")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Health Technology Assessment for Fast-Track Elective Knee and Hip Arthroplasty in a High-Volume Orthopaedic Hospital in Italy
Authors Restelli U, Vitale J, Croce E, Bernareggi S, Guida S, Silvola S, Banfi G, Zagra L
Received 19 February 2024
Accepted for publication 11 July 2024
Published 5 August 2024 Volume 2024:16 Pages 537—545
DOI https://doi.org/10.2147/CEOR.S464775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Samer Hamidi
Umberto Restelli,1 Jacopo Vitale,2 Edoardo Croce,3 Susan Bernareggi,3 Stefania Guida,3 Sofia Silvola,1,4 Giuseppe Banfi,3,5 Luigi Zagra3
1LIUC University, Castellanza, Italy; 2Schulthess Klinik, Zürich, Switzerland; 3IRCCS Istituto Ortopedico Galeazzi, Milan, Italy; 4Department of Public Health Medicine, School of Health System & Public Health, Faculty of Health Science, University of Pretoria, Pretoria, South Africa; 5Vita-Salute San Raffaele University, Milan, Italy
Correspondence: Umberto Restelli, Email [email protected]
Objective: The objective of the analysis presented is to assess the efficacy of a fast-track pathway for elective hip and knee arthroplasty, compared to the traditional approach, adopted within a research hospital located in Milan (Italy), in terms of length of stay reduction and related direct medical costs.
Methods: A monocentric observational retrospective study was implemented considering adult subjects who underwent elective primary total hip or knee replacement, with a diagnosis of primary or secondary osteoarthritis. Exclusion criteria were subjects admitted via emergency department, subjects undergoing knee or hip replacement because of fractures or prosthesis revision. The analysis compared the length of stay and the direct medical costs, assuming the hospital perspective, of subjects admitted in the pre-fast-track period (years 2016/2017) and during the fast-track period (years 2018/2019).
Results: Knee replacement mean costs are 5,599 € (± 1,158.3 €) in the pre-fast-track period and 4,487 € (± 978.4 €) in the fast-track period (− 1,112 €; − 19.9%). Hip replacement mean costs in the pre-fast-track period are 5,364 € (± 1,037.2 €) and 4,450 € (± 843.7 €) in the fast-track period (− 914 €; − 17.0%). The adoption of fast-track pathway led to a statistically significant decrease of days of hospitalization of − 2.8 (− 37.6%) in knee replacement and of − 2.9 (− 39.2%) in hip replacement.
Conclusion: The fast-track pathway adopted proved to be effective, reducing patients’ length of stay, and sustainable and efficient, reducing direct medical costs, for both elective hip and knee replacement surgeries.
Keywords: health economics, direct medical costs, observational, hip replacement, knee replacement
Introduction
Osteoarthritis (OA) is a common chronic health condition involving several alterations of joint tissues, including cartilage degradation, and leading to pain, stiffness, swelling and joint functional limitations.1 The Global Burden of Disease Study 2021 reports a global age-standardized prevalence rate per 100,000 people of osteoarthritis of 6,967.3 (6,180.7–7,686.1) in 2021, being higher in females (8,049.4; 7,137.2–8,892.7) than in males (5,773.4; 5,125.9–6,421.0), equal to more than 600 million individuals.2 The prevalence and incidence of knee and hip OA have been more studied than other joints; Cui et al3 reported that, in 2020, there were about 654 million individuals, aged over 40 years old, with knee OA worldwide. Similarly, the prevalence of symptomatic hip OA in adults aged over 45 years old has been estimated to be higher than 10%.4 OA has a high impact on chronic pain in Western society and in Italy it represents the main cause of total joint replacement in the 89.6% and 94.5% of cases, respectively, for hip and knee;5 thus, the incidence of arthroplasty surgery is increasing too. According to the 2020 annual report of the Italian Arthroplasty Registry, individuals undergoing elective hip and knee surgical procedures for OA were 71,626 and 82,815, respectively.5 For both procedures, the prevalence is higher among women (53.2%) than men and the mean age in 2019 was 65.5 years for males and 69.8 years for females. Kremers et al6 estimated that people in the United States who are currently living with an artificial hip or knee are 0.83% and 1.52%, respectively.6
Generally, clinical trials for hip and knee arthroplasty include too few patients to provide clear information on the efficacy of new health technologies; therefore, a multimodal standardized method for the assessment of health technology in orthopaedics is needed. In this context, Health Technology Assessment (HTA) represents a multidisciplinary approach providing information about the effectiveness, costs and impact of new health technologies in health care and is the key to the integration of technological evolution and the increasing requests of a more qualified health care.7 The lack of application of a standardized method to evaluate health technologies in the orthopaedic field makes HTA approach necessary to improve care treatment for patients and to share high-quality scientific evidence on specific methodology in health sciences.
