")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Healthcare Resource Use and Costs Among Individuals with Vitiligo and Psychosocial Comorbidities: Retrospective Analysis of an Insured US Population
Authors Lofland JH, Darbha S, Naim AB, Rosmarin D
Received 13 February 2024
Accepted for publication 17 July 2024
Published 8 August 2024 Volume 2024:16 Pages 557—565
DOI https://doi.org/10.2147/CEOR.S463987
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Giorgio Colombo
Jennifer H Lofland,1 Samyuktha Darbha,2 Ahmad B Naim,1 David Rosmarin3
1US Medical Affairs, Incyte Corporation, Wilmington, DE, USA; 2Health Economics and Outcomes Research, Datawave Solutions Corp, Cranbury, NJ, USA; 3Department of Dermatology, Indiana University School of Medicine, Indianapolis, IN, USA
Correspondence: Jennifer H Lofland, US Medical Affairs, Incyte Corporation, 1801 Augustine Cut-Off, Wilmington, DE, 19803, USA, Tel +1 302 498 5861, Email [email protected]
Purpose: This study aimed to describe healthcare resource utilization and costs among individuals with vitiligo who were diagnosed with ≥ 1 psychosocial comorbidity, using data from US claims databases.
Patients and Methods: A retrospective, observational cohort analysis of the IBM MarketScan Commercial and Medicare supplemental claims databases for US individuals with vitiligo aged ≥ 12 years and a first vitiligo claim between January 1 and December 31, 2018, was undertaken to assess psychosocial burden, including mental and behavioral health comorbidities.
Results: Of the 12,427 individuals included in the analysis, nearly 1 in 4 (23.5%) who had vitiligo were also diagnosed with ≥ 1 psychosocial comorbidity. A greater percentage of these individuals versus those who were not diagnosed with a psychosocial comorbidity had a vitiligo-related prescription claim (50.2% vs 45.4%; P< 0.0001), especially for oral corticosteroids (25.4% vs 16.6%; P< 0.0001) and low-potency topical corticosteroids (9.0% vs 7.6%; P< 0.05). Total vitiligo-related healthcare resource utilization and costs were consistent among individuals with and without psychosocial comorbidity despite significantly (P< 0.05) higher vitiligo-related ER visit utilization and expenditure among those with psychosocial comorbidity. Furthermore, individuals diagnosed with vitiligo and ≥ 1 psychosocial comorbidity had significantly (P< 0.0001) greater utilization of all-cause mean prescription claims (25.0 vs 12.8), outpatient services (other than physician and ER visits: 19.5 vs 11.3), outpatient physician visits (10.1 vs 6.4), inpatient stays (0.6 vs 0.1), and ER visits (0.4 vs 0.2) and incurred significantly higher mean (SD) direct medical expenditures ($18,804 [$46,621] vs $9833 [$29,094] per patient per year; P< 0.0001).
Conclusion: Individuals with vitiligo who were diagnosed with ≥ 1 psychosocial comorbidity incurred greater total all-cause but not vitiligo-related healthcare resource utilization and expenditures than those without diagnosis of psychosocial comorbidities. Identification of psychosocial comorbidities in individuals with vitiligo may be important for multidisciplinary management of vitiligo to reduce overall burden for individuals with vitiligo.
Keywords: vitiligo, mental health, behavioral health, healthcare resource utilization, HCRU, healthcare costs
Introduction
Vitiligo is a chronic autoimmune disease in which patches of skin are progressively depigmented due to melanocyte destruction.1 The prevalence of vitiligo in the United States ranges from 0.1% to 1.5%, thus affecting up to 5 million people based on 2022 US population estimates.2–5 Vitiligo is associated with significant quality-of-life impairment in routine activities, employment, and psychosocial health.6,7 Notably, individuals with vitiligo are approximately 5 times more likely to have depression than healthy individuals.8,9 In a previous study, individuals with vitiligo were more likely to be hospitalized for a mental health condition, with higher costs of inpatient care and increased length of stay, than those without vitiligo.10 In this cohort study, we analyzed healthcare resource utilization and costs among individuals with vitiligo and psychosocial burden, including mental and behavioral health comorbidities, in the United States using data from a claims database.
