")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 16
Insights into the Refusal of Free Screening Mammograms: Exploring Contributing Factors
Authors Alshamsan B , Alajlan T, Alsalhi A, Rabbani U
Received 5 April 2024
Accepted for publication 13 August 2024
Published 17 August 2024 Volume 2024:16 Pages 471—481
DOI https://doi.org/10.2147/BCTT.S472367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pooja Advani
Bader Alshamsan,1,2 Tasneem Alajlan,3,4 Ahlam Alsalhi,4 Unaib Rabbani5
1Department of Medicine, College of Medicine, Qassim University, Qassim, Saudi Arabia; 2Medical Oncology Department, Prince Faisal Cancer Center, King Fahad Specialist Hospital, Qassim Cluster, Qassim, Saudi Arabia; 3Health and Curative Programs Department, Public Health and Community Health Administration, Qassim Cluster, Buraidah, Saudi Arabia; 4Family Medicine Department, Almuntazah PHC, King Fahad Specialist Hospital, Qassim Cluster, Buraidah, Saudi Arabia; 5Family Medicine Department, Family Medicine Academy, Qassim Health Cluster, Buraidah, Saudi Arabia
Correspondence: Bader Alshamsan, Department of Medicine, College of Medicine, Qassim University, King Abdulaziz Road, Buraydah, Qassim, 52571, Saudi Arabia, Email [email protected]
Background: Despite the availability of free screening mammograms (SMG) through the Breast Cancer Early Detection (BCED) Program in the Qassim region of Saudi Arabia, a notable gap exists between program implementation and the actual uptake of SMG. This study aims to assess the refusal rate, identify barriers to participation, and shed light on the factors influencing women’s decisions regarding SMG.
Methods: A cross-sectional study was conducted among consecutive women aged 40– 69 participating anonymously in the BCED program in September 2023. The participants were administered a validated Arabic language survey encompassing breast cancer screening backgrounds and knowledge, reasons for refusal, and factors influencing SMG reconsideration. Logistic regression was employed to identify factors linked with SMG refusal using SPSS version 28.
Results: Of the 2446 eligible women in the study, 576 (23.6%) declined to undergo SMG. The median age of participants was 49 years, primarily married (91.5%) and residing in central cities (60.3%). Previous mammogram history was reported by 21.4%, with only 12.9% performing regular SMGs every 1– 2 years. Married women had a 31% lower refusal likelihood to SMG compared to widowed/divorced women (Adjusted Odds Ratio [aOR] = 0.69, p = 0.02). Women residing in peripheral areas showed approximately 1.45 times higher odds of refusal compared to those in central cities (aOR = 1.45, p < 0.001), and women without prior history of SMG had 2.13 times higher odds of refusal (aOR = 2.14, p < 0.001).
Conclusion: The refusal rate for SMG in the Qassim region aligns closely with rates observed in developed countries. Despite this progress, significant barriers to SMG uptake persist, and tailored interventions targeting specific demographic groups and addressing these barriers are essential to improving screening participation, promoting a culture of proactive screening behavior, and ensuring equitable access to screening services for all eligible women.
Keywords: screening mammograms, breast cancer, Qassim, Saudi Arabia
Introduction
Breast cancer (BC) stands as the most prevalent cancer among females worldwide and in Saudi Arabia (SA).1,2 In 2020, BC accounted for 35% of new cases and 8.4% of cancer-related deaths among females in SA.2 Although the age-standardized incidence rate (ASR) of BC among females in SA and the Qassim region is lower than the global rate at 28.4 and 28.1 vs 54.1 per 100,000 women.1,3 However, there has been a notable increase in the annual percentage change (APC) from 2002 to 2016, with rates of 4.8% and 7%, respectively.4 Screening mammograms (SMG) is vital in early BC detection and mortality reduction.5 However, the rate of screen-detected BC in SA is low at 11.2%,6 indicating limited uptake of SMG and emphasizing the need for enhanced efforts to promote BC screening. The National Breast Cancer Early Detection (BCED) Program in Saudi Arabia received approval in May 2011 and was officially established in March 2012,7 with Qassim region initiating the regional SMG initiative as early as 2007.8 The program is designed to provide free screening mammograms to women aged between 40 and 69 years without genetic predisposition, having a history of chest radiotherapy for Hodgkin’s lymphoma between the ages of 10 to 30 years, prior history of breast or ovarian cancer, family history of breast or ovarian cancer, or BC symptoms such as breast pain, lumps, or discharge.7 Women can enter the program through self-referral or referral by a healthcare practitioner. The recommended frequency for screening is every two years. The program in the Qassim region follows the same guidelines and procedures as the rest of Saudi Arabia. Notably, the practitioners involved in the program are predominantly female, aligning with practices in many international programs. The utilization rate of SMG among eligible women in SA varies between 6%-47%,9–18 in contrast to the higher rates of 58%-89% reported in Western countries.19–22 Commonly cited obstacles to undergoing SMG include lack of time, fear of discovering cancer or undergoing cancer treatment, apprehensions related to hospitals and healthcare facilities, discomfort or embarrassment during the procedure, concerns of pain, perception of not needing it without breast lumps, a belief of being too young and reservation about radiation exposure as documented in numerous studies.9,10,16,23–28
Qassim, located centrally within SA, is one of the nation’s 13 administrative regions. It spans an area of 73,000 square kilometers, representing approximately 3.2% of the country’s land area. It hosts a population of 1.45 million and an annual growth rate of 2.36%.29,30 In efforts to combat BC, the BCED program in Qassim employs various strategies, including conducting awareness campaigns, organizing educational workshops, and deploying mobile SMG units. The program provides free SMG and operates through 149 primary healthcare centers connected to 7 mammogram centers.31 Suspected cases detected during screenings undergo further evaluation by specialized health practitioners, and confirmed cases are referred to the oncology center. Despite these efforts, there remains a notable gap between program implementation and the actual uptake of SMG among eligible women. Therefore, this research aims to assess the SMG refusal rate, identify barriers to participation, and shed light on the factors influencing women’s decisions regarding SMG. The insights gained from this study are intended to inform evidence-based aimed at improving BC screening efforts and ultimately enhancing health outcomes in the Qassim region.