The need to improve patients’ medical assistance, quality of life and to obtain data about the financial impact of hip and knee surgery due to OA have led the Italian National Institute of Health to allocate resources to assist patients with this specific orthopaedic disease and invest in new health technologies.
The health technology considered in the analysis is a fast-track pathway for subjects undergoing elective hip and knee arthroplasty at IRCCS Galeazzi Orthopedic Hospital. The pathway is aimed at reducing surgical invasiveness in terms of limited use and early removal of devices, reduction of perioperative fasting, early feeding, and mobilization.
To the best of our knowledge, only a previous study evaluated, through an HTA approach, the efficacy of an innovative Enhanced Recovery After Surgery pathway (ERAS) for hip and knee arthroplasty.8 In detail, it was shown that perioperative pathways promoting length of stay reduction, tissue-sparing surgical approach, multimodal pain management and early mobilization could be effective in reducing costs and improve patients’ outcomes after hip and knee surgery than the traditional approaches.8 The Galeazzi – Sant’Ambrogio Hospital (Milan, Italy) is a high-volume research hospital and the first institute in Italy for number of joint arthroplasties (>4,000/year) and such high number of these surgical procedures guarantees the possibility to perform an analysis based on a significant number of cases.
Therefore, the present study aims to assess the efficacy of the fast-track pathway for elective hip and knee arthroplasty (years 2018–2019), in terms of length of stay reduction, compared to the traditional approach (years 2016–2017) at the IRCCS Galeazzi – Sant’Ambrogio Hospital and the related direct medical costs.
Material and Methods
Study Design and Subjects
This retrospective study was conducted, in accordance with the STROBE guidelines,9 considering patients receiving surgical interventions for hip and knee replacement at the IRCCS (specialist clinic) Galeazzi – Sant’Ambrogio Hospital, located in Milan (Italy), between 1st January 2016 and 31st December 2019. In particular, patients who underwent elective primary total hip or knee replacement, with a diagnosis of primary or secondary osteoarthritis were included in the study procedures; patients admitted via emergency department, undergoing knee or hip replacement because of fractures or prosthesis revision were excluded. Details of inclusion and exclusion are reported in Figure 1. According to Article 110-bis, Legislative Decree 196/2203,
the processing of personal data collected for clinical activity, for research purposes, by the Scientific Institutes for Research, Hospitalization and Healthcare (IRCCS) does not constitute further processing by third parties;
therefore, the IRCCS are allowed to carry out research without new informed consent. National guidelines are available online at http://www.agenziafarmaco.gov.it/sites/default/files/decreto_24062003_inglese.pdf; https://www.gazzettaufficiale.it/eli/id/2019/06/12/19G00059/sg. All methods were carried out in accordance with relevant guidelines. Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.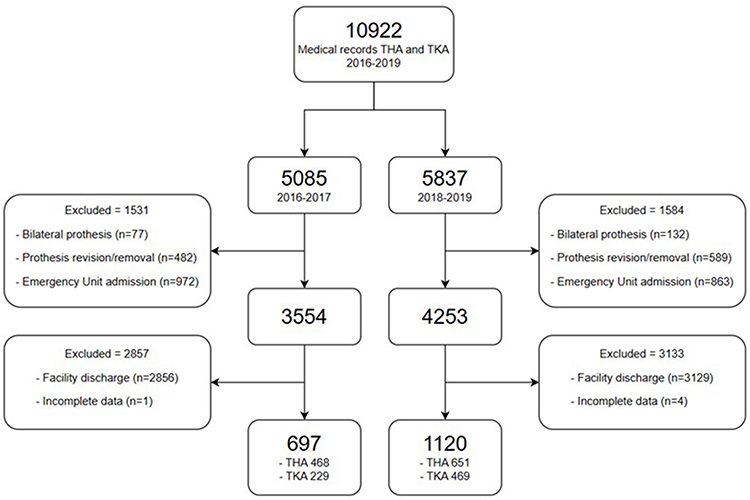 |
Figure 1 Flow chart of the study participants, highlighting inclusion and exclusion criteria. |
The analysis considered surgical interventions performed in two periods, based on whether fast-track was implemented or not. Pre-fast-track period is that between 2016 and 2017, while patients receiving knee or hip surgery in 2018 and 2019 were assigned to the fast-track group. To ensure comparability among the two groups, only subjects with a discharge at domicile were considered in the analysis. Demographic information of each patient was collected through the administrative databases of the hospital.
