")
Back to Journals » Clinical Ophthalmology » Volume 18
Clinical Results of a Trifocal Toric Intraocular Lens Using the Holladay Total Surgically Induced Astigmatism Formula for Correcting Low Corneal Astigmatism in Japanese Patients
Authors Bissen-Miyajima H , Ota Y, Yaguchi S, Nakamura K, Sasaki N
Received 9 November 2023
Accepted for publication 13 February 2024
Published 8 March 2024 Volume 2024:18 Pages 755—763
DOI https://doi.org/10.2147/OPTH.S448427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hiroko Bissen-Miyajima,1 Yuka Ota,1 Saori Yaguchi,1 Kunihiko Nakamura,1 Noriyuki Sasaki2
1Department of Ophthalmology, Tokyo Dental College Suidobashi Hospital, Tokyo, Japan; 2Alcon Japan Ltd, Tokyo, Japan
Correspondence: Hiroko Bissen-Miyajima, Department of Ophthalmology, Tokyo Dental College, Suidobashi Hospital, Kandamisaki‑cho 2‑9‑18, Chiyoda‑ku, Tokyo, 101‑0061, Japan, Tel +81-3-5275-1856, Email [email protected]
Purpose: To evaluate the effectiveness and safety of the AcrySof IQ PanOptix toric intraocular lens (IOL) with cylinder power of 1.0 D (TFNT20) in a Japanese population with low corneal astigmatism and compare with historical control data for nontoric IOLs.
Setting: Tokyo Dental College Suidobashi Hospital, Tokyo, Japan.
Design: Prospective, single-center study.
Methods: Patients ≥ 20 years old received TFNT20 IOL in at least 1 eye based on Alcon Toric calculator (Holladay Total surgically induced astigmatism). Effectiveness endpoints included the percentage of eyes with refractive cylinder ≤ 0.25 D at 30– 60 days after surgery, which was compared with a historical control threshold rate of 29.2% for nontoric IOLs and refractive cylinder ≤ 0.50 D. Monocular uncorrected distance visual acuity (UDVA; 5 m), uncorrected intermediate visual acuity (UIVA; 60 cm), uncorrected near visual acuity (UNVA; 40 cm), and adverse events were evaluated.
Results: Of 41 eyes implanted with TFNT20 IOLs, 37 eyes (90%) achieved refractive cylinder ≤ 0.25 D at 30– 60 days after surgery, demonstrating the superiority of TFNT20 compared with historical data (P< 0.0001). Refractive cylinder of ≤ 0.50 D was achieved by 41 eyes (100%). At 30– 60 days, mean ± SD monocular CDVA was − 0.15 ± 0.07 logMAR, UDVA was − 0.09 ± 0.09 logMAR, UIVA was − 0.00 ± 0.07 logMAR, and UNVA was 0.03 ± 0.07 logMAR. Six eyes (15%) had elevated postoperative intraocular pressure, which returned to normal and was not device-related.
Conclusion: TFNT20 IOLs successfully reduced postoperative refractive cylinder and provided good distance, intermediate, and near uncorrected VAs in Japanese patients with low corneal astigmatism.
Keywords: trifocal IOL, toric IOL, low corneal astigmatism, toric calculator, visual acuity
Introduction
Modern presbyopia-correcting intraocular lenses (PC IOLs), particularly trifocal platforms, substantially minimise spectacle dependence in implanted patients by offering good vision across various distances.1–3 This is in contrast to conventional monofocal IOLs, where most patients required spectacles for near vision.4,5 However, it is noteworthy that postoperative residual astigmatism has been reported to significantly impact the performance of PC IOLs.6–9
The prevalence of astigmatism >0.5 D is increasing in an aging Japanese population, with rates as high as 89–91% among Japanese men and women over the age of 80 years.10,11 The recommended magnitude of preoperative corneal astigmatism for considering the use of toric platforms during IOL implantation varies among surgeons. Typically, for monofocal IOLs, astigmatism of ≥1.0 D for some or ≥1.50 D for others is corrected with toric IOLs. However, when it comes to PC IOLs, the threshold is lower, and corneal astigmatisms of ≥0.75 D are suggested to be corrected with a toric model.6
It is possible for some eyes with low astigmatism (ie, 0.50 to 0.75 D) to achieve better visual function with toric IOLs. Currently, studies using monofocal toric IOLs and PC toric IOLs with low cylinder are limited.12–15
The AcrySof IQ PanOptix Toric IOL (Alcon Vision LLC) is a trifocal IOL that was designed to provide far, intermediate, and near vision and is available in different cylinder powers to reduce pre-existing corneal astigmatism. AcrySof IQ PanOptix Toric IOL models TFNT30–60, with cylinder powers ranging from 1.5 to 3.75 D calculated at the IOL plane (which approximately corrects an average of 70% of this amount of astigmatism at the corneal plane), have been globally introduced and utilized. Recently, model TFNT20 with 1.0 D cylinder at the IOL plane, designed to correct approximately 0.7 D of corneal astigmatism, became available. The magnitude of correction of astigmatism may vary slightly based on the axial length, anterior chamber depth of the implanted eye, and the spherical equivalent of the IOL. To the best of our knowledge, there are no published prospective studies evaluating TFNT20.