Patients and Methods
A cross-sectional study was conducted among consecutive women aged 40 to 69 years who visited primary health care centers between September 3 and October 2, 2023. These women were eligible for the screening mammography (SMG) program, which targets all eligible visitors to the centers, regardless of the reason for their visit. While the SMG program is part of the routine care for eligible women, the research study sought additional participation and data collection. The study was approved by the Regional Research Ethics Committee of Health and Curative Programs Department, Public Health and Community Health Administration, Qassim Cluster, Qassim Province (number 607/45/1567). Informed consent was obtained from all participants in adherence to ethical guidelines. All methods were conducted in compliance with the Declaration of Helsinki and the relevant guidelines and regulations. Eligibility for the study was determined based on criteria identical to those of the BCED program for screening mammography.7 Only those who expressed willingness to participate, had not been referred for SMG within the past two years and confirmed their capability to complete the survey were included. The sample size was determined using the OpenEpi program, considering an expected refusal rate of 49% based on the previous local data of the BCED program in June 2023. With a confidence level of 95% and a precision of 2%, the required sample size was calculated to be 2395 women. With an expected response rate of 50%, the targeted screened women for the study were set at 4800 women.
Survey Structure and Data Management
The survey questions were adopted from the revised Champion’s barriers scale for SMG32 and reported barriers from previous studies.9,10,16,23–28 The survey was pilot-tested on 30 women and underwent meticulous translation into Arabic and validation by healthcare professionals specializing in biolinguistics to ensure clarity, appropriateness, and precision in content and translation. A thorough back-translation process ensured accuracy, considering Arabic was the participants’ native language. The survey consisted of three sections. The first part involved assessing eligibility through five binary questions. The second part focused on gathering background information from participants, including demographic details such as age, residence, marital status, education level, height, weight, previous history of mammogram (MGM), and attitude towards regular SMG, comprising a total of 13 binary/multiple-choice/open-ended questions. Lastly, the third part comprised four multiple-choice questions to gauge knowledge about SMG, one binary question concerning SMG uptake response, and 20 questions (binary/open-ended) exploring reasons for refusal and the potential impact of specific suggestions to reconsider SMG; see Appendix 1for details. Prospective participants were informed about the study by their healthcare providers during primary healthcare visits. Informed consent was obtained from all participants, including those who were illiterate through oral explanations provided by trained research assistants. The questionnaire was administered face-to-face to all participants. Research assistants read the questions aloud and recorded the responses directly into the online survey system. This method ensured that all participants, regardless of literacy level, could accurately contribute to the study. De-identified data were entered into an encrypted Microsoft Excel database and stored on a password-protected computer. Participant IDs were assigned for confidentiality. Data access was restricted to delegated research team members via secure email accounts.
Statistical Analysis
Descriptive and inferential statistics were employed using SPSS version 28. Frequencies, proportions, means, and standard deviations summarized the data. The age was stratified into three groups (40–49), (50–59), and 60 to 69). The Body Mass Index (BMI) is distributed into normal weight (<25), overweight (25 to <30), and obese (≥30). The residency in Qassim was classified into two groups: central for living in the main cities and peripheral for towns and villages. The correct answer for each of the four knowledge questions scored 2; the incorrect answer is 0, and the unknown is 1, giving a total of 8. The participants were classified based on knowledge as good (7–8), intermediate (5–6), and poor (≤4). Chi-square and t-tests assessed differences in refusal based on socio-demographic characteristics. Logistic regression analysis, with crude and adjusted odds ratios (OR) and 95% confidence intervals (CI), identified factors associated with BC screening refusal (p < 0.05).
Results
Participants’ Characteristics, Backgrounds, and Knowledge About SMG
A total of 2446 participants were included in the study, and the details of eligibility screening are illustrated in the flow diagram (Figure 1). The median age of participants was 49 years (IQR: 44–56), and 51% were between the 40–49 age group. The majority were currently married individuals (91.5%), and 7.9% were widowed or divorced. Educational level diversity was evident, and 21.3% were illiterate. The employment status indicated that 18.9% of participants were employed, while 81.1% were not. Residency patterns showed that 60.3% resided in central cities and 39.7% in peripheral areas. The median weight was 73 (IQR:66–80) Kg, the median height was 157 (IQR:154–160) cm, and the median BMI was 29.2 (IQR: 26.8–32.9) Kg/m2. The distribution is as follows: normal weight 316 women (12.9%), while the majority either overweight 1011 (41.3%) or obese 1024 (42.0%). Notably, 523 (21.4%) of participants had a history of previous mammograms (range 1–6). Among those with a history of mammograms, the median age at first mammogram was 45 (IQR:42–51) years, and only 315 (12.9%) performed SMG regularly every 1–2 years.
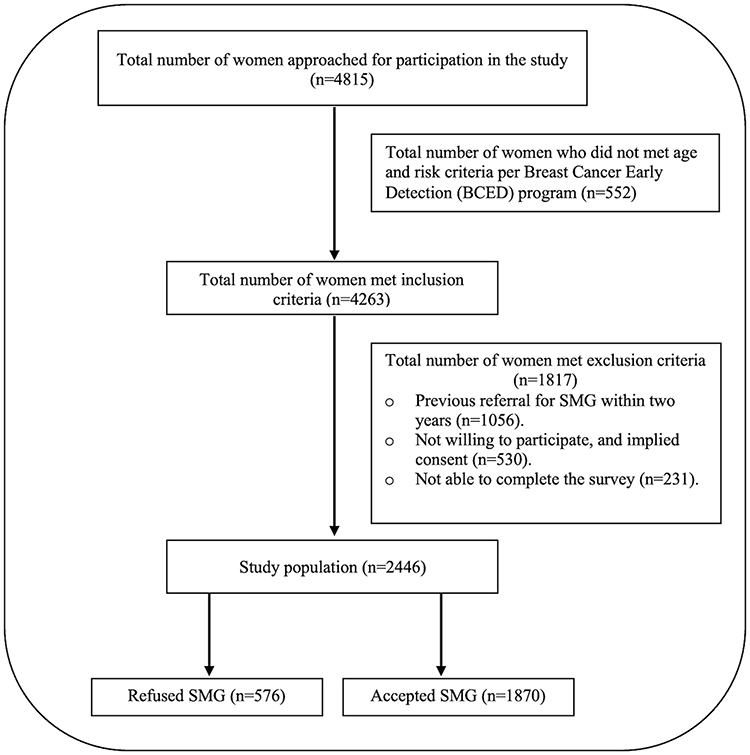 |
Figure 1 Flow chart for the study population. |
Regarding awareness regarding SMG, the majority, 89.2% (2183 women), acknowledged that SMG is considered the standard for early detection of BC. Concerning the availability of free mammogram screening programs in the region, a significant proportion, 92% (2251 women), were aware of the programs. Participants were also asked about the recommended age for women to commence mammograms. The majority, 84.1% (2060 women), correctly identified that it should be done for women 40 years and above. As for the frequency of SMG, the data revealed that 69.4% (1698 women) were familiar with the guideline recommendation for SMG every 1–2 years. Overall, 71.9% (1759 women) exhibited a good knowledge score, and only 9.7% (238 women) were categorized as having poor knowledge of SMG in Qassim.
