman PK, Shin JE, Lewis SA, et al. Production of MHCII-expressing classical monocytes increases during aging in mice and humans. Aging Cell. 2022;21(10):e13701. doi:10.1111/acel.13701
31. Murray MA, Chotirmall SH. The impact of immunosenescence on pulmonary disease. Mediators Inflamm. 2015;2015:692546. doi:10.1155/2015/692546
32. Puissant-Lubrano B, Apoil PA, Guedj K, et al. Distinct effect of age, sex, and CMV seropositivity on dendritic cells and monocytes in human blood. Immunol Cell Biol. 2018;96(1):114–120. doi:10.1111/imcb.1004
33. Fernandez IE, Kass DJ. Do circulating monocytes promote and predict idiopathic pulmonary fibrosis progression? Am J Respir Crit Care Med. 2021;204(1):9–11. doi:10.1164/rccm.202101-0207ED
34. Oliveira da Silva C, Monte-Alto-Costa A, Renovato-Martins M, et al. Time course of the phenotype of blood and bone marrow monocytes and macrophages in the lung after cigarette smoke exposure in vivo. Int J Mol Sci. 2017;18(9). doi:10.3390/ijms18091940
35. Sangani RG, Deepak V, Ghio AJ, et al. Interstitial lung abnormalities and interstitial lung diseases associated with cigarette smoking in a rural cohort undergoing surgical resection. BMC Pulm Med. 2022;22(1):172. doi:10.1186/s12890-022-01961-9
36. Prevention WDoT. Smoking Cessation; 2022. Available from: https://dhhr.wv.gov/wvdtp/cessation/pages/default.aspx.
37. Cardarelli K, Westneat S, Dunfee M, May B, Schoenberg N, Browning S. Persistent disparities in smoking among rural Appalachians: evidence from the mountain air project. BMC Public Health. 2021;21(1):270. doi:10.1186/s12889-021-10334-6
38. Gouveia TDS, Trevisan IB, Santos CP, et al. Smoking history: relationships with inflammatory markers, metabolic markers, body composition, muscle strength, and cardiopulmonary capacity in current smokers. J Bras Pneumol. 2020;46(5):e20180353. doi:10.36416/1806-3756/e20180353
39. Terashima T, Wiggs B, English D, Hogg JC, van Eeden SF. The effect of cigarette smoking on the bone marrow. Am J Respir Crit Care Med. 1997;155(3):1021–1026. doi:10.1164/ajrccm.155.3.9116981
40. Goto Y, Ishii H, Hogg JC, et al. Particulate matter air pollution stimulates monocyte release from the bone marrow. Am J Respir Crit Care Med. 2004;170(8):891–897. doi:10.1164/rccm.200402-235OC
41. Nemmar A, Inuwa IM. Diesel exhaust particles in blood trigger systemic and pulmonary morphological alterations. Toxicol Lett. 2008;176(1):20–30. doi:10.1016/j.toxlet.2007.09.006
42. Su TC, Hwang JJ, Yang YR, Chan CC. Association between long-term exposure to traffic-related air pollution and inflammatory and thrombotic markers in middle-aged adults. Epidemiology. 2017;28(Suppl 1):S74–S81. doi:10.1097/EDE.0000000000000715
43. Fessler MB, Carnes MU, Salo PM, et al. House dust endotoxin and peripheral leukocyte counts: results from two large epidemiologic studies. Environ Health Perspect. 2017;125(5):057010. doi:10.1289/EHP661
44. Karakaya A, Yucesoy B, Sardas OS. An immunological study on workers occupationally exposed to cadmium. Hum Exp Toxicol. 1994;13(2):73–75. doi:10.1177/096032719401300202
45. Byrne AJ, Powell JE, O’Sullivan BJ, et al. Dynamics of human monocytes and airway macrophages during healthy aging and after transplant. J Exp Med. 2020;217(3). doi:10.1084/jem.20191236
46. Gibbings SL, Goyal R, Desch AN, et al. Transcriptome analysis highlights the conserved difference between embryonic and postnatal-derived alveolar macrophages. Blood. 2015;126(11):1357–1366. doi:10.1182/blood-2015-01-624809
47. Misharin AV, Morales-Nebreda L, Reyfman PA, et al. Monocyte-derived alveolar macrophages drive lung fibrosis and persist in the lung over the life span. J Exp Med. 2017;214(8):2387–2404. doi:10.1084/jem.20162152
48. Klotz O. Pulmonary anthracosis -a community disease. Am J Public Health. 1914;4(10):887–916. doi:10.2105/ajph.4.10.887
49. Pinsky PF, Kramer BS. Lung cancer risk and demographic characteristics of current 20–29 pack-year smokers: implications for screening. J Natl Cancer Inst. 2015;107(11). doi:10.1093/jnci/djv226
50. Force US, Krist AH, Davidson KW, et al. Screening for lung cancer: US preventive services task force recommendation statement. JAMA. 2021;325(10):962–970. doi:10.1001/jama.2021.1117
51. Bellou V, Belbasis L, Evangelou E. Tobacco smoking and risk for pulmonary fibrosis: a prospective cohort study from the UK biobank. Chest. 2021;160(3):983–993. doi:10.1016/j.chest.2021.04.035
