")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Dynamics and Efficacy: A Comprehensive Evaluation of the Advanced Dengue Fever Surveillance and Early Warning System in Ningbo City, 2023
Authors Zhang Y, Abudunaibi B, Zhao Y, Zhang D, Chu Y, Lei S, Gu X, Lao X, Wu X, Yao W, Chen Y, Tong F
Received 27 March 2024
Accepted for publication 1 August 2024
Published 9 August 2024 Volume 2024:17 Pages 1947—1955
DOI https://doi.org/10.2147/RMHP.S470237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kyriakos Souliotis
Yanwu Zhang,1,* Buasiyamu Abudunaibi,2,* Yunkang Zhao,2 Dongliang Zhang,1 Yanru Chu,1 Song Lei,1 Xiaomin Gu,1 Xuying Lao,1 Xianhao Wu,1 Weitao Yao,1 Yi Chen,1 Feng Tong1
1Department of Infectious Disease Control and Prevention, Ningbo Prefectural Center for Disease Control and Prevention, Ningbo, Zhejiang Province, People’s Republic of China; 2State Key Laboratory of Vaccines for Infectious Diseases, Xiang’ an Biomedicine Laboratory, School of Public Health, Xiamen University, Xiamen, Fujian Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng Tong; Yi Chen, Ningbo Prefectural Center for Disease Control and Prevention, Ningbo, Zhejiang Province, People’s Republic of China, Email [email protected]; [email protected]
Objective: To conduct a comprehensive evaluation of the Dengue Fever Surveillance and Early Warning System deployed in Ningbo City during 2023, focusing on its capacity for timely identification and reporting of dengue fever cases, particularly imported cases from endemic regions.
Methods: A detailed data of patient clinical features and blood profile trends was collected from clinical records and surveillance reports, focusing on the rapid diagnostic processes and surveillance rigor. This study assessed the effectiveness of the system in identifying and reporting dengue cases and identified the limitations of the existing framework through a basic statistical approach.
Results: The system demonstrated timely identification and reporting of dengue fever cases, with a particular emphasis on imported cases. However, several limitations were identified, including the need for more precise monitoring criteria and improved coordination with medical entities.
Conclusion: The study underscores the critical role of public health bodies in managing disease outbreaks and advocates for enhanced methodologies to refine epidemic control efforts. The findings contribute to the advancement of early warning mechanisms and the improvement of proactive infectious disease monitoring in metropolitan environments, providing valuable insights for fortifying the Dengue Fever Surveillance and Early Warning System in Ningbo City.
Keywords: Dengue fever, Imported, Surveillance, Early-warning
Introduction
Dengue fever (DF) is categorized as a Class B infectious disease under China’s “Law on the Prevention and Treatment of Infectious Diseases”. It is an acute vector-borne infectious disease caused by the dengue virus (DENV) and transmitted through the bite of Aedes mosquitoes.1 To date, four serotypes of dengue virus have been identified, ranging from DENV-1 to DENV-4. Infection can result in a variety of clinical symptoms, from the most common dengue fever to dengue haemorrhagic fever (DHF) and dengue shock syndrome, which are classified as severe dengue. DHF is characterized by bleeding, blood plasma leakage, and low platelet count, while DSS is marked by dangerously low blood pressure. Other commonly noted symptoms as headaches, rash pain in joint and muscle, nausea and vomiting.2 Primary infection with one serotype of DENV usually results in a mild illness with lifelong immunity to that serotype but only partial and temporary cross-immunity to other serotypes. Secondary infection with a different serotype can lead to more severe disease due to antibody-dependent enhancement (ADE).
In 2019, dengue fever was listed by the World Health Organization as one of the top ten global health threats, exerting a substantial socioeconomic and disease burden,3 particularly in tropical and subtropical regions.4,5 Since China’s first reported outbreak of dengue fever in 1978,6 there has been a continuous increase in both the number of reported cases of dengue fever in regions.7 Notably, the southern and coastal regions of China have experienced large-scale dengue fever outbreaks and frequent local epidemics,2 with the upward trend in disease burden becoming increasingly apparent.8
The peak years of dengue fever epidemics in China were 2014 and 2019, characterized by a high number of reported cases and extensive impact.9,10 Imported cases of dengue fever remain the primary cause of outbreaks within the country.2,11 Due to the control policies for the COVID-19 pandemic, the number of reported dengue fever cases from 2020 to 2022 was significantly lower than in 2019. However, as COVID-19 control measures are adjusted and cross-border travel increases, the prevention and control of dengue fever are facing more severe challenges.