Materials and Methods
A retrospective, observational cohort analysis of the IBM (now Merative) MarketScan Commercial (for employer health plans) and Medicare supplemental claims databases was performed to identify individuals with an International Classification of Diseases, 10th revision (ICD-10) diagnosis code for vitiligo (codes: A67.2 [vitiligo of pinta], L80 [vitiligo], H02.73X [vitiligo of eye/eyelids and periocular area]) from January 1 through December 31, 2018 (index date corresponds with the first claim in this period). The databases were linked by encrypted unique patient IDs. Data in these databases included healthcare resource utilization. Eligible individuals were ≥12 years old with a medical claim for vitiligo in 2018 (first claim was index date) and 12 continuous months of post-index enrollment in their healthcare plan. Comorbidities and prescription data were identified based on prespecified codes from ICD-10 and the National Drug Code, respectively, during the 12-month post-index period for each individual. Psychosocial comorbidities included depression, anxiety, adjustment disorder, bipolar disorder, schizophrenia, attention-deficit/hyperactivity disorder, alcohol abuse, and substance abuse.11 Sleep disorder was also captured but was not used for group stratification purposes (ie, recorded for both groups). Prescription data included all paid costs captured in the claims data in the IBM MarketScan Commercial and Medicare supplemental claims databases. Demographics, healthcare resource utilization, and expenditures were aggregated at an individual level and summarized per patient per year (PPPY; defined as the average of total costs in 1 year per patient; expenditures were in 2018 US dollars [$]). Out-of-pocket costs were not available in this dataset and not included in