Out of 2446, the majority of participants accepted SMG 1870 (76.5%), and 576 women (23.5%) refused the SMG. There was a statistically significant difference based on responses to SMG uptake with marital status (p=0.003), education level (p=0.01), residence (p<0.001), previous history of performing SMG (p<0.001), and following SMG regularly (p<0.001). There was a higher refusal rate in women ≥60 years (27.1%) compared to younger women (22.8%), but that was not statistically significant (p=0.2). There were no differences based on employment status (p=0.2), knowledge score (p=0.5), or BMI (p=0.77). The details of participants’ characteristics stratified by response to SMG uptake are presented in Table 1.
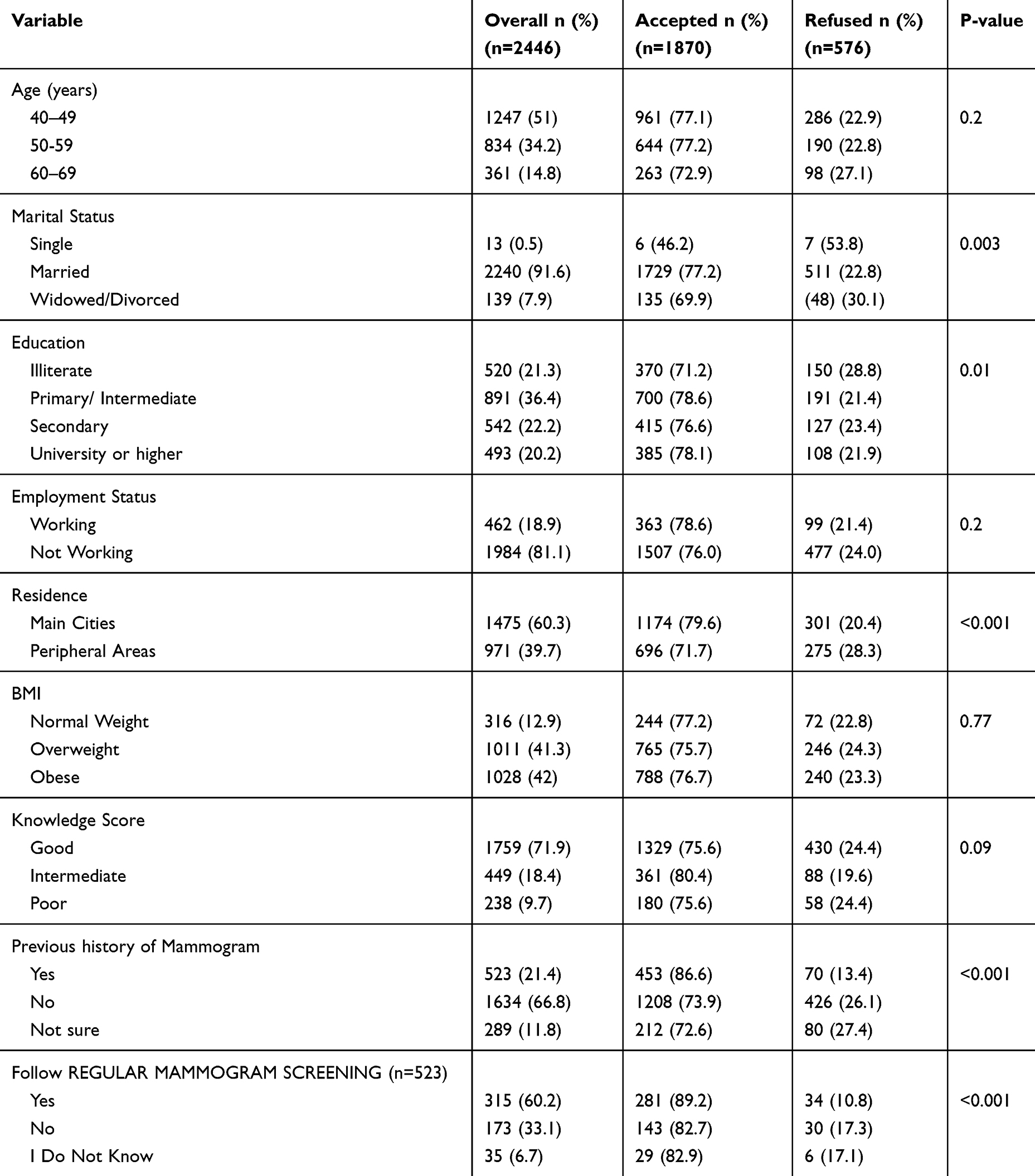 |
Table 1 Participants’ Characteristics Stratified by Response to Screening Mammogram Uptake (n=2446) |
Reasons and Factors Associated with Refusing SMG
Among the 23.5% (576 women) who refused SMG services, the primary reasons cited were a perceived lack of necessity due to the absence of a lump (74.0%). Following this, concerns regarding difficulty accessing mammogram sites (63.9%) and fear of receiving unfavorable news (55.7%). Additional significant factors included time constraints (53.3%), apprehension about radiation exposure (48.6%), and fear of mammogram-associated pain (48.4%). Furthermore, some participants expressed embarrassment (35.1%) about breast exposure, while others cited feeling too young for screening (27.8%) or religious constraints (25.0%). A smaller proportion reported concerns about hospital facilities (29.9%) or past negative experiences with mammogram screenings (19.8%). A minority also provided miscellaneous reasons in response to the open-ended question, including an inability to leave the house (2), fear of impacting pregnancy or lactation (3), feeling too old for screening (2), other meanings for fear of BC discovery (8), or geographical distance from mammogram centers (6).
Further details on these reasons are provided in Table 2.
