")
Back to Journals » Clinical Optometry » Volume 16
Digital Challenges: Investigating Computer Vision Syndrome in Thai Esports Through a Case-Control Approach
Authors Chaiwiang N , Koo-akarakul J
Received 22 January 2024
Accepted for publication 15 July 2024
Published 29 July 2024 Volume 2024:16 Pages 201—210
DOI https://doi.org/10.2147/OPTO.S460868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Mr Simon Berry
Narttaya Chaiwiang, Juthamanee Koo-akarakul
Department of Optometry, Ramkhamhaeng University, Bangkok, Thailand
Correspondence: Juthamanee Koo-akarakul, Department of Optometry, Ramkhamhaeng University, Bangkok, 10240, Thailand, Email [email protected]
Purpose: To determine the factors associated with eyestrain in esports athletes in Bangkok compared with controls.
Patients and Methods: A cross-sectional descriptive study was conducted between April and June 2023, involving 160 male participants (aged 20– 35 years) who used digital devices, consisting of esports athletes and a control group. Data were collected using a general information questionnaire, Computer Vision Syndrome Questionnaire (CVS-Q), and Depression anxiety stress scale-21 (DASS-21). Ophthalmic instruments were used for the eye examinations by an optometrist.
Results: Seventy-six esports athletes showed significantly lower visual performance than controls in logMAR visual acuity (p < 0.020), phoria (p < 0.001), negative fusional vergence (blur, break, and recovery) (p < 0.012, p < 0.004 and p < 0.039), positive fusional vergence (blur, break, and recovery) (p < 0.005, p < 0.001 and p < 0.005), monocular estimation method (p < 0.001), monocular and binocular accommodative facility (p < 0.001), and vergence facility (p < 0.001). A study on risk factors for CVS found that esports athletes were significantly more likely to have CVS (p < 0.001). Work environments with high-intensity lighting significantly increase the risk of CVS compared to low-intensity lighting (p < 0.001). The use of a digital device for > 4 h/day, having a history of alcohol consumption, and stress significantly increased the risk of CVS (p < 0.001, p < 0.023, p < 0.048).
Conclusion: This study found that esports athletes experienced vision health problems, indicating the need to prevent eyestrain caused by the use of digital devices.
Keywords: esports athlete, eyestrain, CVS-Q, digital devices, visual performance
Introduction
Electronic sports, commonly referred to as esports, are competitive video gaming conducted over the Internet, where participants often collaborate in teams to strategize and defeat their rivals. Esports has earned recognition as a form of “virtual sport”, with participants being called “esports athletes” or “esports players”.1 Nowadays, esports competitions are captivating a broad age range, especially the younger demographic,2 driven by perceived benefits, such as career opportunities and increased earnings. As a result, a segment of enthusiasts aims for a professional status as an esports athlete. Industries worldwide, particularly in the United States, Europe, and Asia, are investing in advanced technologies to enhance online gaming experiences and entertain esports players, thus nourishing the sector’s sustained growth and exponential economic success.3
However, devoting oneself to a career as a professional esports athlete can lead to various health challenges owing to the extensive hours dedicated to honing their skills. A survey across nine universities in the United States and Canada found that the majority practiced for 3–10 hours daily. Health issues included 56% experiencing eye fatigue, 42% back and neck pain, 36% reporting wrist pain, and 32% facing hand pain. Additionally, nearly 40% of participants reported inadequate physical exercise, with only 2% actively monitoring and caring for their health.4 Prior research has shown that the foremost health conditions faced by esports athletes in the United States and Canada involve ocular problems. Extensive digital device usage is a well-established risk factor for computer vision syndrome (CVS).5 Since esports athletes require digital devices for training, they are likely to develop CVS as well.
Internet Gaming Disorder (IGD) is characterized by a loss of control over online or offline gaming, prioritizing it above other activities, and continuing to play despite negative consequences for at least a year. To further manage this condition, IGD is included in both the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and the International Classification of Diseases (ICD-11).6 Surveys suggest a higher prevalence of gaming disorders or addiction among young people in Asian countries (10–15%) compared to Western countries (1–10%).7 While IGD can lead to physical problems like dry eyes and digital eyestrain (DES) from prolonged screen time,8–10 it can also cause mental health issues like anxiety and depression.11 It is important to note that while IGD research provides valuable insights, esports has gained recognition as a legitimate sport with different training structures and demands compared to unrestricted gaming habits. Given the similarities in intense gaming habits between those with IGD and esports athletes, we also aimed to explore the mental health of Thai esports athletes, which remains a limited study in this field.12
Although eyestrain has been identified as a prominent symptom, investigations into the health of esports athletes, specifically regarding eye health, remain limited in Thailand. Hence, this paper aims to meticulously examine the ocular and visual characteristics of esports athletes, with the goal of enhancing ocular health and preventing visual complications among this unique group.
Materials and Methods
Study Sources and the Population
A cross-sectional descriptive study was conducted among a specific group of esports athletes (n = 80) in Bangkok and compared with a control group (n = 80) from April to June 2023. A total of 160 male participants aged 20–35 years who used digital devices participated in this study. The esports athletes were male, aged 20–35 years old, and registered by the Thailand Esports Federation in 2023, practicing for competing in professional competitions. The control group were male, aged 20–35 years old, with corrected visual acuity of 20/25 or better, uses digital devices, and not working as esports athletes or gamers who play to entertain an audience (eg streamers, gaming entertainers, online gaming performers). Four esports athletes and six controls were excluded from this study by having a history of systemic diseases, ocular diseases (including trauma, surgery, or inflammation), use of medications potentially causing CVS, or reported dry eye symptoms (as a known CVS symptom).13–15 The study comprised two parts: a questionnaire and ophthalmic examinations conducted by an optometrist.
