")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Comparison of the Accuracy of HSV1 and HSV2 Antibody Tests with PCR in the Diagnosis of Recurrent Genital Herpes
Authors Deng J, Ye YJ, Chen QP, Zhang YJ, Liu JF
Received 21 March 2024
Accepted for publication 31 July 2024
Published 23 August 2024 Volume 2024:17 Pages 1887—1893
DOI https://doi.org/10.2147/CCID.S470020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Jia Deng, Yu-Jian Ye, Qiu-Ping Chen, Yi-Jin Zhang, Ji-Feng Liu
Department of Dermatology, Hangzhou Third People’s Hospital, Hangzhou, People’s Republic of China
Correspondence: Ji-Feng Liu, Department of Dermatology, Hangzhou Third People’s Hospital, No. 38 of West Lake Road, Shangcheng District, Hangzhou, Zhejiang, 310009, People’s Republic of China, Tel/Fax +86 0571-87827514, Email [email protected]
Objective: To assess the accuracy of HSV1and HSV2 antibody testing in identifying genital herpes infection.
Methods: A cohort of 299 patients previously diagnosed with recurrent genital herpes, confirmed via PCR, were tested using ELISA for HSV1 and HSV2 IgM and IgG antibodies. The study compared the accuracy of HSV1 and HSV2 antibody tests in diagnosing genital herpes.
Results: Among 299 patients, 14 tested positives for HSV1 DNA. Of these, 9 had HSV1 IgG antibodies, but none had HSV2 IgG antibody. Among 278 patients with HSV2 DNA, 149 had HSV1 IgG, 9 had HSV2 IgG, and 97 had both. Seven patients had both HSV1 and HSV2 DNA; 3 had HSV1 IgG, 1 had HSV2 IgG, and 3 had both. The accuracy of HSV1 IgG for HSV1 infection was 64.2%, and for HSV1 and HSV2 co-infection, 85.7%. The accuracy of HSV2 IgG for HSV2 infection was 38.1%, and for HSV1 and HSV2 co-infection, 57.1%. The combined antibody positivity accuracy was 34.9%.
Conclusion: Genital herpes is primarily caused by HSV2 (92.98%). A smaller percentage is HSV1 (4.67%) or co-infection (2.34%). Despite relatively low diagnostic accuracy (34.9– 85.7%) for antibody detection, combined antibody testing is necessary. Herpes DNA testing is recommended for accurate diagnosis. Absence of antibodies does not rule out genital herpes and clinical assessment is essential.
Keywords: antibody test, DNA test, genital herpes, HSV-1, HSV-2
Introduction
Genital herpes (GH) is a sexually transmitted infection characterized by recurring outbreaks, predominantly affecting the genital region and adjacent skin and mucous membranes. In the United States, about 1 in every 6 people ages 14 to 49 has genital herpes, the positivity rate of herpes antibody testing can be influenced by factors such as the timing of the test relative to infection onset, individual immune response variability, and potential genetic mutations affecting antibody production. GH is caused by the herpes simplex virus (HSV), which can be classified into HSV-1 and HSV-2 serotypes. GH is predominantly attributed to HSV-2 infection; however, the annual incidence of GH induced by HSV-1 infection is on the rise, correlating with shifts in sexual behavior.1 Since the latent infection of HSV cannot be completely eliminated from the body at present, the disease duration is protracted and the disease tends to relapse, causing great suffering to patients. GH-induced genital ulcers significantly increase the transmission of syphilis and human immunodeficiency viruses (HIV),2,3 and HSV has a synergistic pathogenic effect with HIV.4 Female patients have an increased risk of developing cervical cancer, and HSV infection during pregnancy carries the possibility of fetal malformations. Newborns can be infected with the virus during delivery and develop diseases, such as herpesvirus encephalitis, resulting in disability or death.5 Therefore, GH is a public health concern that seriously threatens the health of patients, and requires accurate diagnosis and standardized treatment.