the analysis. Error claims (ie, those with missing age or gender and or negative total costs) were excluded from the analyses. Data from the study population were summarized using descriptive statistics, and the subgroups of individuals with and without ≥1 diagnosed psychosocial comorbidity were compared using the chi-square test for categorical variables and t test for continuous variables.
Results
Overall, 18,309 individuals ≥12 years old were identified as being diagnosed with vitiligo in 2018; 12,427 who had ≥12 months of continuous post-index coverage were included in the analyses (Table 1). Mean (SD) age was 43.7 (16.9) years, and 53.2% were female. Most individuals (93.5%) were identified from the MarketScan Commercial database, and 6.5% were identified from the Medicare supplemental claims database. Almost one-fourth (23.5%) had a diagnosis of ≥1 psychosocial condition, with the most common psychosocial comorbidities among those individuals being depression (30.8%), adjustment disorder (20.3%), anxiety (20.3%), and sleep disorder (18.4%). Sleep disorder was recorded in a significantly lower percentage of individuals with vitiligo who did not have diagnosed psychosocial comorbidities (7.2%; P<0.0001). Approximately one-tenth (9.0%) of individuals with vitiligo had ≥1 comorbid autoimmune disorder, which occurred at a similar rate in individuals with versus without ≥1 psychosocial condition (Table 1).
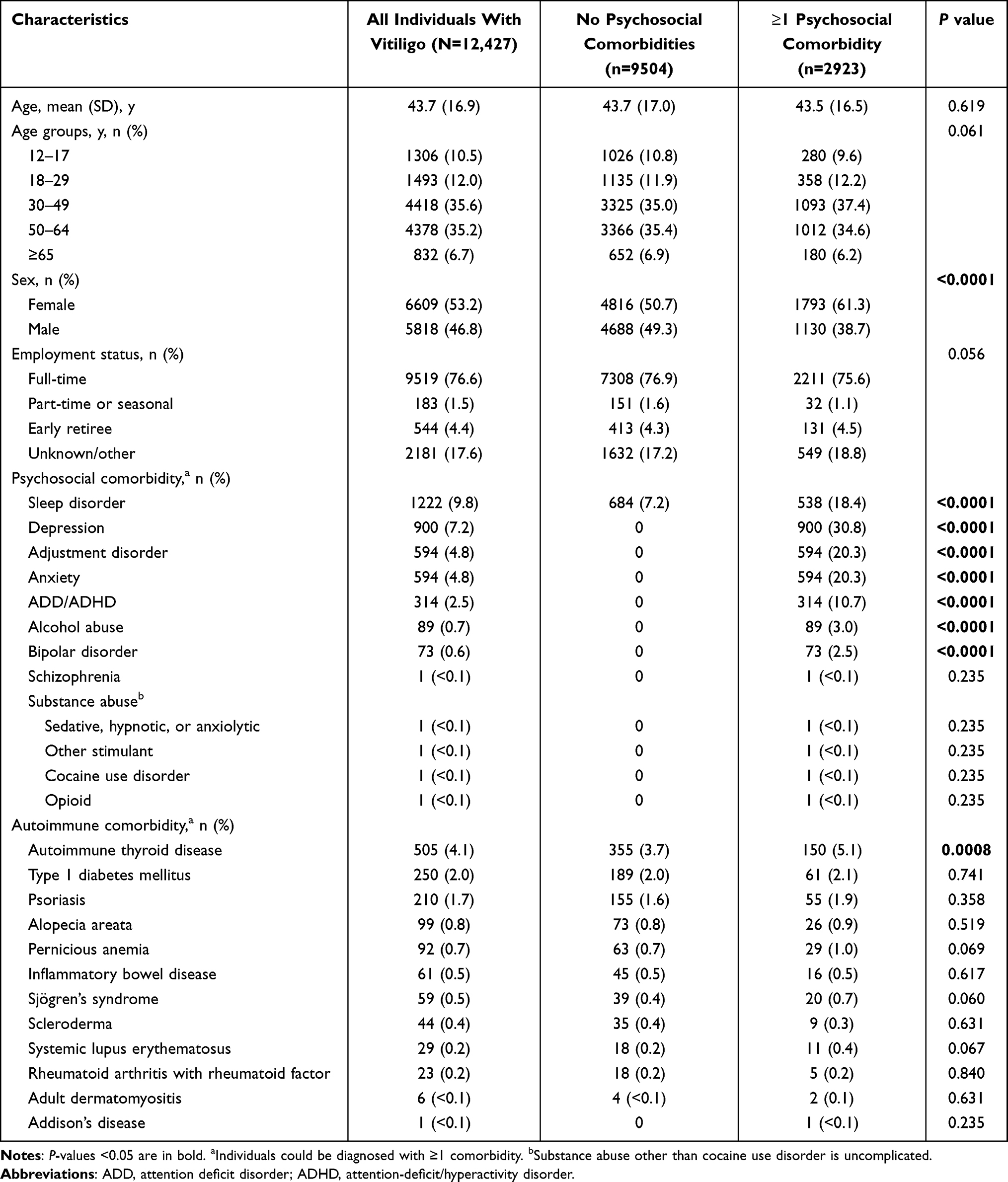 |
Table 1 Demographics and Baseline Characteristics of Individuals Diagnosed with Vitiligo |