52. Weiss W. Smoking and pulmonary fibrosis. J Occup Med. 1988;30(1):33–39.
53. Fraser E, Denney L, Antanaviciute A, et al. Multi-modal characterization of monocytes in idiopathic pulmonary fibrosis reveals a primed type I interferon immune phenotype. Front Immunol. 2021;12:623430. doi:10.3389/fimmu.2021.623430
54. Teoh AKY, Jo HE, Chambers DC, et al. Blood monocyte counts as a potential prognostic marker for idiopathic pulmonary fibrosis: analysis from the Australian IPF registry. Eur Respir J. 2020;55(4). doi:10.1183/13993003.01855-2019
55. Osaka D, Shibata Y, Abe S, et al. Relationship between habit of cigarette smoking and airflow limitation in healthy Japanese individuals: the Takahata study. Intern Med. 2010;49(15):1489–1499. doi:10.2169/internalmedicine.49.3364
56. McKeever T, Saha S, Fogarty AW. The association between systemic inflammatory cellular levels and lung function: a population-based study. PLoS One. 2011;6(7):e21593. doi:10.1371/journal.pone.0021593
57. Wu X, Wang C, Li H, et al. Circulating white blood cells and lung function impairment: the observational studies and Mendelian randomization analysis. Ann Med. 2021;53(1):1118–1128. doi:10.1080/07853890.2021.1948603
58. Lubin JH, Caporaso NE. Misunderstandings in the misconception on the use of pack-years in analysis of smoking. Br J Cancer. 2013;108(5):1218–1220. doi:10.1038/bjc.2013.76
59. Peto J. That the effects of smoking should be measured in pack-years: misconceptions 4. Br J Cancer. 2012;107(3):406–407. doi:10.1038/bjc.2012.97
60. Pleasants RA, Rivera MP, Tilley SL, Bhatt SP. Both duration and pack-years of tobacco smoking should be used for clinical practice and research. Ann Am Thorac Soc. 2020;17(7):804–806. doi:10.1513/AnnalsATS.202002-133VP
61. Patel AA, Yona S. Inherited and environmental factors influence human monocyte heterogeneity. Front Immunol. 2019;10:2581. doi:10.3389/fimmu.2019.02581
62. Barnes PJ. Sex differences in chronic obstructive pulmonary disease mechanisms. Am J Respir Crit Care Med. 2016;193(8):813–814. doi:10.1164/rccm.201512-2379ED
63. Radkiewicz C, Dickman PW, Johansson ALV, Wagenius G, Edgren G, Lambe M. Sex and survival in non-small cell lung cancer: a nationwide cohort study. PLoS One. 2019;14(6):e0219206. doi:10.1371/journal.pone.0219206
64. Hlapcic I, Dugac AV, Popovic-Grle S, et al. Influence of disease severity, smoking status and therapy regimes on leukocyte subsets and their ratios in stable chronic obstructive pulmonary disease. Arch Med Sci. 2022;18(3):672–681. doi:10.5114/aoms.2020.100720
65. Yang J, Qiao M, Li Y, et al. Expansion of a population of large monocytes (atypical monocytes) in peripheral blood of patients with acute exacerbations of chronic obstructive pulmonary diseases. Mediators Inflamm. 2018;2018:9031452. doi:10.1155/2018/9031452
66. Hai Y, Chen N, Wu W, et al. High postoperative monocyte indicates inferior Clinicopathological characteristics and worse prognosis in lung adenocarcinoma or squamous cell carcinoma after lobectomy. BMC Cancer. 2018;18(1):1011. doi:10.1186/s12885-018-4909-1
67. Kumagai S, Marumo S, Shoji T, et al. Prognostic impact of preoperative monocyte counts in patients with resected lung adenocarcinoma. Lung Cancer. 2014;85(3):457–464. doi:10.1016/j.lungcan.2014.06.015
68. Van Tiel E, Peeters PH, Smit HA, et al. Quitting smoking may restore hematological characteristics within five years. Ann Epidemiol. 2002;12(6):378–388. doi:10.1016/s1047-2797(01)00282-4
69. Leifert JA. Anaemia and cigarette smoking. Int J Lab Hematol. 2008;30(3):177–184. doi:10.1111/j.1751-553X.2008.01067.x
70. Spivak JL. Cancer-related anemia: its causes and characteristics. Semin Oncol. 1994;21(2 Suppl 3):3–8.
71. Caro JJ, Salas M, Ward A, Goss G. Anemia as an independent prognostic factor for survival in patients with cancer: a systemic, quantitative review. Cancer. 2001;91(12):2214–2221.
72. Gurun Kaya A, Ozyurek BA, Sahin Ozdemirel T, Oz M, Erdogan Y. Prognostic significance of red cell distribution width in idiopathic pulmonary fibrosis and combined pulmonary fibrosis emphysema. Med Princ Pract. 2021;30(2):154–159. doi:10.1159/000511106
73. Sarkar M, Rajta PN, Khatana J. Anemia in chronic obstructive pulmonary disease: prevalence, pathogenesis, and potential impact. Lung India. 2015;32(2):142–151. doi:10.4103/0970-2113.152626
74. Balasubramanian A, Putcha N, MacIntyre NR, et al. Diffusing capacity and mortality in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2022. doi:10.1513/AnnalsATS.202203-226OC
75. Ley B, Collard HR, King TE Jr. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(4):431–440. doi:10.1164/rccm.201006-0894CI
76. Liber AC, Warner KE. Has underreporting of cigarette consumption changed over time? Estimates derived from US national health surveillance systems between 1965 and 2015. Am J Epidemiol. 2018;187(1):113–119. doi:10.1093/aje/kwx196
77. Anderson AE
78. Auerbach O, Hammond EC, Garfinkel L, Benante C. Relation of smoking and age to emphysema. Whole-lung section study. N Engl J Med. 1972;286(16):853–857. doi:10.1056/NEJM197204202861601
79. Gillooly M, Lamb D. Microscopic emphysema in relation to age and smoking habit. Thorax. 1993;48(5):491–495. doi:10.1136/thx.48.5.491
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023