")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Khat Chewing and Type 2 Diabetes Mellitus
Authors Badedi M , Darraj H , Hummadi A, Najmi A, Solan Y, Zakry I, Khawaji A, Zaylai S, Rajeh N, Alhafaf H, Hakami W, Bakkari A, Kriry M, Dagreri A, Haddad E
Received 1 December 2019
Accepted for publication 17 January 2020
Published 10 February 2020 Volume 2020:13 Pages 307—312
DOI https://doi.org/10.2147/DMSO.S240680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Antonio Brunetti
Mohammed Badedi,1 Hussain Darraj,1 Abdulrahman Hummadi,1 Abdullah Najmi,2 Yahiya Solan,1 Ibrahim Zakry,1 Abdullah Khawaji,1 Sayedah Zaylai,1 Norah Rajeh,1 Hassan Alhafaf,1 Wali Hakami,1 Awaji Bakkari,1 Maryam Kriry,1 Abdulraheem Dagreri,1 Ebrahim Haddad1
1Jazan Diabetes and Endocrine Center, Ministry of Health, Jazan, Saudi Arabia; 2Jazan Health Affairs, Ministry of Health, Jazan, Saudi Arabia
Correspondence: Mohammed Badedi
Jazan Diabetes Center, Ministry of Health, Saudi Arabia, PO Box 604, Abu Arish, Jazan 45911, Saudi Arabia
Tel +966 559154136
Email [email protected]
Objective: Knowledge about the effects of khat chewing on type 2 diabetes mellitus (T2DM) development and glycemic control is very sparse. Emerging data suggest that khat chewing may increase the risk of T2DM occurrence. Therefore, this study aimed to measure the prevalence of khat chewing in Saudi people with T2DM in Jazan, Saudi Arabia and to determine the association of khat chewing with T2DM development and glycemic control in T2DM.
Methods: This is an analytical, cross-sectional study that included 472 Saudi participants selected randomly from primary healthcare centers in Jazan, Saudi Arabia. A chi-square test and logistic regression were performed in the statistical analysis.
Results: The prevalence of khat chewing in Saudi patients with T2DM in Jazan was 29.3%. After adjusting for covariates, khat chewing was significantly associated with T2DM (odds ratio 3.5), indicating that khat chewers had a more than three times higher risk of developing T2DM than those who do not chew khat. However, there was no association between khat chewing and glycemic control in T2DM.
Conclusion: Khat chewing was highly prevalent in Saudi people with T2DM in Jazan, Saudi Arabia. There was an association between khat chewing and the development of T2DM. Establishing the causal association of khat chewing with T2DM development and glycemic control and clarifying the biological role of khat in T2DM are important aims for future studies.
Keywords: type 2 diabetes mellitus, catha edulis, khat chewing
Introduction
Diabetes mellitus is a metabolic disorder characterized by chronically high levels of glucose in the blood (known as hyperglycemia) due to insulin deficiency, resistance or both.1 Diabetes mellitus may lead to serious complications that increase morbidity and mortality.2 In Saudi Arabia, the prevalence of type 2 diabetes mellitus (T2DM) was 18.3% and becomes a major health concern.3
Khat (also known as catha edulis) is an amphetamine-like stimulant in the form of plant leaves that are chewed for euphoric effects.4 Khat contains psychoactive substances, cathinone and cathine, which have a stimulating effect on the sympathetic nervous system and give the chewer a temporary sensation of activeness and happiness,5 mood disturbance and anxiety.6 Khat is commonly abused by Ethiopian and Somali people in East Africa and Yemeni people in the southern Arabian Peninsula.7 With the recent globalization, African and Arabian immigrants have spread khat chewing to Europe,8,9 Australia10,11 and the United States.12 The World Health Organization (WHO) categorized khat as an illegal drug and indicated that its abuse may cause a range of health problems.13 In Jazan, Saudi Arabia, about 33.2% of people chew khat as a habit because the Jazan region borders Yemen to the south, which is considered the main producer of khat to Jazan.14
There is growing evidence of the effect of khat chewing on T2DM and glycemic control.15–19 However, the role of khat chewing in T2DM is not fully understood. Up to our knowledge, very few published papers have tried to draw a conclusion about khat chewing and it effect on T2DM and glycemic control. Thus, the aim of this study was to measure the prevalence of khat chewing in Saudi patients with T2DM in Jazan and to investigate the association of khat chewing with the risk of T2DM occurrence and glycemic control.