Currently, China does not have endemic areas for dengue fever,1 but due to the widespread and expanding distribution of the Aedes mosquito vector, local transmission of dengue fever is highly likely in the event of imported cases, especially if not promptly identified and managed, thus complicating the control efforts. Therefore, establishing an efficient surveillance information system for the early detection and diagnosis of imported dengue cases is of positive significance for epidemic prevention and control. The key to the recognition and diagnosis of dengue fever lies with healthcare institutions and professionals. Enhancing the diagnostic capabilities of relevant medical personnel aids in case detection.12 However, studies show that the awareness rate of dengue-related knowledge among medical personnel is below 60%, and only 65.2% inquire about the travel history of patients with fever,13,14 leading to the potential misdiagnosis or underdiagnosis of dengue fever patients. To minimize the uncertainties of subjective judgment by medical staff and to leverage the proactive case finding and support role of disease control institutions, the use of information technology and medical big data to improve the sensitivity of dengue fever surveillance has become a focal point in research for disease prevention and control.
In 2022, the Center for Disease Control and Prevention in Ningbo established and implemented an early warning system for dengue fever.15 This study examines the epidemiological characteristics of dengue fever cases in Ningbo for the year 2023, discussing the practical role of the early warning system in the prevention and control of dengue fever outbreaks and providing a basis for the system’s optimization and the adjustment of dengue fever control strategies.
Methods
Study Design
Initially, this study provides a descriptive analysis of the epidemiological status and clinical characteristics of the dengue fever cases in Ningbo in 2023. Then it compares the promptness of the dengue fever Infectious Disease Report Card surveillance with that of the Ningbo’s novel early warning system for dengue fever within the same year.
Data Collection
All data used in this study were obtained from the Chinese Center for Disease Control and Prevention (CDC) information system, ensuring compliance with relevant data protection and privacy regulations. The dataset includes dengue fever infectious disease report cards for Ningbo, starting from January 1, 2023. It encompassed both clinically diagnosed cases and those confirmed by laboratory tests. Additionally, epidemiological investigation reports and laboratory test results for all reported cases were also collected from the system.
Additionally, information on suspected dengue fever cases identified from January 1, 2023 was gathered from Ningbo’s early warning system for dengue fever. This encompassed medical records, clinical symptoms, laboratory tests, and diagnoses. The system’s criteria for suspected cases included patients presenting with fever accompanied by a decrease in platelets or white blood cells.
Information on patients’ travel dates was collected to identify potential exposure periods and link them to the incubation period of dengue fever; the onset date of symptoms was collected to determine the timeline of infection; the date of diagnosis by both doctors and the system were collected to ensure accurate tracking of case progression and response times.
Statistical Analysis
Data entry and organization related to this study was performed in Excel 2019. Epidemiological Reports for dengue infections are collated in Word 2019. Continuous quantitative variables were described by median (M) ± interquartile range (IQR), and categorical qualitative variables by frequencies and percentages (%). Statistical analysis was performed by SPSS version 21.0, and differences were statistically significant at p ≤ 0.05. Graphs were plotted using OrignPro version 2022; Map is plotted using ArcMap version 10.8.
Results
Epidemiological Characteristics
In 2023, Ningbo witnessed 57 dengue fever cases, with 55 confirmed and 2 clinically diagnosed (Table 1). All were non-native: 49 domestically acquired—predominantly from Xishuangbanna, Yunnan (44 cases), Fuzhou, Fujian (4 cases) and Guangdong (1 case)—and 8 internationally, with Thailand, Myanmar, Singapore, Cambodia and Maldives as the sources. The detection mechanisms were multifaceted: 44 cases through proactive medical consultations, 9 via traveler screenings, and 4 through the city’s early warning system. Importantly, no local transmissions followed these imported incidents.