During the 12-month post-index period, 52.8% of all 12,247 individuals diagnosed with vitiligo were seen by a dermatologist for any reason, and 46.5% had a pharmacy claim for prespecified vitiligo-related prescriptions. Half (50.2%) of 2923 individuals with ≥1 diagnosed psychosocial comorbidity had a pharmacy claim for vitiligo-related treatments (vs 45.4% of 9504 individuals without a diagnosed psychosocial comorbidity; P<0.0001). Overall, individuals with versus without ≥1 psychosocial comorbidity had greater utilization of vitiligo-related pharmacy claims (1.5 vs 1.2; P<0.01; Figure 1A); however, total mean (SD) PPPY vitiligo-related pharmacy costs were similar ($238 [$1592] vs $217 [$1205]; P=0.52; Figure 1B). Individuals with versus without ≥1 psychosocial comorbidity had similar rates of ≥1 vitiligo-related inpatient stay (0.6% vs 0.3%; P=0.07), outpatient visit (93.6% vs 94.1%; P=0.33), and emergency room (ER) visit (0.4% vs 0.2%; P=0.10); healthcare resource utilization and costs were consistent in both groups for vitiligo-related inpatient stays and outpatient physician visits. Significant differences were, however, seen for vitiligo-related ER visits healthcare resource utilization (0.01 vs 0.00; P<0.05) and mean (SD) PPPY healthcare expenditures ($22 [$535] vs $3 [$67]; P<0.05) among individuals with versus without ≥1 psychosocial comorbidity. Nevertheless, total annual vitiligo-related expenditure was similar for the 2 groups (mean [SD] PPPY, $1187 [$5012] vs $1112 [$4228]; P=0.47).
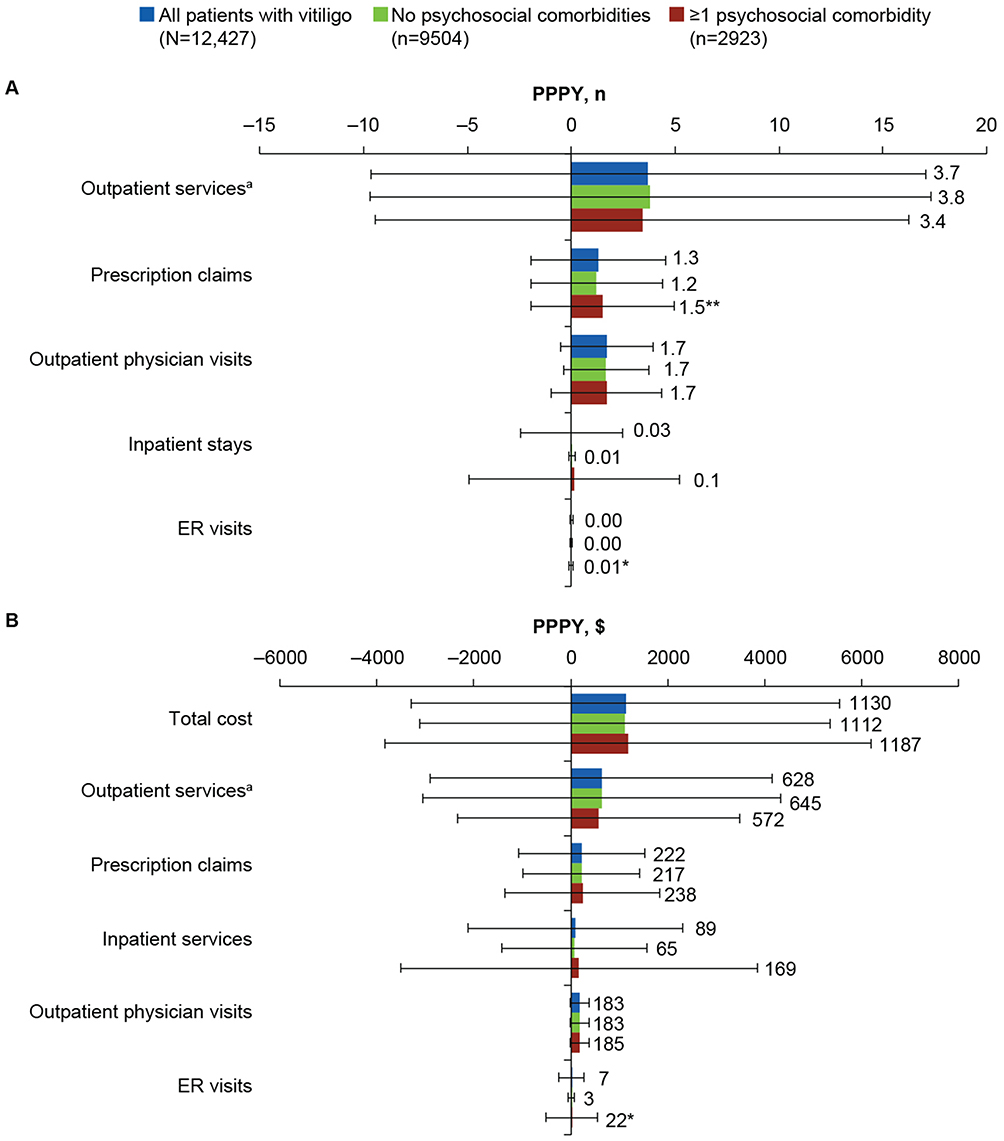 |
Figure 1 Vitiligo-related healthcare resource (A) utilization and (B) expenditure costs grouped by psychosocial comorbidity status in individuals with vitiligo. aDoes not include ER and physician visits. *P<0.05; **P<0.01. Abbreviations: ER, emergency room; PPPY, per patient per year. |