Surveys and Questionnaires
A survey questionnaire, including the general information questionnaire, Computer Vision Syndrome Questionnaire (CVS-Q), and Depression anxiety stress scale-21 (DASS-21), was used to identify the factors associated with eyestrain. The Wangsan et al16 adaptation of the Computer Vision Syndrome Questionnaire (CVS-Q), originally developed by del Mar Seguí et al17 was used in this study. This version, validated for the Thai population, was chosen for its language suitability and established reliability for our participants. Diagnosis of CVS was based on a sum score of ≥6 on the CVS-Q. The Thai version of the DASS-21 was developed by Oei et al18 from the National Center for HIV Epidemiology and Clinical Research (NCHECR) of Australia. This questionnaire contains 21 items and is designed to quantitatively measure the negative emotional states of depression (items 3, 5, 10, 13, 16, 17, and 21), anxiety (items 2, 4, 7, 9, 15, 19, and 20), and stress (items 1, 6, 8, 11, 12, 14, and 18) with scoring from 0 to 3 for all participants.19 The interpreting DASS-21 score for negative emotional states of depression was rated on a five-point scale ranging from 0 to 4 (normal), to 5–6 (little), to 7–10 (moderate), to 11–13 (severe), and 14 or more (very severe). The anxiety interpretation of the DASS-21 is also divided into five levels: 0–3 (normal), 4–5 (little), 6–7 (moderate), 8–9 (severe), and 10 or more (very severe). The evaluation of stress using the DASS-21 consists of: 0–7 (normal), 8–9 (little), 10–12 (moderate), 13–16 (severe), and 17 or more (very severe).
Ophthalmic Examination
The participants underwent a comprehensive eye examination, including assessment of visual acuity at a distance using the Early Treatment of Diabetic Retinopathy Study (ETDRS) chart, with outcomes recorded in logMAR units, as well as refraction procedures and screening for ocular disease. Phoria measurements were conducted using an alternate cover test with a prism bar at both 6 m and 40 cm. The examiner alternately observed eye movements under occlusion and adjusted the power of the prism bar until no movement was detected. Recorded magnitudes of the prism with negative values indicated exophoria and positive values indicated esophoria. Near-positive (PFV) and negative fusional vergence (NFV), representing the convergence and divergence amplitudes, respectively, were assessed using a prism bar. Measurements were recorded when participants reported blurring, diplopia, and recovery (return to single vision). The convergence amplitude was evaluated using the near point of convergence (NPC) procedure by bringing the target as close as possible to the nose and recording the range where diplopia was observed. The accommodative amplitude was measured through the near point of accommodation (NPA) procedure, bringing the target as close as possible to the nose while maintaining readability of the 20/32 near visual acuity letter. The accommodative response was assessed using the monocular estimation method (MEM) technique. The accommodative facility was measured using the flipper bar with ±2.00 D lenses performed both monocularly and binocularly, as well as the vergence facility using the flipper bar with 12 BO and 3 BI prisms, performed binocularly. All the near-visual function tests were conducted at a 40 cm distance.
Ethical Approval
This study was approved by the Research Ethics Committee of the Ramkhamhaeng University (No. RU-HRE 66/0028) and adhered to the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all the participants.
Statistical Analysis
The results are expressed as mean ± standard deviation (S.D). Chi-square and Student’s t-test were used to compare between control group and esports athletes, as appropriate. All statistical significance was expressed as p-value < 0.05. Data were extracted into an Excel spreadsheet and analyzed using PASW Statistics software (version 18.0; SPSS Inc., Chicago, IL, USA).
Results
Basic Characteristics of Study Population
All participants were male (aged 20–35 years) and categorized into two groups: 76 esports athletes and 74 controls. Most of the participants had a bachelor’s degree (88.00%), followed by postgraduate degree (4.67%), associate diploma (5.33%), and secondary education (2.00%). Most participants lived in Bangkok (98.67%), were single (86.00%), did not smoke tobacco (88.67%), and drank alcohol (54.00%). Among the participants, 66.67% worked in high-intensity light environments, while 33.33% worked in low-intensity light environments. The control group comprised participants from various occupations, including office workers (32.43%), students (27.03%), business entrepreneurs (14.86%), public servants (9.46%), daily employees (6.76%), motorbike taxi drivers (4.05%), monks (2.70%), chef (1.35%) and unemployed individuals (1.35%). Most participants used digital devices continuously for more than four hours per day.
Ophthalmic Examination
Participants exhibited various refractive errors with the following distribution: 38.67% myopia, 9.33% hyperopia, 8.00% astigmatism, 41.33% myopia with astigmatism, 2.67% hyperopia with astigmatism, and 8.00% emmetropia (data not shown). Eye examination at a far distance (6 m) of the esports athletes and the control group revealed that the corrected visual acuity in logMAR units of the control group was 0.005 ± 0.027, which was statistically significant to the esports athletes for 0.013 ± 0.043 (p < 0.020). The other eye examination at near distance (40 cm) which is significantly different between esports athletes and control group, respectively, included phoria (3.556 exophoria ± 3.369∆ and 3.029 exophoria ± 5.530∆, p < 0.001), blur value of NFV (11.866 ± 4.529 and 11.972 ± 3.509, p < 0.012), break value of NFV (18.493 ± 5.841 and 19.069 ± 3.743, p < 0.004), recovery value of NFV (10.746 ± 4.128 and 12.971 ± 3.119, p < 0.039), blur value of PFV (14.032 ± 5.349 and 16.103 ± 3.959, p < 0.005), break value of PFV (21.630 ± 7.323 and 23.347 ± 4.783, p < 0.001), recovery value of PFV (12.397 ± 5.504 and 14.542 ± 4.216, p < 0.005), MEM (0.445 ± 0.415 and 0.414 ± 0.196, p < 0.001), monocular accommodative facility or MAF (12.322 ± 6.365 and 13.472 ± 2.658, p < 0.001), binocular accommodative facility or BAF (8.315 ± 6.418 and 9.611 ± 2.890, p < 0.001), and vergence facility (8.958 ± 5.413 and 12.451 ± 2.906, p < 0.001). The results not previously mentioned were found to have no significant differences between the two groups, as indicated in Table 1.