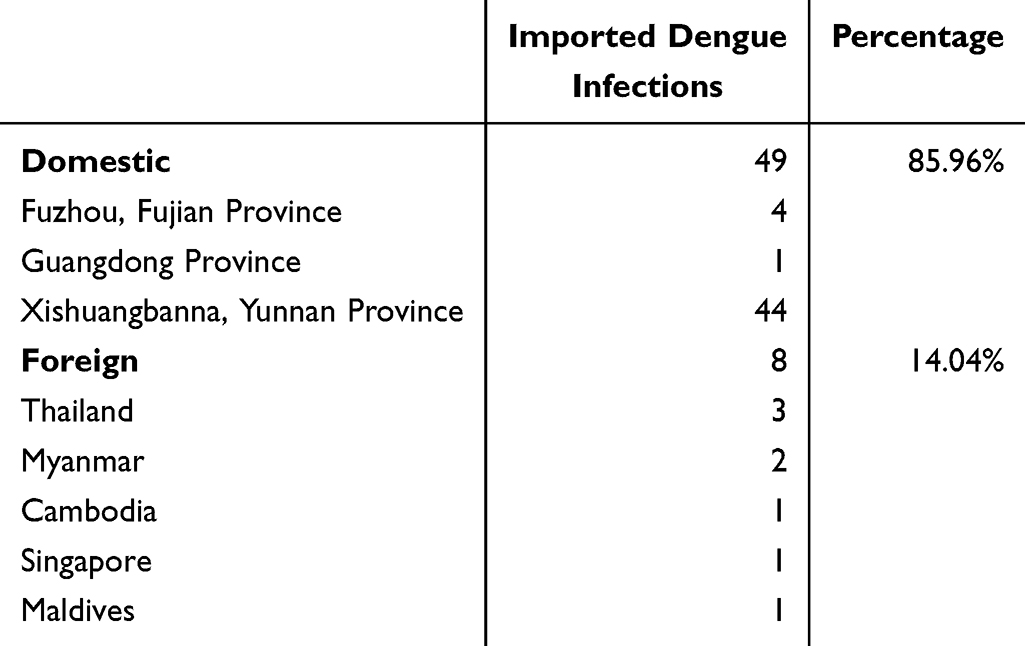 |
Table 1 Imported Sources of Dengue Fever Cases in Ningbo in 2023 |
The onset of dengue fever in Ningbo was documented on August 3, 2023. An analysis of the incidence pattern revealed a pronounced peak in the months of August and September, registering 21 and 25 cases respectively, before a decline to 10 cases by October and 1 case in November, delineating this period as the critical phase of the outbreak (Figure 1A). The spatial distribution of cases was extensive, encompassing nine of the ten counties and districts within Ningbo, with Ninghai being the sole exception (Figure 1B). The highest concentration of cases was reported in Yinzhou with 22 occurrences, indicating a localized intensity of transmission.
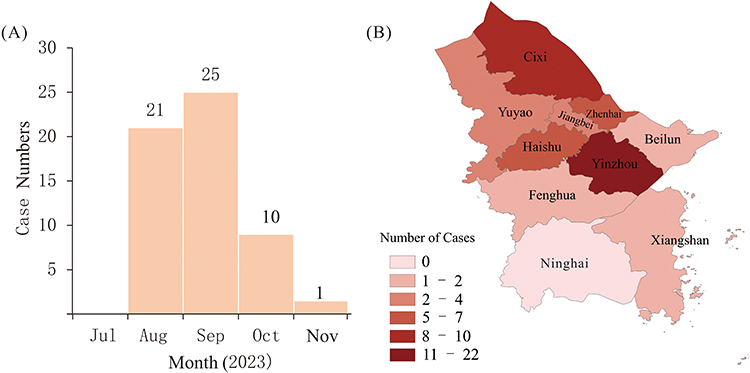 |
Figure 1 The Temporal and Regional Distribution for Dengue Infections in Ningbo, 2023. Notes: (A) is the temporal distribution on the dengue cases in the study, the horizontal axis is the months when the cases were detected, before August, there were no cases, while the last dengue fever case in Ningbo City was detected on November 22nd, the cases detected after that were not depicted. (B) is the regional distribution on the cases, we use shades of color to differentiate the number of cases in different areas. |
The healthcare infrastructure’s response was reflected in the detection of cases across various levels: 18 at primary healthcare facilities, 15 at county-level, and 24 at city-level medical institutions. Demographically (Table 2), altogether, for both domestic and foreign imported cases, the outbreak affected 57 individuals, comprising 20 males and 37 females, exhibiting a female-to-male ratio of approximately 2:1. The patients ranged from 7 to 78 years of age, with a median age of 37, and the most affected age group being 20–49 years, accounting for 64.91% of cases. Employment data revealed houseworkers and the unemployed (31.58%) and industrial workers (19.30%) as the predominant occupational groups impacted, followed by business service personnel (14.04%). Other affected occupational categories included teachers, retirees, office workers, students, farmers, individual business owners, and catering service personnel, each constituting a smaller fraction of the total cases.