The purpose of this study was to evaluate the effectiveness and safety of TFNT20 following cataract removal in a Japanese population with low corneal astigmatism. Historical control data from Japanese patients with low corneal astigmatism implanted with nontoric IOLs were used to assess the superiority of TFNT20.16–18 By focusing directly on patients with low astigmatism, this analysis aims to evaluate the safety and performance of PanOptix toric IOLs with low dioptric cylinder power.
Methods
Study Design
This was a prospective, single-center study (NCT04542525) in patients undergoing cataract surgery who were eligible to receive the AcrySof IQ PanOptix Toric IOL (model TFNT20) in at least 1 eye, based on the Alcon Toric calculator (Holladay Total surgically induced astigmatism [SIA]).19 The toric calculator was used for every patient before TFNT20 implantation.
Calculation of the toricity of the IOL was performed in the Alcon Toric calculator, with the option of Holladay Total SIA algorithm activated. This program takes into account the anterior cornea, along with factors such as predictions of SIA and other variables derived from the analysis of previous case series. In addition, the algorithm incorporates the prediction of posterior corneal astigmatism. While it predominantly classifies posterior astigmatism as “against-the-rule”, the compensations vary based on the type and magnitude of anterior corneal astigmatism and the IOL power.19,20
Preoperative corneal astigmatism was measured using an autokeratometer (Tonoref II; Nidek). Measurements were sequentially performed 3 times on the same day to confirm stable results. All eyes were confirmed within a given threshold (eg, the difference in astigmatism magnitude within 0.15 D and the difference in axis within 5°). At the time of astigmatism measurement, the orthoptist confirmed the ocular surface and let the patient blink before each measurement. The head position of the patient was checked at each measurement. The eye recommended by the Alcon Toric calculator to receive the TFNT20 was included in this study. Eligible patients attended the preoperative and operative visits, as well as 3 postoperative visits (days 1–2, 7–14, and 30–60) for each implanted eye.
Included in the study were patients ≥20 years old with age-related cataracts and with potential postoperative corrected distance visual acuity (CDVA) of 0.5 decimal (0.3 logMAR) or better. Excluded from the study were patients with 3 consecutive unstable measurements by an autokeratometer and irregular corneal astigmatism assessed by topography (TMS-5; Tomey); history of ophthalmic pathology; previous intraocular or corneal surgery; or patients who required additional procedures during surgery.
The trial was conducted in accordance with the principles of the Declaration of Helsinki and in compliance with good clinical practice. It was approved by the Tokyo Dental College Suidobashi Hospital Institutional Review Board. All patients provided written informed consent before the initiation of any study-specific procedures.
Selection of Intraocular Lens
The IOL power (spherical equivalent) was calculated using the Barrett Universal II formula after measuring axial length, anterior corneal curvature, anterior chamber depth, and lens thickness with the IOL Master 700 (Carl Zeiss Meditec AG). Anterior corneal astigmatism was measured using an autokeratometer (Tonoref II; Nidek), and these data were entered into the Alcon Toric calculator with the Holladay Total SIA formula activated, as previously explained, to determine the toric IOL to be implanted.19,20
Surgical Procedure
All surgeries were performed by a single surgeon (HBM) through a 2.2-mm temporal corneal incision. All IOLs were successfully implanted in the capsular bag. The peripheral marking dots of the positive cylinder axis were aligned according to the preoperative plan, at or close to the steepest corneal meridian, using a digital marker that compared preoperative images of the conjunctival vessels captured by the IOLMaster700 with the intraoperative image of the eye seen through the microscope, creating overlays in the eyepiece to guide IOL placement (Callisto eye; Carl Zeiss Meditec AG).
Outcomes
The primary effectiveness endpoint was the percentage of eyes with ≤0.25 D refractive cylinder at 30–60 days after surgery. Secondary effectiveness endpoints were percentage of eyes with ≤0.50 D refractive cylinder at 30–60 days after surgery and mean (of both absolute and vectorial magnitude) of refractive cylinder at 30–60 days after surgery.