Currently, the laboratory diagnosis of GH primarily involves virus culture, serum antibody testing, antigen testing, and polymerase chain reaction (PCR). The operability, periodicity, positivity rate, and sensitivity of different assays vary. Among these methods, herpes virus antibody testing is convenient and fast. It can be used for epidemiological investigation of asymptomatic patients and has a wide range of clinical applications. It is recommended to conduct tests that can differentiate between HSV1 and HSV2 infections, as patients infected with different types of HSV have varying prognoses and require different follow-up measures.6 Antibodies against structural glycoprotein G (gG-1 in HSV-1 and gG-2 in HSV-2) are used clinically for serotyping.7 Nevertheless, the positivity rate for HSV-2 detection is comparatively low. Van Rooijen et al6 reported a positivity rate of 69.70% for HSV-2 antibody; however, the number of cases is relatively small, only 33 individuals. Hence, we included a cohort of 299 patients with recurrent GH who exhibited positive results in HSV DNA testing. Subsequently, these patients were assessed for the presence of HSV1 and HSV2 IgG antibodies.
By comparing the accuracy of HSV1 and HSV2 IgG antibody tests with DNA test by fluorescence quantitative PCR, this study seeks to provide a more comprehensive understanding of the diagnostic efficacy of these tests in a clinical setting. The significance of this research lies in its potential to enhance the diagnostic approach for GH, ensuring timely and accurate identification of HSV1 and HSV2 infections. This is crucial for implementing appropriate treatment strategies, reducing the transmission risk of associated infections, and improving patient outcomes. Additionally, understanding the diagnostic accuracy of antibody testing can guide future developments in GH diagnostic protocols, contributing to better disease management and patient care.
Patients and Methods
General Data
A total of 299 patients diagnosed with recurrent genital herpes (GH), treated at the Department of Venereal Diseases of our hospital between October 2019 and April 2023, were included in this study. These patients exhibited distinct clinical features, including erythematous blisters, and experienced recurrent episodes exceeding three occurrences, meeting the diagnostic criteria outlined by the National Health and Family Planning Commission of the People’s Republic of China.
Inclusion criteria: Patients exhibited typical clinical manifestations of genital herpes such as erythema and vesicles, had experienced three or more recurrences, age from 19 to 79 years old. The cohort included 181 males and 118 females. Exclusion criteria: Patients with autoimmune diseases such as lupus erythematosus and dermatomyositis, malignant tumors, syphilis, HIV antibody positivity, or those who had used immunosuppressive agents within the past three months were excluded. All patients signed informed consent forms, and this study was reviewed by the Hangzhou Third People’s Hospital ethics committee and approved. Laboratory Methods: fluorescence quantitative PCR diagnostic Kit for HSV1,2 was purchased from Beijing Bohui Innovation Biotechnology Group Co., Ltd. PCR was performed using Thermofisher ABI 7500. Herpes simplex virus type antibody assay kit (enzyme-linked immunosorbent assay) was purchased from Zhenzhou Auto Bioengineering Co., Ltd., ELISA was conducted using the Addcare ELISA 600 microplate reader from Yantai Addcare Bio-Tech Limited Company.
Specimen Collection: Genital herpes vesicles were disinfected with iodophor, then punctured using a sterile swab to collect vesicular fluid, which was stored at −80°C for PCR detect. Simultaneously, 5 mL of peripheral venous blood was collected with EDTA anticoagulant. The serum was separated and stored at −80°C for HSV antibody test.