Fast-Track Pathway
Table 1 shows the details of the preoperative, intraoperative and postoperative phases of the fast-track pathway for hip and knee arthroplasty at IRCCS Galeazzi Orthopedic Hospital. The main characteristics of the fast-track pathway are as follows: 1) specific attention to preparing patients before surgery via direct interaction with surgeons, anesthesiologists, nurses, physiatrists, and physiotherapists; 2) reduced surgical invasiveness, determined not only by the surgical act itself but also by the limited use and early removal of devices such as nasogastric tubes and bladder surgical catheters; 3) reduction of perioperative fasting, early feeding, and mobilization. Therefore, the final aim of fast-track surgery is to promote early discharge (5th day), to promote a faster and more efficient functional recovery, and to reduce associated costs.
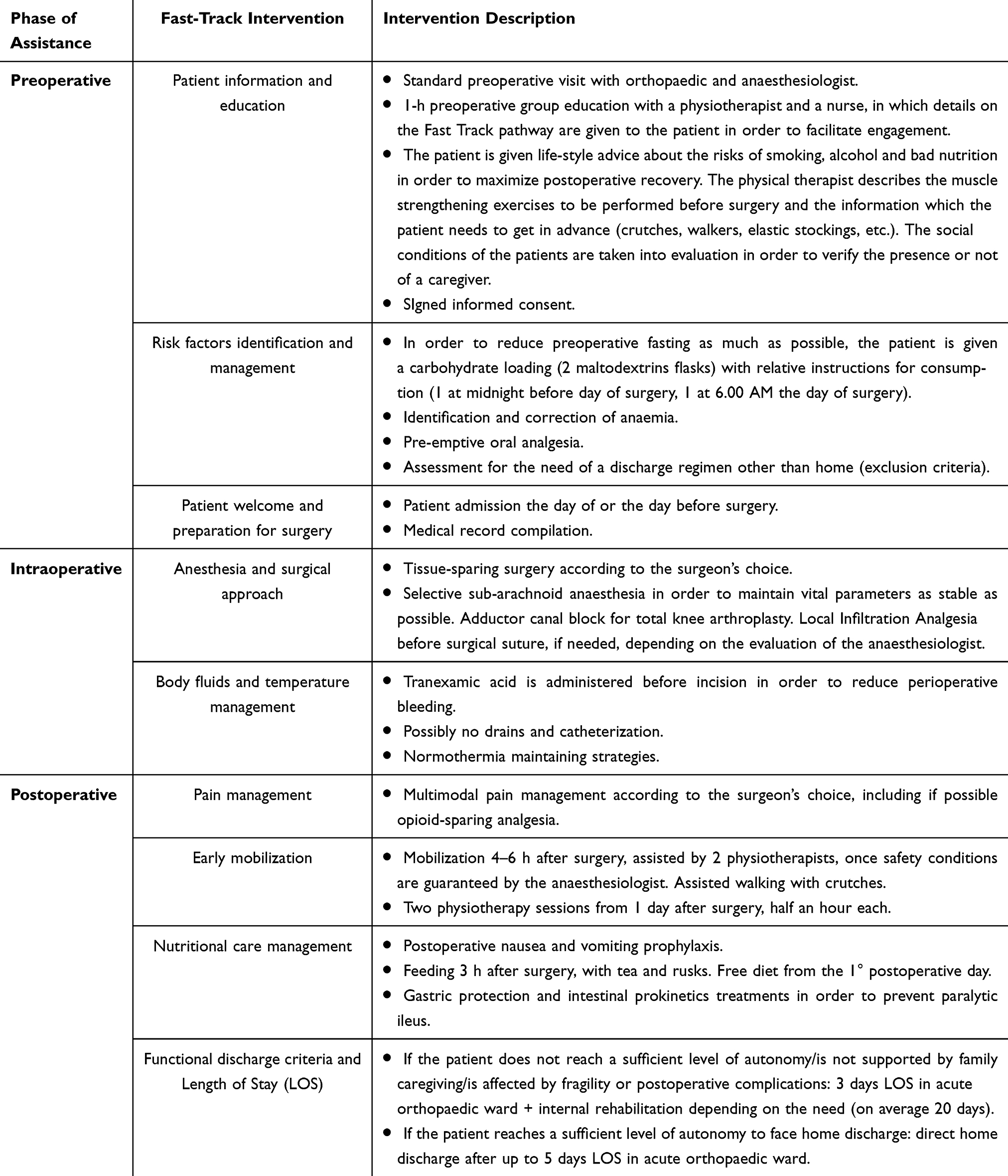 |
Table 1 Description of the Key Phases of the Fast-Track Pathway at IRCCS Galeazzi Orthopedic Hospital |
Data Mining and Cost Analysis
The process from pre-admission examination to discharge was analysed with the support of the hospital staff (anaesthesiologist, physiotherapist, surgeon, scientific director and researchers). Flow and cost data have been extracted using the Hospital Information System and a business intelligence software, while clinical data have been collected manually from patients’ medical records. Afterwards, all data were reported in an electronic database for the statistical analyses. Each medical record information related to the following phases was considered in the analysis to assess the economic impact of interventions from the hospital perspective: 1) pre-admission, admission, and pre-surgery activities; 2) surgical intervention; 3) post-surgery activities before discharge. In detail, the data extracted and reprocessed for the analysis, as presented in the sections below, were related with patient gender and age, type of surgical intervention, date and hour of admission and discharge, date and hour in which the patient entered and exit operating theatre, number and type of transfusions, x-rays, surgical kit, prosthesis type, drugs administered during the hospitalization (including anesthesia), biopsy, cultural tests, and surgeon visits. Furthermore, the cost related to the tests performed and to drugs administered, hotel costs, general costs, technologies amortization costs, human resources costs were collected. The pre-admission tests and visits were considered to be the same for each patient as the pre-admission process is standardized as the schedule of post-surgery rehabilitation.