Supportive effectiveness endpoints included monocular uncorrected distance visual acuity (UDVA) at 5 m, monocular CDVA (5 m), monocular uncorrected intermediate visual acuity (UIVA) at 60 cm, monocular uncorrected near visual acuity (UNVA) at 40 cm, and IOL misalignment at 30–60 days after surgery. For UNVA assessment, the visual acuity chart was aligned at eye level, and the distance was checked with a measuring tape. IOL misalignment was determined as the difference between intended axis obtained by the calculator and the axis mark of the IOL image from anterior optical coherence tomography (CASIA 2; Tomey). The changes between preoperative corneal astigmatism and postoperative refractive astigmatism were evaluated using double-angle vector plots. Safety endpoints were assessed, including adverse events (AEs) such as secondary surgical intervention (SSI), increased intraocular pressure (IOP), and posterior capsulotomy.
Statistical Analysis
For sample size calculation, the percentage of nontoric control was estimated based on historic combined studies of nontoric IOLs conducted in Japan (TFNT00: 135 eyes, SN6AD1: 128 eyes, and SV25T0: 128 eyes).16–18 According to the Holladay Total SIA formula, 137/391 eyes that received nontoric IOLs would have qualified for TFNT20 IOLs. Of these eyes, 29.2% achieved refractive cylinder ≤0.25. Based on the results from a TFNT20 study in the United States (NCT01533831), it was estimated that 60.9% of eyes would achieve ≤0.25 D refractive cylinder in the current study. It was determined that 30 eyes from 30 patients in the TFNT20 group would yield 91.6% statistical power (1-sided alpha of 2.5%) to demonstrate the superiority of TFNT20 to nontoric IOLs for the proportion of eyes achieving ≤0.25 D refractive cylinder using an exact test of binomial proportion.