The most prescribed vitiligo-related therapies among all 12,427 individuals in the analysis set were topical calcineurin inhibitors (TCI; 21.1%), oral corticosteroids (OCS; 18.7%), and medium-potency topical corticosteroids (TCS; 9.8%; Figure 2A). There were significant differences in categories of therapies being prescribed for vitiligo among individuals with versus without ≥1 diagnosed psychosocial comorbidity, including prescribed OCS (25.4% vs 16.6%; P<0.0001), TCI (19.3% vs 21.7%; P<0.01), low-potency TCS (9.0% vs 7.6%; P<0.05), and laser therapy (5.1% vs 6.1%; P<0.05; Figure 2B). Prescription patterns for other therapies were comparable between the groups.
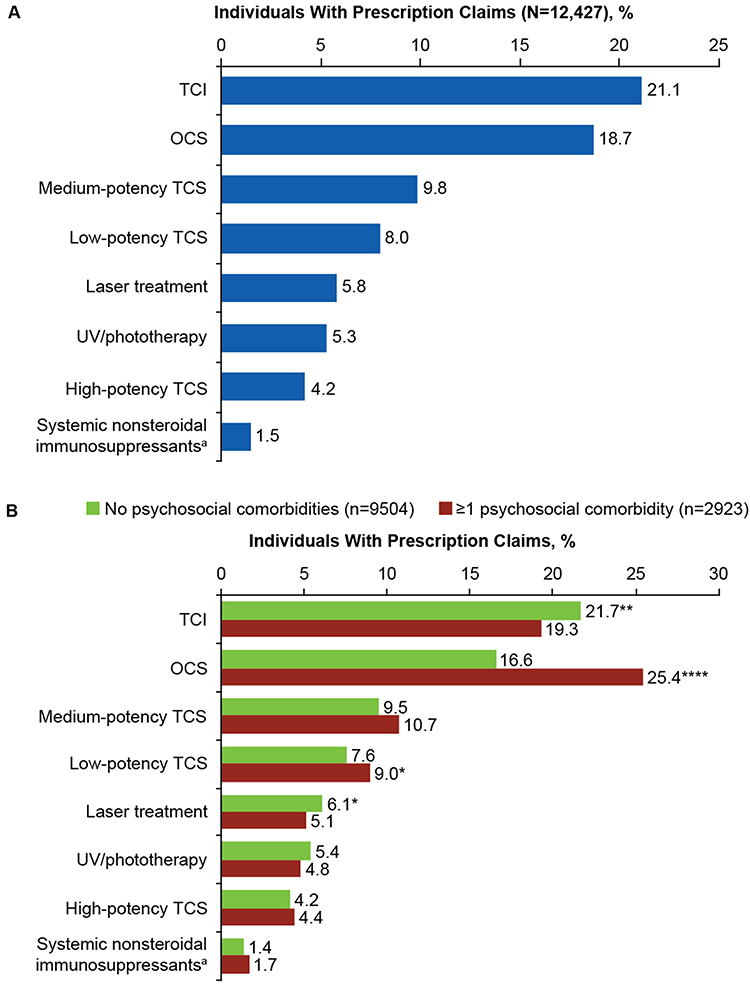 |
Figure 2 Percentage of individuals with prescription claims for vitiligo (A) among all individuals and (B) grouped by psychosocial comorbidity status. aSystemic nonsteroidal immunosuppressants include cyclosporine and methotrexate. Statistical analysis was performed using the chi-square test: *P<0.05; **P<0.01; ****P<0.0001. Abbreviations: OCS, oral corticosteroids; TCI, topical calcineurin inhibitor; TCS, topical corticosteroids; UV, ultraviolet. |
Among all 12,427 individuals in the analysis set, 99.7% had ≥1 all-cause outpatient medical visit during the 12-month post-index follow-up, and 91.4% had post-index prescription claims for any reason. All-cause ER visits were made by 15.1% of individuals, and 4.0% had a hospital admission, with a mean (SD) inpatient stay of 5.3 (14.2) days. Mean (SD) cost of all-cause and vitiligo-related healthcare PPPY for all individuals with vitiligo was $11,943 ($34,248) and $1130 ($4425), respectively (Table 2). More individuals with versus without ≥1 psychosocial comorbidity had an all-cause inpatient stay (6.7% vs 3.1%; P<0.0001), visited the ER (23.8% vs 12.5%; P<0.0001), and had prescription claims (96.4% vs 89.8%; P<0.0001). Individuals with versus without ≥1 psychosocial comorbidity had significantly (P<0.0001) greater utilization of all-cause mean prescription claims (25.0 vs 