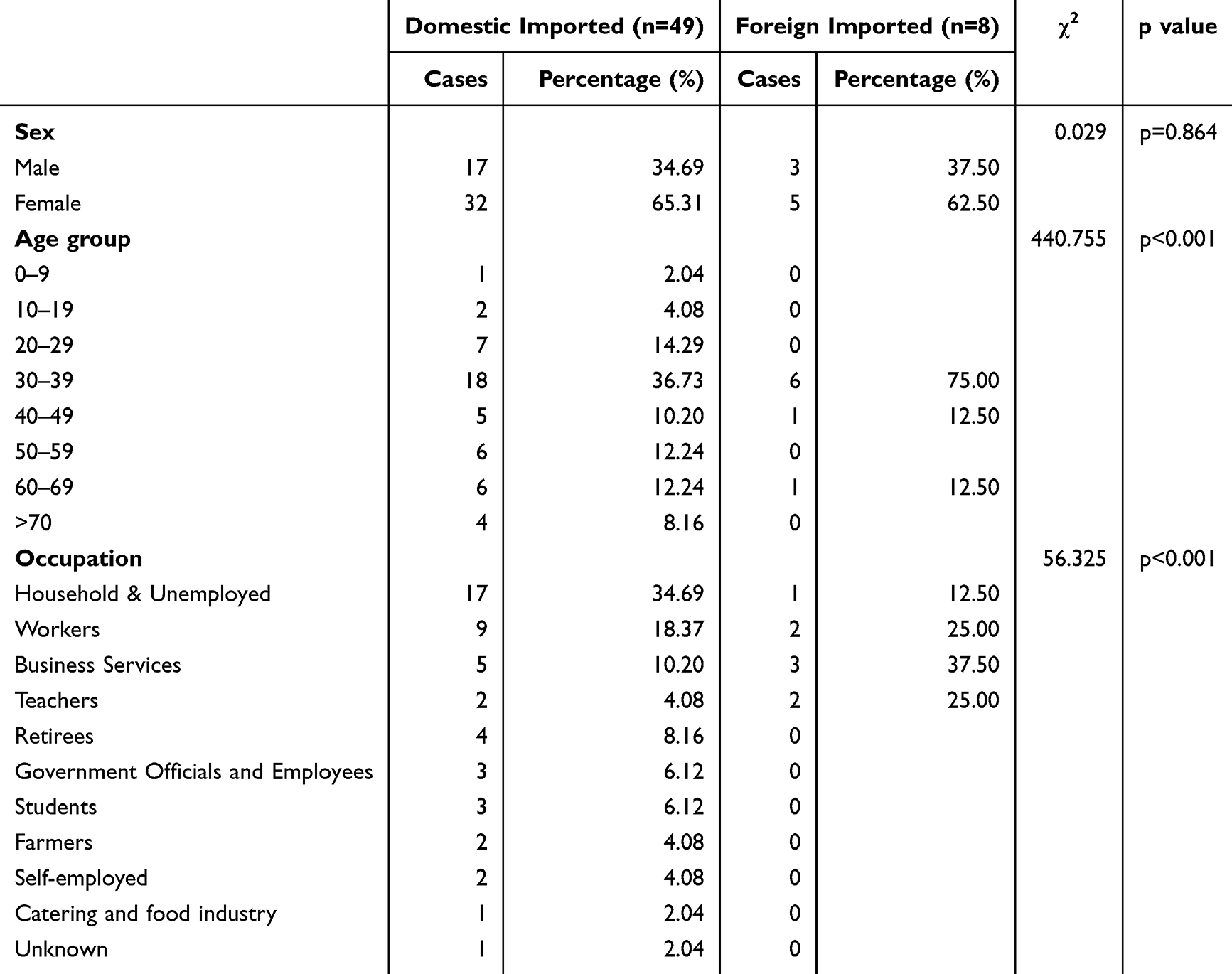 |
Table 2 Demographic Characteristics of Dengue Fever Cases in Ningbo, 2023 |
Clinical Characteristics
In the 44 patients diagnosed with dengue fever through proactive medical consultation, fever emerged as the most common initial symptom, manifesting in 97.73% (43/44) of instances. Only a solitary case presented with headache as the initial complaint. Hematological abnormalities were prevalent, with a leukopenia detected in 26 patients (59.09%). Concurrent leukopenia and thrombocytopenia were observed in 11 patient (25.00%), while isolated thrombocytopenia was evident in 4 patients (9.09%). Interestingly, one patient exhibited thrombocytosis, and two maintained normal leukocyte and platelet counts.
Within the subset of nine cases identified via the screening of travel companions, four were asymptomatic, carrying the virus without clinical manifestations, whereas the other five developed febrile symptoms. Blood test analysis revealed leukopenia in four of these patients and thrombocytopenia in one. The dengue fever early warning system successfully flagged three instances of fever with leukopenia and one instance of both leukopenia and thrombocytopenia.
Analyzing the complete set of 53 symptomatic cases, fever was a universal symptom. Of these, 33 patients experienced fever alongside leukopenia, 5 with isolated thrombocytopenia, 12 with both leukopenia and thrombocytopenia, 2 with normal leukocyte and platelet levels, and one unique case of fever with thrombocytosis.