The primary effectiveness analysis was performed using an exact test of binomial proportion (1-sided alpha of 2.5%) to compare the proportion of eyes with ≤0.25 D refractive cylinder at 30–60 days after surgery to the rate from previous studies. The success criterion for the superiority of TFNT20 to nontoric IOLs was defined as a statistically significant difference between the percentage of eyes in the present study with ≤0.25 D refractive cylinder and the historical control threshold rate of 29.2%.
Results
Patients
A total of 41 eyes from 32 Japanese patients received the TFNT20 IOL after cataract removal; all patients who met the inclusion criteria completed the study. Patient demographics and types of preoperative corneal astigmatism are shown in Table 1.
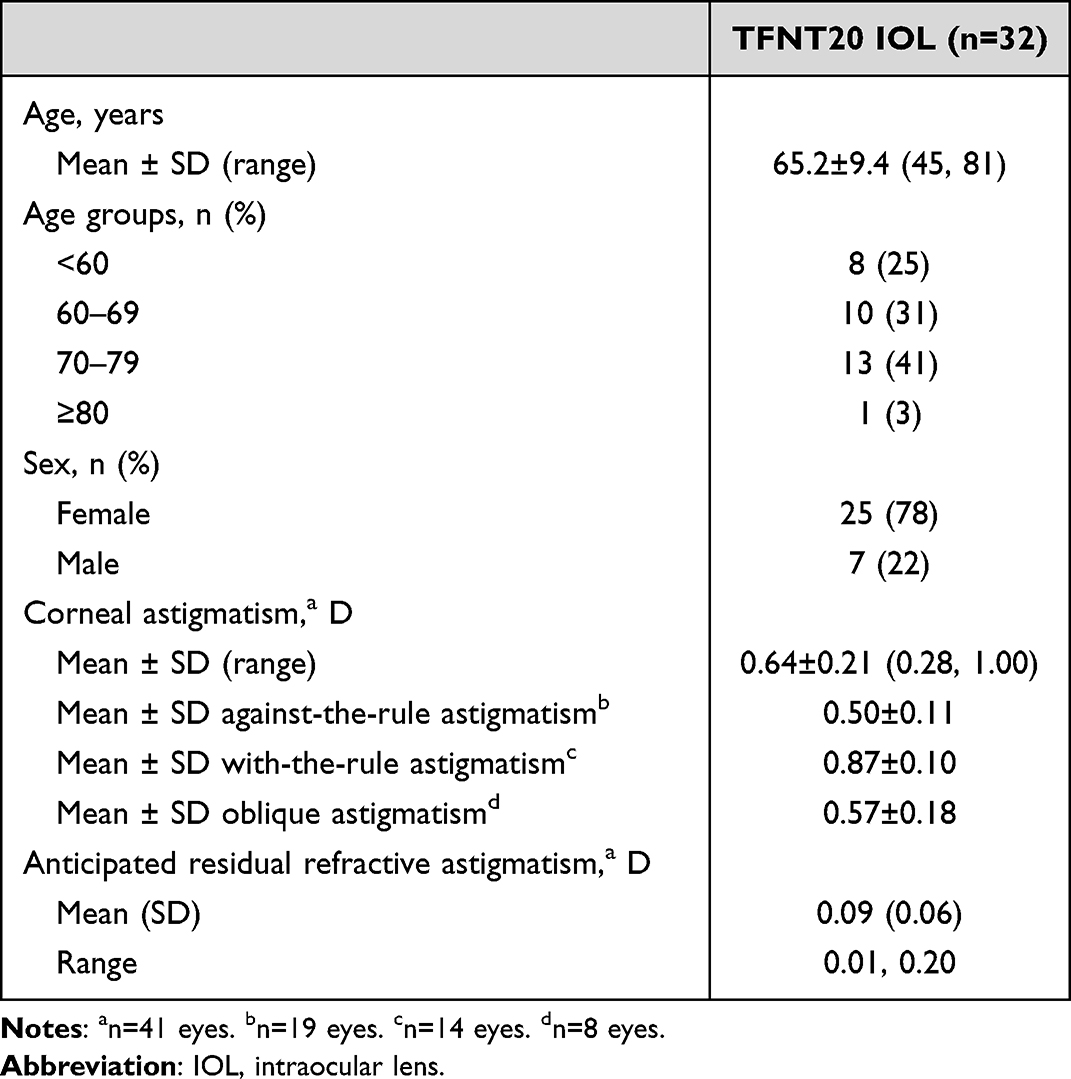 |
Table 1 Patient Demographics and Baseline Characteristics (All-Implanted Data Set) |
Effectiveness Outcomes
Refractive Outcomes
For the primary effectiveness endpoint, 90% (37/41) of eyes achieved the residual refractive cylinder of ≤0.25 D at 30–60 days after surgery (Figure 1). This result was superior to the historical threshold rate of 29.2% (P<0.0001) with nontoric IOLs. Furthermore, ≥93% of eyes achieved refractive cylinder of ≤0.25 D at the early postoperative stage of 1–2 days and 7–14 days. For the secondary effectiveness endpoint, 100% (41/41) of eyes achieved the absolute refractive cylinder of ≤0.5 D at 30–60 days after surgery (Figure 1).
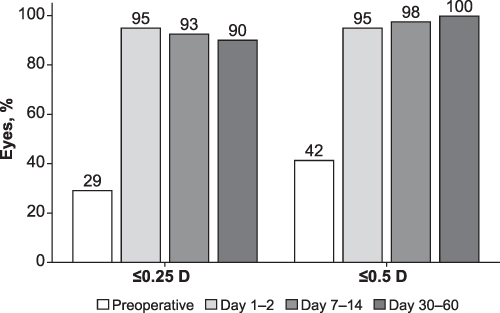 |
Figure 1 Percentage of eyes within a specified threshold of absolute magnitude of refractive astigmatism (all-implanted analysis set). |
Double-angle vector plots of the preoperative corneal astigmatism and postoperative refractive astigmatism are shown in Figure 2. Preoperatively, eyes with against-the-rule (ATR) astigmatism were dispersed to a slightly higher cylinder. The mean ± SD preoperative corneal cylinder was 0.64 ± 0.21 D, and postoperative refractive cylinder was 0.05 ± 0.15 D at 30–60 days after surgery (P<0.0001). The mean ± SD centroids (vectorial aggregation) of both preoperative and postoperative astigmatism were low (0.06 ± 0.68 D and 0.02 ± 0.16 D, respectively) and did not show statistically significant differences (x-axis, P=0.562; y-axis, P=0.129).