12.8), outpatient services (other than physician and ER visits: 19.5 vs 11.3), outpatient physician visits (10.1 vs 6.4), inpatient stays (0.6 vs 0.1), and ER visits (0.4 vs 0.2; Figure 3A). Mean (SD) all-cause PPPY total healthcare expenditures ($18,804 [$46,621] vs $9833 [$29,094]) and costs related to outpatient services ($8942 [$31,580] vs $4518 [$18,310]), prescriptions ($4229 [$14,760] vs $2872 [$14,399]), inpatient services ($3289 [$21,211] vs $1185 [$10,821]), outpatient physician visits ($1274 [$1149] vs $782 [$729]), and ER visits ($1069 [$3799] vs $476 [$2440]) were significantly (P<0.0001) higher among individuals with versus without ≥1 psychosocial comorbidity (Figure 3B).
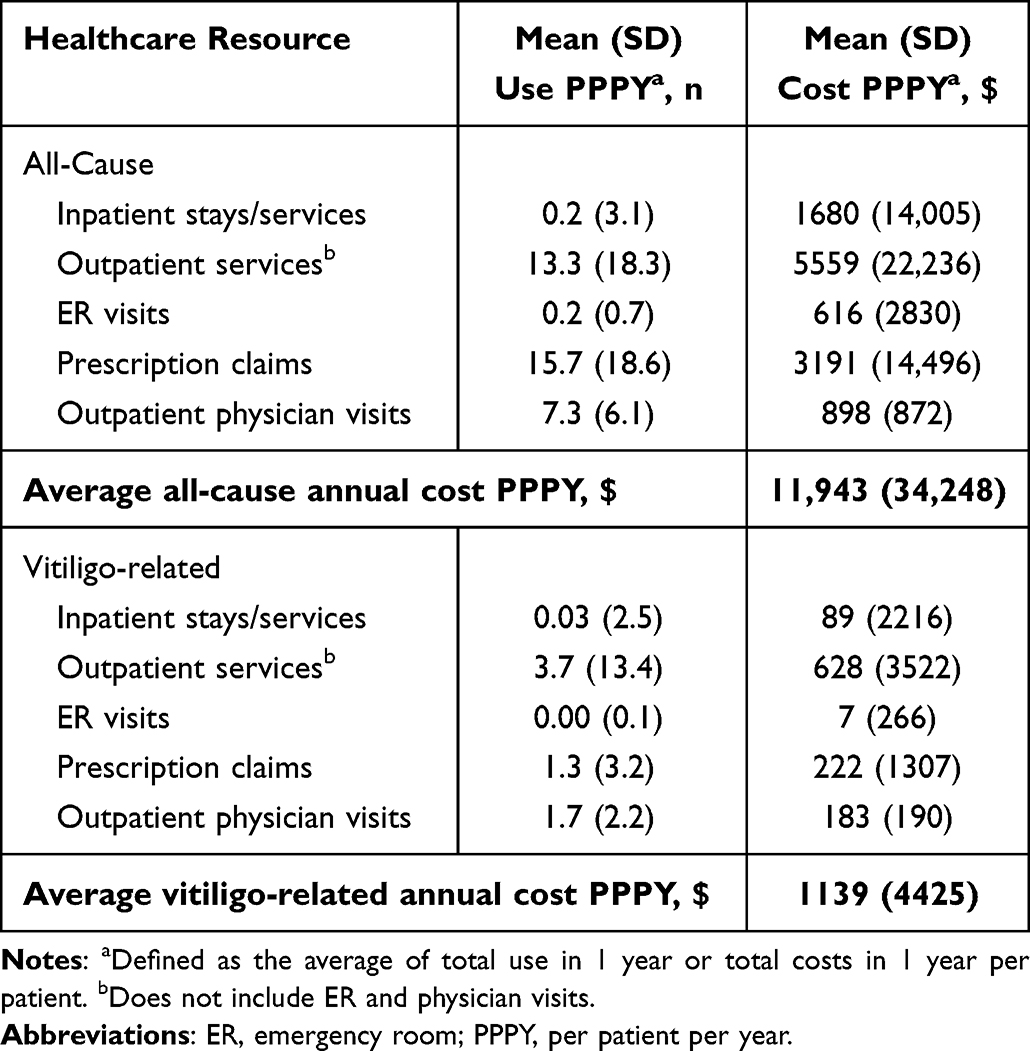 |
Table 2 Healthcare Resource Utilization for All Individuals with Vitiligo |
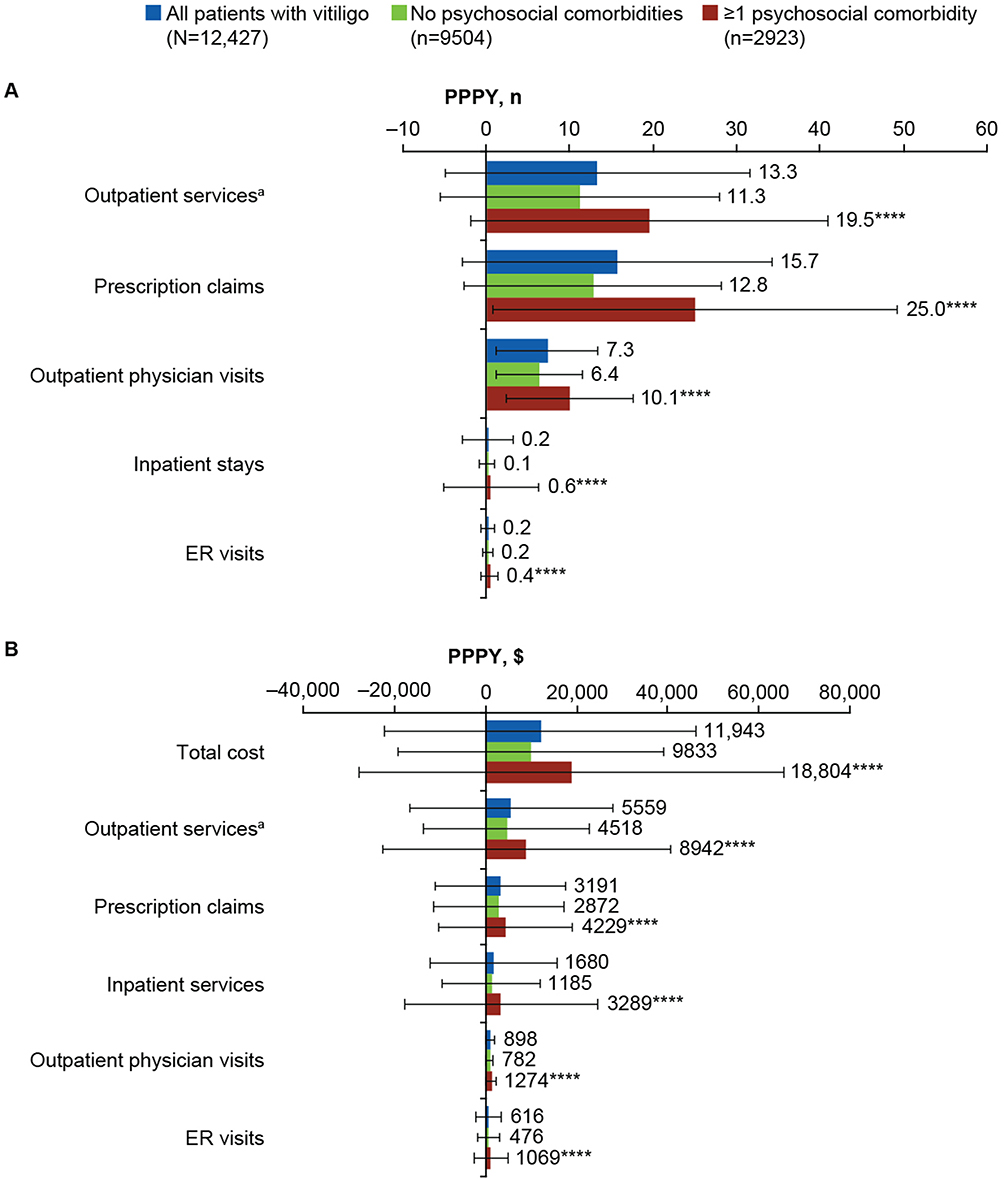 |
Figure 3 All-cause healthcare resource (A) utilization and (B) expenditure costs grouped by psychosocial comorbidity status in individuals with vitiligo. aDoes not include ER and physician visits. ****P<0.0001. Abbreviations: ER, emergency room; PPPY, per patient per year. |
Discussion
Our analysis of US insurance claims databases found that nearly 1 in 4 individuals with vitiligo was diagnosed with ≥1 psychosocial comorbidity. A higher percentage of individuals with ≥1 psychosocial comorbidity had a pharmacy claim for vitiligo-related treatments, especially for OCS and low-potency TCS. OCS may be prescribed during vitiligo flares,12 which were reported to occur during periods of stress in nearly two-thirds of patients in a recent global survey.13 Thus, greater claims for OCS in this subpopulation could be an indicator of increased vitiligo activity during periods of increased psychosocial stress14 among individuals with mental health comorbidities.
