")
Back to Journals » Clinical Ophthalmology » Volume 18
Dry Eye Disease in the Middle East and Northern Africa: A Position Paper on the Current State and Unmet Needs
Authors Lazreg S, Hosny M, Ahad MA, Sinjab MM , Messaoud R, Awwad ST, Rousseau A
Received 3 October 2023
Accepted for publication 24 January 2024
Published 6 March 2024 Volume 2024:18 Pages 679—698
DOI https://doi.org/10.2147/OPTH.S436027
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Sihem Lazreg,1 Mohamed Hosny,2 Muhammad A Ahad,3 Mazen M Sinjab,4 Riadh Messaoud,5 Shady T Awwad,6 Antoine Rousseau7
1Ophthalmology Cabinet, Blida, Algeria; 2Refractive and Cornea Service, Cairo University Hospitals, Cairo, Egypt; 3Department of Ophthalmology, Anterior Segment Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 4Dr Sulaiman Al Habib Hospital, DHCC, Dubai, United Arab Emirates; 5Department of Ophthalmology, Tahar SFAR University Hospital, Mahdia, Tunisia; 6Department of Ophthalmology, American University of Beirut - Medical Center, Beirut, Lebanon; 7Department of Ophthalmology, Bicêtre Hospital, Paris-Saclay University, Le Kremlin-Bicêtre, France
Correspondence: Antoine Rousseau, Pierre Testas Building, Bicêtre Hospital, 78 Rue du Général Leclerc, Le Kremlin-Bicêtre, 94270, France, Tel +33145213690, Email [email protected]
Abstract: In the Middle East and Northern Africa (MENA), dry eye disease (DED) is often misdiagnosed or overlooked. This review summarizes a series of conversations with ophthalmologists in the region around a variety of climatic, lifestyle, and iatrogenic factors that contribute to specific features of DED in the MENA region. These considerations are further classified by patient lifestyle and surgical choices. All statements are based on discussions and formal voting to achieve consensus over three meetings. Overall, a deeper understanding of the disease characteristics of DED specific to MENA can better guide local eyecare practitioners on appropriate management and follow-up care. Additionally, population-based studies and patient and physician education on ocular surface diseases, together with the use of culturally appropriate and language-specific questionnaires can help ease the public health burden of DED in this region.
Keywords: ocular surface, regional clinical practice, epidemiology, treatment, patient outcomes
Introduction
Dry eye disease (DED) is a common disease of the ocular surface that can significantly impact patient-related quality of life. In 2017, the Tear Film and Ocular Surface Society International Dry Eye Workshop 2 (TFOS DEWS II) report redefined DED as “a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles”. Overall, the TFOS DEWS II initiative indicates that dry eye disease is a global public health problem.1 Global epidemiologic data suggest that the prevalence of DED varies significantly, with a range of 5% to 50%.1 Extrapolation of the global prevalence rates indicates an estimated population of 400 million to 3.7 billion patients with DED worldwide.2 Approximately 25% of patients who refer to eye clinics report DED-related symptoms.3
While most patients perceive DED merely as a discomfort, one third perceive it as a disease or even a handicap.4 Among patients with DED, the most common symptoms include irritated, itchy, and dry eyes, with stinging/burning, foreign body sensation, grittiness, tearing, and blurred vision. DED presents a substantial socioeconomic burden worldwide. Cost estimates for DED range between $300 and $1100 per patient annually in European countries, with additional costs due to decreased work productivity.5
DED is also a significant clinical problem that is often overlooked or misdiagnosed in developing countries and/or emerging economies, especially in the Middle East and Northern Africa (MENA). Additionally, there is a relative scarcity of epidemiologic data and peer-reviewed publications on DED originating from this region.6–10 The lack of uniformity in existing publications limits reasonable estimates of the prevalence and burden of DED in the region.6–10 Given the geographic size of area and population living in the region, there is an emergent need to establish a uniform approach for the management of DED for healthcare providers in MENA.
Countries such as Egypt, Algeria, and Tunisia in North Africa, and Lebanon, Saudi Arabia, and the United Arab Emirates in the Middle East have country-specific differences in the epidemiology of DED, including prevalence and associated risk factors. Such region-specific differences in DED-related factors need to be highlighted to provide local eyecare practitioners with a better understanding of managing DED in MENA.
Hence, a group of experts held a series of three meetings to discuss: 1) the epidemiological features of DED in MENA, 2) the different diagnostic modalities, 3) treatment options, 4) therapeutic strategies, and 5) perioperative management. This paper provides a practical and adapted approach for ophthalmologists in MENA to improve diagnostic modalities and ensure appropriate management and follow-up of DED.
Approach for Achieving Consensus
The expert panel of six regional physicians and a chairperson from outside MENA met in three virtual meetings. Consensus on all statements and discussion was reached through voting, alignment, and written agreement.
Etiology of Dry Eye Disease
Several comprehensive reviews on the pathogenesis of DED have been published,11–13 and the reader is referred to them for detailed information. Dry eye disease is generally categorized as having evaporative, aqueous deficient, or mixed etiology,14 with about 70% of cases having evaporative causes.15 Both evaporative and aqueous deficient types of DED have multifactorial etiologies that ultimately results in loss of tear film homeostasis along with inflammation and ocular tissue damage, further exacerbating tear film dysfunction.14 The primary cause of evaporative DED is believed to be meibomian gland dysfunction (MGD), which is present in at least 86% of DED cases.16 Decreased lipids production in MGD reduces the tear film lipid layer thickness (LLT), which can lead to more rapid tear film evaporation and tear film instability.17–20 Tear film instability can also result from decreased tear production secondary to dysfunction in pathways that stimulate the lacrimal glands or defects in the lacrimal gland itself.21 The both the loss of tear film stability and increased tear osmolarity stimulate increased levels of inflammatory cells (CD4 and CD8 T cells) and enhanced production and secretion of a large number of pro-inflammatory cytokines and chemokines, including interleukin (IL)-1β, IL-6, IL-8, tumor necrosis factor-α, CCL3, CCL4, and CCL5.12,22 These inflammatory cells, cytokines, and chemokines induce epithelial damage and further tear dysregulation, resulting in a cycle of DED pathogenesis.12
Epidemiology of Dry Eye Globally and in MENA
Epidemiological studies report a wide range of DED prevalences based on disease definition, method of diagnosis, population surveyed, and how data are analyzed. A study that combined systematic literature in combination with Bayesian analysis reported that the prevalence of DED was 27.76% across Asia, 22.70% in Europe, 25.93% across the Middle East, 9.04% in Australia, 47.52% across Africa, 5.5% in North America, 12.80% across South America, and 32.00% in India.23 Another systematic review published 2 years earlier found similar trends in the regional prevalences of DED: high DED rates in Africa, moderate rates in Asia and Europe, and lower rates in North America.24 Several factors have been suggested as potential reasons for regional differences in the prevalence of DED, including climate, weather parameters, environmental exposures, and socioeconomic considerations.24,25 However, validating clear relationships between these factors and DED prevalence is difficult because of the very large number of potential confounders.
Additional studies focusing specifically on DED in MENA have indicated by-country prevalences ranging from 6.8% to 69%.8–10,26 One systematic review indicated that the estimated prevalence of DED in Saudi Arabia ranged from 32.1% to 62.4%, and from 6.8% to 28% in Egypt.26 Prevalences for countries having only a single estimate indicated DED values of 69% for Palestine (West Bank), 52% for Jordan, 27.2% for Iraq, 10% for United Arab Emirates, 28.5% for Tunisia, 36.4% for Lebanon, and 40% for Libya.26 Additional sources have indicated a DED prevalence of 15% for Israel,27 65.2% for Syria,28 and 52.8% for Turkey.29
Taken together, the varied outcomes reported in the above-mentioned studies indicate that the overall prevalence of DED in MENA is not clearly established. Additionally, because of differences in the diagnostics, criteria, and methodologies used, it is tenuous at best to draw any specific conclusions from DED data in MENA. Furthermore, to the best of our knowledge, no international multicenter epidemiological studies have been conducted in the region, and current data are specific to studies performed in individual countries.
Impact on Quality of Life
Quality of life can be significantly impaired in patients with DED in MENA. DED affects vision-related daily life activities such as reading, using computers or other digital devices, watching television, and driving. Professional activities and work productivity are negatively impacted by DED, with the most pronounced effect noted among Saudi Arabian office workers.30
Multiple studies have reported depression and anxiety resulting from impaired quality of life due to DED.31,32 One questionnaire-based study reported that 42% of 476 patients with DED in Saudi Arabia were diagnosed with depression.33 The authors concluded that DED was a possible risk factor for developing depression, including more severe forms of depression. Additionally, depression among DED patients is reported to be significantly more prevalent among females and young adults, compared to older adults.33 Another study from Saudi Arabia reported that DED might also impact quality of sleep among patients.34
Specific Risk Factors for DED in MENA
A listing of the numerous risk factors for DED more broadly is provided in Table 1. Consistent with studies in other regions, studies conducted in Saudi Arabia and Lebanon indicate that aging and female sex are risk factors for DED.7–9 Autoimmune diseases, such as Sjögren syndrome, rheumatoid arthritis, and thyroid disease are also major risk factors for DED.35,36 However, factors specific to the MENA region include environment, lifestyle, and demographics.