The direct medical costs considered refer to year 2022, while the cost of prosthesis refers to the year in which each prosthesis was implanted.
Pre-Admission, Admission, and Pre-Intervention Activities
These activities include pre-admission examinations (echocardiogram, laboratory examinations, x-ray for 50% of patients, surgeon 30 minutes visit, anaesthesiologist 20 minutes visit, nursing 60 minutes assistance), pre-intervention visits (15 minutes for n = 1 anaesthesiologist and 15 minutes for n = 1 physiotherapist for the pre-fast-track period; 15 minutes for n = 1 anaesthesiologist and 30 minutes for n = 1 physiotherapist for the fast-track period) and the care activities performed by nursing staff, nursing assistant and physiotherapist between the admission and the intervention.
Surgical Intervention
Surgical intervention costs include the cost per minute of the surgical team (n = 1 anaesthesiologist, n = 2 surgeons, n = 1 operating room nurse, n = 1 nurse, n = 1 social care worker) and the surgical intervention duration; the transportation of the patient from the ward to the operating room and from the operating room to the ward (10 minutes for n = 1 social care workers per each transportation); non-woven fabrics, surgical kits; anaesthesiologic drugs; blood transfusions; intra-intervention x-ray; and prosthesis.
Post-Surgery Activities
In the post-intervention phase, the cost per day of hospitalization including care, physiotherapy, post-intervention x-ray, biopsy, cultural tests, and surgeon visit costs are included.