Individuals with ≥1 psychosocial comorbidity also had greater overall prescription claims versus those without a diagnosed psychosocial comorbidity, which is not unexpected given the potential need for treatment of associated comorbidities. Although approximately 1 in 10 individuals with vitiligo also had ≥1 comorbid autoimmune disorder, individual rates were similar in those with and without ≥1 psychosocial comorbidity. This indicates that psychosocial comorbidity is likely related to vitiligo rather than comorbid autoimmune burden. Individuals diagnosed with ≥1 psychosocial comorbidity also had disproportionately greater utilization of all-cause ER, outpatient services, outpatient physician visits, inpatient stays, and prescription claims. These differences were further reflected in direct costs PPPY in healthcare expenditures, highlighting the greater financial burden incurred by individuals with vitiligo who were diagnosed with ≥1 psychosocial comorbidity versus those without a psychosocial comorbidity. Total vitiligo-related healthcare resource utilization and costs were similar for individuals with versus without ≥1 psychosocial comorbidity. There was, however, higher annual vitiligo-related utilization for ER visits and pharmacy claims as well as higher expenditure for ER visits among individuals with versus without ≥1 psychosocial comorbidity, suggesting increased vitiligo-related distress (and possibly flares) among individuals who have psychosocial comorbidities. Additionally, the imbalance in all-cause total utilization and costs despite consistent vitiligo-related total utilization and costs among individuals with versus without ≥1 psychosocial comorbidity suggests that psychosocial burden contributes largely to the disparity.
The underlying comparability between the MarketScan Commercial and Medicare supplemental populations and the prevailing 2018 US census population, with only a slight overrepresentation of female patients (51.5% vs 50.5%) and an underrepresentation of patients aged 65 years and older (4% vs 9%), provides a strong platform for this analysis. Limitations of this study are those consistent with retrospective, administrative claims analyses, including the potential for sampling bias, incomplete records, improper data entry, and differences in actual versus physician-directed medication use. Data analyzed in this study were the latest available at the time of analysis, with the 2018 index period and 12-month post-index period (into 2019) predating the COVID-19 pandemic. Variables pertaining to individual and disease characteristics (eg, ethnicity/race, Fitzpatrick skin type, vitiligo extent, body surface area) were not available, so associations between these characteristics could not be analyzed. Furthermore, the cohorts in the study were not matched with respect to these variables, nor were data available for individuals without vitiligo who had mental and/or behavioral disorders, thus limiting the generalizability of the analysis. Healthcare resource utilization and costs directly related to mental and/or behavioral disorders were not collected. Data were not provided regarding whether diagnosis of psychosocial conditions occurred before or after the onset of vitiligo, and prespecified vitiligo-related treatments may not have been used for the treatment of vitiligo. No multivariate analyses were performed to determine relationships. Individuals who were not diagnosed with a psychosocial comorbidity may have undiagnosed conditions, potentially biasing the data in this group. Furthermore, out-of-pocket expenditures, which may be considerable due to payers not covering some vitiligo therapies,15 were not available within the dataset. Likewise, the direct, individual, and societal costs of vitiligo may be underreported in US claims databases.
Conclusions
In summary, nearly 1 in 4 individuals with vitiligo identified in a US claims database were diagnosed with ≥1 psychosocial comorbidity. While further investigation is required to better understand the burden of psychosocial comorbidities in individuals with vitiligo, we found that these individuals incurred greater all-cause but not vitiligo-related healthcare consumption and expenditures versus those with vitiligo but without diagnosed psychosocial conditions. These findings emphasize the need to identify psychosocial comorbidities among individuals with vitiligo and reduce the associated burden through multidisciplinary management of their vitiligo, including ensuring effective management of mental and behavioral health comorbidities.
Abbreviations
ER, emergency room; ICD-10, International Classification of Diseases, 10th revision; OCS, oral corticosteroids; PPPY, per patient per year; TCI, topical calcineurin inhibitors; TCS, topical corticosteroids.
Data Sharing Statement
Access to individual patient-level data is not available for this study.
Ethics Approval and Informed Consent
Ethics approval of the study protocol and informed consent were not required based on the use of deidentified insurance claims data and no direct patient involvement.
Acknowledgments
We thank Vijay N. Joish, MS, PhD (Incyte Corporation, at the time of the study) for leading the development of the analysis for this study, which was funded by Incyte (Wilmington, DE, USA), as well as Shreekant Parasuraman, PhD, and Jinan Liu, PhD, of Incyte for their critical review of the manuscript. Writing assistance was provided by Joshua Solomon, PhD, of ICON (Blue Bell, PA, USA) and was funded by Incyte.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was provided by Incyte Corporation (Wilmington, DE, USA). The sponsor had roles in study design, data analysis, and data interpretation.