Experimental Methods
HSV DNA Typing Test
DNA isolation was carried out following the instructions provided in the kit. Following this, 5μL each of the negative control, DNA from the sample to be tested, and the positive control were introduced into the PCR reaction tube containing the prepared reagent. The tube was tightly sealed and subjected to centrifugation at a low speed. For detection, the HSV1 channel was marked as JOE (utilizing 4’,5’-dichloro-2’,7’-dimethoxyfluorescein), the HSV2 channel as FAM (employing carboxyfluorescein), and the internal control channel as ROX (using carboxy-X-Rhodamine). The reaction conditions for the enzyme uracil-N-glycosylase (UNG) were as follows: the enzyme reaction was carried out at 37 °C for 300 seconds; a pre-denaturation step at 95 °C for 300 seconds; a denaturation step at 95 °C for 10 seconds; and annealing, elongation, and fluorescence detection at 60 °C for 50 seconds. This entire process was repeated for 45 cycles. The interpretation of results was based on the CT values obtained.
HSV Serum Antibody Typing Test
A designated number of precoated wells were counted, leaving one well vacant. Subsequently, 100 uL of the negative control was introduced into three wells, while 100 uL of the positive control was added to two wells. The remaining wells received 100 uL of sample diluent. Lastly, 10 uL of the test sample was added to the wells containing the sample diluent. The liquid in the wells was gently agitated to achieve uniform mixing, followed by affixing the microplate sealers. The mixture was then incubated in a 37 °C water bath for 45 minutes. Following this, a microplate washer was employed for six wash cycles, and the plate was subsequently dried on absorbent paper. Following these steps, 100uL of enzyme conjugate was added to each well, excluding the empty well. The microplate sealers were then affixed, and the mixture was incubated in a 37 °C water bath for 45 minutes. The process was reiterated by repeating step 3. Subsequently, 50 uL of each of the substrate solution and chromogenic solution were added to each well, gently shaken to ensure even mixing, and placed in a light-free environment at 37 °C for 10 minutes. Finally, 50 uL of stop solution was added, shaken thoroughly, and the HSV serum antibody typing test was performed immediately. The absorbance value of each well was assessed at a single wavelength of 450 nm using a microplate reader. A zero setup was performed utilizing the empty well, and the absorbance value for each well was determined. Subsequently, the absorbance value of each well was determined at a double wavelength of 450/(620–630) nm.
Calculation of Results: The cut-off value is determined by adding 0.1 to the average optical density (OD) value of the negative control. Should the OD value of the negative control be lower than 0.05, it is to be considered as 0.05 for calculation purposes.
Assessment of Validity: A valid result is indicated by an OD value of the positive control that is equal to or greater than 0.7, and an OD value of the negative control that is equal to or less than 0.1.
Statistical Analysis
Statistical analysis was performed using SPSS version 24.5. The t-test was employed for analyzing measured data, while the chi-squared test was utilized for counting data. P < 0.05 was considered as statistical significance.
Results
Among the 299 patients with recurrent GH, 181 individuals were male with an average age of 43.71±12.35 years old, and 118 individuals were female with an average age of 42.12±12.87 years old. There was no significant difference in age between male and female (t = 1.07, P > 0.05).
Moreover, among the diagnosed cases, 14 patients were HSV1 infection, 278 patients were HSV2 infection, and 7 patients were HSV1 and HSV2 co-infection. Notably, HSV2 infection predominated in both male and female groups, with a relatively smaller number of patients diagnosed with HSV1 infection and HSV1 and HSV2 co-infection. There was no significant difference in HSV1, HSV2, and HSV1, 2 co-infection between male and female groups (Table 1).