For each day of hospitalization, hotel costs were considered, as calculated by the hospital financial office. Unit cost data considered in the analysis are reported in Table 2. General costs were considered, being 22% of the costs emerged in the analysis. Since prosthesis cost represents almost 30% of the total cost of interventions, a further analysis was conducted excluding the cost of prosthesis to verify if the cost difference between the two scenarios (pre-fast-track and fast-track) may have been influenced by this element.
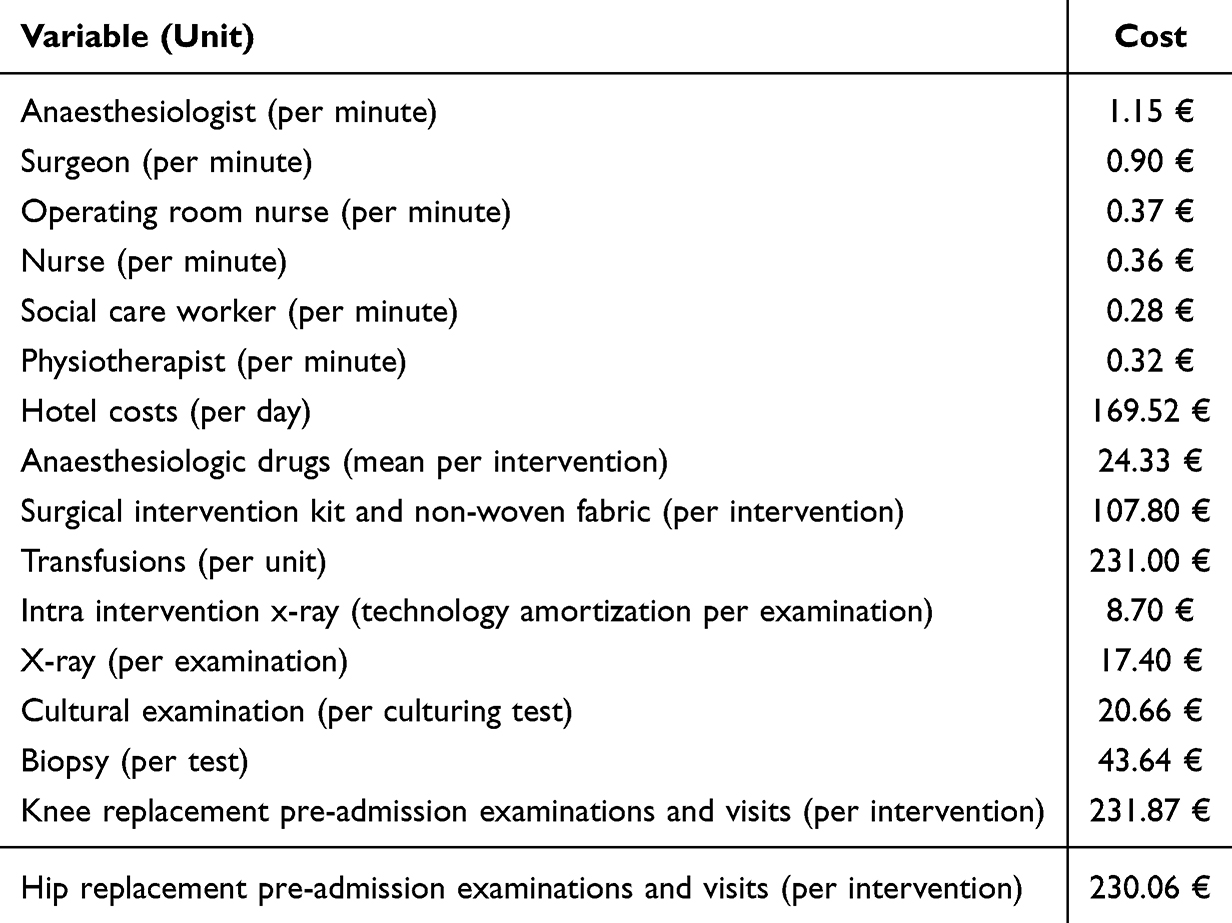 |
Table 2 Cost Data Considered in the Analysis (Source: Hospital Financial Office) |
Statistical Analysis
Means, standard deviations, medians and interquartile range values were used to summarize countable and continuous variables. Percentages and the number of patients were used to summarize categorical variables. Statistical comparisons across the groups of interest were performed using Pearson’s chi-squared test used for categorical variables, and for continuous variables, comparisons across patient groups were carried out using one-way ANOVA. A p value of ≤0.05 was set to define statistical significance. The primary endpoints of the analysis are the length of stay and direct medical costs assuming the hospital perspective.
Results
A total number of 1,817 patients were included in the analysis. Subjects considered in the pre-fast-track period are 229 for knee replacement and 468 for hip replacement, while subjects considered in the fast-track period are 469 for knee replacement and 651 for hip replacement. The characteristics of subjects included in the analysis are presented in Table 3.