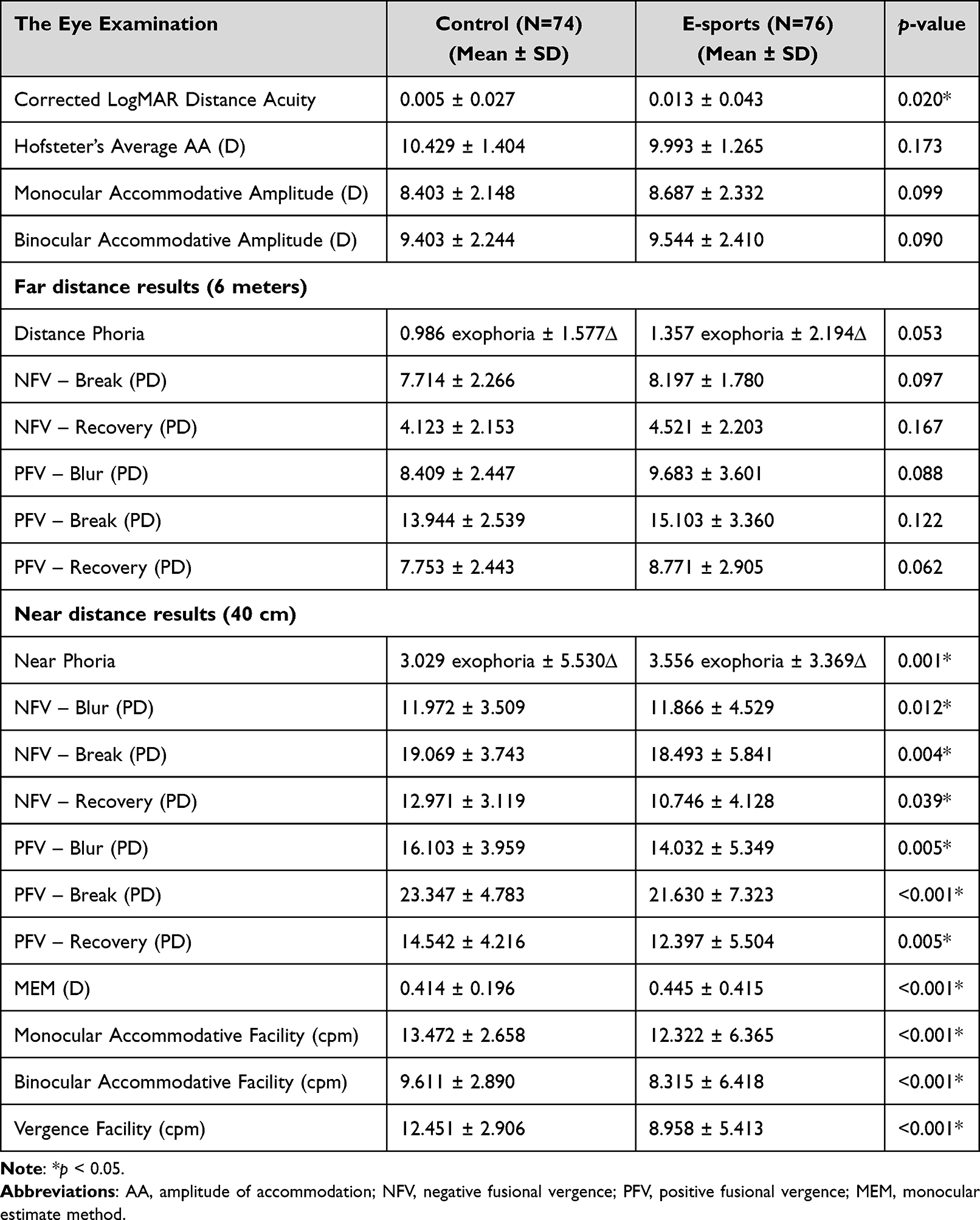 |
Table 1 The Ophthalmic Examination Results (n = 150) |
Comparison of Demographic Factors Between Esports Athletes and Control Group
Esports athletes had a significantly higher incidence of computer vision syndrome (CVS) compared to the control group (p < 0.001) and were also slightly older (28.48 ± 4.26 years and 26.95 ± 4.65 years, p < 0.040). Working in environments with high-intensity illumination was statistically significant compared to low-intensity illumination (p < 0.001). Digital device usage exceeding 4 hours daily, more common in esports athletes, was significantly different to usage under 4 hours daily (p < 0.001). Alcohol consumption also differed significantly between the two groups (p < 0.023), with esports athletes reporting higher intake. Stress levels were also significantly higher among esports athletes compared to the control group (5.80 ± 4.59 and 4.42 ± 3.85, p < 0.048). No significant differences were found between the two groups regarding medication use, smoking, depression, and anxiety (Table 2).