 |
Table 1 Risk Factors for Dry Eye Disease |
Environmental Factors
Environmental conditions in MENA vary widely, with significant differences in climates, ranging from mountainous to coastal regions, sandy deserts, and polluted megalopolises. The arid climate is a hallmark of MENA, leading to increased time spent indoors in air-conditioned (AC) environments.40 AC, especially with prolonged duration of exposure, is a known risk factor for DED; one analysis of participant activity logs (N=35) reported that a mean of 4.9 hours of AC exposure was linked to dry eye symptoms.41,42 Additionally, dry, sandy air in desert regions or salty air in windy coastal areas may cause or exacerbate DED symptoms. Pollution, which is also associated with DED, is of particular concern in MENA’s megalopolises, including Cairo43 and Beirut.44 High exposure to ultraviolet light and living in a hot, dry, windy, or dusty environment, which is common in MENA, may give rise to pterygium, a fibrovascular proliferative lesion of the bulbar conjunctiva that extends over the corneal surface.45 These lesions may be associated with decreased visual acuity,45 increased corneal irregularity,46 and eye redness.47 Based on symptoms and abnormal Schirmer test results, there is a high prevalence of DED in patients with primary and recurrent pterygium.48
Iatrogenic Risk Factors
Contact lens (CL) wear is prevalent in MENA, especially among young adults, and much of it is unsupervised, including the use of cosmetic CLs. CL-related dry eye is recognized as a specific entity49 and could be aggravated by exposure to AC. In a Saudi Arabian study, up to one third of CL wearers reported significant DED symptoms.50 Although published data are unavailable in some MENA countries—especially Egypt and Lebanon—the volume of corneal refractive and cataract surgeries is constantly increasing. These surgical procedures can result in corneal nerve damage (especially laser in situ keratomileusis) and may cause or exacerbate dry eye symptoms during the initial 6 months following surgery.49,51,52 Fortunately, this complication is generally transient and can be treated with artificial tear substitutes.53
Use of specific medications has been associated with increased risk for developing DED (Table 2).37,54,55 For example, the long-term use of glaucoma medications can trigger or exacerbate DED, especially in patients using one or more topical formulations containing preservatives, such as benzalkonium chloride (BAK).49 A Tunisian study of 120 patients with glaucoma on topical therapy found that 90% of patients reported some form of DED.56 Another Tunisian study of 155 medically-managed patients with glaucoma reported that the main risk factors for DED were advanced age, duration of glaucoma treatment, use of multiple therapies, and the use of antiglaucoma medications containing BAK.57 Although specific data are lacking for MENA, generally, DED can also be caused by estrogen-containing hormone replacement therapies, antihistamines, and psychotropic drugs, many of which reduce lacrimal secretion.49 Caffeine may also be associated with increased risk for DED,58 but the available data are not yet consistent enough to draw a firm conclusion.7,59
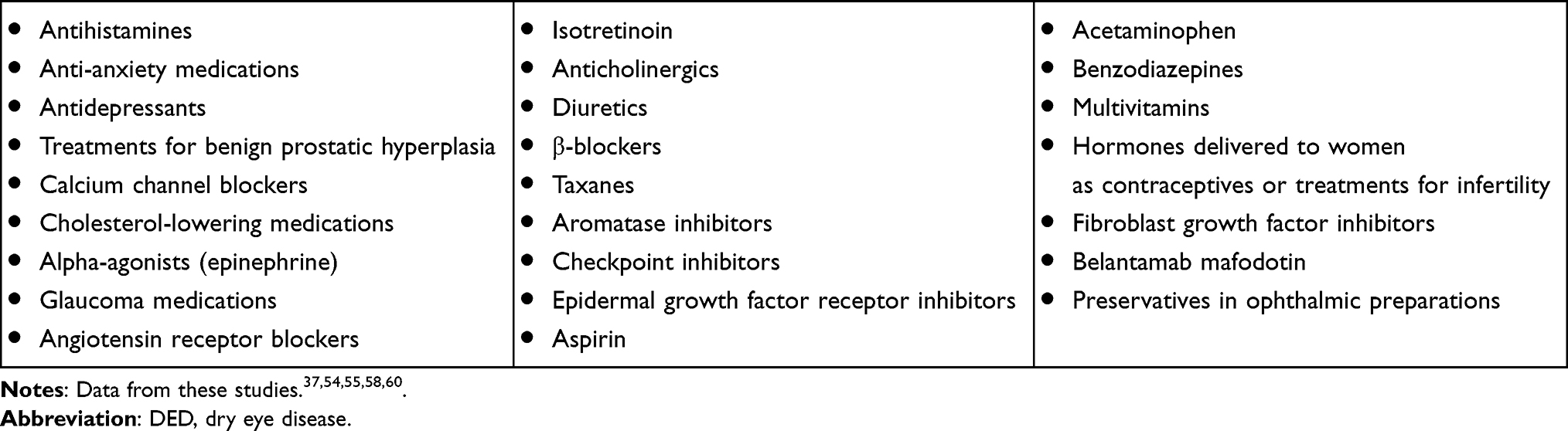 |
Table 2 Medications That Increase Risk for DED |
Lifestyle
There is widespread use of digital devices in MENA. Prolonged use of video display terminals (VDTs) and computers reduces blink rates and increases the proportion of incomplete blinks, leading to computer vision syndrome, which is highly prevalent but often misdiagnosed in MENA. Computer vision syndrome is a combination of oculomotor/vergence system abnormalities, tear film instability, and ocular inflammation, which can lead to DED.61,62
Smoking is another significant risk factor for DED in Saudi Arabia and Egypt, but not in Dubai.63 Shisha cafés are very popular in some MENA countries, such as Egypt, and smoke from hookah sessions may be damaging to the ocular surface. Previous studies indicate that, in a 20- to 80-minute hookah session, users may smoke the equivalent of 100 or more cigarettes.64 In addition, the use of charcoal as a heating source in Shisha cafés generates large amounts of carbon monoxide and polycyclic aromatic hydrocarbons, which are irritating to the ocular surface. These data suggest that frequent visits to Shisha cafés could promote DED. However, a study from Dubai did not find an association between exposure to smoking/shisha and DED.10
Dietary Habits
Many clinicians recommend and many patients take omega-3 fatty acid dietary supplements to reduce inflammation. However, the efficacy of omega-3 fatty acid supplementation in improving the signs and symptoms of DED remains controversial.65 For instance, the DREAM study concluded that patients with DED who received omega-3 fatty acid supplementation did not show a significant improvement in symptoms compared to a similar cohort that received olive oil as placebo.66 It is possible, however, that omega-9 fatty acids, which are present in olive oil, could improve DED signs and symptoms similar to omega-3 fatty acids.67 A meta-analysis of randomized clinical trials of omega-3 fatty acids concluded that they can be effective for treating DED.68 However, there are currently no available data on omega-3 intake and DED in MENA.
A separate meta-analysis suggested that vitamin D deficiency was associated with worsening of dry eye symptoms and reduced tear production in patients with DED;62 vitamin D deficiency is highly prevalent in Lebanon. In a study with 446 participants, up to 71.9% of the study population had vitamin D deficiencies.69 Hence, vitamin D deficiency may be another MENA-specific factor predisposing patients to DED.
Inflammation and Infections
Trachoma is fortunately no longer as prevalent as it used to be in MENA. However, in some regions where the prevalence used to be high (notably, remote rural regions of Tunisia70), a significant number of patients suffer from the sequelae of trachomatous infections, which can cause severe meibomian gland dysfunction (MGD) and aqueous deficiency.71
Vernal keratoconjunctivitis (VKC) is another common inflammatory DED risk factor in MENA. VKC exacerbates the problem of DED via two pathways: the pathophysiology of the disease itself, where the ocular surface is involved in an inflammatory reaction that slowly destroys the accessory lacrimal apparatus and goblet cells, and the chronic use of topical anti-inflammatory and antihistamine agents that contain preservatives that further contribute to ocular surface damage.
Unmet Needs in DED Epidemiological Research in MENA
There is a significant need for epidemiological, population-based studies of DED in MENA. In particular, studies that are more realistic and based on questionnaires that are standardized across different countries to identify regional specificities in DED prevalence and treatment are needed. There is a need to determine proactive public health measures to decrease the burden of DED in MENA.
Diagnostic Procedures in DED
Patient Interview
An expert panel agreed that a detailed patient history is crucial to identify DED and its risk factors in MENA. This includes daily living activities and occupation, focusing on environmental, systemic, and ocular risk factors, assessing DED symptoms and their consequences in daily life and socio-professional productivity. According to the expert panel, three DED symptoms seem more specific to the MENA region, as follows:
- Light sensitivity, the most commonly-reported symptom in two studies from MENA (Jordan and Lebanon)8,72
- Difficulty opening eyes upon waking due to overnight air conditioning
- Fluctuating vision or blurred vision caused by tear film instability, which may be exacerbated by environmental conditions
The panel recommends that validated symptom questionnaires, such as the Dry Eye Questionnaire 5 (DEQ-5),73 Ocular Surface Disease Index (OSDI),74 and Standard Patient Evaluation of Eye Dryness (SPEED),75 are helpful in evaluating symptoms and the impact of these symptoms on vision and daily life. These questionnaires are critical for monitoring DED progression and response to treatments and should be used at the beginning of the consultation. Among the validated DED symptom questionnaires, only OSDI is available in Arabic. The OSDI is a useful tool for assessing the severity of DED. Patients are considered positive for DED if their total OSDI score is ≥13, with further subdivisions into mild (score 13–22), moderate (score 23–32), and severe (score 33–101). The panel also suggested that a visual analogue scale of DED symptoms may provide a quick and reliable assessment of disease severity and patient burden.76
Clinical Examination
Clinical evaluation of patients who may have DED should be stepwise, beginning with a careful inspection of the facial and eyelid skin to detect associated skin diseases such as acne rosacea. The blink rate dynamics should also be assessed, as reduced blinking rates or partial blinking are frequently observed in patients with DED. Decreased blink rates can result from a variety of factors, including computer vision syndrome and Parkinson disease.77,78 These phenomena increase ocular surface exposure and tear film evaporation and reduce meibomian gland drainage.79
Slit lamp examination should first include a careful assessment of the eyelid margins to detect anterior and posterior blepharitis and eyelash abnormalities. The ocular surface should be examined before fluorescein instillation to observe lid-parallel conjunctival folds (LIPCOF), which are helpful in diagnosing dry eye.80 The presence of foamy tears on the eyelid margins, also called saponification of tears, is an indirect indicator of meibomian gland deficiency.
Slit lamp examination should be followed by evaluating: i) tear film stability, which can be considered compromised if tear break-up time (TBUT) is shorter than 10 seconds and may indicate an evaporative component of DED; and ii) tear secretion, using either tear meniscus height (TMH) or the Schirmer I test. A TMH <0.3 mm or Schirmer I test <10 mm/5 min indicate an aqueous deficient component of dry eye.81
Tarsal conjunctiva should be examined for papillae, follicles, or fibrotic scars to exclude any differential diagnoses or co-existing conditions, such as allergic conjunctivitis or sequelae from trachomatous or viral conjunctivitis. Pterygium has been described in association with DED in many countries, including MENA. Pterygium is more prevalent in Algeria (18%) than Saudi Arabia (0.074%),82 and it may exacerbate dry eye symptoms in affected patients.83 DED may occur in young patients with VKC, though the diagnosis of both conditions is challenging due to overlapping symptoms.
Fluorescein staining is crucial to assess corneal and conjunctival damage. Staining occurs when the integrity of the corneal epithelium is compromised due to a disruption in superficial cell tight junctions or defective glycocalyx. The staining can be visualized with a yellow filter. The use of semi-quantitative staining scales, such as the Oxford score, is helpful as a somewhat objective measure and facilitates follow-up.81 Lissamine green is a vital dye that stains corneal epithelial cells only if the cell membrane is damaged, irrespective of the presence of mucin.81 However, lissamine green is not readily available, and the panel agreed that fluorescein is sufficient for daily practice. Meibomian gland expression should be routinely performed at the end of the examination to avoid interference with the previous steps of the clinical assessment.
Ancillary Investigations
Among the multiple imaging techniques available to quantify and assess the ocular surface, the expert panel agreed that infrared meibography is a valuable noninvasive tool to visualize meibomian gland anatomy, quantify meibomian gland loss, and further guide DED treatment.81 Other tools, such as tear film interferometry, tear osmolarity, matrix metalloproteinase 9 (MMP-9),84 aberrometry, and meniscometry can also be helpful81 but are primarily only available in specialized centers.