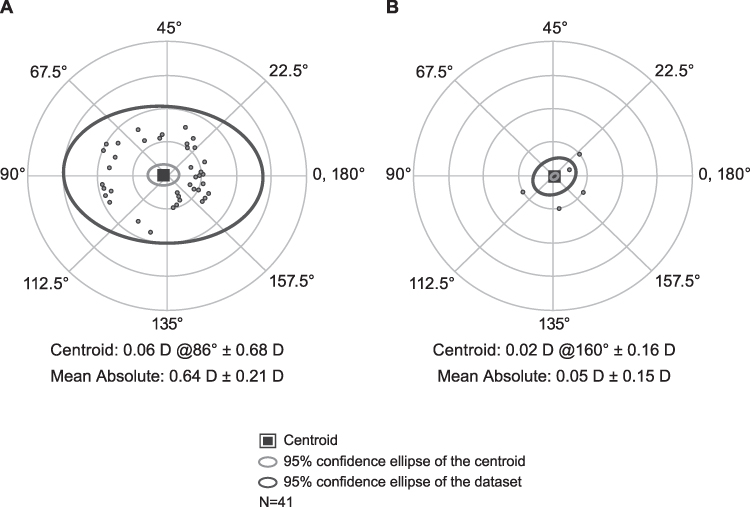 |
Figure 2 Double-angle plots of the preoperative keratometric astigmatism (A) and postoperative refractive astigmatism (B). Concentric circles indicate 0.5 D cylinder steps. Horizontal and vertical axes in both plots range from −2 D to +2 D. |
Postoperative refractive astigmatism prediction error is shown in Figure 3. A total of 40/41 eyes (98%) were within the 0.5 D ring, and the mean absolute error was 0.14 ± 0.13 D; the remaining eye was 0.53 D.
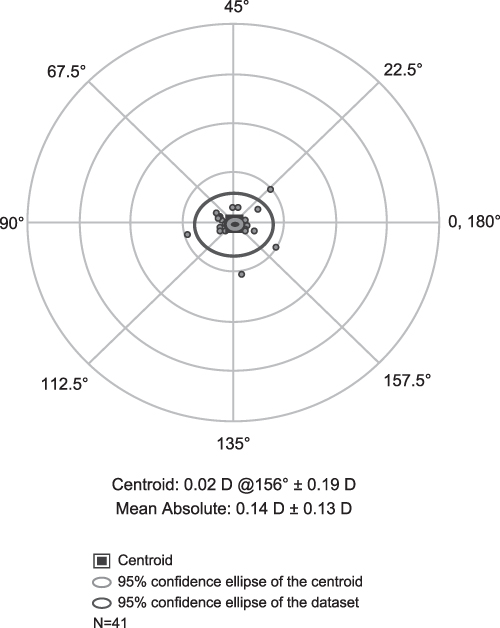 |
Figure 3 Double-angle plot of postoperative refractive astigmatism prediction error of the formula. Concentric circles indicate 0.5 D cylinder steps. Horizontal and vertical axes in both plots range from −2 D to +2 D. |
Visual Outcomes
For the supportive effectiveness endpoints, CDVA, UDVA, UIVA, and UNVA improved at 1–2 days following surgery compared with preoperative VA and remained stable or continued to improve over time (Figure 4). At 30–60 days after surgery, 100% of eyes (41/41) achieved monocular CDVA ≥1.0, 90% (37/41) achieved monocular UDVA ≥1.0, 76% (31/41) achieved monocular UIVA ≥1.0, and 100% (41/41) achieved UNVA of ≥0.4. At 30–60 days after surgery, mean ± SD monocular CDVA was –0.15 ± 0.07 logMAR, mean ± SD monocular UDVA was −0.09 ± 0.09 logMAR, mean ± SD monocular UIVA was −0.00 ± 0.07 logMAR, and mean ± SD monocular UNVA was 0.03 ± 0.07 logMAR. Mean IOL misalignment was 3.8 ± 3.5°.
 |
Figure 4 Percentage of eyes with TFNT20 achieving visual acuity ≥1.0 for CDVA, UDVA, and UIVA, and ≥0.4 for UNVA. Abbreviations: CDVA, corrected distance visual acuity; UDVA, uncorrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected near visual acuity. |
Safety
No SSIs or posterior capsulotomies were reported. A mild increase in IOP occurred in 6 eyes (15%) of 5 patients. However, these events were not device-related, and resolved within 1 week of onset.
Discussion
This prospective study was the first assessment of the efficacy and safety of the TFNT20 IOLs in Japanese eyes with low astigmatism and their superiority to nontoric IOLs using historical data. For these eyes, either TFNT00 or TFNT30 had been selected until TFNT20 became available. In this study, the low amount of preoperative cylinder was successfully reduced with TFNT20. Residual refractive cylinder of ≤0.25 was achieved by 37/41 (90%) eyes with TFNT20 IOLs at 30–60 days after implantation; this was significantly above the historical threshold rate of 29.2% for nontoric IOLs and demonstrated the superiority of TFNT20 (P<0.0001).