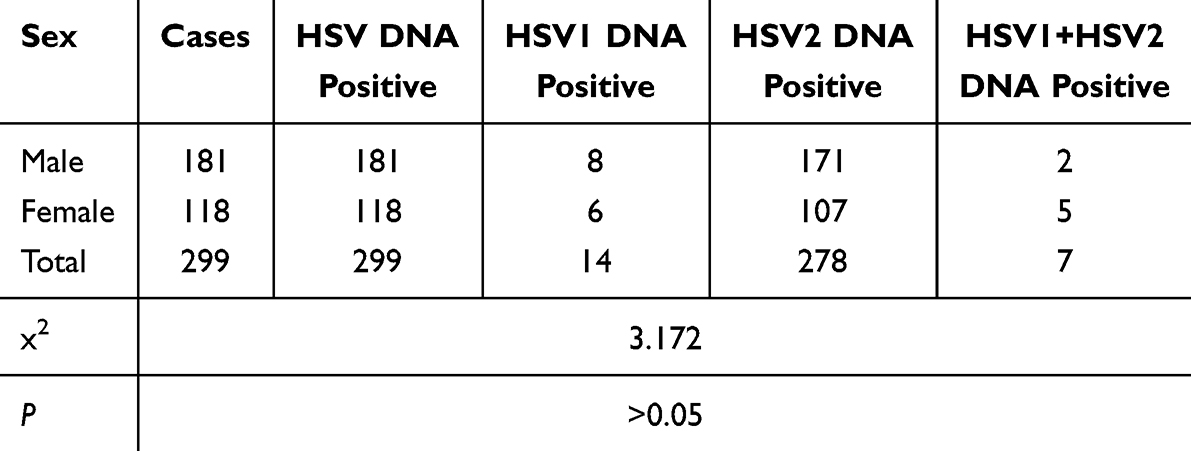 |
Table 1 Comparison of Positive DNA Test Results in Male and Female Patients with Genital Herpes |
In the study, 161 patients tested positive for HSV1 IgG antibody, 10 tested positive for HSV2 IgG antibody, and 100 tested positive for both HSV1 and HSV2 IgG antibodies. Patients demonstrating positive HSV1 antibody and being doubly positive for both HSV1 and HSV2 antibodies were prevalent in both male and female groups, while a limited number of patients tested positive for HSV2 antibody. There was no significant difference in positive cases with different HSV antibodies between male and female groups (Table 2).
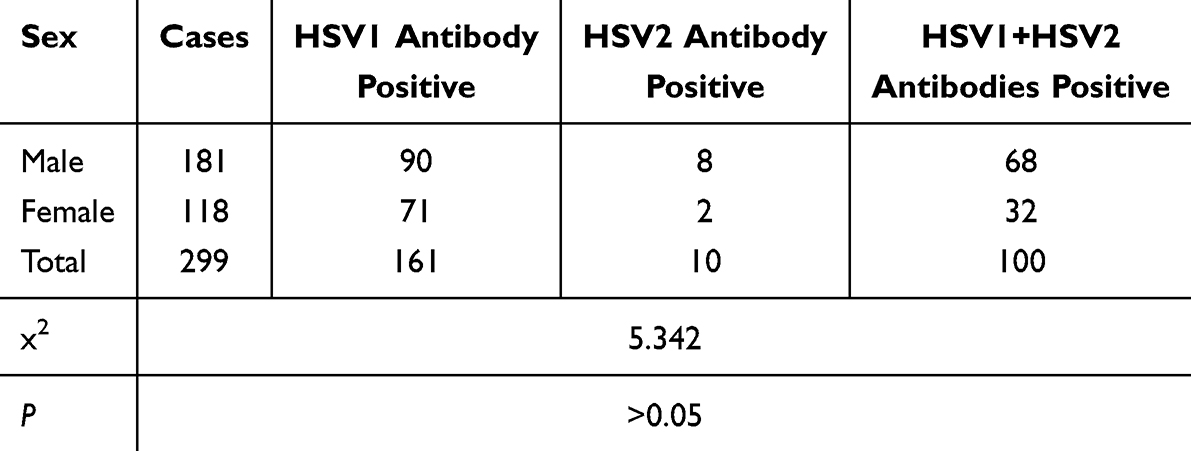 |
Table 2 Comparison of Positive Antibody Test Results in Male and Female Patients with Genital Herpes |
Out of the 14 patients diagnosed with HSV1 infection, 9 tested positive for HSV1 IgG antibody. None of them exhibited positive results for HSV2 IgG antibody or a combination of HSV1 and HSV2 IgG antibodies. The positive antibody among this group was 64.2%. Among the 278 patients diagnosed with HSV2 infection, 149 were positive for HSV1 IgG antibody, 9 were positive for HSV2 IgG antibody, and 97 were doubly positive for HSV1 and HSV2 IgG antibodies. The positive rate was 38.1% for HSV2 IgG antibody. Among the patients diagnosed with HSV1 and HSV2 co-infection, 3 were positive for HSV1 IgG antibody, 1 was positive for HSV2 IgG antibody, and 3 were double positive for HSV1 and HSV2 IgG antibodies (Table 3).