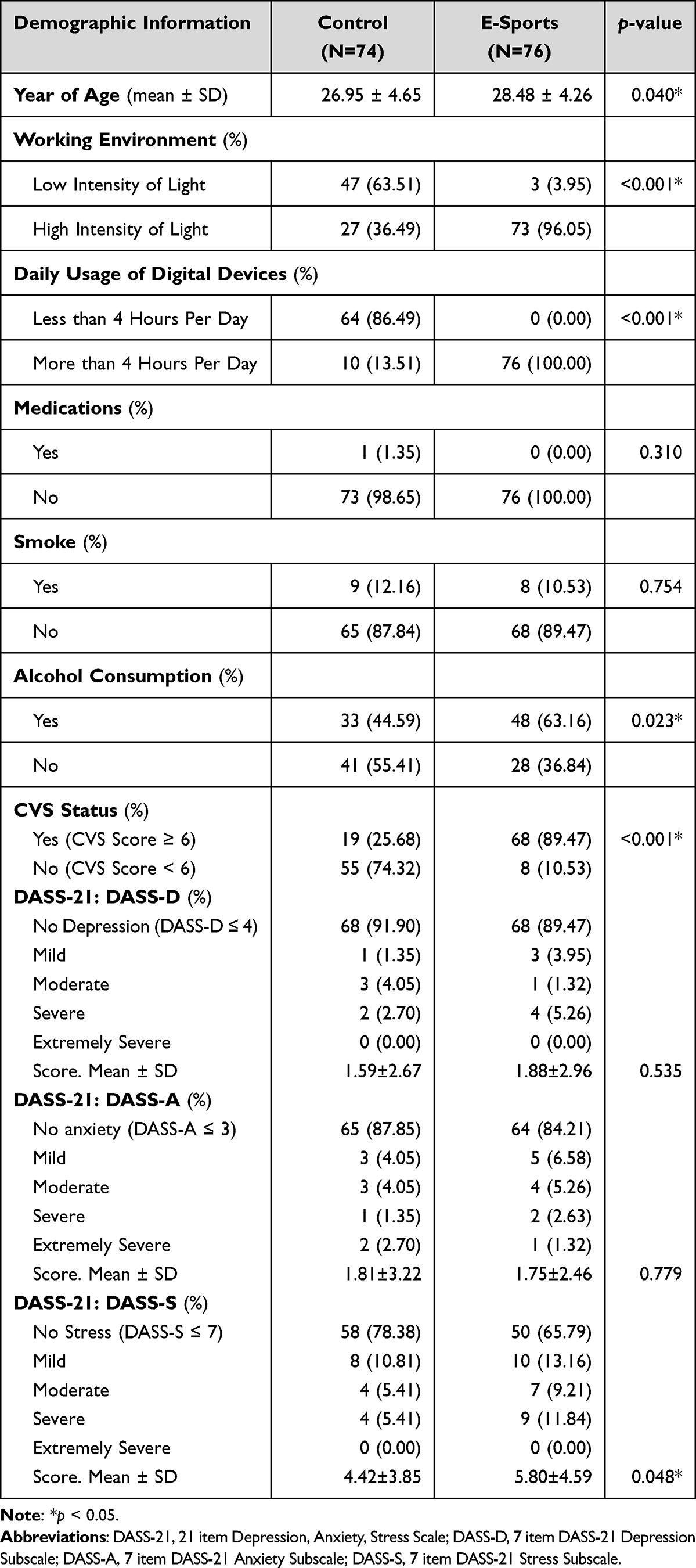 |
Table 2 The Demographic Information About the Participants (n = 150) |
Discussion
Comparison of Eye Examination Between Esports Athletes and Control
Comparing the fully corrected visual acuity, esports athletes exhibited a worse outcome than the control group, aligning with findings in Abdelaziz et al, which indicated a higher risk of dry eye in groups with more daily computer use compared to the control group. Consequently, a decrease in visual acuity was observed.20,21 Previous study indicated that a decrease in visual acuity was not correlated with dry eye but was associated with the blink rate.22,23 Prolonged digital device exposure causes a reduction in the blink rate and completeness of the blink,24 leading to a disruption in ocular surface moisture balance and a subsequent decrease in visual acuity.25
In the visual function examination at 6 m, the phoria at a far distance for the esports group tended to be more exophoric than that of the control group, although the difference was not statistically significant. This finding is similar to that of Lee et al, who reported no significant differences in phoria before and after playing video games on a computer screen. Lee et al revealed the function of tonic vergence, which has no correlation with the viewing distance of individuals, resulting in no variation in the vergence values.26 The examination also revealed no significant differences in negative fusional vergence (NFV) for either break or recovery values between the esports athletes and the control group. Similarly, the positive fusional vergence (PFV) values for blur, break, and recovery were not significantly different between the two groups. This lack of significant differences may be because viewing at far distances did not necessarily cause eye accommodation and convergence, leading to the absence of blur values in NFV at far distances.27 In these considerations, there were no differences in the vergence function between the two participant groups at far distances.
In the examination of near vision (at 40 cm), esports athletes exhibited a statistically significant increase in exophoria compared with the control group. This difference may have been caused by the extended daily use of computers and insufficient breaks by esports athletes. This finding agreed with a study conducted by Lee et al in 2019, in which participants demonstrated an increased exophoric alignment at near distance after engaging in computer screen gaming for four hours. Additionally, Lee et al reported that participants' eye alignment returned to values similar to pre-gaming levels after a day of eye rest.26 Analysis of the eye’s convergence and divergence abilities at close distances revealed that esports athletes had significantly lower values for blur, break, and recovery in negative fusional vergence (NFV) compared to the control group. This outcome is in line with the findings of Watten et al in 1994, who showed that prolonged computer screen use throughout the day reduced positive fusional vergence (PFV).28 Corresponding research by Gratton et al and Gur et al aligns with our study’s observations of decreased NFV and PFV following computer use.29,30 However, Amy and James (2018) proposed that individuals with vergence dysfunctions, such as convergence insufficiency or decompensated heterophoria, may manifest reduced NFV or PFV. Such conditions could contribute to an increased prevalence of ocular symptoms in individuals with these anomalies compared with those without such conditions.31
When comparing the monocular accommodative amplitude, there was no statistically significant difference between the esports athletes and the control group. The amplitude of accommodation, determined using Hofstetter’s formula, which considers the participant’s age, also showed no significant difference, despite esports athlete’s mean age being significantly higher. This lack of difference could be caused by the study’s inclusion of participants aged 20–35 years, potentially explaining the similarity in the monocular accommodative amplitude between the two groups. These findings were consistent with those of Wolffsohn et al.32 Similarly, when assessing binocular accommodative amplitude, which represents the combined ability to accommodate at the highest power while maintaining fusion (single vision), no significant difference was observed between the esports athletes and control group. This result stems from the fact that both the esports athletes and control group exhibited similar accommodative amplitudes. Notably, no prior research has examined binocular accommodative amplitude values or reported similar results in the same aspect.