Among the 44 individuals who actively sought medical care for dengue fever, a significant majority of 90.91% (40/44) received a diagnosis during their initial medical consultation. The median duration from the first symptom manifestation to presenting at a healthcare facility was a mere 1 day (IQR= 2). Impressively, the timeline from initial medical consultation to an established diagnosis by a doctor (Median=0, IQR=1) or the system (Median=0, IQR=0)was typically instantaneous. Furthermore, the median time span from the onset of symptoms to the confirmation of dengue fever by a doctor was 3 days (IQR=4), while the system basically captures the cases earlier (Median=2, IQR=3), which underscores the efficiency of the diagnostic process. It is noteworthy that due to the diversity of travelling modes and limitations of the study, the time of entry into Ningbo was determine. The median time from arrival to symptom onset for these cases was 4 days (IQR=3), with the longest being 10 days, so it is believed that both new systems and doctors were able to diagnose and screen for cases within the longest incubation period.
Of the 57 patients confirmed with dengue infection, serotyping was performed on 42 subjects. The analysis revealed that Dengue serotype I (DENV-1) was predominant, with 38 instances traced back to importations from Yunnan, Fujian, Thailand, Myanmar, and Singapore. Meanwhile, Dengue serotype II (DENV-2) was identified in 4 cases, with these infections originating from Yunnan, Thailand, and Cambodia.
Comparison of Dengue Fever Surveillance on the Early Warning System and Infectious Disease Report Card
The early warning system for dengue fever in Ningbo City is currently capable of issuing alerts on a “T+1” basis, with the workflow depicted in Figure 2. In 2023, the system successfully detected four cases of dengue fever in the city. Remarkably, three of these cases eluded clinical diagnosis and were only identified following screening prompted by alerts from the early warning system. In one particular case, a patient returning from Yunnan was not clinically diagnosed as having dengue fever until the disease control department intervened, despite seeking medical care for fever and leukopenia. Subsequent contact tracing investigations revealed that non-disclosure of travel history by patients and a lack of diagnostic acumen among primary healthcare workers were the main causes of the initial oversight and misdiagnosis.
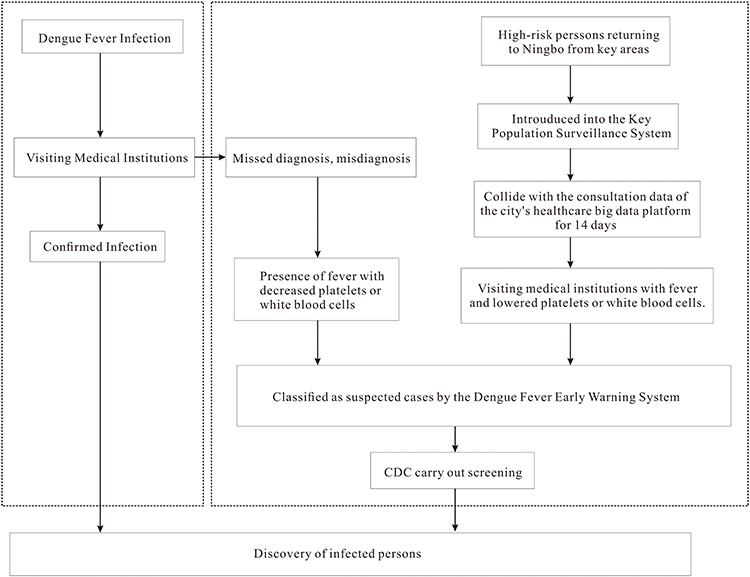 |
Figure 2 The flow chart of dengue fever prevention and control in Ningbo. |
Upon comparison with the data from the conventional infectious disease report cards for 2023, as presented in Figure 3, the newly introduced surveillance system has shown enhanced capabilities for early detection. While in most cases (n=33), there were no differences in reporting time between the novel surveillance system and the traditional system, only four of the remaining cases were lagging (3 of them lagged for 1 days, and only 1 lagged for 4 days), the rest were all leading (leading days: 1–3). These findings clearly suggest that the new system offers greater promptness in detecting cases of infectious diseases.