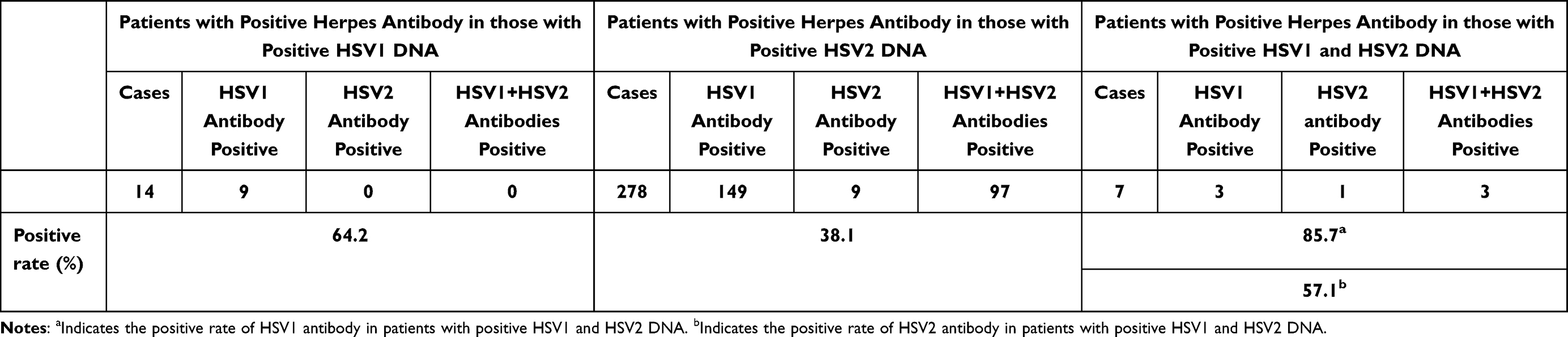 |
Table 3 Comparison of Positive DNA and Antibody Test Results in 299 Patients with Genital Herpes |
Discussion
At present, laboratory diagnosis of GH primarily includes virus isolation and culture, Western blot detection, antibody detection and fluorescence quantitative PCR detect. Isolation and culture of HSV from skin lesions or blisters are the gold standard for detection. However, the experimental conditions of HSV culture are stringent, and the procedure is cumbersome and time-consuming, hence it is only used in scientific research. Direct immunofluorescence is a rapid and cost-effective method, providing results within a few hours. However, it necessitates the collection of fluid from the blister and employs fluorescence microscopy, making it particularly suitable for detection in patients exhibiting typical clinical symptoms. PCR can serve as a diagnostic tool for detecting HSV infection in both skin lesions and the central nervous system. Its sensitivity for virus detection surpasses that of viral culture by more than fourfold, particularly in skin lesions with low viral content like erosions and scabs.7 Additionally, PCR can be employed for typing purposes. However, a PCR machine is required, and the process is more complex and demanding. At present, serum antibody detection remains the primary method of clinical diagnosis, especially when there are no blisters and skin erosions. Nevertheless, in the early stage of HSV infection, there are no antibodies against the virus in the serum. Alternatively, the immune function of the body is compromised, which cannot produce detectable antibodies, or the amount of antibody is very low in the body, leading to false negative results. Mutation in gG-2 gene may also result in negative HSV2 antibody test results.8 Among the 299 patients with recurrent GH in this study, 14 were infected with HSV1, 278 were infected with HSV2, and 7 were co-infected with HSV1 and HSV2. This prevalence is significantly lower than the reported rates of 37% in Canada9 and 72% in New Zealand.10 The observed prevalence aligns with the traditional sexual behavior patterns observed in China.