The accommodative response, assessed using the MEM, revealed that esports athletes exhibited a significantly higher lag of accommodation than the control group. This outcome aligns with findings from studies conducted by Fogt et al and Sigamani et al, where the MEM values of the control group exhibited more lag than the standard value, although the difference was not statistically significant.33,34 The divergence results may stem from variations in participant characteristics and vision usage, given that this study focused on esports athletes with advanced gaming skills and professional expertise who also demonstrated faster saccades than individuals with general-level gaming skills.35
A prior study by Iribarren et al indicated that prolonged computer use reduces accommodative facilities, leading to increased eyestrain and discomfort.36 Similar to these findings, our study observed that both monocular and binocular accommodative facility values in esports athletes were significantly lower than those in the control group. Additionally, the vergence facility in esports athletes was significantly lower than the control group, consistent with a study by Padavettan et al, which showed that the reduction in vergence facility was associated with the use of eyesight at near distances.37 In contrast, Rosenfield et al found no significant difference in accommodative and vergence facilities before and after computer use. This contradiction may be due to the study design, which compared values before and after 25 min of computer use in the same participants, representing a relatively short duration of computer screen time.38 Unlike the Rosenfield et al study, our investigation focused on esports athletes who engaged in continuous computer use for several hours daily. This prolonged computer use may be a contributing factor affecting accommodative and vergence facilities, potentially leading to eyestrain.
Factor Associated with Computer Vision Syndrome (CVS)
This study identified factors associated with computer vision syndrome (CVS), including occupation, occupation-related characteristics, time spent on electronic devices, and alcohol consumption. Specifically, esports athletes were found to develop CVS significantly higher than other occupations. This risk is attributed to the nature of esports athlete’s work, which involves prolonged use of computer screens. Additionally, the prevalence of CVS in esports athletes was determined to be 89.47%, significantly higher than the control group, which had a prevalence of 25.68%. These findings align with those of studies conducted by Tubtimhin and Puthaburi,39 Wangsan et al,16 and Fenga40 et al, all of which reported CVS prevalence in the range of 72.1% to 88.6%.
The findings from the previous study align with the results of this research, indicating that the continuous use of electronic devices for more than four hours a day is associated with a higher prevalence of eyestrain.41 Agarwal et al and Zayed et al also indicated that using computers for more than 4 h a day can cause eyestrain.42,43 These results were further supported by our study, which revealed that esports athletes are significantly more at risk of computer vision syndrome (CVS) than the control group. Eyestrain in esports athletes can be caused by abnormal contractions and relaxations of the orbicularis oculi, one of the muscles surrounding the eye.44 The excessive accommodation, acquired by prolonged exposure to computer screens or electronic devices, leads to a decreased blink rate. This prolonged exposure causes the ocular surface to be exposed to air for extended periods, resulting in tear film instability and dry eye.45 Dry eye symptoms contribute to CVS symptoms, and prolonged accommodation causes headaches and eye discomfort.46,47
This study demonstrated that high-intensity illumination in the working environment, mostly found in esports settings, significantly increased the incidence of eyestrain compared to areas with low-intensity illumination, which was consistent with the findings of Agarwal et al (2013).42 Working in an environment with excessive light illumination can lead to eyestrain because the eyes need to accommodate more than usual light, resulting in reduced visual acuity. Maintaining light intensity within the range of 400–500 lx, as recommended by the Department of Labor Protection and Welfare in “The standard of light intensity in the workplace” announcement, can enhance employee vision and reduce the risk of eyestrain.39
Alcohol consumption was identified as one of the factors associated with CVS. This study revealed that alcohol consumption was significantly higher among esports athletes who experienced more eyestrain compared to the control group. The impact of alcohol consumption, whether short- or long-term, can decrease the blood supply to the retina48 and reduce neurotransmitter levels. These effects can lead to optic nerve ischemia, resulting in loss of the visual field and decreased visual acuity. Furthermore, alcohol consumption has been linked to various eye conditions including dry eye,49 cataract,50,51 glaucoma,52 and retinal degeneration.53,54
Assessing anxiety and depression symptoms, this study found no significant differences between esports athletes and the control group. This seems to differ from the previous research by Pereira et al, who reported that a significant portion (almost a quarter) of electronic football athletes showed symptoms of anxiety and depression.55 Similarly, Lee et al found high depression scores among esports athletes across several countries, with particularly high scores in South Korea.56 Seffah et al also highlighted the link between excessive screen time, sleep deprivation, and negative mental health outcomes, including anxiety and depression.57 Additionally, Idris et al found a correlation between IGD (Internet Gaming Disorder) and anxiety/depression in esports athletes, potentially due to prolonged screen exposure, a common factor in both conditions.11
However, the lack of difference in this study could be due to the similar prevalence of anxiety in the control group. Working individuals and laborers, as in this case, might also experience anxiety due to work pressures and job demands.58–60 Furthermore, anxiety and depression often share overlapping symptoms, making it possible for someone with anxiety to also experience depression.61,62 This overlap might explain why both groups showed similar levels of anxiety and depression in this study. Interestingly, stress levels were significantly higher among esports athletes compared to the control group. While Rudolf et al reported that most esports athletes experience low-level stress,63 the unique stressors faced by esports athletes, such as performance pressure, expectations, handling defeats, team conflicts, and online toxicity, can potentially impact their mental health.12
This study has limitations related to the specificity of the sample population, which comprised esports athletes in comparison to the control group. Additionally, the age range of the participants was restricted to individuals between 20 and 35 years, and the study exclusively involved male participants. As a result, certain analyses, including those related to factors such as anxiety, depression, and medications, showed no statistically significant differences. The impact of alcohol consumption on CVS should be investigated further, focusing on the amount and frequency of drinking as potential contributing factors. These limitations highlight the need for caution when generalizing the findings beyond the scope of the specified sample characteristics.