In addition to imaging the ocular surface, assessments of the tear film itself are critical in for evaluating patients with suspected DED.85 These assessments each capture information on tear film characteristics key to DED. TBUT, the time that elapses between a complete blink and the appearance of the first break in the tear film, assesses tear film evaporation rates.81 During a TBUT assessment, instilling sodium fluorescein stain can help the tear film be more visible. Alternatively, non-invasive breakup time assessments involve observing the specular reflection of an illuminated grid pattern from the tear film.81 To evaluate tear film production, the Schirmer test uses standardized strips of filter paper placed in the temporal inferior cul-de-sac. After 5 minutes, the length of wetting on the paper is measured, with values <10 mm indicating meaningfully reduced tear production.81,86 Interferometry permits determination of the tear film’s LLT, which appears thinner in patients with DED versus healthy controls.87 Additionally, tear film hyperosmolarity, a defining characteristic of DED, is often assessed via electrical impedance.87
The Remaining Challenge in DED Diagnosis in MENA
One significant challenge of identifying and treating DED in MENA is the lack of awareness of this disease among non-ophthalmic practitioners and general ophthalmologists. DED is often misdiagnosed as allergic conjunctivitis in MENA, so it should be classified in terms of pathophysiology and severity, using both signs and symptoms.88 Additionally, many systemic diseases are associated with DED (eg, Sjögren syndrome, rheumatoid arthritis, systemic lupus erythematosus, thyroid conditions; Table 1), which may complicate DED diagnosis and its treatment.38
Additionally, MENA has very few ocular surface and corneal specialists, so ocular surface diseases are often managed by general ophthalmologists. For example, there are about 500 ophthalmologists in Lebanon, with only 35 ocular surface and corneal specialists.71 Another major gap in MENA is the lack of validated questionnaires adapted to the local languages for more standardized data collection and proper scoring and analyses. We recommend a minimal diagnostic assessment tool to improve the diagnosis and management of DED in MENA (Table 3). To facilitate the diagnosis and treatment of DED in MENA, therefore, education on the ocular surface can be improved among general ophthalmologists, and minimal diagnostic procedures should be standardized.
 |
Table 3 Minimal Diagnostic Assessment Tool for Patients Seeking Care for Dry Eye Disease |
Therapeutic Tools
DED treatment should aim to address the major cause of DED in each patient (ie, aqueous deficiency or hyper-evaporation). The main factors influencing disease management are the severity of the disease, the underlying etiology, and the response to treatment. However, other factors may influence the selection of treatment, such as access to reimbursement, cost of treatment, patient adherence, socioeconomic status, distance from the treatment center, and age.89 DED management and treatment recommendations should be done in stages, but therapies must be tailored to individual patient profiles and needs.90
Tear Substitutes
Tear replacement with tear substitutes (TSs; also known as artificial tears) is the mainstay of DED treatment. Many different classes and formulations are available, including drops, gels, ointments, and lubricants, mainly as over-the-counter (OTC) products, and their availability differs significantly among MENA countries.90 The main types of ingredients used in the composition of TSs are viscosity-enhancing agents (eg, hyaluronic acid [HA]), osmoprotectants, lipids, antioxidants, and vitamins.91
TSs have widely different properties in terms of composition, water-binding capacity, ocular surface residency time, viscosity, osmolarity/osmolality, and pH. Each of these properties may affect a drop’s overall effect, use, and tolerability, ultimately influencing their ability to protect and restore the damaged ocular surface.92 To determine the suitability of a TS for treating DED, it is important to assess its physical properties. TSs with moderately high viscosity and a near-physiological pH provide good tear distribution and ocular comfort; however, very high viscosity formulations may be uncomfortable for the patient.93–95 Polymers, such as hyaluronic acid or carboxymethyl cellulose sodium, are sometimes included in TSs. Polymers tend to have similar effects on DED signs and symptoms despite any molecular differences,96 but TS formulations containing multiple polymers been shown to improve tear film characteristics.95
Viscosity-Enhancing Agents
Carboxymethylcellulose (CMC) is a common viscosity-enhancing agent used in TSs91 that is beneficial for patients with mild to moderate DED; it improves corneal surface wettability and tear film integrity.97 Other viscosity-enhancing agents used in TSs include hydroxypropyl methylcellulose (HPMC), carbomers, HA, polyvinyl alcohol, povidone, dextran, and hydroxypropyl-guar (HP-guar). These agents have mucoadhesive and mucomimetic properties and play a protective role on the ocular surface. Carbomers increase the viscosity and thickness of tears and decrease drag during blinking. They also improve hydration and alleviate irritation due to dry eye. Many TSs include HA, a natural component of the tear film that is also present in the outer cornea and vitreous.98
HA has water-binding, lubricating, and antioxidant properties on the ocular surface,2 and HA-based TSs—at an optimal concentration of 0.2%—have epithelium-healing properties,99 reduce squamous metaplasia, and improve goblet cell and epithelial cell morphology.98 In ophthalmic formulations, HA concentrations range between 0.1% and 0.4%, which are considered safe and effective for treating DED. There are some gaps in the literature regarding the optimal concentration, drop frequency, and molecular weight of HA, and potential differences exist in optimizing treatment for different severities and subtypes of DED.2 HA concentrations of 0.1% and 0.2% resulted in improved TBUT and ocular surface staining compared to placebo drops,2 and patients subjectively preferred 0.2% HA over 0.1% HA.2 Generally, TSs with 0.1% and 0.2% HA produce symptom relief, greater patient comfort, and improved objective and subjective measures of dry eye.2 Some have postulated that improved Schirmer test scores reported in the literature could be due to the resolution of ocular inflammation by HA, leading to improved lacrimal gland function.2 Studies of higher HA concentrations (>0.2%) reported longer tear film stability and transient visual blur that resolved within 5 minutes of administration.2,100
Previous studies have investigated low (60 kDa) to high (3000 kDa) molecular weight HA.2,100 Higher molecular weight HA has antiangiogenic, anti-inflammatory, and immunosuppressive properties,2 whereas low molecular weight HA can be pro-inflammatory.
HA is considered a non-Newtonian fluid that changes its viscosity against shear stress, such as blinking, mimicking the normal tear film.101 This non-Newtonian behavior allows HA to have thicker viscosity when the eye is open, increasing its ocular surface residence time, thereby reducing evaporation. During blinks, however, the viscosity of HA decreases, reducing the amount of the molecule that is washed out from the ocular surface and preventing friction-related ocular tissue damage.101 Additionally, differences in physiochemical properties of various HA molecules result in variant-specific rheological properties that could be optimized for particular clinical situations. In patients with elevated ocular surface inflammation and epithelial damage, for example, high molecular weight HA—with higher viscosity at low shear stress—may be more appropriate than a lower molecular weight, less viscous HA molecule.101 Once inflammation and epithelial damage has resolved, patients can be transitioned to a lower-viscosity HA to maintain a stable tear film quality.101
HA receptors are present in the cornea and may be involved in the wound-healing properties of this substance.99 HA stimulates corneal epithelial repair both in vitro and in vivo in a concentration-dependent manner.99 A study by Camilleri et al of denuded rabbit corneas found that 0.2% HA stimulated corneal epithelial migration for different ranges of molecular weight of HA.99
Lipid-based TSs may substitute for a deficient lipid layer and are indicated in evaporative or mixed DED with both aqueous-deficient and evaporative components. Lipid-based TSs can reduce dry eye symptoms, decrease evaporation, increase tear film stability, and mitigate the effect of ocular surface lesions.102–104
Osmoprotectants
Hyperosmolarity induced by DED causes apoptosis of corneal and conjunctival epithelial cells. Osmoprotectants such as L-carnitine, erythritol, betaine, sorbitol, glycerin, and trehalose have been used in some TS formulations to help prevent apoptosis, with positive experimental and clinical results.91
Ectoin is a bacteria-derived extremolyte with the ability to protect proteins and biological membranes from damage caused by extreme environmental conditions such as heat, ultraviolet light, high osmolarity, or desiccation. Ectoin is used as a primary treatment in many DED cases or as an adjuvant with other TSs. Ectoin seems to be effective in alleviating the symptoms of DED as well as VKC, but clinical data are limited.105
Topical Vitamins
Dexpanthenol is a provitamin and an alcohol analog of vitamin B5 (pantothenic acid). In vitro studies indicate that dexpanthenol promotes corneal and conjunctival epithelial healing,106,107 and a randomized controlled trial (RCT) reported that dexpanthenol improved disturbances in corneal epithelium permeability in patients with DED.108
Vitamin B12 (cyanocobalamin) eye drops have proven effective at improving both corneal epithelial healing and nerve regeneration in an animal model of DED.109 Sodium hyaluronate eye drops containing vitamin B12 are commonly used for improving the corneal epithelium.110
Vitamin A increases the expression of conjunctival mucins, promotes corneal and conjunctival wound healing, and reduces corneal keratinization. Several studies confirmed the efficacy of topical vitamin A (either as an ointment or eye drop) for reducing the signs and symptoms of DED.107
Preserved Vs Preservative-Free, and Multidose Vs Unidose DED Treatments
Preservative-free eye drops are preferable in the treatment of DED, but in cases of very mild dryness with only occasional use of lubricants, some preservatives might be clinically acceptable.
Despite the possible harmful effects of preservatives on the ocular surface, it is important to remember that preservative-free preparations carry the potential risk of microbial contamination, and single-dose therapies should be discarded immediately after use. Additionally, cost assessment is important when choosing the best eye drops for each patient, considering that preservative-free eye drops are often more expensive. Ideally, all prescribed dry eye products should be supplied in unit-dose or preservative-free multidose bottles. Preservative-free alternatives should be recommended, especially for patients who require frequent daily instillation, such as patients with severe DED.90
Multidose containers are more cost-effective, convenient, and carry a better carbon footprint than single-dose containers. Unidose drops may be more expensive in some countries—though prices are similar across the Gulf region—and can be difficult to handle for some patients. The opened containers may be reused, though there is a risk of ocular complications. Additionally, unidose formulations have a relatively long shelf life, while opened multidose vials should be consumed within a given time, especially if preservative-free. For the best overall patient adherence and outcomes, patient preference must be considered when selecting a treatment program for DED.
Topical Anti-Inflammatory/Immunomodulatory Agents
Inflammation is a core element of the TFOS DEWS II definition of DED. Ocular surface inflammation in DED is caused by damage induced by hyperosmolarity and desiccation, which are present to some degree in virtually all patients with DED. Anti-inflammatory and immunomodulatory agents are essential in treating DED to break the inflammatory cycle that induces and perpetuates ocular surface damage.84
Steroids
Topical steroids such as loteprednol etabonate (LE), dexamethasone, prednisone, methylprednisolone, fluorometholone, and hydrocortisone are effective in breaking the inflammatory cycle in DED.111 Topical steroids can be used to rapidly decrease DED signs and symptoms, and in severe cases requiring ophthalmic cyclosporine, they can also help improve tolerance to cyclosporine.112,113 Topical steroids may be prescribed for a short-term course to treat disease flares, but long-term use of topical corticosteroids is not recommended due to the risk of steroid-related side effects, such as increased intraocular pressure (IOP), severe steroid-induced glaucoma, and cataract formation. Steroids with more favorable safety profiles, such as LE, may offer better therapeutic options, with the potential for fewer steroid-related side effects.
Dexamethasone, prednisone, and methylprednisolone can pass through the cornea into the anterior chamber. These molecules are very effective in reducing DED signs and symptoms but are associated with high rates of steroid-induced ocular side effects. For this reason, their use should be restricted to controlling severe disease, in patients with a low steroid response or steroid nonresponders; even in these cases, only short-term therapy should be prescribed.