The positive rate of HSV1 antibody detection was relatively high. However, out of the 299 patients with recurrent GH, only 21 had HSV1 infection, either alone or in combination with HSV2. While 261 patients had positive HSV1 antibody detection, including double positivity for HSV1 and HSV2 antibodies. The diagnostic accuracy of GH caused by HSV1 infection was only 8.05%, with a high false positive rate. According to Wald,11 HSV-1 antibody testing is ineffective in the diagnosis of GH due to the high seroprevalence of HSV-1 in the general population. In our study, 285 patients were diagnosed with HSV2, which includes cases of both HSV1 and HSV2 co-infection. Moreover, 110 patients showed positive results for HSV2 antibodies, and among them, a subset demonstrated double positivity for both HSV1 and HSV2 antibodies, yielding an overall accuracy of 36.45%. This accuracy is obviously lower than the 69.7% reported by van Rooijen6 and the 82.6% reported by Summerton.12 These discrepancies may be attributed to variations in patient populations, testing methodologies, and the sensitivity of the diagnostic kits used. Our findings indicate it is necessary to improve the diagnosis accuracy of HSV infection.
From a clinical perspective, the relatively low diagnostic accuracy of antibody testing for GH, especially for HSV1, suggests that relying solely on serological tests could lead to misdiagnosis and inadequate patient management. This could result in inappropriate treatment strategies and persistent transmission of the virus. Therefore, incorporating molecular biological detection methods such as PCR, despite their complexity and cost, could enhance diagnostic precision and improve patient outcomes.
In terms of public health implications, our study reinforces the need for comprehensive diagnostic approaches to manage GH effectively. Accurate identification of HSV types is crucial for epidemiological surveillance, guiding public health interventions, and formulating targeted prevention strategies. The high seroprevalence of HSV1 and the increasing incidence of HSV1-induced GH emphasize the importance of continuous monitoring and updating diagnostic criteria to reflect current epidemiological trends. Overall, our findings advocate for a multifaceted diagnostic strategy combining serological and molecular methods to achieve accurate and timely detection of GH, ultimately benefiting clinical practice and public health efforts.
Limitations of this study include a relatively modest sample size and a focus on a single geographic region, which may limit the generalizability of the findings. Additionally, the reliance on antibody testing may not capture all cases of genital herpes, particularly in the early stages of infection or in individuals with compromised immune systems. Furthermore, the study did not account for potential mutations in the gG-2 gene, which could affect HSV2 antibody test results.
Our findings underscore the importance of using a combination of diagnostic methods, including fluorescence quantitative PCR detect for HSV DNA, to ensure accurate diagnosis and appropriate treatment. For future research, it is recommended to conduct larger, multicenter studies to validate these results and explore the impact of genetic mutations on diagnostic accuracy. Additionally, developing more sensitive and specific antibody tests could improve the early detection of genital herpes.
Conclusion
In summary, the diagnostic accuracy of HSV2 IgG antibodies in GH is relatively low, and the rate of false negatives is high. Hence, negative results in antibody tests do not conclusively exclude the presence of GH. Additionally, a minority of GH cases may be attributed to HSV1 infection. Therefore, if feasible, it is recommended to employ fluorescence quantitative PCR detection for HSV1 and HSV2 DNA. Factors such as the timing of serological specimen collection and patient immune status can significantly influence the results. To improve positivity rates, specimens should be collected at optimal times, and a combination of diagnostic methods should be utilized.