Conclusion
This comprehensive study systematically compared eye examination results between esports athletes and a control group. The current results showed that esports athletes exhibited significantly worse fully corrected visual acuity than the control group, potentially linked to increased dry eye risk and decreased blink rates associated with prolonged computer use. No significant differences were observed in the far-distance phoria and fusional vergence parameters between groups. However, a near-vision examination revealed a significant increase in exophoria among esports athletes, possibly due to prolonged computer use and inadequate breaks. Accommodative and vergence functions, assessed through various methods, demonstrated significant differences in several results, indicating the impact of continuous computer use on these parameters. Further analysis revealed that occupational factors, high light exposure, prolonged digital device use, and alcohol consumption were significant risk factors for Computer Vision Syndrome (CVS) in esports athletes. Esports athletes were found to have significantly higher CVS, emphasizing the need for prevention in this population. Although the study acknowledged the limitations of sample specificity and age range, it provided valuable insights into the visual health of esports athletes. This study contributes to a broader understanding of the implications of extensive digital device use on ocular health. These findings suggest that factors like prolonged screen time, excessive lighting, and higher stress levels might contribute to a higher risk of CVS among esports athletes.
Acknowledgments
This work was supported by grants from the Research and Development Institute of Ramkhamhaeng University, Thailand. We are grateful for the support provided by the Faculty of Optometry, Ramkhamhaeng University.
Disclosure
There is no conflict of interest regarding the publication of this paper.
References
1. Jenny SE, Manning RD, Keiper MC, Olrich TW. Virtual(ly) athletes: where esports fit within the definition of “sport”. Quest. 2017;69(1):1–18. doi:10.1080/00336297.2016.1144517
2. Keiper M, Manning R, Jenny S, Olrich T, Croft C. No reason to lol at lol: the addition of esports to intercollegiate athletic departments. J Study Sports Athl Educ. 2017;11(2):1–18. doi:10.1080/19357397.2017.1316001
3. Bányai F, Zsila Á, Griffiths MD, Demetrovics Z, Király O. Career as a professional gamer: gaming motives as predictors of career plans to become a professional esport player. Front Psychol. 2020;11:1866. doi:10.3389/fpsyg.2020.01866
4. DiFrancisco-Donoghue J, Balentine J, Schmidt G, Zwibel H. Managing the health of the eSport athlete: an integrated health management model. BMJ Open Sport Exerc Med. 2019;5(1):e000467. doi:10.1136/bmjsem-2018-000467
5. Alabdulkader B. Effect of digital device use during COVID-19 on digital eye strain. Clin Exp Optom. 2021;104(6):698–704. doi:10.1080/08164622.2021.1878843
6. WHO. ICD-11 for Mortality and Morbidity Statistics. WHO; 2024.
7. Chung T, Sum S, Chan M, Lai E, Cheng N. Will esports result in a higher prevalence of problematic gaming? A review of the global situation. J Behav Addict. 2019;8(3):384–394. doi:10.1556/2006.8.2019.46
8. Mylona I, Deres ES, Dere GS, Tsinopoulos I, Glynatsis M. The impact of internet and videogaming addiction on adolescent vision: a review of the literature. Front Public Health. 2020;8:63. doi:10.3389/fpubh.2020.00063
9. Floros GD, Glynatsis MN, Mylona I. No end in sight; assessing the impact of internet gaming disorder on digital eye strain symptoms and academic success. Eur J Investig Health Psychol Educ. 2024;14(3):531–539. doi:10.3390/ejihpe14030035
10. Kaur K, Gurnani B, Nayak S, et al. Digital eye strain- a comprehensive review. Ophthalmol Ther. 2022;11(5):1655–1680. doi:10.1007/s40123-022-00540-9
11. Idris MF, Saini SM, Sharip S, Idris NF, Ab Aziz NF. Association between the internet gaming disorder and anxiety and depression among university students during COVID-19 pandemic. Healthcare. 2023;11(8):1103. doi:10.3390/healthcare11081103
12. Kegelaers J, Trotter MG, Watson M, et al. Promoting mental health in esports. Front Psychol. 2024;15:1342220. doi:10.3389/fpsyg.2024.1342220
13. Talens-Estarelles C, García-Marqués JV, Cerviño A, García-Lázaro S. Dry eye-related risk factors for digital eye strain. Eye Contact Lens. 2022;48(10):410–415. doi:10.1097/icl.0000000000000923
14. Sánchez-Valerio MDR, Mohamed-Noriega K, Zamora-Ginez I, Baez Duarte BG, Vallejo-Ruiz V. Dry eye disease association with computer exposure time among subjects with computer vision syndrome. Clin Ophthalmol. 2020;14:4311–4317. doi:10.2147/opth.S252889