LE is a steroid therapy developed via retrometabolic drug design, modifying an inactive metabolite of prednisolone acetate, with the goals of preserving prednisolone acetate’s anti-inflammatory effects while enabling rapid metabolism of inactive metabolites, thereby reducing the potential for steroid-related adverse events (AEs). LE effectively reduces the signs and symptoms of moderate to severe DED:114,115 In a prospective, double-masked, multicenter RCT, 0.5% LE started 2 weeks before beginning long-term topical 0.05% cyclosporine provided more rapid improvements in Schirmer scores, ocular surface staining, and DED symptoms compared with topical cyclosporine or TSs alone. Additionally, LE induction therapy significantly improved topical cyclosporine tolerance and decreased the risk of having to stop cyclosporine therapy.112 Additionally, LE therapy seemed to have a lower incidence of AEs such as increased IOP, steroid-induced glaucoma, ocular hypertension, and cataract formation. For these reasons, LE is the only steroid formulation that can be used for extended periods of time.114–116
Fluorometholone can reduce ocular surface signs in patients with DED and prevent worsening DED due to desiccating stress.117
Hydrocortisone at a low concentration (0.001%) does not reach the aqueous humor118 and is effective at reducing the signs and symptoms of DED, with a very good safety profile.119
Immunomodulatory Agents
Cyclosporine is an immunosuppressive agent that reduces T cell growth and activity.111 Several studies, many of which evaluated patients with DED receiving 0.05% or 0.1% cyclosporine for up to 8 weeks, and meta-analyses support the efficacy of cyclosporine drops for DED.120–123 While cyclosporine does not demonstrate the rapid anti-inflammatory effect of steroids, it is relatively safe and effective for treating both aqueous-deficient and evaporative DED/MGD.111 Additionally, quality of life studies have concluded that topical cyclosporine can be a cost-effective treatment for DED compared to ocular lubricants. The Asclepius Panel recommended a DED treatment paradigm that starts with a steroid, such as LE, for immediate anti-inflammatory action, symptomatic relief, and disease control,123 then at 2 weeks, adding cyclosporine while decreasing the steroid frequency, which can help encourage patient adherence.124 Because cyclosporine and LE act on different steps of the inflammatory cascade, their concomitant use can have a synergistic effect.124 Additionally, maintaining the steroid therapy throughout cyclosporine treatment can help alleviate cyclosporine-related stinging, a commonly reported AE.124 Topical cyclosporines, however, are not available in some MENA countries.
Tacrolimus is a macrolide that modulates the immune response by inhibiting T and B cell activation.125,126 Tacrolimus eye drops are effective for severe inflammatory aqueous-deficient DED cases, such as graft-versus-host disease, Sjögren syndrome,125 and severe allergic disease.126 Although multiple studies have reported conflicting data, tacrolimus may be more potent and faster acting than cyclosporine.127,128 In MENA, tacrolimus is available in some countries as an in-house preparation, where it is mainly used for patients with refractory DED or who are intolerant of cyclosporine eye drops.
Lifitegrast is an integrin antagonist, engineered to act as a competitive antagonist to block binding between lymphocyte function-associated antigen 1 (LFA-1) and intercellular adhesion molecule 1 (ICAM-1), inhibiting T cell migration into target tissues, reducing cytokine release, and reducing further T cell recruitment.111 Lifitegrast eye drops have been evaluated in 3 multicenter RCTs, including more than 1000 patients with moderate to severe DED. The outcomes indicate an improvement in the signs or symptoms (not both) with 2 weeks of treatment.129–131 The 5% ophthalmic solution was approved in July 2016 in the United States (US), approved in the United Arab Emirates (UAE) for about 3 years, and has recently been approved in Saudi Arabia.
Blood-derived eye drops, such as autologous or heterologous serum or platelet-rich plasma eye drops, contain a high concentration of proteins, particularly pro-healing molecules such as epithelial neurotrophins.111,132 Blood-derived eye drops directly support corneal epithelial cell proliferation and migration, and they indirectly enhance epithelial viability by binding and neutralizing inflammatory cytokines. Blood-derived eye drops have shown efficacy for managing DED, improving signs and symptoms within a few weeks. However, because these treatments are resource-intensive, have limited availability, and can be associated with infectious complications, they are currently reserved for the most severe DED cases.
Inflammatory Modulation with Systemic and Topical Antibiotics
Systemic tetracycline, tetracycline analogues (eg, doxycycline, minocycline), and macrolides (eg, azithromycin) may decrease bacterial load across a range of tissues, including the ocular surface. By reducing the levels of bacteria that produce lipolytic exo-enzymes and lipases, for example, systemic antibiotics can positively impact the meibum for patients with MGD. Additionally, while systemic antibiotics are typically thought of in terms of their anti-bacterial effects, they also have anti-inflammatory properties, including at the ocular surface.111
Systemic tetracyclines, however, may cause gastrointestinal symptoms and photosensitivity, can interact with anticoagulant therapy, and are contraindicated during pregnancy and in children younger than 8 years old. Additionally, systemic macrolides can cause diarrhea, nausea, and vomiting.
To reduce systemic side effects, antibiotics can be used to treat ocular surface conditions via topical administration: topical azithromycin is effective in the management of MGD and evaporative DED.111 Thus, the panel agreed that topical azithromycin is preferred in cases of isolated DED, and systemic antibiotics should be reserved for cases resistant to topical treatment and/or cases associated with other systemic features, such as acne rosacea, which require systemic treatment. Currently, there is no standardization on the optimal posology and modalities of prescription of these agents.
Dietary and Lifestyle Factors
Many clinicians recommend, and many patients take, omega-3 fatty acid dietary supplements, which can have some anti-inflammatory activity. However, contradictory evidence has been published (as discussed above) of the effectiveness of omega-3 fatty acid supplementation in improving symptoms or signs of DED.65,133 Currently, there are no data available on omega-3 intake and DED in MENA.
Lifestyle Interventions
The panel agreed that eye care providers should advise their patients with DED to minimize time spent on digital devices and video display terminals and to reduce smoking and exposure to smoke, though clinical studies on associations between smoking and/or smoke exposure and DED are not conclusive.
Some case reports have described encouraging results for patients with DED who use moisture chamber goggles and air humidifiers. Currently, there are no RCTs that have investigated the therapeutic value of these devices, but we think that these could be a potential adjunct to prescription treatments, especially in conditions that may promote dry eye symptoms, such as AC.111
Other Procedures
Lacrimal occlusion with punctal or canalicular plugs has been used to treat DED for decades. Punctal plugs typically are associated with a low rate of AEs, and they are effective for retaining the natural tear film and prolonging the effect of tear substitutes in DED. Their use is recommended in patients with aqueous deficient DED.111,134 A wide variety of punctal plugs are available, with multiple options for plug designs, placement (ie, punctal vs canalicular), and resorbability. The indications for punctal plugs have expanded, now including numerous ocular surface diseases. Their use for managing evaporative DED, however, remains controversial, even though clinical data indicate that punctal plugs are effective in treating evaporative dry eye and improving meibomian gland status and lipid layer stability.111 One caveat to the use of punctal plugs in DED is that they should not be used in active inflammatory ocular surface disease as they reduce the ability of the ocular surface to flush out circulating toxins, exacerbating dry eye signs and symptoms.
Additional treatments that may help patients with more difficult-to-treat DED include bandage and scleral contact lenses and autologous serum eye drops.111 Bandage contact lenses protect the cornea and decrease the abrasive effects of eyelids during blink. Bandage contact lenses can facilitate corneal tissue repair, decrease pain, stabilize the tear film, and restore normal epithelial cell turnover.135 Scleral contact lenses also protect the ocular surface and maintain ocular surface hydration.135 Autologous serum eye drops are used in a variety of ocular surface conditions—most importantly, DED, non-healing corneal epithelial defects, and neurotrophic keratopathy—and they are believed to contain multiple factors that stimulate ocular surface healing.136 However, a meta-analysis of several clinical trials evaluating the effects of autologous tears found that they provide inconsistent benefit; additionally, there is a need for more standardized questionnaires and objective clinical tests to assess the value of autologous tears in the treatment of DED.137
In-Office Treatments for MGD
As a first line of treatment, many eye care providers recommend improving eyelid hygiene, which can be achieved using eyelid-warming masks (eg, EyeBag, EyeBag Company Ltd, Halifax, West Yorkshire, UK; Therapearl Bausch + Lomb Inc, Rochester, NY, USA; and Eyegiene, Eyedetec Medical Inc, Danville, CA, USA), which facilitate meibum expression. Beyond these devices, a variety of in-office treatments are now available to treat MGD.
Thermal pulsation systems (TPSs) combine heat and mechanical compression of the meibomian glands. Commercially available systems include Lipiflow (Johnson and Johnson Inc, New Brunswick, NJ, USA), Ilux (Alcon Inc, Fort Worth, TX, USA), and Tearcare (Sight Sciences, Menlo Park, CA, USA). In patients with MGD, TPSs improve symptoms overall and enhance tear film stability.138 Additionally, TPSs may provide more sustained improvements than traditional eyelid hygiene,138 but the long-term efficacy of TPSs needs further evaluation.139
Intense pulse light (IPL) therapy delivers pulses of non-coherent light (500 to 1200 nm) to the eyelids to improve meibum expression.139 A recent systematic review and meta-analysis concluded that, though IPL therapy alone is not superior to eyelid hygiene alone,140 it may be an effective and relatively safe treatment for MGD when combined with meibomian gland expression. IPL therapy does not always provide consistent results, with its efficacy being influenced by the number and frequency of treatments.140 Additionally, the efficacy of IPL therapy may decrease within 6 months after the last treatment.140 Contraindications to the use of IPL therapy are epilepsy, pregnancy, metal implants, photosensitivity or photosensitizing treatments, and active infection. Additionally, IPL therapy may not be tolerated well on darker skin tones, hence limiting use in the MENA region.
Intraductal probing of meibomian glands with a microcannula is performed at the slit lamp and can offer symptomatic relief to patients with obstructive MGD.141 It involves passing a 2-mm probe directly into the orifice of each meibomian gland, allowing meibum egress. Although intraductal probing is relatively safe, it can cause lid hemorrhage and may require re-treatments.139
Overall, currently available in-office procedures for DED can help alleviate dry eye signs and symptoms without a high rate of AEs, but their use in MENA is limited due to by-country availability and cost, resulting in a wide disparity in use across the region.