Disclosure
JHL and ABN are employees and shareholders of Incyte Corporation. SD is an employee of Datawave Solutions. DR has received honoraria as a consultant for AbbVie, Abcuro, Almirall, AltruBio, Arena, Astria, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Concert, CSL Behring, Dermavant Sciences, Dermira, Incyte, Janssen, Kymera, Kyowa Kirin, Lilly, Nektar, Novartis, Pfizer, RAPT, Regeneron Pharmaceuticals, Recludix, Revolo Biotherapeutics, Sanofi, Sun Pharmaceuticals, UCB, Viela Bio, and Zura Bio; has received research support from AbbVie, Amgen, Bristol Myers Squibb, Celgene, Dermira, Galderma, Incyte, Janssen, Lilly, Merck, Nektar, Novartis, Pfizer, RAPT, and Regeneron Pharmaceuticals; and has served as a paid speaker for AbbVie, Amgen, Bristol Myers Squibb, Celgene, Dermavant, Incyte, Janssen, Lilly, Novartis, Pfizer, Regeneron Pharmaceuticals, and Sanofi. The authors report no other conflicts of interest in this work.
References
1. Rodrigues M, Ezzedine K, Hamzavi I, Pandya AG, Harris JE. New discoveries in the pathogenesis and classification of vitiligo. J Am Acad Dermatol. 2017;77(1):1–13. doi:10.1016/j.jaad.2016.10.048
2. Kruger C, Schallreuter KU. A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol. 2012;51(10):1206–1212. doi:10.1111/j.1365-4632.2011.05377.x
3. Bibeau K, Pandya AG, Ezzedine K, et al. Vitiligo prevalence and quality of life among adults in Europe, Japan and the USA. J Eur Acad Dermatol Venereol. 2022;36(10):1831–1844. doi:10.1111/jdv.18257
4. Gandhi K, Ezzedine K, Anastassopoulos KP, et al. Prevalence of vitiligo among adults in the United States. JAMA Dermatol. 2022;158(1):43–50. doi:10.1001/jamadermatol.2021.4724
5. US Census Bureau. U.S. Population Estimated at 332,403,650 on Jan. 1, 2022. Available from: https://www.census.gov/library/stories/2021/12/happy-new-year-2022.html.
6. Morrison B, Burden-Teh E, Batchelor JM, Mead E, Grindlay D, Ratib S. Quality of life in people with vitiligo: a systematic review and meta-analysis. Br J Dermatol. 2017;177(6):e338–e339. doi:10.1111/bjd.15933
7. Silverberg JI, Silverberg NB. Association between vitiligo extent and distribution and quality-of-life impairment. JAMA Dermatol. 2013;149(2):159–164. doi:10.1001/jamadermatol.2013.927
8. Lai YC, Yew YW, Kennedy C, Schwartz RA. Vitiligo and depression: a systematic review and meta-analysis of observational studies. Br J Dermatol. 2017;177(3):708–718. doi:10.1111/bjd.15199
9. Wang G, Qiu D, Yang H, Liu W. The prevalence and odds of depression in patients with vitiligo: a meta-analysis. J Eur Acad Dermatol Venereol. 2018;32(8):1343–1351. doi:10.1111/jdv.14739
10. Patel KR, Singam V, Rastogi S, Lee HH, Silverberg NB, Silverberg JI. Association of vitiligo with hospitalization for mental health disorders in US adults. J Eur Acad Dermatol Venereol. 2019;33(1):191–197 doi:10.1111/jdv.15255.
11. Ezzedine K, Eleftheriadou V, Jones H, et al. Psychosocial effects of vitiligo: a systematic literature review. Am J Clin Dermatol. 2021;22(6):757–774. doi:10.1007/s40257-021-00631-6
12. Kim SM, Lee HS, Hann SK. The efficacy of low-dose oral corticosteroids in the treatment of vitiligo patients. Int J Dermatol. 1999;38(7):546–550. doi:10.1046/j.1365-4362.1999.00623.x
13. Hamzavi IH, Bibeau K, Grimes P, et al. Exploring the natural and treatment history of vitiligo: perceptions of patients and healthcare professionals from the global VALIANT study. Br J Dermatol. 2023;189(5):569–577. doi:10.1093/bjd/ljad245
14. Henning SW, Jaishankar D, Barse LW, et al. The relationship between stress and vitiligo: evaluating perceived stress and electronic medical record data. PLoS One. 2020;15(1):e0227909. doi:10.1371/journal.pone.0227909
15. Blundell A, Sachar M, Gabel CK, Bercovitch LG. The scope of health insurance coverage of vitiligo treatments in the United States: implications for health care outcomes and disparities in children of color. Pediatr Dermatol. 2021;38(2):79–85. doi:10.1111/pde.14714
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.