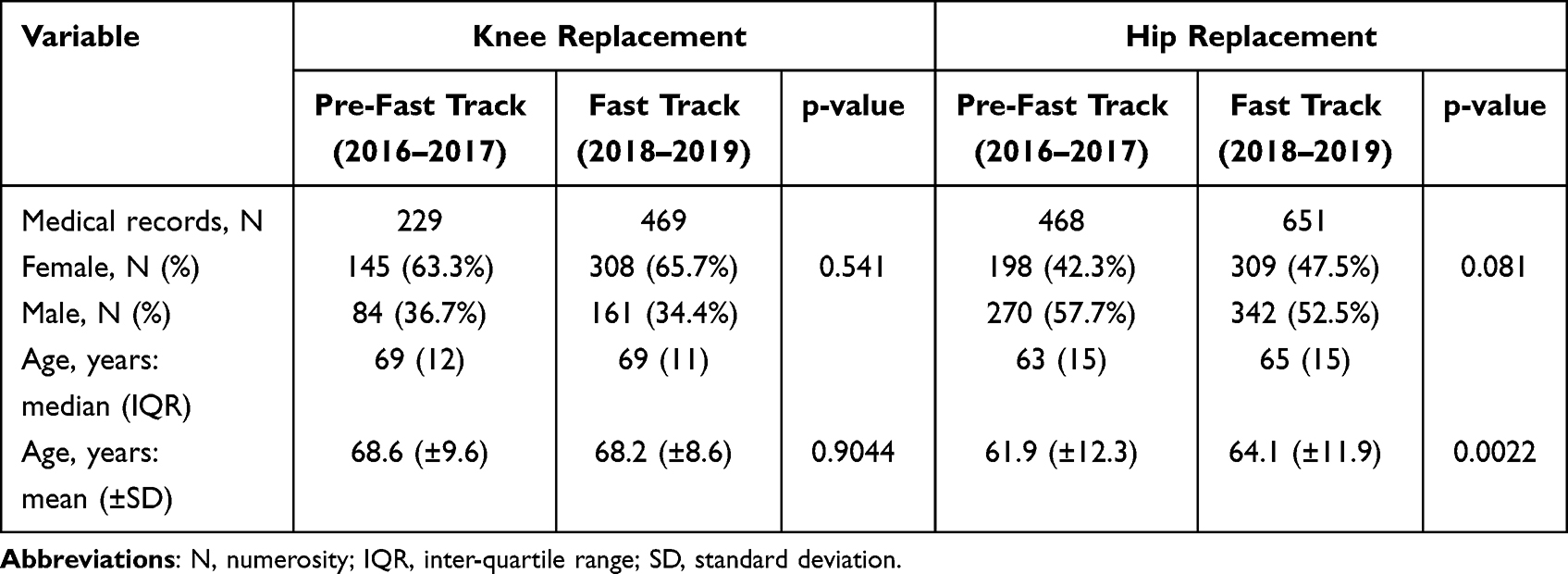 |
Table 3 Demographic Characteristics of the Patients (Total N = 1,817) Considered in the Analysis |
Considering the number of days of hospitalization, the adoption of fast-track leads to a decrease of −2.8 days (−37.6%) in knee replacement, from a mean number of days of 7.6 (± 2.8), to a mean number of days of 4.8 (± 1.8), and of −2.9 days (−39.2%) in hip replacement, from a mean number of days of 7.3 (± 2.7) to a mean number of days of 4.4 (± 2.0), as reported in Table 4. The difference in terms of length of stay between pre-fast-track period and fast-track is statistically significant both for knee replacement and hip replacement.
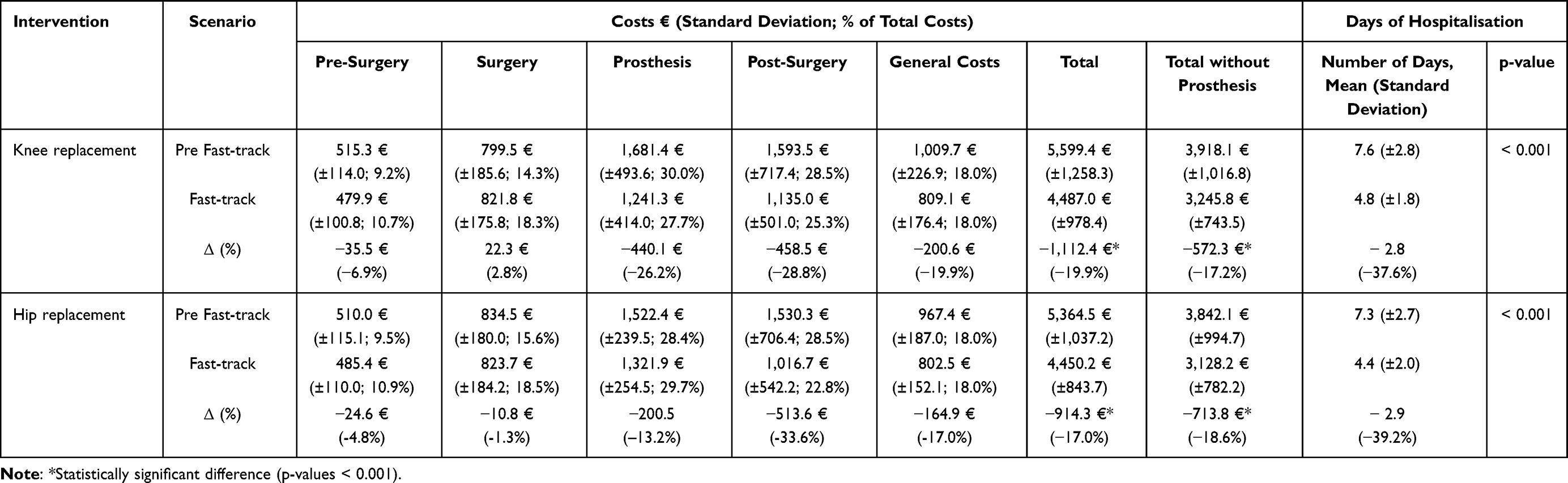 |
Table 4 Results of the Economic Analysis and Number of Days of Hospitalisation Between Pre-Fast-Track (2016–2017) and Fast-Track (2018–2019) Pathways |
Knee replacement mean costs are equal to 5,599 € (±1,258.3 €) in the pre-fast-track period, and to 4,487 € (±978.4 €) in the fast-track period, with a mean lower cost of the latter of −1,112 € (−19.9%). Excluding the cost of prostheses from the analysis, the mean costs in the pre-fast-track period for knee replacement are equal to 3,918 € (±1,016.8 €), while the mean cost of the intervention in the fast-track period is equal to 3,2456 € (±743.5 €), being 672 € lower (−17.2%).