Abbreviations
GH, genital herpes; HSV, herpes simplex virus; PCR, Polymerase Chain Reaction; ABI, Applied Biosystems, Inc.; ELISA, Enzyme-Linked Immunosorbent Assay; DNA, Deoxyribo Nucleic Acid; UNG, uracil-N-glycosylase; IgG, immunoglobulin G.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Hangzhou Third People’s Hospital. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
No external funding received to conduct this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jama M, Mair Owen E, Nahal B, Obasi A, Emily Clarke T. Twenty years of herpes simplex virus type 2 (HSV-2) research in low-income and middle-income countries: systematic evaluation of progress made in addressing WHO prioritiesfor research in HSV-2 epidemiology and diagnostics. BMJ Glob Health. 2024;9(7):e012717. doi:10.1136/bmjgh-2023-012717
2. Tuddenham S, Ghanem KG. Management of adult syphilis: key questions to inform the 2021 centers for disease control and prevention sexually transmitted infections treatment guidelines. Clin Infect Dis. 2022;74(Suppl_2):S127–S133. doi:10.1093/cid/ciac060
3. Johnston C. Diagnosis and management of genital herpes: key questions and review of the evidence for the 2021 centers for disease control and prevention sexually transmitted infections treatment guidelines. Clin Infect Dis. 2022;74(Suppl_2):S134–S143. doi:10.1093/cid/ciab1056
4. Glynn JR, Biraro S, Weiss HA. Herpes simplex virus type 2: a key role in HIV incidence. AIDS. 2009;23(12):1595–1598. doi:10.1097/QAD.0b013e32832e15e8
5. Ehsanipoor RM, Major CA. Herpes simplex and HIV infections and preterm PROM. Clin Obstet Gynecol. 2011;54(2):330–336. doi:10.1097/GRF.0b013e318217d7a6
6. van Rooijen MS, Roest W, Hansen G, Kwa D, de Vries HJ. False-negative type-specific glycoprotein G antibody responses in STI clinic patients with recurrent HSV-1 or HSV-2 DNA positive genital herpes, The Netherlands. Sex Transm Infect. 2016;92(4):257–260. doi:10.1136/sextrans-2015-052213
7. Johnston C, Corey L. Current concepts for genital herpes simplex virus infection: diagnostics and pathogenesis of genital tract shedding. Clin Microbiol Rev. 2016;29(1):149–161. doi:10.1128/CMR.00043-15
8. Daikoku T, Horiba K, Kawana T, Hirano M, Shiraki K. Novel deletion in glycoprotein G forms a cluster and causes epidemiologic spread of herpes simplex virus type 2 infection. J Med Virol. 2013;85(10):1818–1828. doi:10.1002/jmv.23668
9. Dabestani N, Katz DA, Dombrowski J, Magaret A, Wald A, Johnston C. Time trends in first-episode genital herpes simplex virus infections in an urban sexually transmitted disease clinic. Sex Transm Dis. 2019;46(12):795–800. doi:10.1097/OLQ.0000000000001076
10. AlMukdad S, Farooqui US, Harfouche M, Aldos L, Abu-Raddad LJ. Epidemiology of herpes simplex virus type 2 in Canada, Australia, and new Zealand: systematic review, meta-analyses, and meta-regressions. Sex Transm Dis. 2022;49(6):403–413. doi:10.1097/OLQ.0000000000001612
11. Wald A, Ashley-Morrow R. Serological testing for herpes simplex virus (HSV)-1 and HSV-2 infection. Clin Infect Dis. 2002;35(Suppl 2):S173–S182. doi:10.1086/342104
12. Summerton J, Riedesel M, Laeyendecker O, et al. Effect of sexually transmitted disease (STD) coinfections on performance of three commercially available immunosorbent assays used for detection of herpes simplex virus type 2-specific antibody in men attending Baltimore, Maryland, STD clinics. Clin Vaccine Immunol. 2007;14(12):1545–1549. doi:10.1128/CVI.00120-07
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.