Therapeutic Strategies
A therapeutic strategy should follow the staged management and treatment recommendations for DED published in the TFOS DEWS II report,111 compensating for patient specifics and the local availability of treatments. Table 4 summarizes the main steps adapted from the TFOS DEWS II management report111 and the report from the management and treatment subcommittee, International Workshop on MGD.111,142
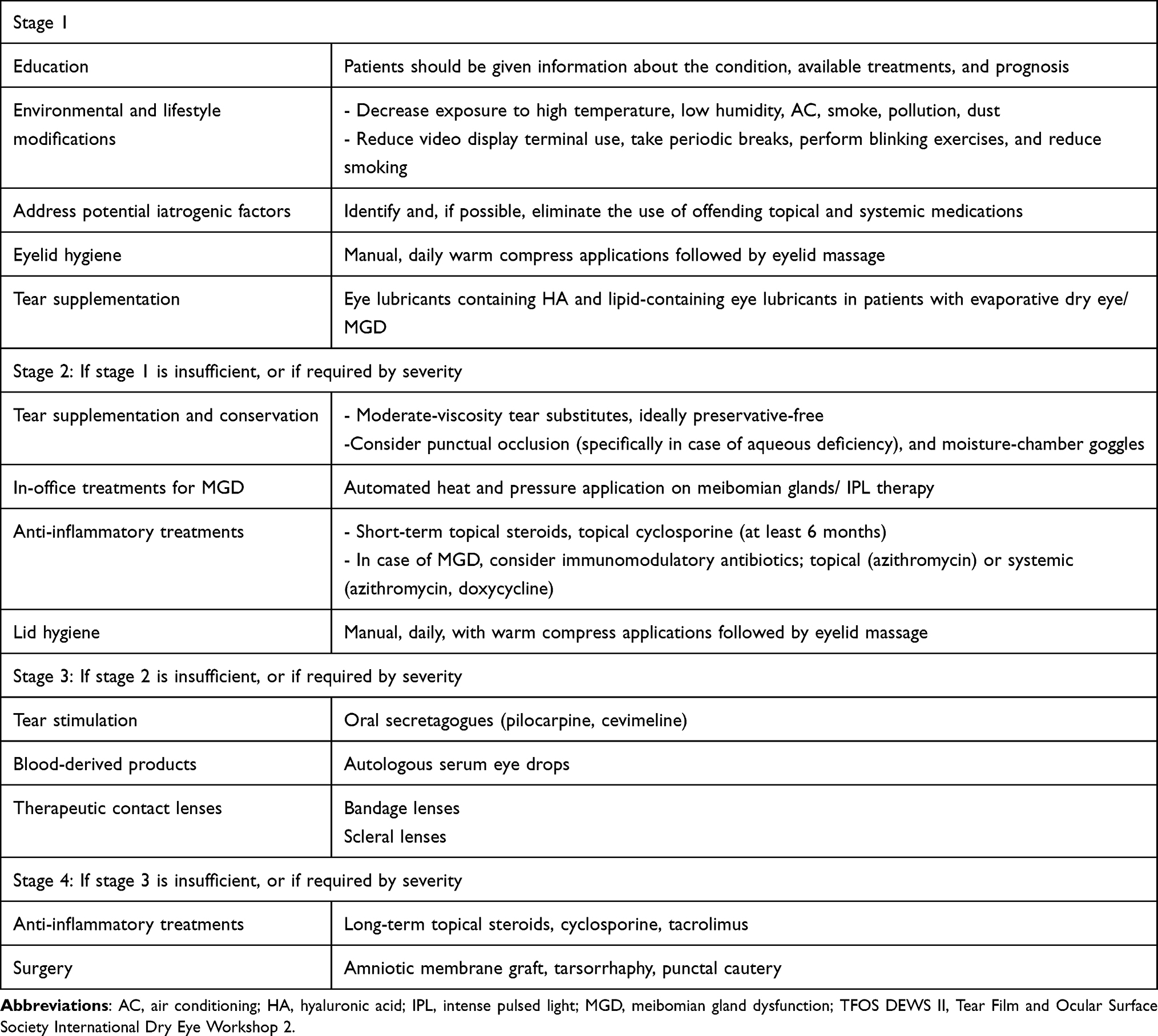 |
Table 4 Staged Treatment of Dry Eye Disease, Adapted from the TFOS DEWS II Management report111 and the Report on the Management and Treatment Subcommittee of the International Workshop on MGD.142 |
Perioperative DED Management
Corneal Refractive Surgery
Corneal refractive surgeries may induce or aggravate preexisting DED that is already prevalent among contact lens wearers seeking refractive surgery. DED can be exacerbated through various mechanisms, including corneal nerve damage, surgical trauma, postoperative inflammation, and toxicity of perioperative eye drops.143 Preoperative DED may cause topographical errors, which can be detrimental to the final refractive results. Postoperative DED may last up to 12 months and alter the quality of vision and the quality of life and is considered a major cause of dissatisfaction after refractive surgery. Therefore, every candidate for corneal refractive surgery should undergo a thorough preoperative evaluation of the ocular surface, including an assessment of risk factors, symptoms, and comprehensive clinical examination.
As there is often a mismatch between symptoms and signs in dry eyes, using several tests, such as questionnaires, slit-lamp examination, and tear film biomarkers (osmolarity and staining), could be extremely helpful for detecting as many patients with DED as possible.
If a patient with DED is determined to undergo refractive surgery, the dry eye should be treated before proceeding with surgery. Treatment options include TS, nutritional supplementation, topical cyclosporine, topical steroids, and punctal plugs.143 The duration of preoperative treatment should be based on the status of the DED symptoms. The choice of the procedure should be based on DED status, as LASIK is considered a greater risk for postoperative DED than surface ablation or small incision lenticule extraction (SMILE).144 The panel agreed that preoperative optimization of the ocular surface decreases the incidence and severity of postoperative symptoms of the condition.145
Cataract Surgery
Increased life expectancy in the general MENA population has resulted in a greater number of patients presenting for cataract surgery, as well as an increasing prevalence of DED signs and symptoms in the elderly. Low-grade and/or non-symptomatic DED is extremely common in cataract surgery candidates and can be exacerbated postoperatively. In the PHACO study, a prospective, multicenter, observational study of 136 patients who were scheduled to undergo cataract surgery, the majority of patients (62.9%) had a TBUT ≤5 seconds, 77% of eyes had positive corneal staining, and 50% of eyes had positive central corneal staining. Eighteen percent had a Schirmer score with anesthesia ≤5 mm.146
Additionally, DED can induce errors in IOL power calculation due to inaccurate keratometry measurements.147,148 It can also falsely induce higher-order aberrations and irregular astigmatism, thus limiting the use of premium IOLs.
DED can impair the postoperative quality of vision and comfort, resulting in an unsatisfied patient and an unsatisfied surgeon. Hence, preoperative evaluation for DED for all cataract candidates is crucial to mitigate these risks.148
Preoperative evaluation should be standardized and include both an assessment of the symptoms and a comprehensive clinical examination of the ocular surface.149 Preoperative treatment is adapted to the clinical findings and treatment should follow the same staged system outlined above.
Cataract surgery may exacerbate DED between 1 week and 3 months postoperatively. Hence, patients should be adequately treated with preservative-free eye drops, TS, and steroids with close postoperative follow-up. Non-steroidal eye drops should be avoided in patients with DED because there is an increased risk of corneal melting and perforation. Intraoperatively, exacerbation of dry eye may be mitigated by a short duration of surgery and reduced exposure to microscope lighting. It has been postulated that coating the cornea with an ophthalmic viscosurgical device instead of frequent balanced salt solution (BSS) instillation can protect the ocular surface and lower the incidence and severity of DED postoperatively.
Conclusions
DED has specific epidemiologic features in MENA due to climatic, lifestyle, and iatrogenic factors. Management of DED should account for pathophysiology, patient lifestyle, and whether the patient may undergo LASIK or cataract surgery in the near future.
The initial patient history and, perhaps, language-specific and culturally appropriate DED questionnaires can serve as an appropriate first step in screening. The constellation of signs and symptoms in DED overlap across mild, moderate, and severe disease, and the outcomes of a thorough history-taking, along with the responses to questionnaires, may aid in determining appropriate management. The lack of availability of some diagnostic tests and therapeutic options in MENA limits our ability to propose specific criteria for diagnosis and management. Additionally, the education of ophthalmologists and general healthcare providers on ocular surface diseases remains a challenge in many regions in MENA.
As with any scientific article, the present document comes with limitations. As a consensus document, the statements herein are derived from a panel of experts. However, such panels are of limited size, and individual members inherently have personal biases. Achieving consensus on the statements in this article, however, ensures that they are not merely a single person’s thought, but are ideas supported by multiple people, all of whom are experts in the area. Thus, while the n-value may be limited, the quality of each panel participant is very high,150 and consensus documents are viewed throughout the scientific community as an important adjunct to formal treatment guidelines.151
The broader implications are that DED in the MENA region is likely much more common than the current literature indicates. Patient and physician education is a critical first step in addressing the public health burden of DED in the region. Furthermore, population-based studies in MENA on the epidemiology, diagnosis, and management of DED are warranted in the future.
Funding
Bausch & Lomb provided funding for the author meetings for the development of this manuscript and for the Open Access to this manuscript. Emmanuelle Gorsse of JBH Sante, France provided editorial support, and this service was paid for by Bausch & Lomb. The authors were involved in the entire process, from design to critical revision of the manuscript, and maintained complete control over its direction and content. Bausch & Lomb did not have any influence on the manuscript content.
Disclosure
Dr. Sihem Lazreg has acted as occasional consultant for Thea, Bausch & Lomb, Allergan, Quantel, Santen and Orchedia.
Dr. Mohamed Hosny has acted as occasional consultant for Alcon, Ziemer, Schwind, Tracey and Bausch & Lomb.
Dr. Muhammad Ahad has acted as occasional consultant for Bausch & Lomb, AbbVie and Alcon.
Dr. Mazen Sinjab has acted as occasional consultant for Bausch & Lomb.
Dr. Riadh Messaoud has acted as occasional consultant for Bausch & Lomb, Thea and Unimed.
Dr. Shady T. Awwad has acted as occasional consultant for Bausch & Lomb.
Dr. Rousseau has acted as occasional consultant for AbbVie, Horus Pharma, Glaukos, Thea, received speaker honoraria from AbbVie, Horus Pharma, Bausch & Lomb, Alnylam, Thea, travel grants from Horus Pharma, Thea, personal fees from Santen and research grant from Alnylam, Thea.
Authors have no other conflicts of interest to declare in this paper.
References
1. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
2. Hynnekleiv L, Magno M, Vernhardsdottir RR, et al. Hyaluronic acid in the treatment of dry eye disease. Acta Ophthalmol. 2022;100(8):844–860. doi:10.1111/aos.15159
3. O’Brien PD, Collum LM. Dry eye: diagnosis and current treatment strategies. Curr Allergy Asthma Rep. 2004;4(4):314–319. doi:10.1007/s11882-004-0077-2
4. Labetoulle M, Rolando M, Baudouin C, van Setten G. Patients’ perception of DED and its relation with time to diagnosis and quality of life: an international and multilingual survey. Br J Ophthalmol. 2017;101(8):1100–1105. doi:10.1136/bjophthalmol-2016-309193
5. Clegg JP, Guest JF, Lehman A, Smith AF. The annual cost of dry eye syndrome in France, Germany, Italy, Spain, Sweden and the United Kingdom among patients managed by ophthalmologists. Ophthalmic Epidemiol. 2006;13(4):263–274.