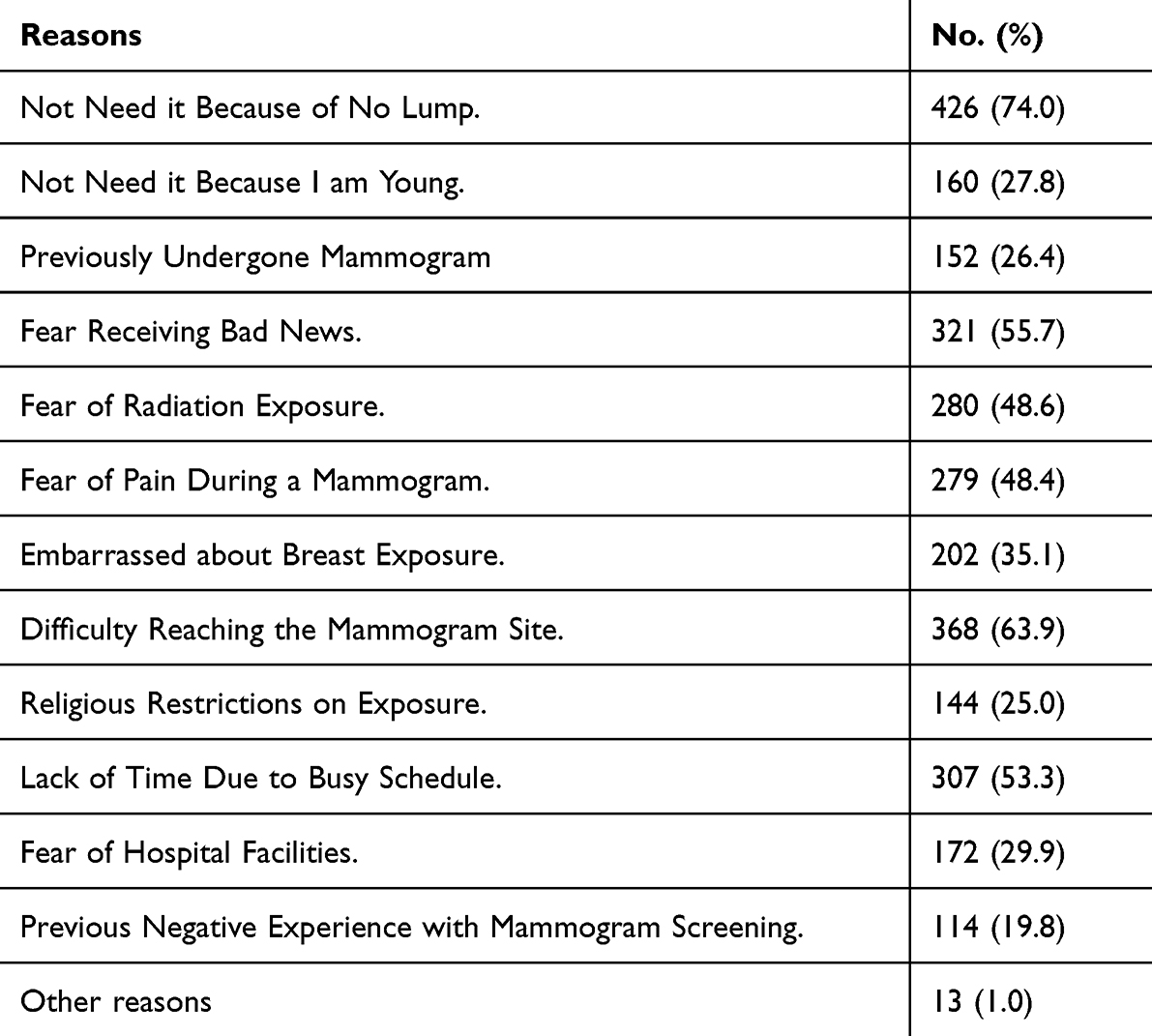 |
Table 2 The Participant’s Reasons for Refusal of Screening Mammogram (n=576) |
Multivariate analysis identified marital status, residential location, and mammogram history as independent predictors of mammogram rejection in our participants. Widowed/Divorced women had a 1.55-fold increase in the likelihood of refusing SMG compared to married women (Adjusted Odds Ratio [OR] = 1.55, p = 0.01). Women residing in peripheral areas showed approximately 1.45 times higher odds of refusal than those in central cities (Adjusted OR = 1.45, p < 0.001). Furthermore, women without prior mammograms had 2.13 times higher odds of refusal (Adjusted OR = 2.13, p < 0.001), as shown in Table 3.
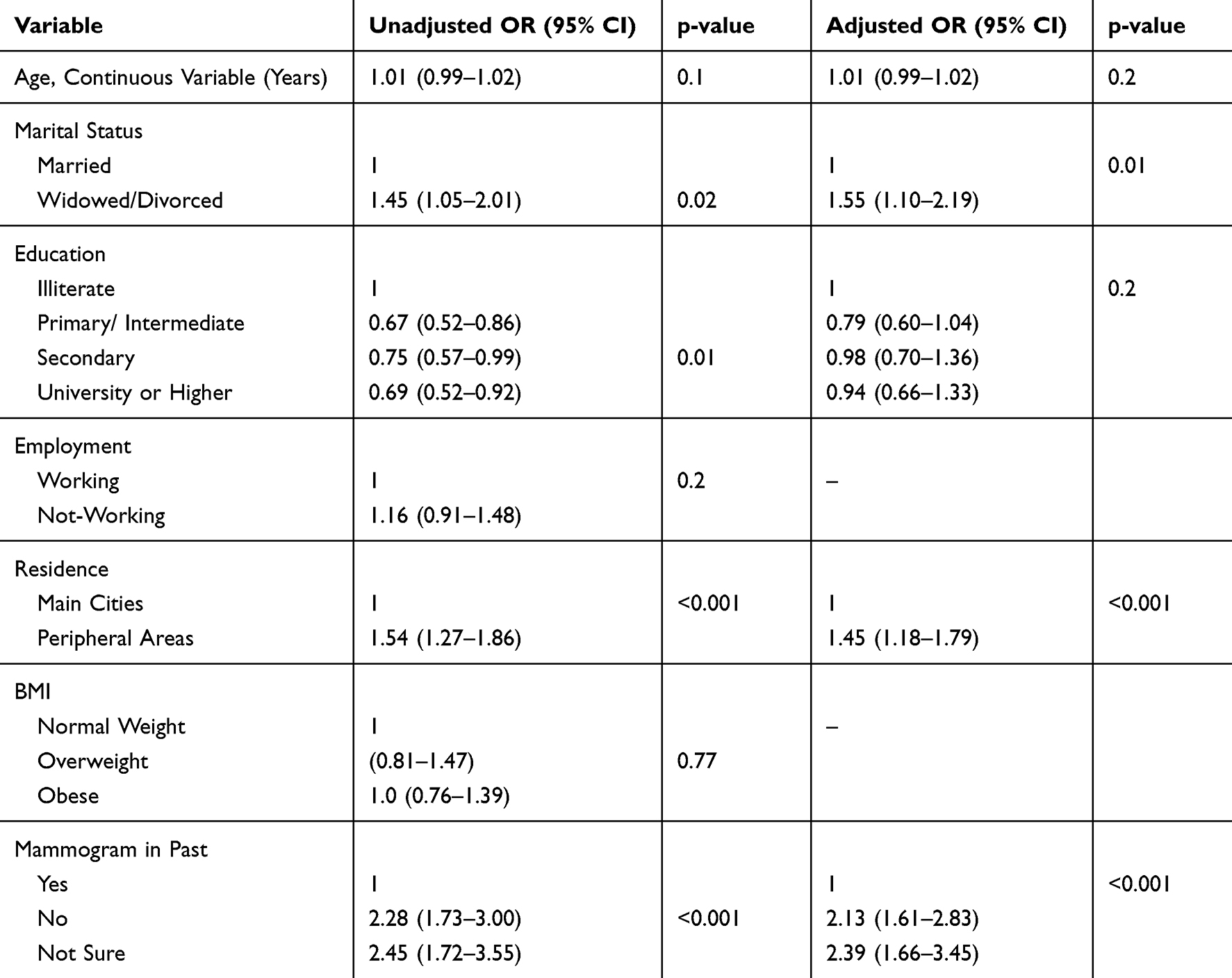 |
Table 3 Predictors of Mammogram Rejection Among Women in Qassim, Saudi Arabia |
Participants who declined SMG were surveyed regarding their willingness to reconsider in various scenarios. When offered a female healthcare examiner, 58.9% expressed agreement. Positive perceptions were observed regarding the availability of free transportation to the mammogram center, with 65.5% agreeing. Consideration of scheduling convenience revealed that 58.9% agreed with the idea of having appointments during non-working hours. Similarly, 52.4% expressed agreement with the provision of sick leave for a mammogram during working hours. Including a counseling session with a healthcare provider received favorable responses, with 53% in agreement, as shown in Table 4.
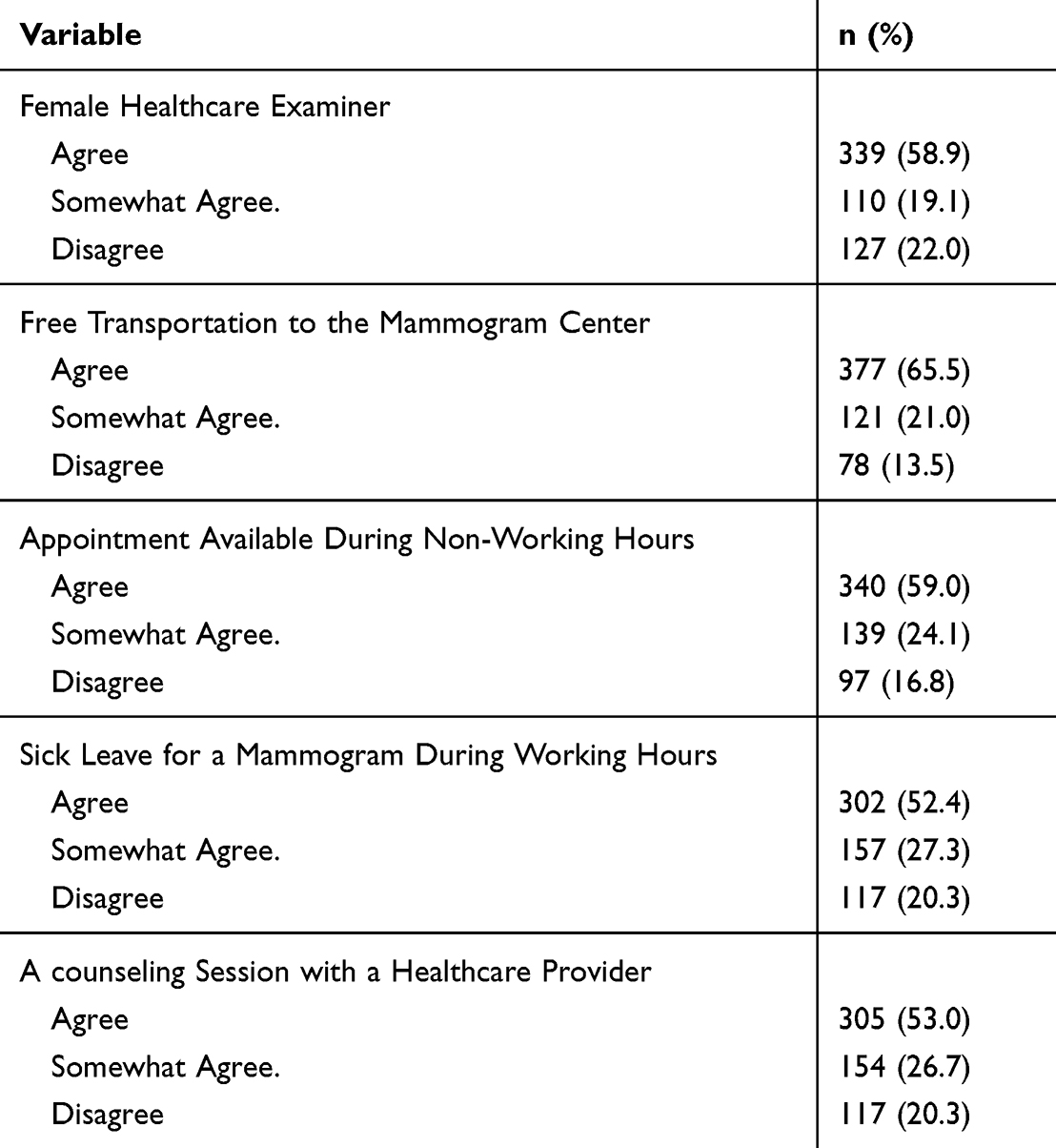 |
Table 4 Factors Influencing Reconsideration of SMG Among Refusers (n=576) |
Discussion
The insight gained from this study sheds light on the SMG refusal rate among Saudi women in the Qassim region and emphasizes factors influencing SMG uptake and developing targeted interventions. Our analysis revealed that 23.5% of eligible women declined the service. These findings highlight the necessity for targeted interventions and tailored educational campaigns to address specific barriers faced by different demographic groups. Participants’ decisions to decline SMG were primarily influenced by the absence of a lump, difficulty in accessing mammogram sites, fear of receiving bad news, time constraints, apprehensions regarding radiation exposure, and concerns about mammogram-associated pain, embarrassment, or religious constraints. Marital status, residence, and previous history of performing mammograms emerged as independent predictors of mammogram rejection among participants. Despite these challenges, the study identifies potential facilitators that could positively influence women’s willingness to reconsider screening mammography. These include the presence of a female healthcare examiner, free transportation to the mammogram center, convenient scheduling, provision of sick leave during working hours, and the inclusion of counseling sessions with healthcare providers. These results underscore the potential influence of specific facilitators on individuals’ willingness to reconsider and actively participate in screening mammography.