Toric IOLs are widely accepted to reduce refractive astigmatism, improving uncorrected VA.21–23 Based on favorable results, there is a growing trend toward the use of toric lenses, even for eyes with lower astigmatism. A comparative study in 94 eyes reported that a monofocal toric IOL with low cylinder provided lower residual refractive cylinder (0.31 vs 0.53 D; P<0.01) and significantly better UDVA (0.01 vs 0.07 log MAR; P<0.02) compared with a nontoric monofocal IOL.15 For PC IOLs, reduction of refractive astigmatism improved not only UDVA but also UIVA and UNVA. In a study of ReSTOR IOL (ART2), postoperative refractive cylinder of a toric IOL was significantly lower compared to that with nontoric IOL (−0.18 vs −0.91 D, respectively; P<0.01), and UDVA, UIVA, and UNVA were significantly better with the toric model.12 Another study of ReSTOR (SND1T2) reported that 70.5% of patients achieved postoperative refractive cylinder of <0.25 D and 88.7% achieved postoperative refractive cylinder of <0.50 D; mean cylinder was −0.19 ± 0.30 D.14 In a study of 26 eyes of 22 patients in Spain, the use of the trifocal toric FineVision PODFT (PhysIOL s.a.) with a cylinder power of 1.0 D resulted in 73% of eyes achieving postoperative refractive cylinder of ≤0.25 D and all eyes (100%) achieving postoperative cylinder of ≤0.50 D; mean cylinder was −0.16 ± 0.22 D.13 This study used the FineVision Toric Calculator. These results are consistent with the outcomes of the current study using the TFNT20 IOLs and Alcon toric calculator (Holladay Total SIA formula), where most eyes (90%) achieved postoperative refractive cylinder of ≤0.25 D and all eyes (100%) achieved postoperative refractive cylinder of ≤0.50 D; mean cylinder was 0.05 ± 0.15 D.
For trifocal IOLs, a postoperative cylinder of 0.0–0.5 D is recommended to achieve optimal VAs at all distances and astigmatism of ≤0.75 D for useful VA.6 Based on the outcomes of this study as well as previous reports, a trifocal IOL with 1.0 D cylinder would be recommended for cases with low corneal astigmatism.
Challenges for correcting low amounts of astigmatism include the accuracy of the measurement of corneal astigmatism and the selection of toric calculator. In this clinical study, the value of corneal anterior astigmatism obtained by autokeratometer was used in all cases. Cases that showed unstable results from 3 consecutive measurements or irregular astigmatism by corneal topography and anterior optical coherence tomography were excluded. The Alcon Toric calculator (Holladay Total SIA formula) was used in all cases.19 The algorithm in the Holladay Total SIA formula takes into account the relationship between the total SIA vector and meridian of preoperative keratometric astigmatism. This algorithm includes factors such as posterior corneal astigmatism associated with postoperative refractive astigmatism, surgically induced astigmatism, IOL tilt, and eccentricity. In this study, 29% and 42% of the eyes with preoperative astigmatism of ≤0.25 and ≤0.5 D, respectively, were selected for TFNT20 with a cylinder power of 1.0 D by a calculator considering total SIA. Double-angle plots of the preoperative keratometric astigmatism in Figure 2 show that most cases were ATR astigmatism. The postoperative refractive cylinder prediction error was 0.14 D. The Alcon toric calculator (Holladay Total SIA formula) worked well with the temporal corneal incision in eyes with low amounts of astigmatism. As this formula is suitable for cases with 2.2–2.5-mm temporal incision, results using a different formula should be evaluated for cases with different incisions, such as superior, steep axis, or width >2.5 mm.
Additional challenges may include external factors such as dry eye and patient collaboration. Dry eye has been reported to increase corneal irregular astigmatism;24 furthermore, dry eye may affect the measurement accuracy of corneal astigmatism.25 In the current study, the ocular surface and tear breakup time were examined using fluorescein staining and slit-lamp, and none of the patients had dry eyes that may have impacted the astigmatism measurements. To achieve accurate measurements, the patients were asked to cooperate in stabilizing their head position and opening their eyelids during the examination.