6. Bukhari A, Ajlan R, Alsaggaf H. Prevalence of dry eye in the normal population in Jeddah, Saudi Arabia. Orbit. 2009;28(6):392–397. doi:10.3109/01676830903074095
7. Alshamrani AA, Almousa AS, Almulhim AA, et al. Prevalence and risk factors of dry eye symptoms in a Saudi Arabian population. Middle East Afr J Ophthalmol. 2017;24(2):67–73. doi:10.4103/meajo.MEAJO_281_16
8. Sherry A, Aridi M, Ghach W. Prevalence and risk factors of symptomatic dry eye disease in Lebanon. Cont Lens Anterior Eye. 2020;43(4):355–358. doi:10.1016/j.clae.2019.08.001
9. Yasir ZH, Chauhan D, Khandekar R, Souru C, Varghese S. Prevalence and determinants of dry eye disease among 40 years and older population of Riyadh (except capital), Saudi Arabia. Middle East Afr J Ophthalmol. 2019;26(1):27–32. doi:10.4103/meajo.MEAJO_194_18
10. Alkabbani S, Jeyaseelan L, Rao AP, Thakur SP, Warhekar PT. The prevalence, severity, and risk factors for dry eye disease in Dubai - A cross sectional study. BMC Ophthalmol. 2021;21(1):219. doi:10.1186/s12886-021-01978-4
11. Perez VL, Stern ME, Pflugfelder SC. Inflammatory basis for dry eye disease flares. Exp Eye Res. 2020;201:108294. doi:10.1016/j.exer.2020.108294
12. Periman LM, Perez VL, Saban DR, Lin MC, Neri P. The immunological basis of dry eye disease and current topical treatment options. J Ocul Pharmacol Ther. 2020;36(3):137–146. doi:10.1089/jop.2019.0060
13. Kumar NR, Praveen M, Narasimhan R, et al. Tear biomarkers in dry eye disease: progress in the last decade. Indian J Ophthalmol. 2023;71(4):1190. doi:10.4103/IJO.IJO_2981_22
14. Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II report executive summary. Ocul Surf. 2017;15(4):802–812. doi:10.1016/j.jtos.2017.08.003
15. Sun M, Moreno IY, Dang M, Coulson-Thomas VJ. Meibomian gland dysfunction: what have animal models taught us? Int J Mol Sci. 2020;21(22):8822. doi:10.3390/ijms21228822
16. Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea. 2012;31(5):472–478. doi:10.1097/ICO.0b013e318225415a
17. Chhadva P, Goldhardt R, Galor A. Meibomian gland disease: the role of gland dysfunction in dry eye disease. Ophthalmology. 2017;124(11):S20–S26. doi:10.1016/j.ophtha.2017.05.031
18. Kim WJ, Ahn YJ, Kim MH, Kim HS, Kim MS, Kim EC. Lipid layer thickness decrease due to meibomian gland dysfunction leads to tear film instability and reflex tear secretion. Ann Med. 2022;54(1):893–899. doi:10.1080/07853890.2022.2056238
19. Li J, Ma J, Hu M, Yu J, Zhao Y. Assessment of tear film lipid layer thickness in patients with Meibomian gland dysfunction at different ages. BMC Ophthalmol. 2020;20(1):394. doi:10.1186/s12886-020-01667-8
20. Covita A CM, Leahy C. Correlation between meibomian gland appearance and tear breakup time using a slit scanning ophthalmoscope. Invest Ophthalmol Vis Sci. 2019;60(9):6793.
21. Doctor MB, Basu S. Lacrimal gland insufficiency in aqueous deficiency dry eye disease: recent advances in pathogenesis, diagnosis, and treatment. Semin Ophthalmol. 2022;37(7–8):801–812. doi:10.1080/08820538.2022.2075706
22. Li DQ, Luo L, Chen Z, Kim HS, Song XJ, Pflugfelder SC. JNK and ERK MAP kinases mediate induction of IL-1beta, TNF-alpha and IL-8 following hyperosmolar stress in human limbal epithelial cells. Exp Eye Res. 2006;82(4):588–596. doi:10.1016/j.exer.2005.08.019
23. Papas EB. The global prevalence of dry eye disease: a Bayesian view. Ophthalmic Physiol Opt. 2021;41(6):1254–1266. doi:10.1111/opo.12888
24. Wan Y, Zhang M, Li X. The global prevalence of dry eye disease and its association with economy: a systematic review. Res Square. 2019;2019:1.
25. Berg EJ, Ying GS, Maguire MG, et al. Climatic and environmental correlates of dry eye disease severity: a report from the Dry Eye Assessment and Management (DREAM) Study. Transl Vis Sci Technol. 2020;9(5):25. doi:10.1167/tvst.9.5.25
26. Aljarousha MA, Badarudin NE, Che Azemin MZ, Aljeesh Y, Abuimara A. A systematic review on prevalence, risk factors, clinical diagnosis and medical management of dry eye disease in the Arab population. dry eye; artificial tears; contact lenses; glaucoma; Arab population. Afr Vision Eye Health. 2021;80(1):a591. doi:10.4102/aveh.v80i1.591
27. Gantz L, Rosenfield M. Digital eye strain symptoms during online university learning in Israel and the USA during the COVID-19 pandemic. Invest Ophthalmol Vis Sci. 2021;62(8):1975.
28. Ghach W, Bakkar MM, Aridi M, Beshtawi I, Doughaily R, Al-Fayoumi N. Prevalence and behavioral-based risk factors (eye cosmetic and tobacco use) of symptomatic dry eye disease in four Middle Eastern countries: Lebanon, Syria, Jordan, and Palestine. Clin Ophthalmol. 2022;16:3851–3860. doi:10.2147/OPTH.S385040
29. Köksoy Vayısoğlu S, Öncü E, Dursun Ö, Dinç E. Investigation of dry eye symptoms in lecturers by ocular surface disease index. Turk J Ophthalmol. 2019;49(3):142–148. doi:10.4274/tjo.galenos.2018.67915
30. Binyousef FH, Alruwaili SA, Altammami AF, Alharbi AA, Alrakaf FA, Almazrou AA. Impact of dry eye disease on work productivity among Saudi workers in Saudi Arabia. Clin Ophthalmol. 2021;15:2675–2681. doi:10.2147/OPTH.S313158
31. Labbé A, Wang YX, Jie Y, Baudouin C, Jonas JB, Xu L. Dry eye disease, dry eye symptoms and depression: the Beijing Eye Study. Br J Ophthalmol. 2013;97(11):1399–1403. doi:10.1136/bjophthalmol-2013-303838
32. Wan KH, Chen LJ, Young AL. Depression and anxiety in dry eye disease: a systematic review and meta-analysis. Eye. 2016;30(12):1558–1567. doi:10.1038/eye.2016.186
33. Al-Dairi W, Al Sowayigh OM, Alkulaib NS, Alsaad A. The relationship of dry eye disease with depression in Saudi Arabia: a cross-sectional study. Cureus. 2020;12(12):1.
34. Almutairi R, Algezlan S, Bayamin R, et al. The association between dry eye and sleep quality among the adult population of Saudi Arabia. Cureus. 2022;14(3):1.
35. Rana HS, Akella SS, Clabeaux CE, Skurski ZP, Aakalu VK. Ocular surface disease in thyroid eye disease: a narrative review. Ocul Surf. 2022;24:67–73. doi:10.1016/j.jtos.2022.02.001
36. Lemp MA. Dry eye (keratoconjunctivitis sicca), rheumatoid arthritis, and Sjögren’s syndrome. Am J Ophthalmol. 2005;140(5):898–899. doi:10.1016/j.ajo.2005.06.031
37. Ziaragkali S, Kotsalidou A, Trakos N. Dry eye disease in routine rheumatology practice. Mediterr J Rheumatol. 2018;29(3):127–139. doi:10.31138/mjr.29.3.127
38. Golden MI, Meyer JJ, Patel BC. Dry eye syndrome. In: StatPearls. StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC.; 2023.
39. Ben-Eli H, Aframian DJ, Ben-Chetrit E, et al. Shared medical and environmental risk factors in dry eye syndrome, Sjogren’s syndrome, and B-cell non-Hodgkin lymphoma: a case-control study. J Immunol Res. 2019;2019:9060842. doi:10.1155/2019/9060842
40. Amoatey P, Omidvarborna H, Baawain MS, Al-Mamun A, Bari A, Kindzierski WB. Association between human health and indoor air pollution in the Gulf Cooperation Council (GCC) countries: a review. Rev Environ Health. 2020;35(2):157–171. doi:10.1515/reveh-2019-0065
41. García-Marqués JV, Talens-Estarelles C, García-Lázaro S, Wolffsohn JS, Cerviño A. Systemic, environmental and lifestyle risk factors for dry eye disease in a Mediterranean caucasian population. Cont Lens Anterior Eye. 2022;45(5):101539. doi:10.1016/j.clae.2021.101539
42. Iyer JV, Lee SY, Tong L. The dry eye disease activity log study. ScientificWorldJournal. 2012;2012:589875. doi:10.1100/2012/589875
43. Hereher M, Eissa R, Alqasemi A, El Kenawy AM. Assessment of air pollution at Greater Cairo in relation to the spatial variability of surface urban heat island. Environ Sci Pollut Res Int. 2022;29(15):21412–21425. doi:10.1007/s11356-021-17383-9
44. Yu D, Deng Q, Wang J, et al. Air pollutants are associated with dry eye disease in urban ophthalmic outpatients: a prevalence study in China. J Transl Med. 2019;17(1):46. doi:10.1186/s12967-019-1794-6
45. Hilmi MR, Kamal K, Ariffin A, et al. Effects of different types of primary pterygium on changes in oculovisual function. Sains Malays. 2020;49:383–388. doi:10.17576/jsm-2020-4902-16
46. Hilmi MR, Khairidzan MK, Azemin M. Changes in apical corneal curvature in unilateral primary pterygium and normal adults using simulated-K and corneal irregularity measurement. Internat J Allied Health Sci. 2019;3:588–594.
47. Azemin MZC, Tamrin MIM, Hilmi MR, Kamal KM. Inter-grader reliability of a supervised pterygium redness grading system. Adv Sci Lett. 2016;22(10):2885–2888. doi:10.1166/asl.2016.7125
48. Tan J, Vollmer-Conna U, Tat L, Coroneo M. Dry-eye disease in recurrent pterygium. Ophthalmic Res. 2019;61(4):199–203. doi:10.1159/000493544
49. Gomes JAP, Azar DT, Baudouin C, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2017;15(3):511–538. doi:10.1016/j.jtos.2017.05.004
50. Alamri A, Amer KA, Aldosari AA, et al. Assessment of dry eye syndrome among contact lens users in Asir region, Saudi Arabia. Cureus. 2022;14(1):1.
51. Mohamed MS, Abu-Steit MH, Shalaby AM, Sherif AM. Evaluation of dry eye syndrome after LASIK and surface ablation: a comparative study. J Egypt Ophthalmol Soc. 2015;108(4):221–226. doi:10.4103/2090-0686.174681
52. Miura M, Inomata T, Nakamura M, et al. Prevalence and characteristics of dry eye disease after cataract surgery: a systematic review and meta-analysis. Ophthalmol Ther. 2022;11(4):1309–1332. doi:10.1007/s40123-022-00513-y
53. Toda I. LASIK and the ocular surface. Cornea. 2008;27(Suppl 1):S70–S76. doi:10.1097/ICO.0b013e31817f42c0
54. Galor A, Feuer W, Lee DJ, et al. Prevalence and risk factors of dry eye syndrome in a United States veterans affairs population. Am J Ophthalmol. 2011;152(3):377–384.e2. doi:10.1016/j.ajo.2011.02.026
55. Paulsen AJ, Cruickshanks KJ, Fischer ME, et al. Dry eye in the Beaver Dam Offspring Study: prevalence, risk factors, and health-related quality of life. Am J Ophthalmol. 2014;157(4):799–806. doi:10.1016/j.ajo.2013.12.023
56. Leila K, Gatfaoui F, Mahjoub A, et al. [Impact of glaucoma medications and ocular surface disease on the quality of life of glaucoma patients in the district of Sousse (Tunisia)] Impact du traitement antiglaucomateux et de la pathologie de la surface oculaire sur la qualité de vie des patients glaucomateux dans la région de Sousse (Tunisie). J Fr Ophtalmol. 2019;42(5):464–470. doi:10.1016/j.jfo.2018.06.007
57. Lajmi H, Hmaied W, Achour BB, Zahaf A. Risk factors for ocular surface disease in Tunisian users of preserved antiglaucomatous eye drops. J Curr Ophthalmol. 2021;33(2):128–135. doi:10.4103/JOCO.JOCO_226_20
58. Moss SE, Klein R, Klein BE. Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. 2000;118(9):1264–1268. doi:10.1001/archopht.118.9.1264
59. Magno MS, Utheim TP, Morthen MK, et al. The relationship between caffeine intake and dry eye disease. Cornea. 2023;42(2):186–193. doi:10.1097/ICO.0000000000002979
60. Kam KW, Di Zazzo A, De Gregorio C, Narang P, Jhanji V, Basu S. A review on drug-induced dry eye disease. Indian J Ophthalmol. 2023;71(4):1263–1269. doi:10.4103/IJO.IJO_2782_22
61. Kamøy B, Magno M, Nøland ST, et al. Video display terminal use and dry eye: preventive measures and future perspectives. Acta Ophthalmol. 2022;100(7):723–739. doi:10.1111/aos.15105
62. Liu J, Dong Y, Wang Y. Vitamin D deficiency is associated with dry eye syndrome: a systematic review and meta-analysis. Acta Ophthalmol. 2020;98(8):749–754. doi:10.1111/aos.14470
63. Aziz BF, Tawfik CA. Prevalence of dry eye disease among healthy Egyptian population. J Egypt Ophthalmol Soc. 2020;113(4):133–141. doi:10.4103/ejos.ejos_29_20
64. Blachman-Braun R, Del Mazo-Rodríguez RL, López-Sámano G, et al. Hookah, is it really harmless? Respir Med. 2014;108(5):661–667. doi:10.1016/j.rmed.2014.01.013
65. Asbell PA, Maguire MG, Pistilli M, et al. n-3 fatty acid supplementation for the treatment of dry eye disease. N Engl J Med. 2018;378(18):1681–1690.