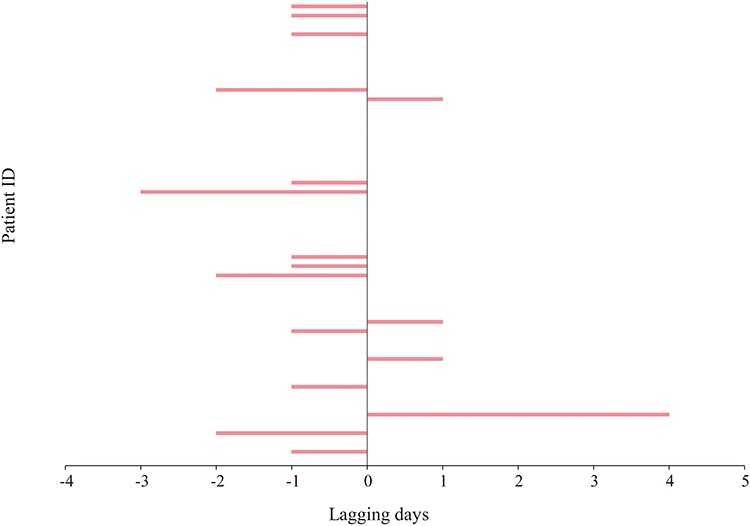 |
Figure 3 Reporting times of Dengue infections for the new system lagging those for traditional surveillance. Notes: The horizontal axis is the lagging days of dengue infections reported by the new system to the traditional surveillance systems, the numbers on the axis represents the lagging days, for example, lagging −1 day means the dengue infections reported by the new system led the traditional surveillance systems by 1 day, while 1day means the dengue infections reported by the new system lagged the traditional surveillance systems by 1 day. The vertical axis represents the Patient ID of the dengue infections in the study. When there were no leading or lagging days for the reporting times for the new system and traditional surveillance, there will be no lagging lines in the figure. |
Discussion
The investigation into the 2023 dengue fever infections in Ningbo City indicates that all recorded cases were domestically imported, with the majority originating from the Xishuangbanna of Yunnan. This contrasts with historical data, which shows that the importation of dengue fever into Zhejiang Province and Ningbo City had primarily been from foreign countries, especially Southeast Asian countries, and regions.16–18 The recent trend reflects a notable change in the epidemiology of dengue importation to Ningbo City, shifting from international to domestic sources. This alteration could be linked to the increased domestic travel following the easing of COVID-19 restrictions. According to statistics from the China Tourism Academy and the Yunnan Provincial Department of Culture and Tourism, domestic travel saw a significant upsurge, with tourism reaching 1.839 billion from June to August 2023.19 Notably, Xishuangbanna alone attracted over 38 million visitors in the first half of 2023,20 while international travel from mainland China was recorded at 40.37 million trips.21 These insights suggest that dengue fever prevention and control strategies need to be dynamically tailored to reflect changes in regional human movement patterns.
The temporal distribution of dengue fever cases in Ningbo City, as depicted by the epidemic curve, indicates that August and September are the months with the highest incidence rates. This pattern is consistent with the peak dengue periods observed in other regions such as Xishuangbanna in Yunnan and Fuzhou in Fujian,22,23 underscoring the seasonality of dengue outbreaks. The convergence of these months with the height of summer travel and the beginning of the academic year results in heightened population flux. Moreover, the warm and humid conditions prevalent in the summer months create ideal breeding environments for Aedes mosquitoes, the primary vectors of dengue fever. Surveillance data confirms that the population density of adult and larval stages of Aedes mosquitos surges to its zenith during this period.24 In the presence of a considerable number of hosts and an abundance of mosquitoes, even a single imported case can potentially spark a local epidemic. Historical data corroborate that cities like Ningbo, Hangzhou, and Zhoushan have encountered indigenous dengue outbreaks in these critical months.18,25 Consequently, the period demands intensified dengue control efforts. Building on the proactive identification and management of imported cases, it is crucial to implement community health campaigns aimed at the elimination of mosquito breeding sites to thwart endemic transmissions.
The analysis of case detection methods shows that a significant majority (77.19%) of dengue fever cases were detected through proactive patient-seeking healthcare services, with initial diagnoses capturing 90% of these instances. This high detection rate implies a commendable level of diagnostic acumen within the medical facilities of Ningbo. Despite the city not being a known hotspot for endemic dengue fever, the occurrence of imported cases and sporadic local outbreaks suggests that its healthcare professionals are reasonably aware of the disease. Nonetheless, there is an absence of comprehensive data regarding the depth of knowledge that healthcare workers in Ningbo possess about dengue prevention and control measures. A survey conducted in Zhoushan City in 2018 revealed that 65.28% of healthcare personnel had an accurate understanding of dengue prevention and control knowledge, with less than half regularly asking fever patients about their travel history—a significant gap that could affect disease management.26 In response, at the start of 2023, Ningbo made dengue prevention and control a priority. The city has since taken steps to enhance the detection efficiency of its medical system and the preparedness of healthcare workers by introducing intelligent systems for epidemiological history assessment in diagnostic processes, automated travel history alerts in self-service kiosks, and prominent educational signage. It has also improved diagnostic speed with the rollout of rapid dengue testing services and bolstered healthcare worker knowledge through targeted dengue-related educational programs.