This study had some limitations, including a relatively short follow-up time, lack of a control group, and a small patient population. The superiority of TFNT20 compared with historical data was notable in this small Japanese patient population. The differences in refraction and astigmatism among countries and in a large number of Japanese patients have been reported.26,27 Future studies in other populations with a larger sample size and a control group would be warranted to confirm these outcomes. Following cataract surgery, an ATR shift of 0.2–0.3 D was observed in eyes with preoperative ATR and oblique astigmatism.28 Long-term multicenter studies are needed to observe the effects of aging on corneal astigmatism. The effects of posterior corneal astigmatism were not evaluated, as the Holladay Total SIA formula was used. Because this study was part of the clinical trial for approval in Japan, postoperative refractive cylinder, VA, and other visual function assessments (ie, photopic and mesopic contrast sensitivities) were required, while other IOL evaluations may have been limited. To achieve better surgical outcomes with toric IOL of low cylinder, further studies evaluating the refractive cylinder are necessary. An additional limitation of this study was that it did not include a vectorial analysis of the change in astigmatism, which would have provided the angle of error (arithmetic and absolute), correction index, magnitude of error, and the difference vector. These additional analyses were outside the scope of this report. Finally, pupil size was not evaluated in this study, and future studies should assess the influence of pupil size on astigmatism.
Conclusion
Good visual performance was reported in Japanese patients with the TFNT20 IOL, and no serious AEs were observed. Most eyes (90%) achieved ≤0.25 residual refractive cylinder. The reduction in refractive cylinder achieved with the TFNT20 may improve visual acuity and spectacle independence in this patient population. Additional long-term studies are needed to further evaluate the effects of TFNT20 and compare the visual acuity of TFNT20 and TFNT00 in patients with low astigmatism.
Data Sharing Statement
The data used to support the primary findings of this study are available upon reasonable request from the study sponsor, Alcon Research LLC.
Acknowledgments
The authors thank Lisa Denny, PhD, and Natalia Zhukovskaya, PhD, of ICON plc (Blue Bell, PA, USA) for medical writing support, which was funded by Alcon Vision LLC.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was funded by Alcon Vision LLC. Alcon assisted with the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, and approval of the manuscript.
Disclosure
Dr Hiroko Bissen-Miyajima received grants and research support from Alcon, Johnson & Johnson Vision, and HOYA, and is a consultant for Alcon, Johnson & Johnson Vision, BVI, and Zeiss. Dr Yuka Ota, Dr Saori Yaguchi, and Dr Kunihiko Nakamura received grants and research support from Alcon Vision LLC, Johnson & Johnson Vision, and HOYA. Noriyuki Sasaki is an employee of Alcon Japan Ltd. The authors report no other conflicts of interest in this work.
References
1. Galvis V, Escaf LC, Escaf LJ, et al. Visual and satisfaction results with implantation of the trifocal Panoptix® intraocular lens in cataract surgery. J Optom. 2022;15(3):219–227. doi:10.1016/j.optom.2021.05.002
2. Ang RET. Long-term trifocal toric intraocular lens outcomes in Asian eyes after cataract surgery. J Cataract Refract Surg. 2023;49(8):832–839. doi:10.1097/j.jcrs.0000000000001195
3. Niazi S, Gatzioufas Z, Dhubhghaill SN, et al. Association of patient satisfaction with cataract grading in five types of multifocal IOLs. Adv Ther. 2023;41(1):231–245. doi:10.1007/s12325-023-02698-5
4. Tan N, Zheng D, Ye J. Comparison of visual performance after implantation of 3 types of intraocular lenses: accommodative, multifocal, and monofocal. Eur J Ophthalmol. 2014;24(5):693–698. doi:10.5301/ejo.5000425
5. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;12(12):CD003169. doi:10.1002/14651858.CD003169.pub4
6. Hayashi K, Yoshida M, Igarashi C, Hirata A. Effect of refractive astigmatism on all-distance visual acuity in eyes with a trifocal intraocular lens. Am J Ophthalmol. 2021;221:279–286. doi:10.1016/j.ajo.2020.07.051
7. Singh A, Pesala V, Garg P, Bharadwaj SR. Relation between uncorrected astigmatism and visual acuity in pseudophakia. Optom Vis Sci. 2013;90(4):378–384. doi:10.1097/OPX.0b013e318288afb5
8. Ang RE. Comparison of tolerance to induced astigmatism in pseudophakic eyes implanted with small aperture, trifocal, or monofocal intraocular lenses. Clin Ophthalmol. 2019;13:905–911. doi:10.2147/OPTH.S208651
9. Carones F. Residual astigmatism threshold and patient satisfaction with bifocal, trifocal and extended range of vision intraocular lenses (IOLs). Open J Ophthalmol. 2017;7(1):1–7. doi:10.4236/ojoph.2017.71001
10. Sawada A, Tomidokoro A, Araie M, Iwase A, Yamamoto T. Refractive errors in an elderly Japanese population: the Tajimi study. Ophthalmology. 2008;115(2):363–370.e363. doi:10.1016/j.ophtha.2007.03.075
11. Asano K, Nomura H, Iwano M, et al. Relationship between astigmatism and aging in middle-aged and elderly Japanese. Jpn J Ophthalmol. 2005;49(2):127–133. doi:10.1007/s10384-004-0152-1
12. Hao J, Tan LZ, Li L, et al. Comparison of visual quality in cataract patients with low astigmatism after ART2 or ReSTOR intraocular lens implantation. Int J Ophthalmol. 2019;12(3):424–428. doi:10.18240/ijo.2019.03.12
13. Orts-Vila P, Aguilar-Corcoles S, Tello-Elordi C, et al. Trifocal toric intraocular lenses in eyes with low amount of corneal astigmatism. Int J Ophthalmol. 2020;13(10):1567–1573. doi:10.18240/ijo.2020.10.09
14. Levitz L, Reich J, Roberts K, Hodge C. Evaluation of toric intraocular lenses in patients with low degrees of astigmatism. Asia Pac J Ophthalmol. 2015;4(5):245–249. Available from: https://oce.ovid.com/journals/apjoo/201509000/01599573-201509000-00002.