For what concerns hip replacement, the mean cost in the pre-fast-track period is 5,364 € (±1,037.2 €), the mean cost in the fast-track period is 4,450 € (±843.7 €), with a mean lower cost in the fast-track period of −914 € (−17.0%). Also in this case, excluding the cost of prosthesis, the fast-track scenario is associated with a mean lower cost than the pre-fast-track one, being 3,842 € (±994.7 €) and 3,128 € (±782.2 €), respectively, with a differential cost of −713 € (−18.6%).
The main cost component of the total cost is represented by prosthesis, being almost 30% in both scenarios (30.0% and 27.7% for knee replacement; and 28.4% and 29.7% for hip replacement), followed by post-intervention costs (28.5% and 25.3% for knee replacement; and 28.5% and 22.8% for hip replacement). Excluding the cost of prosthesis, the main difference between the two scenarios is observed in the post-intervention costs. Details on the cost of the two interventions in the two scenarios are reported in Table 4.
Discussion
The authors assessed the effectiveness and economic implications of adopting a fast-track pathway aimed at optimising knee replacement and hip replacement procedures. In particular, the effectiveness of the pathway was assessed considering the length of stay (LOS) of subjects who underwent surgery in the years 2016–2017 (pre-fast-track period) and in the years 2018–2019 (fast-track period).
Hospitalization length represents the major contributor to costs associated with hip and knee surgery.10 In the last decade, a trend towards decreasing LOS was registered11 and several studies were developed to investigate whether a significant shortening in the hospitalization duration could have an impact on postoperative complication rate. Sarpong and colleagues11 in 2019 analysed data from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) registry, considering the years from 2006 to 2016, to investigate the 30-days complication days and unplanned readmissions. They showed a LOS significant reduction over the considered decade, associated with significantly lower rates of deep vein thrombosis, sepsis, and urinary tract infections in the first 30 days after surgery. Also, a decreasing in readmission rates was observed. Similarly, Morcos and colleagues12 evidenced that the lowest risk of 30-days complications following hip arthroplasty is associated with discharge on 0–2 postoperative days,12 while Benito and colleagues13 showed a significant lower 90-day readmission rate for subjects discharged on the first postoperative day, when compared to a cohort with a greater LOS from 2 to 4 days.13 The adoption of the proposed fast-track pathway allowed to reduce the mean number of days of hospitalization by −2.8 in subjects undergoing knee replacement and by -2.9 in subjects undergoing hip replacement, representing not only an advantage with reference to assistance costs but also clinical, reducing patient’s risk to develop postoperative complication. Direct medical costs related to fast-track compared with pre-fast-track period show a statistical significant reduction equal to −1,112 € (−19.9%) for knee replacement and to −914 € (−17.0%) for hip replacement. Also excluding the cost of prosthesis from the analysis, a statistically significant difference in terms of costs is observed related to fast-track pathway: −672 € (−17.2%) for knee replacement and −714 € (−18.6%) for hip replacement. The main percentage cost reduction for both interventions is observed in the post-intervention phase, with a reduction of costs in the fast-track scenario of −28.8% for knee replacement and of −33.6% for hip replacement.
A previous preliminary analysis of the consequences of adopting fast-track pathway was conducted by Vanni and colleagues.8 However, the analysis did not measure real costs related to the two alternative pathways but estimated the theoretical consequences of adopting the fast-track pathway. The costs measured in the analysis are in line with the previously published analyses. Stargardt14 calculated the cost of hip replacement intervention in 5 Italian hospitals (among other European hospitals), being between 4,524 € and 8,482 €.14 More recently, Fidanza and colleagues15 estimated the cost of hip replacement intervention in an Italian public hospital, being equal to 6,000.2 €.15 The analysis conducted allowed to assess in a solid way the economic consequences and the effectiveness of fast-track, comparing real data from medical records within the same specialist clinic orthopaedic hospital in the pre-fast-track period and in the fast-track period, measuring costs and length of stay in 698 knee replacement interventions and in 1,119 hip replacement interventions.
Conclusion
The adoption of fast-track pathway is associated with a significant decrease in length of stay for both knee replacement (−2.8 days) and hip replacement (−2.9 days) and with a statistically significant decrease in total costs of −1,112 € (−19.9%) and −914 € (−17.0%), respectively. This pathway proved to be effective (mean length of stay reduction), efficient and sustainable (mean direct medical cost reduction). Therefore, its adoption could represent an improvement in terms of organizational efficiency, allowing the opportunity, based on capacity, to improve the number of surgical interventions performed and reduce waiting lists.