The demographic composition of our study sample mirrors that of our population, with a younger age group and a higher-than-average BMI, categorized as overweight or obese. Additionally, the majority were married, resided in central cities, and educated.6,9,10,16,24,27,33,34 Our study’s age representation, particularly with a significant proportion of women aged 40–49 years, supports the generalizability of our findings to similar demographic groups within the eligible screening age range. In Saudi Arabia, the median age at breast cancer diagnosis is 45.7 years, which aligns with data from other Arab countries, Asia, and the Caribbean.6,35 Research across our region, encompassing areas like Saudi Arabia, the United Arab Emirates, and Egypt, consistently reveals suboptimal utilization of screening mammography. Studies indicate that 40% to 92% of women have never undergone mammography.16,17,33,36 This underutilization contributes to a lower rate of screen-detected tumors. For example, among 2212 consecutive women diagnosed with localized disease, only 11.2% had tumors detected through screening.6 In contrast, Western countries typically report higher rates, ranging from 22% to 48%.37,38 These disparities in screening rates have significant implications for the timing of diagnosis and subsequent management strategies.
In the last decade, the Ministry of Health has implemented significant efforts through various measures such as awareness campaigns, screening programs, and the introduction of mobile clinics to enhance screening uptake. Our findings, with 23.6% of eligible women declining the service, indicate the effectiveness of national and regional, aligning with observed improvement in other countries over time.38,39 Significantly, our results suggest a comparable refusal rate to developed countries like Canada (28%) and Scotland (25%) and approaching the levels observed in Denmark (16.9%) and Australia (17%).19,39,40 This progress indicates an improvement in the acceptance and participation in SMG, which is essential for enhancing early detection and the management of BC within our regions. However, despite the majority (76.4%) accepting SMG in our study, questions remain regarding their adherence to the screening pathway, warranting further examination. Previous reports showed that among women exhibiting a positive attitude toward screening mammograms, only 30–50% underwent the procedure.9,41
A notable finding from our study is the primary reason for refusing SMG, which is the “perceived lack of necessity due to the absence of a lump” (74%). This highlights a significant misunderstanding among participants about the purpose of breast cancer screening, which is intended for asymptomatic women to detect cancer at an early stage. This finding underscores a critical gap in knowledge about breast cancer screening programs. Despite generally high knowledge scores reported in our study, the misconception that screening is unnecessary without symptoms suggests that the tool used to measure knowledge might not have captured this aspect adequately. Therefore, future research should address these issues while assessing knowledge of and attitudes toward SMG. Nonetheless, educational interventions are required to address this misunderstanding among women. Our findings indicate that educational campaigns should emphasize that breast cancer screening is crucial in the absence of symptoms, aiming to correct this prevalent misconception and improve screening uptake. Future research should incorporate comprehensive tools that better assess understanding of the asymptomatic nature of screening.
Additionally, special attention should be given to improving participation among illiterate women. Tailored educational interventions, such as visual aids, community-based programs, and verbal communication strategies, could be highly effective. Collaborating with community leaders and healthcare providers to deliver culturally appropriate and accessible information can also help bridge this gap and enhance participation rates in this vulnerable group.
However, in our study, a significant portion of participants, representing one-fourth of the sample, cited religious constraints as a primary reason for declining screening, emphasizing its substantial impact. This finding shed light on religious beliefs toward SMG. Previous research has indicated that religious beliefs, particularly among Muslim women, may influence socio-ethical, cultural, and religious perspectives on health practices related to BC screening.42–44 To address these challenges, our study advocates implementing educational initiatives to overcome these barriers.
Multivariant analysis showed that marital status, residence, and previous history of performing mammograms were independent factors in accepting mammograms, which agrees with previous studies.16,38 There was a notable trend among women from peripheral areas to decline SMG, which aligns with previous studies. Systematic reviews of 28 and 21 studies highlighted that rural populations were less inclined to undergo SMG and an increased likelihood of diagnosis at advanced stages of BC.45,46 Conversely, no difference in SMG uptake was observed based on residential locations in Scotland and Australia.19
No significant link was found between knowledge scores and refusal rates. This lack of association may stem from the fact that most participants displayed high knowledge scores, with just a small fraction (9.7%) having low scores. However, a clear correlation emerged between knowledge scores and education level. Those with higher education had significantly lower rates of poor knowledge scores compared to the illiterate group (p<0.001), consistent with previous research.16,27 Regarding refusal rates among women 60 years and older, it was higher at 27.1%, although not statistically significant (p=0.2). While education showed a higher refusal rate in univariate analysis, this association did not reach statistical significance in multivariate analysis.
With SMG accessible in all Saudi regions and provided free of charge, urgent measures are needed to enhance compliance with BC screening through intensive educational campaigns. Emphasizing the importance of screening for individuals within specific age groups and locations, irrespective of symptoms, is crucial. Additionally, addressing religious beliefs through community involvement, particularly with religious figures, is indispensable. Comprehensive strategies that target identified barriers and capitalize on potential facilitators are essential to improving SMG in the Qassim region. Collaborative efforts involving healthcare providers, community leaders, and policymakers are essential to implementing culturally sensitive and context-specific interventions. Significant strides can be made in early detection and effective management by addressing these challenges and advocating for a proactive approach to BC screening. Ultimately, this can help alleviate the burden of BC on women in the Qassim region of Saudi Arabia.