15. Gundersen KG, Potvin R. Comparing visual acuity, low contrast acuity and refractive error after implantation of a low cylinder power toric intraocular lens or a non-toric intraocular lens. Clin Ophthalmol. 2020;14:3661–3666. doi:10.2147/OPTH.S281178
16. Bissen-Miyajima H, Ota Y, Hayashi K, Igarashi C, Sasaki N. Results of a clinical evaluation of a trifocal intraocular lens in Japan. Jpn J Ophthalmol. 2020;64(2):140–149. doi:10.1007/s10384-019-00712-4
17. Bissen-Miyajima H, Hayashi K, Hirasawa M, et al. Clinical results of tinted aspherical multifocal IOL with +2.5 diopter near add power SN6AD2 (SV25T0). Nippon Ganka Gakkai Zasshi. 2015;119(8):511–520.
18. Bissen-Miyajima H, Hayashi K, Yoshino M, Nakamura K, Yoshida M. Clinical results of +3.0 diopter near add power multifocal intraocular lens for eyes following cataract extraction. Atarashii Ganka. 2010;27:1737–1742.
19. Holladay JT, Pettit G. Improving toric intraocular lens calculations using total surgically induced astigmatism for a 2.5 mm temporal incision. J Cataract Refract Surg. 2019;45(3):272–283. doi:10.1016/j.jcrs.2018.09.028
20. Holladay JT. Calculation of total surgically induced astigmatism with a toric intraocular lens. J Cataract Refract Surg. 2020;46(5):793–794. doi:10.1097/j.jcrs.0000000000000124
21. Holland E, Lane S, Jd H, et al. The AcrySof Toric intraocular lens in subjects with cataracts and corneal astigmatism: a randomized, subject-masked, parallel-group, 1-year study. Ophthalmology. 2010;117(11):2104–2111. doi:10.1016/j.ophtha.2010.07.033
22. Bauer NJ, de Vries NE, Webers CA, Hendrikse F, Nuijts RM. Astigmatism management in cataract surgery with the AcrySof Toric intraocular lens. J Cataract Refract Surg. 2008;34(9):1483–1488. doi:10.1016/j.jcrs.2008.05.031
23. Kessel L, Andresen J, Tendal B, et al. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123(2):275–286. doi:10.1016/j.ophtha.2015.10.002
24. Koh S, Maeda N, Ogawa M, et al. Fourier analysis of corneal irregular astigmatism due to the anterior corneal surface in dry eye. Eye Contact Lens. 2019;45(3):188–194. doi:10.1097/ICL.0000000000000559
25. Epitropoulos AT, Matossian C, Berdy GJ, Malhotra RP, Potvin R. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41(8):1672–1677. doi:10.1016/j.jcrs.2015.01.016
26. Hashemi H, Fotouhi A, Yekta A, et al. Global and regional estimates of prevalence of refractive errors: systematic review and meta-analysis. J Curr Ophthalmol. 2018;30(1):3–22. doi:10.1016/j.joco.2017.08.009
27. Miki A, Fuse N, Fujimoto S, et al. Prevalence, associated factors, and inter-eye differences of refractive errors in a population-based Japanese cohort: the Tohoku Medical Megabank Eye Study. Ophthalmic Epidemiol. 2023;31(1):46–54 doi:10.1080/09286586.2023.2203226.
28. Hayashi K, Sasaki H, Hirata A, Yoshimura K. Comparison of long-term astigmatic changes following cataract surgery among types of corneal astigmatism. Br J Ophthalmol. 2022;107(7):920–926. doi:10.1136/bjophthalmol-2021-321026
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.