Ningbo Center for Disease Control and Prevention, through health monitoring of individuals who had been in contact with confirmed cases, identified nine infected individuals, four of whom were asymptomatic carriers. The presence of asymptomatic infections, which can still transmit the virus despite a lack of symptoms, poses a substantial challenge for disease detection and holds considerable epidemiological significance. Research indicates that asymptomatic individuals represent a staggering 75% of dengue infections.24 Enhanced health surveillance and diligent dengue screenings, especially for travelers who have been in contact with infected individuals, are imperative for revealing these covert infections. The absence of detected infections among non-traveling contacts in this study likely stems from prompt case identification and diagnosis, which preempted the extrinsic incubation period necessary for vectorial capacity development in Aedes mosquitoes. These insights accentuate the necessity of expedited diagnostics and stringent monitoring of potentially exposed individuals to mitigate the risk of secondary dengue transmission.
By examining the clinical presentations of dengue fever, this study revealed distinct hematological patterns: 62.26% of patients displayed a reduction solely in white blood cell (WBC) count, 9.43% had an isolated drop in platelet count, and 22.64% experienced decreases in both WBCs and platelets. These findings align with prior research.27 The data suggests that incorporating these specific hematological markers into the dengue fever monitoring and early warning systems could enable the identification of approximately 95% of cases, as the majority present with fever and these blood count anomalies. Nonetheless, a minority of cases with atypical hematological profiles may evade detection, highlighting an area for potential enhancement of current diagnostic protocols.
Throughout 2023, dengue prevention and control initiatives have seen the surveillance and early warning system effectively execute case alerts and management, thereby cementing the pivotal role of public health agencies in dengue epidemic oversight and reinforcing collaboration with healthcare providers. However, the system currently faces challenges, notably the necessity to refine symptom monitoring criteria. Differential diagnosis is hindered by symptomatic overlaps with other diseases, leading to an overabundance of suspected cases and thereby burdening public health authorities with increased investigative demands. The integration between the monitoring system and medical institutions’ automated dengue alert mechanisms remains incomplete, causing duplicative epidemiological investigations. Moreover, there is a notable information gap regarding individuals returning to Ningbo from dengue-prevalent regions, and a lack of data for those traveling through areas not designated as key, thereby limiting the system’s efficiency in proactive monitoring and early warning capacities.
Limitation
While this evaluation sheds light on the strengths of the Dengue Fever Surveillance and Early Warning System in Ningbo City, certain limitations should be acknowledged. The study primarily focuses on data from 2023, and the long-term sustainability and adaptability of the system over subsequent years remain uncertain. Additionally, the research highlights challenges in symptom monitoring criteria and the integration of alert mechanisms, indicating areas that require further refinement for optimal system performance. What’s more, details of methodology of screening of travelers, dengue detection in health care settings, active and passive case detections, and vector surveillance in the areas of residence of cases should also be discussed further to make outstand the efficiency of the new system.
Conclusion
In conclusion, the evaluation of the novel Dengue Fever Surveillance and Early Warning System in Ningbo City, 2023 underscores the system’s significant contributions to early detection and management of dengue fever outbreaks. The study emphasizes the importance of expedited diagnostics, robust monitoring, and collaboration between public health agencies and healthcare providers in combating infectious diseases. While facing challenges in symptom monitoring and data integration, the system demonstrates promising capabilities in alerting and managing dengue cases promptly. Moving forward, optimizing the system’s performance, addressing limitations, and refining strategies based on research findings will be essential for strengthening disease control measures and safeguarding public health in urban environments like Ningbo City.
Abbreviations
COVID-19, Coronavirus disease 2019; DF, Dengue fever; DENV, dengue virus; DENV-1, dengue fever serotype 1; DENV-2, dengue fever serotype 2.
Funding
Ningbo Top Medical and Health Research Program (No.2023020713); Ningbo Key Laboratory of Virus Research (20221CXJD030031).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhang FC, He JF, Peng J, et al. Guidelines for diagnosis and treatment of dengue in China. Zhonghua Nei Ke Za Zhi. 2018;57(9):642–648. doi:10.3760/cma.j.issn.0578-1426.2018.09.005
2. Wu T, Wu Z, Li YP. Dengue fever and dengue virus in the People’s Republic of China. Rev Med Virol. 2022;32(1):e2245. doi:10.1002/rmv.2245
3. World Health Organization. Ten threats to global health in 2019. Available from: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
4. Wilder-Smith A, Ooi EE, Horstick O, Wills B. Dengue. Lancet. 2019;393(10169):350–363. doi:10.1016/S0140-6736(18)32560-1
5. Kong L, Xu C, Mu P, Li J, Qiu S, Wu H. Risk factors spatial-temporal detection for dengue fever in Guangzhou. Epidemiol Infect. 2018;147:e32. doi:10.1017/S0950268818002820
6. Wu JY, Lun ZR, James AA, Chen XG. Dengue Fever in mainland China. Am J Trop Med Hyg. 2010;83(3):664–671. doi:10.4269/ajtmh.2010.09-0755
7. Xiong Y, Chen Q. [Epidemiology of dengue fever in China since 1978]. Nan Fang Yi Ke Da Xue Xue Bao. 2014;34(12):1822–1825.