15. Auffret É, Gomart G, Bourcier T, Gaucher D, Speeg-Schatz C, Sauer A. Perturbations oculaires secondaires à l’utilisation de supports numériques. Symptômes, prévalence, physiopathologie et prise en charge. J Fr Ophtalmol. 2021;44(10):1605–1610. doi:10.1016/j.jfo.2020.10.002
16. Wangsan K, Upaphong P, Assavanopakun P, et al. Self-reported computer vision syndrome among Thai university students in virtual classrooms during the COVID-19 pandemic: prevalence and associated factors. Int J Environ Res Public Health. 2022;19(7):3996. doi:10.3390/ijerph19073996
17. Seguí Mdel M, Cabrero-García J, Crespo A, Verdú J, Ronda E. A reliable and valid questionnaire was developed to measure computer vision syndrome at the workplace. J Clin Epidemiol. 2015;68(6):662–673. doi:10.1016/j.jclinepi.2015.01.015
18. Oei TP, Sawang S, Goh YW, Mukhtar F. Using the Depression Anxiety Stress Scale 21 (DASS-21) across cultures. Int J Psychol. 2013;48(6):1018–1029. doi:10.1080/00207594.2012.755535
19. Ali AM, Ahmed A, Sharaf A, Kawakami N, Abdeldayem SM, Green J. The Arabic version of the depression anxiety stress scale-21: cumulative scaling and discriminant-validation testing. Asian J Psychiatr. 2017;30:56–58. doi:10.1016/j.ajp.2017.07.018
20. Abdelaziz MM, Fahim SA, Mousa DB, Gaya BI. Effects of computer use on visual acuity and colour vision among computer workers in Zaria. Eur J Sci Res. 2009;35(1):99–105.
21. Olubiyi S, Agbede O, Okesina B, Bode-Kayode A. Pattern of computer usage and visual acuity among computer users at National Open University of Nigeria (NOUN). Int J Nurs Midwifery. 2015;7(7):116–122. doi:10.5897/IJNM2015.0168
22. Bonilla Perdomo C, Castaño Figueroa JN, Gómez De La Hoz MP. Alterations of the ocular surface in users of electronic screens; 2022.
23. Szczotka-Flynn LB, Maguire MG, Ying GS, et al. Impact of dry eye on visual acuity and contrast sensitivity: dry eye assessment and management study. Optom Vis Sci. 2019;96(6):387–396. doi:10.1097/opx.0000000000001387
24. Portello JK, Rosenfield M, Blink Rate CCA. Incomplete blinks and computer vision syndrome. Optometry Vision Sci. 2013;90(5):482–487. doi:10.1097/OPX.0b013e31828f09a7
25. Itokawa T, Okajima Y, Suzuki T, et al. Association among blink rate, changes in ocular surface temperature, tear film stability, and functional visual acuity in patients after cataract surgery. J Ophthalmol. 2019;2019:8189097. doi:10.1155/2019/8189097
26. Lee JW, Cho HG, Moon BY, Kim SY, Yu DS. Effects of prolonged continuous computer gaming on physical and ocular symptoms and binocular vision functions in young healthy individuals. PeerJ. 2019;
27. Azzam D, Ronquillo Y. Snellen Chart StatPearls. StatPearls Publishing Copyright © 2023. StatPearls Publishing LLC; 2023.
28. Watten RG, Lie I, Birketvedt O. The influence of long-term visual near-work on accommodation and vergence: a field study. J human ergol. 1994;23(1):27–39. doi:10.11183/jhe1972.23.27
29. Gratton I, Piccoli B, Zaniboni A, Meroni M, Grieco A. Change in visual function and viewing distance during work with VDTs. Ergonomics. 1990;33(12):1433–1441. doi:10.1080/00140139008925344
30. Gur S, Ron S, Heicklen-Klein A. Objective evaluation of visual fatigue in VDU workers. Occup Med. 1994;44(4):201–204. doi:10.1093/occmed/44.4.201
31. Amy LS, James SW. Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018;3(1):e000146. doi:10.1136/bmjophth-2018-000146
32. Wolffsohn JS, Sheppard AL, Vakani S, Davies LN. Accommodative amplitude required for sustained near work. Ophthalmic Physiol Opt. 2011;31(5):480–486. doi:10.1111/j.1475-1313.2011.00847.x
33. Fogt JS, Onate J, Emerson A, Kraemer W, Fogt N. Visual and ocular characteristics of esports participants. Optometry Vision Sci. 2021;98(7):771–776. doi:10.1097/OPX.0000000000001725
34. Sigamani S, Majumder C, Sukumaran S. Changes in accommodation with visual fatigue among digital device users. Med Hypothesis Discov Innov Optom. 2022;3(2):63–69. doi:10.51329/mehdioptometry153
35. Jeong I, Nakagawa K, Osu R, Kanosue K. Difference in gaze control ability between low and high skill players of a real-time strategy game in esports. PLoS One. 2022;17(3):e0265526. doi:10.1371/journal.pone.0265526
36. Iribarren R, Fornaciari A, Hung GK. Effect of cumulative nearwork on accommodative facility and asthenopia. Intl Ophthalmol. 2001;24(4):205–212. doi:10.1023/A:1022521228541
37. Padavettan C, Nishanth S, Vidhyalakshmi S, Madhivanan N, Madhivanan N. Changes in vergence and accommodation parameters after smartphone use in healthy adults. Indian J Ophthalmol. 2021;69(6):1487–1490. doi:10.4103/ijo.IJO_2956_20
38. Rosenfield M, Gurevich R, Wickware E, Lay M. Computer Vision Syndrome: accommodative and Vergence Facility. Invest Ophthalmol Visual Sci. 2009;50(13):5332.