66. Kuklinski EJ, Hom MM, Ying GS, et al. Associations between systemic omega-3 fatty acid levels with moderate-to-severe dry eye disease signs and symptoms at baseline in the Dry Eye Assessment and Management Study. Eye Contact Lens. 2021;47(1):2–7. doi:10.1097/ICL.0000000000000687
67. Bistrian BR. n-3 fatty acid supplementation and dry eye disease. N Engl J Med. 2018;379(7):690–691.
68. Giannaccare G, Pellegrini M, Sebastiani S, et al. Efficacy of omega-3 fatty acid supplementation for treatment of dry eye disease: a meta-analysis of randomized clinical trials. Cornea. 2019;38(5):565–573. doi:10.1097/ICO.0000000000001884
69. Arabi A, Chamoun N, Nasrallah MP, Tamim HM, Karras S. Vitamin D deficiency in Lebanese adults: prevalence and predictors from a cross-sectional community-based study. Int J Endocrinol. 2021;2021:3170129. doi:10.1155/2021/3170129
70. Dawson CR, Daghfous T, Messadi M, Hoshiwara I, Schachter J. Severe endemic trachoma in Tunisia. Br J Ophthalmol. 1976;60(4):245–252. doi:10.1136/bjo.60.4.245
71. Erickson S, Sullivan AG, Abad JC, et al. TFOS: unique challenges and unmet needs for the management of ocular surface diseases throughout the world. Ocul Surf. 2021;22:242–244. doi:10.1016/j.jtos.2021.08.014
72. Bakkar MM, Shihadeh WA, Haddad MF, Khader YS. Epidemiology of symptoms of dry eye disease (DED) in Jordan: a cross-sectional non-clinical population-based study. Cont Lens Anterior Eye. 2016;39(3):197–202. doi:10.1016/j.clae.2016.01.003
73. Chalmers RL, Begley CG, Caffery B. Validation of the 5-Item Dry Eye Questionnaire (DEQ-5): discrimination across self-assessed severity and aqueous tear deficient dry eye diagnoses. Cont Lens Anterior Eye. 2010;33(2):55–60. doi:10.1016/j.clae.2009.12.010
74. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the Ocular Surface Disease Index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
75. Ngo W, Situ P, Keir N, Korb D, Blackie C, Simpson T. Psychometric properties and validation of the standard patient evaluation of eye dryness questionnaire. Cornea. 2013;32(9):1204–1210. doi:10.1097/ICO.0b013e318294b0c0
76. McMonnies CW. Measurement of symptoms pre- and post-treatment of dry eye syndromes. Optom Vis Sci. 2016;93(11):1431–1437. doi:10.1097/OPX.0000000000000965
77. Al-Mohtaseb Z, Schachter S, Shen Lee B, Garlich J, Trattler W. The relationship between dry eye disease and digital screen use. Clin Ophthalmol. 2021;15:3811–3820. doi:10.2147/OPTH.S321591
78. Karson CN. Spontaneous eye-blink rates and dopaminergic systems. Brain. 1983;106(3):643–653. doi:10.1093/brain/106.3.643
79. Su Y, Liang Q, Su G, Wang N, Baudouin C, Labbé A. Spontaneous eye blink patterns in dry eye: clinical correlations. Invest Ophthalmol Vis Sci. 2018;59(12):5149–5156. doi:10.1167/iovs.18-24690
80. Pult H, Bandlitz S. Lid-parallel conjunctival folds and their ability to predict dry eye. Eye Contact Lens. 2018;44(Suppl 2):S113–S119. doi:10.1097/ICL.0000000000000435
81. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II diagnostic methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
82. Ophthalmology AAO. Pterygium - Middle East/North Africa. 2023. Available from: https://www.aao.org/education/topic-detail/pterygium-middle-east-north-africa.
83. Gupta AKR, Nathwani Y. Correlation between pterygium and dry eye. Kerala J Ophthalmol. 2019;31(3):217–220. doi:10.4103/kjo.kjo_65_19
84. Baudouin C, Irkeç M, Messmer EM, et al. Clinical impact of inflammation in dry eye disease: proceedings of the ODISSEY group meeting. Acta Ophthalmol. 2018;96(2):111–119. doi:10.1111/aos.13436
85. Sweeney DF, Millar TJ, Raju SR. Tear film stability: a review. Exp Eye Res. 2013;117:28–38. doi:10.1016/j.exer.2013.08.010
86. Brott NR, Ronquillo Y. Schirmer Test. In: StatPearls. StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC.; 2023.
87. Herbaut A, Liang H, Denoyer A, Baudouin C, Labbé A. Tear film analysis and evaluation of optical quality: a review of the literature. J Fr Ophtalmol. 2019;42(2):e21–e35. doi:10.1016/j.jfo.2018.12.001
88. Baudouin C, Aragona P, Van Setten G, et al. Diagnosing the severity of dry eye: a clear and practical algorithm. Br J Ophthalmol. 2014;98(9):1168–1176. doi:10.1136/bjophthalmol-2013-304619
89. Al-Maskari AZ, Alarfaj K, Shaheen MS, et al. Middle East preferred practice patterns for dry eye disease: a modified Delphi consensus. Open Ophthalmol J. 2020;15:34–42. doi:10.2174/1874364102115010034
90. Barabino S, Benitez-Del-Castillo JM, Fuchsluger T, et al. Dry eye disease treatment: the role of tear substitutes, their future, and an updated classification. Eur Rev Med Pharmacol Sci. 2020;24(17):8642–8652. doi:10.26355/eurrev_202009_22801
91. Labetoulle M, Benitez-Del-Castillo JM, Barabino S, et al. Artificial tears: biological role of their ingredients in the management of dry eye disease. Int J Mol Sci. 2022;23(5):2434. doi:10.3390/ijms23052434
92. Murube J, Murube A, Zhuo C. Classification of artificial tears. II: additives and commercial formulas. Adv Exp Med Biol. 1998;438:705–715.
93. Arif FH, Kamal MR, Ithnin MK, et al. Evaluation of 18 artificial tears based on viscosity and pH. Malaysian J Ophthalmol. 2020;2(2):96–111. doi:10.35119/myjo.v2i2.109
94. Arif FAC, Hilmi MR, Kamal KM. A prospective contralateral eye comparison of the tolerability of two artificial tears with different physical properties in patients with dry eye disease. Med Hypothesis Discov Innov Optom. 2023;4(1):1–6. doi:10.51329/mehdioptometry167
95. Arif FAC, Hilmi MR, Kamal K, Ithnin M. Comparison of immediate effects on usage of dual polymer artificial tears on changes in tear film characteristics. Mal J Med Health Sci. 2020;17(3):252–258.
96. Arif FAC, Hilmi MR, Md Rejab NS, Wolffsohn JS. Immediate effects of artificial tears with and without preservatives containing hyaluronic acid and carboxymethyl cellulose. Med Hypothesis Discov Innov Optom. 2023;4(3):102–111. doi:10.51329/mehdioptometry179
97. Bruix A, Adán A, Casaroli-Marano RP. [Efficacy of sodium carboxymethylcellulose in the treatment of dry eye syndrome] Eficacia de la carboximetilcelulosa sódica para el tratamiento del síndrome del ojo seco. Arch Soc Esp Oftalmol. 2006;81(2):85–92. doi:10.4321/S0365-66912006000200008
98. Aragona P, Giannaccare G, Mencucci R, Rubino P, Cantera E, Rolando M. Modern approach to the treatment of dry eye, a complex multifactorial disease: a P.I.C.A.S.S.O. board review. Br J Ophthalmol. 2021;105(4):446–453. doi:10.1136/bjophthalmol-2019-315747
99. Camillieri G, Bucolo C, Rossi S, Drago F. Hyaluronan-induced stimulation of corneal wound healing is a pure pharmacological effect. J Ocul Pharmacol Ther. 2004;20(6):548–553. doi:10.1089/jop.2004.20.548
100. Posarelli C, Passani A, Del Re M, et al. Cross-linked hyaluronic acid as tear film substitute. J Ocul Pharmacol Ther. 2019;35(7):381–387. doi:10.1089/jop.2018.0151
101. Aragona P, Simmons PA, Wang H, Wang T. Physicochemical properties of hyaluronic acid-based lubricant eye drops. Transl Vis Sci Technol. 2019;8(6):2. doi:10.1167/tvst.8.6.2
102. Chung SH, Lim SA, Tchach H. Efficacy and safety of carbomer-based lipid-containing artificial tear formulations in patients with dry eye syndrome. Cornea. 2016;35(2):181–186. doi:10.1097/ICO.0000000000000660
103. Baudouin C, Galarreta DJ, Mrukwa-Kominek E, et al. Clinical evaluation of an oil-based lubricant eyedrop in dry eye patients with lipid deficiency. Eur J Ophthalmol. 2017;27(2):122–128. doi:10.5301/ejo.5000883
104. Miháltz K, Faschinger EM, Vécsei-Marlovits PV. Effects of lipid- versus sodium hyaluronate-containing eye drops on optical quality and ocular surface parameters as a function of the meibomian gland dropout rate. Cornea. 2018;37(7):886–892. doi:10.1097/ICO.0000000000001523
105. Bilstein A, Heinrich A, Rybachuk A, Mösges R, Borrelli E. Ectoine in the treatment of irritations and inflammations of the eye surface. Biomed Res Int. 2021;2021:8885032. doi:10.1155/2021/8885032
106. Mencucci R, Favuzza E, Bottino P, et al. A new ophthalmic formulation containing antiseptics and dexpanthenol: in vitro antimicrobial activity and effects on corneal and conjunctival epithelial cells. Exp Eye Res. 2020;201:108269. doi:10.1016/j.exer.2020.108269
107. Fogagnolo P, De Cilla S, Alkabes M, Sabella P, Rossetti L. A review of topical and systemic vitamin supplementation in ocular surface diseases. Nutrients. 2021;13(6):1998. doi:10.3390/nu13061998
108. Göbbels M, Gross D. [Clinical study of the effectiveness of a dexpanthenol containing artificial tears solution (Siccaprotect) in treatment of dry eyes] Klinische Studie zur Wirksamkeit eines dexpanthenolhaltigen Tränenersatzmittels (Siccaprotect) bei der Behandlung Trockener Augen. Klin Monbl Augenheilkd. 1996;209(2–3):84–88. doi:10.1055/s-2008-1035283
109. Romano MR, Biagioni F, Carrizzo A, et al. Effects of vitamin B12 on the corneal nerve regeneration in rats. Exp Eye Res. 2014;120:109–117. doi:10.1016/j.exer.2014.01.017
110. Versura P, Profazio V, Giannaccare G, Fresina M, Campos EC. Discomfort symptoms reduction and ocular surface parameters recovery with Artelac Rebalance treatment in mild-moderate dry eye. Eur J Ophthalmol. 2013;23(4):488–495. doi:10.5301/ejo.5000267
111. Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
112. Sheppard JD, Donnenfeld ED, Holland EJ, et al. Effect of loteprednol etabonate 0.5% on initiation of dry eye treatment with topical cyclosporine 0.05%. Eye Contact Lens. 2014;40(5):289–296. doi:10.1097/ICL.0000000000000049
113. Byun YJ, Kim TI, Kwon SM, et al. Efficacy of combined 0.05% cyclosporine and 1% methylprednisolone treatment for chronic dry eye. Cornea. 2012;31(5):509–513. doi:10.1097/ICO.0b013e31818c69ef
114. Pflugfelder SC, Maskin SL, Anderson B, et al. A randomized, double-masked, placebo-controlled, multicenter comparison of loteprednol etabonate ophthalmic suspension, 0.5%, and placebo for treatment of keratoconjunctivitis sicca in patients with delayed tear clearance. Am J Ophthalmol. 2004;138(3):444–457. doi:10.1016/j.ajo.2004.04.052
115. Villani E, Garoli E, Termine V, Pichi F, Ratiglia R, Nucci P. Corneal confocal microscopy in dry eye treated with corticosteroids. Optom Vis Sci. 2015;92(9):e290–295. doi:10.1097/OPX.0000000000000600
116. Beckman K, Katz J, Majmudar P, Rostov A. Loteprednol etabonate for the treatment of dry eye disease. J Ocul Pharmacol Ther. 2020;36(7):497–511. doi:10.1089/jop.2020.0014
117. Pinto-Fraga J, López-Miguel A, González-García MJ, et al. Topical fluorometholone protects the ocular surface of dry eye patients from desiccating stress: a randomized controlled clinical trial. Ophthalmology. 2016;123(1):141–153. doi:10.1016/j.ophtha.2015.09.029
118. Bucolo C, Fidilio A, Fresta CG, et al. Ocular pharmacological profile of hydrocortisone in dry eye disease. Front Pharmacol. 2019;10:1240. doi:10.3389/fphar.2019.01240
119. Kallab M, Szegedi S, Hommer N, et al. Topical low dose preservative-free hydrocortisone reduces signs and symptoms in patients with chronic dry eye: a randomized clinical trial. Adv Ther. 2020;37(1):329–341. doi:10.1007/s12325-019-01137-8
120. Chen M, Gong L, Sun X, et al. A comparison of cyclosporine 0.05% ophthalmic emulsion versus vehicle in Chinese patients with moderate to severe dry eye disease: an eight-week, multicenter, randomized, double-blind, parallel-group trial. J Ocul Pharmacol Ther. 2010;26(4):361–366. doi:10.1089/jop.2009.0145
121. Baiza-Durán L, Medrano-Palafox J, Hernández-Quintela E, et al. A comparative clinical trial of the efficacy of two different aqueous solutions of cyclosporine for the treatment of moderate-to-severe dry eye syndrome. Br J Ophthalmol. 2010;94(10):1312–1315. doi:10.1136/bjo.2008.150011
122. Sacchetti M, Mantelli F, Lambiase A, Mastropasqua A, Merlo D, Bonini S. Systematic review of randomised clinical trials on topical ciclosporin A for the treatment of dry eye disease. Br J Ophthalmol. 2014;98(8):1016–1022. doi:10.1136/bjophthalmol-2013-304072
123. Wan KH, Chen LJ, Young AL. Efficacy and safety of topical 0.05% cyclosporine eye drops in the treatment of dry eye syndrome: a systematic review and meta-analysis. Ocul Surf. 2015;13(3):213–225. doi:10.1016/j.jtos.2014.12.006
124. Holland EJ, Donnenfeld ED, Lindstrom RL, Pflugfelder SC, Sheppard JD, Solomon KD. Expert consensus in the treatment of dry eye inflammation. Based on the proceedings of a symposium held during the 2006 American Academy of Ophthalmology joint meeting. Ophthalmol Times. 2007;32(Supplement 7):1.
125. Abud TB, Amparo F, Saboo US, et al. A clinical trial comparing the safety and efficacy of topical tacrolimus versus methylprednisolone in ocular graft-versus-host disease. Ophthalmology. 2016;123(7):1449–1457. doi:10.1016/j.ophtha.2016.02.044
126. Miyazaki D, Fukushima A, Ohashi Y, et al. Steroid-sparing effect of 0.1% tacrolimus eye drop for treatment of shield ulcer and corneal epitheliopathy in refractory allergic ocular diseases. Ophthalmology. 2017;124(3):287–294. doi:10.1016/j.ophtha.2016.11.002
127. Heikal MA, Soliman TT, Abousaif WS, Shebl AA. A comparative study between ciclosporine A eye drop (2%) and tacrolimus eye ointment (0.03%) in management of children with refractory vernal keratoconjunctivitis. Graefes Arch Clin Exp Ophthalmol. 2022;260(1):353–361. doi:10.1007/s00417-021-05356-0
128. Moawad P, Shamma R, Hassanein D, Ragab G, El Zawahry O. Evaluation of the effect of topical tacrolimus 0.03% versus cyclosporine 0.05% in the treatment of dry eye secondary to Sjogren syndrome. Eur J Ophthalmol. 2022;32(1):673–679. doi:10.1177/1120672121992680
129. Holland EJ, Luchs J, Karpecki PM, et al. Lifitegrast for the treatment of dry eye disease: results of a Phase III, randomized, double-masked, placebo-controlled trial (OPUS-3). Ophthalmology. 2017;124(1):53–60. doi:10.1016/j.ophtha.2016.09.025
130. Sheppard JD, Torkildsen GL, Lonsdale JD, et al. Lifitegrast ophthalmic solution 5.0% for treatment of dry eye disease: results of the OPUS-1 Phase 3 study. Ophthalmology. 2014;121(2):475–483. doi:10.1016/j.ophtha.2013.09.015
131. Tauber J, Karpecki P, Latkany R, et al. Lifitegrast ophthalmic solution 5.0% versus placebo for treatment of dry eye disease: results of the randomized Phase III OPUS-2 study. Ophthalmology. 2015;122(12):2423–2431. doi:10.1016/j.ophtha.2015.08.001
132. Giannaccare G, Versura P, Buzzi M, Primavera L, Pellegrini M, Campos EC. Blood derived eye drops for the treatment of cornea and ocular surface diseases. Transfus Apher Sci. 2017;56(4):595–604. doi:10.1016/j.transci.2017.07.023
133. Christen WG, Cook NR, Manson JE, et al. Efficacy of marine ω-3 fatty acid supplementation vs placebo in reducing incidence of dry eye disease in healthy US adults: a randomized clinical trial. JAMA Ophthalmol. 2022;140(7):707–714. doi:10.1001/jamaophthalmol.2022.1818
134. Best AL, Labetoulle M, Legrand M, M’Garrech M, Barreau E, Rousseau A. [Punctal and canalicular plugs: indications, efficacy and safety (French translation of the article)] Les bouchons lacrymaux: indications, efficacité et tolérance. J Fr Ophtalmol. 2019;42(4):404–414. doi:10.1016/j.jfo.2018.10.003
135. Sharma N, Sah R, Priyadarshini K, Titiyal JS. Contact lenses for the treatment of ocular surface diseases. Indian J Ophthalmol. 2023;71(4):1135–1141. doi:10.4103/IJO.IJO_17_23
136. Vazirani J, Sridhar U, Gokhale N, Doddigarla VR, Sharma S, Basu S. Autologous serum eye drops in dry eye disease: preferred practice pattern guidelines. Indian J Ophthalmol. 2023;71(4):1357–1363. doi:10.4103/IJO.IJO_2756_22
137. Pan Q, Angelina A, Marrone M, Stark WJ, Akpek EK. Autologous serum eye drops for dry eye. Cochrane Database Syst Rev. 2017;2(2):Cd009327. doi:10.1002/14651858.CD009327.pub3
138. Beining MW, Magnø MS, Moschowits E, et al. In-office thermal systems for the treatment of dry eye disease. Surv Ophthalmol. 2022;67(5):1405–1418. doi:10.1016/j.survophthal.2022.02.007
139. Arita R, Fukuoka S. Non-pharmaceutical treatment options for meibomian gland dysfunction. Clin Exp Optom. 2020;103(6):742–755. doi:10.1111/cxo.13035
140. Leng X, Shi M, Liu X, Cui J, Sun H, Lu X. Intense pulsed light for meibomian gland dysfunction: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2021;259(1):1–10. doi:10.1007/s00417-020-04834-1
141. Maskin SL. Intraductal meibomian gland probing relieves symptoms of obstructive meibomian gland dysfunction. Cornea. 2010;29(10):1145–1152. doi:10.1097/ICO.0b013e3181d836f3
142. Geerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2011;52(4):2050–2064. doi:10.1167/iovs.10-6997g
143. Garcia-Zalisnak D, Nash D, Yeu E. Ocular surface diseases and corneal refractive surgery. Curr Opin Ophthalmol. 2014;25(4):264–269. doi:10.1097/ICU.0000000000000077
144. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C. Dry eye disease after refractive surgery: comparative outcomes of small incision lenticule extraction versus LASIK. Ophthalmology. 2015;122(4):669–676. doi:10.1016/j.ophtha.2014.10.004
145. Ambrósio R Jr, Tervo T, Wilson SE. LASIK-associated dry eye and neurotrophic epitheliopathy: pathophysiology and strategies for prevention and treatment. J Refract Surg. 2008;24(4):396–407.
146. Trattler WB, Majmudar PA, Donnenfeld ED, McDonald MB, Stonecipher KG, Goldberg DF. The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017;11:1423–1430. doi:10.2147/OPTH.S120159
147. Rochet E, Levron A, Agard E, et al. Should artificial tears be used during the preoperative assessment of toric IOLs before age-related cataract surgery? The TORIDE study. J Refract Surg. 2021;37(11):759–766. doi:10.3928/1081597X-20210826-01
148. Labetoulle M, Rousseau A, Baudouin C. Management of dry eye disease to optimize cataract surgery outcomes: two tables for a daily clinical practice. J Fr Ophtalmol. 2019;42(8):907–912. doi:10.1016/j.jfo.2019.03.032
149. ASCRS Preoperative OSD Algorithm. American society of cataract and refractive surgery; 2022. Available from: https://ascrs.org/clinical-education/cornea/ascrs-preoperative-osd-algorithm.
150. Blazey P, Crossley KM, Ardern CL, van Middelkoop M, Scott A, Khan KM. It is time for consensus on ‘consensus statements’. Br J Sports Med. 2022;56(6):306–307. doi:10.1136/bjsports-2021-104578
151. Beighton D. Consensus statements. Caries Res. 2017;51(5):1–2. doi:10.1159/000480305
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.