Ethics and Consent Statements
According to Article 110-bis, Legislative Decree 196/2003, “the processing of personal data collected for clinical activity, for research purposes, by the Scientific Institutes for Research, Hospitalization and Healthcare (IRCCS) does not constitute further processing by third parties”; therefore, the IRCCS are allowed to carry out research without new informed consent. Therefore, based on the aforementioned Legislative Decree, no further ethical committee request was submitted. The scientific direction of the IRCCS Ospedale Galeazzi - Sant’Ambrogio approved the retrospective observational study protocol, which is supervised by the Italian National Institute of Health and waived the need for informed consent. The study complies with the Declaration of Helsinki.
Acknowledgments
The authors would like to thank Dr. Grazia Fontaneto, Dr. Edoardo Fascio, Dr. Paolo Sirtori, Dr. Paolo Perazzo and the administrative and operative offices of the IRCCS Galeazzi – Sant’Ambrogio Hospital for their valuable support during the different phases of data extraction and data mining.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This analysis was supported by the Italian Ministry of Health “Ricerca Corrente” and by a 2018 Ricerca Finalizzata grant (Italian Ministry of Health; Project code. NET-2018-12368077). The APC was funded by the Italian Ministry of Health “Ricerca Corrente”.
Disclosure
The authors declare that they have no competing interests.
References
1. Allen KD, Thoma LM, Golightly YM. Epidemiology of osteoarthritis. Osteoarthr Cartil. 2022;30(2):184–195. doi:10.1016/j.joca.2021.04.020
2. GBD. Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2021;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
3. Cui A, Li H, Wang D, et al. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 2020;29-30:100587. doi:10.1016/j.eclinm.2020.100587
4. Jordan JM, Helmick CG, Renner JB, et al. Prevalence of Hip symptoms and radiographic and symptomatic Hip osteoarthritis in African Americans and Caucasians: the Johnston County osteoarthritis project. J Rheumatol. 2009;36(4):809–815. doi:10.3899/jrheum.080677
5. Bacocco DL, Biondi A, Boniforti F Report annuale Registro Italiano ArtroProtesi 2020; 2020Available from: https://riap.iss.it/riap/it/.
6. Kremers HM, Larson DR, Crowson CS, et al. Prevalence of total Hip and knee replacement in the United States. J Bone Jt Surg Am. 2014;97(17):1386–1397. doi:10.2106/JBJS.N.01141
7. EUnetHTA Joint Action. HTA Core Model Handbook; 2016Available from: https://www.eunethta.eu/wp-content/uploads/2018/03/HTACoreModel3.0-1.pdf%0Ahttp://www.corehta.info.
8. Vanni F, Foglia E, Pennestrì F, et al. Introducing enhanced recovery after surgery in a high-volume orthopaedic hospital: a health technology assessment. BMC Health Serv Res. 2020;20(1):1–15. doi:10.1186/s12913-020-05634-3
9. Vandenbroucke JP, Von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4(10):1628–1654. doi:10.1371/journal.pmed.0040297
10. Mundi R, Axelrod DE, Najafabadi BT, et al. Early Discharge After Total Hip and Knee Arthroplasty—An Observational Cohort Study Evaluating Safety in 330,000 Patients. J Arthroplasty. 2020;35(12):3482–3487.e3. doi:10.1016/j.arth.2020.06.092
11. Sarpong NO, Boddapati V, Herndon CL, et al. Trends in Length of Stay and 30-Day Complications After Total Knee Arthroplasty: an Analysis From 2006 to 2016. J Arthroplasty. 2019;34(8):1575–1580. doi:10.1016/j.arth.2019.04.027
12. Morcos MW, Nowak L, Schemitsch E. Delayed discharge after total Hip arthroplasty is associated with an increased risk of complications. Can J Surg. 2022;65(5):E593–8. doi:10.1503/cjs.021219
13. Benito J, Stafford J, Judd H, et al. Length of Stay Increases 90-day readmission rates in patients undergoing primary total joint arthroplasty. J Am Acad Orthop Surg Glob Res Rev. 2022;6(3):1–5.
14. Stargardt T. Health service costs in Europe: cost and reimbursement of primary Hip replacement in nine countries. Health Econ. 2008;17(1):S9–20. doi:10.1002/hec.1328
15. Fidanza A, Schettini I, Palozzi G, et al. What Is the Inpatient Cost of Hip Replacement? A Time-Driven Activity Based Costing Pilot Study in an Italian Public Hospital. J Clin Med. 2022;11(23):6928. doi:10.3390/jcm11236928
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.