The findings of this study offer valuable insights into enhancing breast screening programs and addressing potential barriers, ultimately improving the effectiveness of BC detection and prevention efforts. However, it’s important to acknowledge a potential limitation, namely the possible lack of generalizability of the findings to the entire population. We observed that despite higher knowledge levels, there were misconceptions about breast cancer screening criteria. This could be due to the potential limitation of the tool to capture the knowledge related to prevailing misconceptions. However, the knowledge tool showed acceptable internal consistency as judged by Cronbach’s alpha (0.703). Additionally, a limitation of the study was that the sample was powered solely for the rejection rate, with no apriori sample size calculations done for factors associated with rejection. However, post-hoc calculations based on observed exposure distribution among the two groups indicated that our sample had a minimum of 95% power for observed odds ratios in the regression model. Moreover, social desirability bias is possible, where women might have responded positively despite not intending to undergo SMG. However, this would minimally impact the validity of our results, as the data collected was completely anonymized for privacy, and participants were consecutive and assured of standard care in the facility regardless of their survey responses. Despite these limitations, the study’s findings will contribute to improving breast screening initiatives and fostering more effective BC detection and prevention strategies.
Conclusion
The refusal rate for SMG among Saudi women in the Qassim region, at 23.5%, aligns closely with rates observed in developed countries. Despite this progress, significant barriers to SMG uptake persist, including logistical challenges, fear of unfavorable health news, and cultural and religious considerations. Tailored interventions targeting specific demographic groups and addressing these barriers are essential to promote a culture of proactive screening behavior and ensure equitable access to screening services for all eligible women.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Regional Research Ethics Committee of Health and Curative Programs Department, Public Health and Community Health Administration, Qassim Cluster, Qassim Province (number 607/45/1567). Participants were required to provide informed consent before participating in the study, demonstrating their understanding of the study’s objectives and expressing their voluntary agreement to participate. All methods were performed following relevant guidelines and regulations.
Acknowledgments
The Researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2024-9/1).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the Breast Cancer: Targets and Therapy to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted without commercial or financial relationships that could be construed as potential conflicts of interest.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Saudi Arabia Source: Globocan Incidence, Mortality and Prevalence by Cancer Site. Available from: https://gco.iarc.fr/today/data/factsheets/populations/682-saudi-arabia-fact-sheets.pdf.
3. Saudi Health Council, National Cancer Center, Saudi Cancer Registry, Cancer Incidence Report, Saudi Arabia 2020. Available: https://shc.gov.sa.
4. Alshamsan B. Trends of cancer incidence in Qassim region, a descriptive analysis of data from the Saudi cancer registry 2002-2016. Int J Health Sci. 2022;16(5):21–31.
5. American Cancer Society Recommendations for the Early Detection of Breast Cancer. ACS Breast Cancer Screening Guidelines. Available: https://www.cancer.org/cancer/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-The-early-detection-of-breast-cancer.html.
6. Alshamsan B, Suleman K, Agha N, et al. Association between obesity and clinicopathological profile of patients with newly diagnosed non-metastatic breast cancer in Saudi Arabia. Int J Womens Health. 2022;14:373–384. doi:10.2147/IJWH.S343558
7. Breast cancer early detection project. Ministry of Health, Saudi Arabia. Available from: https://www.moh.gov.sa/en/Ministry/Projects/breast-cancer/Pages/default.aspx.
8. Akhtar SS, Nadrah HM, Al-Habdan MA, et al. First organized screening mammography programme in Saudi Arabia: preliminary analysis of pilot round. East Mediterr Health J. 2010;16(10):1025–1031. doi:10.26719/2010.16.10.1025
9. Alotaibi AB, Alzhrani A. Barriers to mammogram screening among women in Taif city, Saudi Arabia. IAJPS. 2021;08:216–225. doi:10.5281/zenodo.4642367
10. Abdel-Aziz SB, Amin TT, Al-Gadeeb MB, et al. Perceived barriers to breast cancer screening among Saudi women at primary care setting. Asian Pac J Cancer Prev. 2017;18(9):2409–2417. doi:10.22034/APJCP.2017.18.9.2409
11. Alshahrani M, Alhammam SYM, Al Munyif HAS, et al. Knowledge, attitudes, and practices of breast cancer screening methods among female patients in primary healthcare centers in Najran, Saudi Arabia. J Cancer Educ. 2019;34(6):1167–1172. doi:10.1007/s13187-018-1423-8
12. Alshahrani MS, Sultan SA, Alhammam SY, et al. Assessment and practice of female health care workers regarding risk of breast cancer and screening methods cross-sectional study, Saudi Arabia. Open J Obstet Gynecol. 2020;10(02):201–212. doi:10.4236/ojog.2020.1020017
13. Mahfouz AA, Hassanein MH, Nahar S, et al. Breast cancer knowledge and related behaviors among women in Abha City, southwestern Saudi Arabia. J Cancer Educ. 2013;28(3):516–520. doi:10.1007/s13187-013-0495-8
14. Al-Zalabani AH, Alharbi KD, Fallatah NI, Alqabshawi RI, Al-Zalabani AA, Alghamdi SM. Breast cancer knowledge and screening practice and barriers among women in Madinah, Saudi Arabia. J Cancer Educ. 2018;33(1):201–207. doi:10.1007/s13187-016-1057-7
15. Rehmani R, Elzubair AG, Al Maani M, et al. Population-based health survey in eastern region of Saudi Arabia. East Mediterr Health J. 2013;19(5):417–425. doi:10.26719/2013.19.5.417
16. Al-Wassia RK, Farsi NJ, Merdad LA, Hagi SK. Patterns, knowledge, and barriers of mammography use among women in Saudi Arabia. Saudi Med J. 2017;38(9):913–921. doi:10.15537/smj.2017.9.20842
17. El Bcheraoui C, Basulaiman M, Wilson S, et al. Breast cancer screening in Saudi Arabia: free but almost no takers [published correction appears in PLoS One. 2015;10(4):e0124850]. PLoS One. 2015;10(3):e0119051. doi:10.1371/journal.pone.0119051
18. AlSaleh KA. Efficacy of breast cancer screening program in Kingdom of Saudi Arabia. Saudi Med J. 2022;43(4):428–430. doi:10.15537/smj.2022.43.4.20210823
19. Leung J, Macleod C, McLaughlin D, et al. Screening mammography uptake within Australia and Scotland in rural and urban populations. Prev Med Rep. 2015;2:559–562. doi:10.1016/j.pmedr.2015.06.014
20. Sabatino SA, Coates RJ, Uhler RJ, Breen N, Tangka F, Shaw KM. Disparities in mammography use among US women aged 40-64 years, by race, ethnicity, income, and health insurance status, 1993 and 2005. Med Care. 2008;46(7):692–700. doi:10.1097/MLR.0b013e31817893b1
21. Kim E, Moy L, Gao Y, Hartwell CA, Babb JS, Heller SL. City patterns of screening mammography uptake and disparity across the United States. Radiology. 2019;293(1):151–157. doi:10.1148/radiol.2019190647
22. Wilkinson AN, Billette JM, Ellison LF, Killip MA, Islam N, Seely JM. The impact of organised screening programs on breast cancer stage at diagnosis for Canadian Women Aged 40-49 and 50-59. Curr Oncol. 2022;29(8):5627–5643. doi:10.3390/curroncol29080444
23. Al-Ghadeer B, Al-Ghadeer A, Aldoughan S. Breast cancer knowledge and barriers to screening among women in Al-Ahsa, Saudi Arabia. IJMDC. 2021;5(1):106–112.doi:10.24911/IJMDC.51–1605438509.