39. Tubtimhin S, Puthaburi N. Prevalence and severity of computer vision syndrome of supporting staff in Ubon Ratchathani University. Srinagarind Med J. 2019;34(2):173–177.
40. Fenga C, Aragona P, Cacciola A, et al. Meibomian gland dysfunction and ocular discomfort in video display terminal workers. Eye. 2008;22(1):91–95. doi:10.1038/sj.eye.6703025
41. Cantó-Sancho N, Porru S, Casati S, Ronda E, Seguí-Crespo M, Carta A. Prevalence and risk factors of computer vision syndrome-assessed in office workers by a validated questionnaire. PeerJ. 2023;
42. Agarwal S, Goel D, Sharma A. Evaluation of the factors which contribute to the ocular complaints in computer users. J Clin Diagn Res. 2013;7(2):331–335. doi:10.7860/jcdr/2013/5150.2760
43. Zayed HAM, Saied SM, Younis EA, Atlam SA. Digital eye strain: prevalence and associated factors among information technology professionals, Egypt. Environ Sci Pollut Res Int. 2021;28(20):25187–25195. doi:10.1007/s11356-021-12454-3
44. Sheedy JE. The physiology of eyestrain. J Mod Opt. 2007;54(9):1333–1341. doi:10.1080/09500340600855460
45. Al-Mohtaseb Z, Schachter S, Shen Lee B, Garlich J, Trattler W. The relationship between dry eye disease and digital screen use. Clin Ophthalmol. 2021;15:3811–3820. doi:10.2147/opth.S321591
46. Chawla U, Yadav P, Chugh J, Chadha G. Study of digital eye strain due to extended digital device use among undergraduate medical students during covid - 19 pandemic: a cross sectional study. Int J All Res Educ Sci Methods. 2021;9(3):991–998.
47. Abudawood GA, Ashi HM, Almarzouki NK. Computer vision syndrome among undergraduate medical students in king Abdulaziz University, Jeddah, Saudi Arabia. J Ophthalmol. 2020;2020:2789376. doi:10.1155/2020/2789376
48. Karimi S, Arabi A, Shahraki T. Alcohol and the eye. J Ophthalmic Vis Res. 2021;16(2):260.
49. Magno MS, Daniel T, Morthen MK, et al. The relationship between alcohol consumption and dry eye. Ocular Surf. 2021;21:87–95. doi:10.1016/j.jtos.2021.05.005
50. Fukai K, Terauchi R, Furuya Y, et al. Alcohol use patterns and risk of incident cataract surgery: a large scale case–control study in Japan. Sci Rep. 2022;12(1):20142. doi:10.1038/s41598-022-24465-2
51. Gong Y, Feng K, Yan N, Xu Y, Pan C-W. Different amounts of alcohol consumption and cataract: a meta-analysis. Optometry Vision Sci. 2015;92(4):471–479. doi:10.1097/opx.0000000000000558
52. Han YS, Kim YW, Kim YJ, Park KH, Jeoung JW. Alcohol consumption is associated with glaucoma severity regardless of ALDH2 polymorphism. Sci Rep. 2020;10(1):17422. doi:10.1038/s41598-020-74470-6
53. Adams MK, Chong EW, Williamson E, et al. 20/20--alcohol and age-related macular degeneration: the Melbourne collaborative cohort study. Am J Epidemiol. 2012;176(4):289–298. doi:10.1093/aje/kws004
54. Zhang J, Mitsuhashi T, Matsuo T, Yorifuji T, Hamada J, Liu Y. Alcohol consumption and age-related macular degeneration: a systematic review and dose–response meta-analysis. Curr Eye Res. 2021;46(12):1900–1907. doi:10.1080/02713683.2021.1942070
55. Pereira AM, Teques P, Verhagen E, Gouttebarge V, Figueiredo P, Brito J. Mental health symptoms in electronic football players. BMJ Open Sport Exerc Med. 2021;7(4):e001149. doi:10.1136/bmjsem-2021-001149
56. Lee S, Bonnar D, Roane B, et al. Sleep characteristics and mood of professional esports athletes: a multi-national study. Int J Environ Res Public Health. 2021;18(2). doi:10.3390/ijerph18020664
57. Seffah KD, Salib K, Dardari L, et al. Health benefits of esports: a systematic review comparing the cardiovascular and mental health impacts of esports. Cureus. 2023;15(6):e40705. doi:10.7759/cureus.40705
58. Linden M, Muschalla B. Anxiety disorders and workplace-related anxieties. J Anxiety Disord. 2007;21(3):467–474. doi:10.1016/j.janxdis.2006.06.006
59. Cherry N. Stress, anxiety and work: a longitudinal study. J Occup Psychol. 1978;51(3):259–270. doi:10.1111/j.2044-8325.1978.tb00422.x
60. Kuster AT, Kuster AC, Klaiklang R. Self-representations of quality of life and anxiety of blue-collar workers, Khon Kaen, Thailand. J Health Res. 2017;29(6):449–456.
61. Zbozinek TD, Rose RD, Wolitzky-Taylor KB, et al. Diagnostic overlap of generalized anxiety disorder and major depressive disorder in a primary care sample. Depress Anxiety. 2012;29(12):1065–1071. doi:10.1002/da.22026
62. Steenkamp LR, Hough CM, Reus VI, et al. Severity of anxiety- but not depression- is associated with oxidative stress in major depressive disorder. J Affect Disord. 2017;219:193–200. doi:10.1016/j.jad.2017.04.042
63. Rudolf K, Soffner M, Bickmann P, et al. Media consumption, stress and wellbeing of video game and esports players in Germany: the eSports study 2020. Front Sports Act Living. 2022;4:665604. doi:10.3389/fspor.2022.665604
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.