8. Alel XMLXSX. Assessment research on the disease burden of dengue fever in China from 2010 to 2019 based on disability-adjusted life years. Chin J Vector Biol & Control. 2020;31(5).
9. Guo YH, Lai SJ, Liu XB, Li GC, Yu HJ, Liu QY. Governmental supervision and rapid detection on dengue vectors: an important role for dengue control in China. Acta Trop. 2016;156:17–21. doi:10.1016/j.actatropica.2015.12.011
10. Wang F, Zhu Y, Zhang H, et al. Spatial and temporal analyses of the influences of meteorological and environmental factors on Aedes albopictus (Diptera: Culicidae) population dynamics during the peak abundance period at a city scale. Acta Trop. 2023;245(106964):106964. doi:10.1016/j.actatropica.2023.106964
11. Zhao Z, Li Y, Mou D, et al. [Spatial-temporal analysis on imported dengue fever in six provinces of China, 2016-2018]. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(11):1808–1812. doi:10.3760/cma.j.cn112338-20191231-00923
12. Zhang DL, Wang R, Yi B, et al. Investigation of an outbreak of dengue fever. Preventive Med. 2019;31(8):4.
13. Lun X, Yang R, Lin L, et al. Effects of the source of information and knowledge of dengue fever on the mosquito control behavior of residents of border areas of Yunnan, China. Parasit Vectors. 2023;16(1):311. doi:10.1186/s13071-023-05916-9
14. Lin JF, Li FD, Liu SL, X JP. Analysis of the epidemiological characteristics of imported dengue fever in Zhejiang Province, 2005-2013. Prevent Medi Zhejiang. 2014;26(12):3.
15. Zhang L, Chen Y, Fu GL, et al. Design and application of early warning system for Dengue fever based on big data. China Digital Medicine. 2022;17(10):115–120.
16. Zhang Y, Wang L, Wang G, Xu J, Zhang T. An ecological assessment of the potential pandemic threat of Dengue Virus in Zhejiang province of China. BMC Infect Dis. 2023;23(1):473. doi:10.1186/s12879-023-08444-0
17. Han A, Sun B, Sun Z, et al. Molecular Characterization and Phylogenetic Analysis of the 2019 Dengue Outbreak in Wenzhou, China. Front Cell Infect Microbiol. 2022;12:829380. doi:10.3389/fcimb.2022.829380
18. Yao W, Yang Z, Lou X, Mao H, Yan H, Zhang Y. Molecular Characterization of Dengue Virus Type 1 in Zhejiang in 2019. Front Cell Infect Microbiol. 2021;11(673299). doi:10.3389/fcimb.2021.673299
19. Summer Travel Market Monitor Report. Available from: https://www.mct.gov.cn/whzx/zsdw/zglyyjy/202309/t20230904_947007.html.
20. Press conference of the Information Office of the People’s Government of Yunnan Province. Available from: https://mp.weixin.qq.com/s/hrNGua0iMnBKi09hFGsh-g.
21. Big data on travelling abroad in the first half of the year https://www.mct.gov.cn/whzx/zsdw/zglyyjy/202308/t20230801_946301.html.
22. Lun X, Wang Y, Zhao C, et al. Epidemiological characteristics and temporal-spatial analysis of overseas imported dengue fever cases in outbreak provinces of China, 2005-2019. Infect Dis Poverty. 2022;11(1):12. doi:10.1186/s40249-022-00937-5
23. Sang S, Yue Y, Wang Y, Zhang X. The epidemiology and evolutionary dynamics of massive dengue outbreak in China, 2019. Front Microbiol. 2023;14(1156176). doi:10.3389/fmicb.2023.1156176
24. Guo Z, Liu W, Liu X, et al. Model-based risk assessment of dengue fever transmission in Xiamen City, China. Front Public Health. 2023;11(1079877).
25. Ding Z, Wu C, Wu H, Lu Q, Lin J. The Epidemiology of Imported Acute Infectious Diseases in Zhejiang Province, China, 2011-2016: analysis of Surveillance Data. Am J Trop Med Hyg. 2018;98(3):913–919. doi:10.4269/ajtmh.17-0284
26. Peng L, An T, Yuchao W, Kefeng L, Yaxin D, Jianbo Y. Survey and analysis of dengue prevention and control knowledge of medical personnel in Zhoushan City. J Int Epidem Infectious Dise. 2019;46(3):4.
27. Teotônio I, de Carvalho JL, Castro LC, et al. Clinical and biochemical parameters of COVID-19 patients with prior or active dengue fever. Acta Trop. 2021;214(105782):105782. doi:10.1016/j.actatropica.2020.105782
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.