24. Aljohani A, Saib I, Noorelahi M. Women’s performance of breast cancer screening (breast self-examination, clinical breast exam and mammography). J Health Educ Res Dev. 2016;4(04):16–27. doi:10.4172/2380-5439.1000202
25. Alenezi AM, Thirunavukkarasu A, Wani FA, et al. Female healthcare workers’ knowledge, attitude towards breast cancer, and perceived barriers towards mammogram screening: a multicenter study in North Saudi Arabia. Curr Oncol. 2022;29(6):4300–4314. doi:10.3390/curroncol29060344
26. Al-Mulhim FA. Knowledge and attitude towards screening mammography among 400 women in the eastern province of Saudi Arabia. J Family Community Med. 2001;8(3):73–78. doi:10.4103/2230-8229.98066
27. Abdel-Salam DM, Mohamed RA, Alyousef HY, et al. Perceived barriers and awareness of mammography screening among Saudi women attending primary health centers. Risk Manag Health Policy. 2020;13:2553–2561. doi:10.2147/RMHP.S277375
28. AL-Mulhim F, Bakr R, Almedallah D, Alkaltham N, Alotaibi A, Alnoaim S. Screening mammography and breast self-examination: attitudes and practices of women in the eastern province of Saudi Arabia. Saudi J Health Sci. 2018;7(2):89–100. doi:10.4103/sjhs.sjhs_4_18
29. Geography glance, Qassim Municipality. Available from: https://www.qassim.gov.sa.
30. General Authority for Statistics. Population estimates. Available from: stats.gov.sa/en/43.
31. The Manual for Breast Cancer Early Detection Program, Ministry of Health, Saudi Arabia. Online. Available from: https://www.moh.gov.sa/Ministry/About/HealthPolicies/011.pdf.
32. Champion VL. Revised susceptibility, benefits, and barriers scale for mammography screening. Res Nurs Health. 1999;22(4):341–348. doi:10.1002/(sici)1098-240x(199908)22:4<341::aid-nur8>3.0.co;2-p
33. Elobaid YE, Aw TC, Grivna M, Nagelkerke N. Breast cancer screening awareness, knowledge, and practice among Arab women in the United Arab Emirates: a cross-sectional survey. PLoS One. 2014;9(9):e105783. doi:10.1371/journal.pone.0105783
34. Alanazi MF, Thirunavukkarasu A, Alrowily M, et al. A cross-sectional evaluation of knowledge about breast cancer and perceived barriers to the uptake of mammogram screening among northern Saudi women: a population-based study. Breast Cancer. 2023;15:451–460. doi:10.2147/BCTT.S414635
35. Najjar H, Easson A. Age at diagnosis of breast cancer in Arab nations. Int J Surg. 2010;8(6):448–452. doi:10.1016/j.ijsu.2010.05.012
36. Salama BM M. Factors affecting mammography screening utilization among educated women in Al Beheira governorate. Egypt Indian J Community Med. 2020;45(4):522–525. doi:10.4103/ijcm.IJCM_41_20
37. McPherson CP, Swenson KK, Jolitz G, Murray CL. Survival of women ages 40-49 years with breast carcinoma according to method of detection. Cancer. 1997;79(10):1923–1932. doi:10.1002/(sici)1097-0142(19970515)79:10<1923::aid-cncr13>3.0.co;2-x
38. Jiang L, Gilbert J, Langley H, Moineddin R, Groome PA. Breast cancer detection method, diagnostic interval and use of specialized diagnostic assessment units across Ontario, Canada. cancer du sein: méthode de détection, intervalle diagnostique et recours aux unités d’évaluation diagnostique spécialisées en Ontario (Canada). Health Promot Chronic Dis Prev Can. 2018;38(10):358–367. doi:10.24095/hpcdp.38.10.02
39. Shields M, Wilkins K. An update on mammography use in Canada. Health Rep. 2009;20(3):7–19.
40. Pett L, Hollenberg B, Mahoney J, et al. Participation and adherence to mammography screening in the capital region of Denmark: the importance of age over time. PLoS One. 2023;18(1):e0280790. doi:10.1371/journal.pone.0280790
41. Alshammari SA, Alhazmi AM, Alenazi HA, Alshammari HS, Alshahrani AM. Mammography uptake among the female staff of King Saud university. J Family Med Prim Care. 2020;9(1):221–228. doi:10.4103/jfmpc.jfmpc_706_19
42. Azaiza F, Cohen M. Health beliefs and rates of breast cancer screening among Arab women. J Womens Health. 2006;15(5):520–530. doi:10.1089/jwh.2006.15.520
43. Moey SF, Sowtali SN, Mohamad Ismail MF, Hashi AA, Mohd Azharuddin NS, Che Mohamed N. Cultural, religious and socio-ethical misconceptions among Muslim women towards breast cancer screening: a systematic review. Asian Pac J Cancer Prev. 2022;23(12):3971–3982. doi:10.31557/APJCP.2022.23.12.3971
44. Donnelly TT, Khater AH, Al-Bader SB, et al. Arab women’s breast cancer screening practices: a literature review. Asian Pac J Cancer Prev. 2013;14(8):4519–4528. doi:10.7314/apjcp.2013.14.8.4519
45. Nguyen-Pham S, Leung J, McLaughlin D. Disparities in breast cancer stage at diagnosis in urban and rural adult women: a systematic review and meta-analysis. Ann Epidemiol. 2014;24(3):228–235. doi:10.1016/j.annepidem.2013.12.002
46. Leung J, McKenzie S, Martin J, McLaughlin D. Effect of rurality on screening for breast cancer: a systematic review and meta-analysis comparing mammography. Rural Remote Health. 2014;14(2):2730. doi:10.22605/RRH2730
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.