Methodology
Study Design and Sample Size
Jazan is located in the southwest corner of Saudi Arabia with a predominantly homogenous population that shares similar ethnic and socioeconomic characteristics. In this study, we applied an analytical, cross-sectional design on Saudi participants recruited randomely from primary healthcare (PHC) centers in Jazan (Figure 1).
The sample size was calculated using the Epi Info software program20 with the following parameters: confidence interval, 95%; alpha, 0.5. The expected frequency of khat chewing was obtained from a previous study conducted in Jazan, Saudi Arabia.14 The computed sample size was 383, but 50% (191 subjects) were added to the total calculated sample size for non-respondents. The current study successfully recruited 472 out of the 574 selected participants. About 68 subjects (11.8%) did not meet the inclusion criteria, 22 (3.8%) did not respond and 12 (2.1%) refused to participate in the current study (Figure 1).
Inclusion and Exclusion Criteria
Saudi patients with T2DM who were older than 18 years of age were included. Patients with type 1 diabetes mellitus and gestational diabetes were excluded.
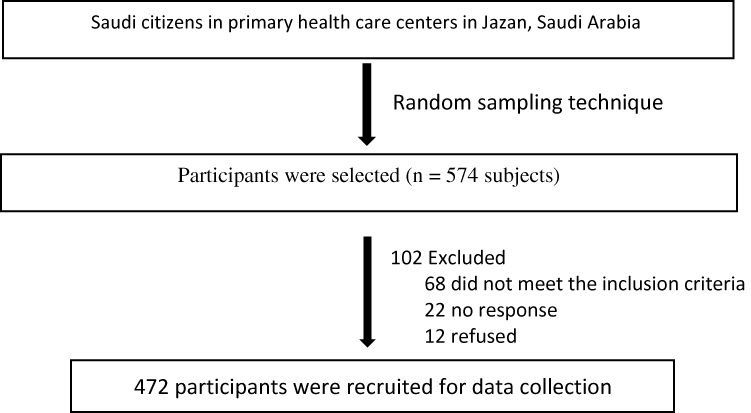 |
Figure 1 Participant enrolment in the current study. |
Covariates and Data Collection
The risk factors (covariates) that were shown in the literature to be associated with T2DM development were accounted in this study. Sociodemographic data, anthropometrics and laboratory measurements were gathered from the participants’ medical records at the diagnosis date of T2DM, including age, sex, body mass index (BMI), waist circumference and glycated hemoglobin (A1C). Additionally, face-to-face interviews with the participants were held and they were asked about history of diabetes in the family, khat chewing, past history of gestational diabetes and physical activity before the diagnosis date of T2DM.
Following the WHO’s guidelines,21 BMI was calculated as weight in kilograms divided by the square of the person’s height in meters. BMI was categorized as not obese if the score was <30 and obese if ≥30. T2DM was diagnosed following the American Diabetes Association’s guidelines.22 A1C ≥7% was categorized as poor glycemic control, while A1C <7% was good glycemic control.23 Waist circumference was measured and classified as obese if ≥94 cm for males and ≥80 cm for females, following the Arabian-specific waist circumference.24 Physical activity of less than 150 mins per week was categorized as physically inactive, following the American Diabetes Association’s guidelines.25
Ethical Consideration
The Jazan Hospital Institutional Review Board (reference number: H-10-Z-068)26 granted ethical approval (No. 1851) for the study, which also complied with the Helsinki Declaration. Written informed consent was obtained from all the participants before enrolment.
Statistical Analysis
Data entry and analysis were performed using Statistical Package for the Social Sciences software version 24.27 The data were coded with anonymous identification numbers in order to guarantee the privacy of the participants. The continuous variables were described by means and standard deviation (SD) and the categorical variables by percentages and frequencies. A chi-square test for independence was used to assess the associations among the categorical variables. Binary logistic regression was used to explore the predictors of T2DM including the significant variables in univariate regression. The assumptions of the binary logistic regression were checked for the presence of outliers and multicollinearity (high inter-correlations among independent variables). In other way in the analysis, an independent t-test was also performed to test for any mean differences between the studied groups. P values <0.05 were considered to be statistically significant.
Results
The current study recruited 472 participants who were categorized into two groups: participants with T2DM and participants without T2DM (Table 1). The participants’ sociodemographic characteristics and their associations are presented in Table 1 using a chi-square test for independence.
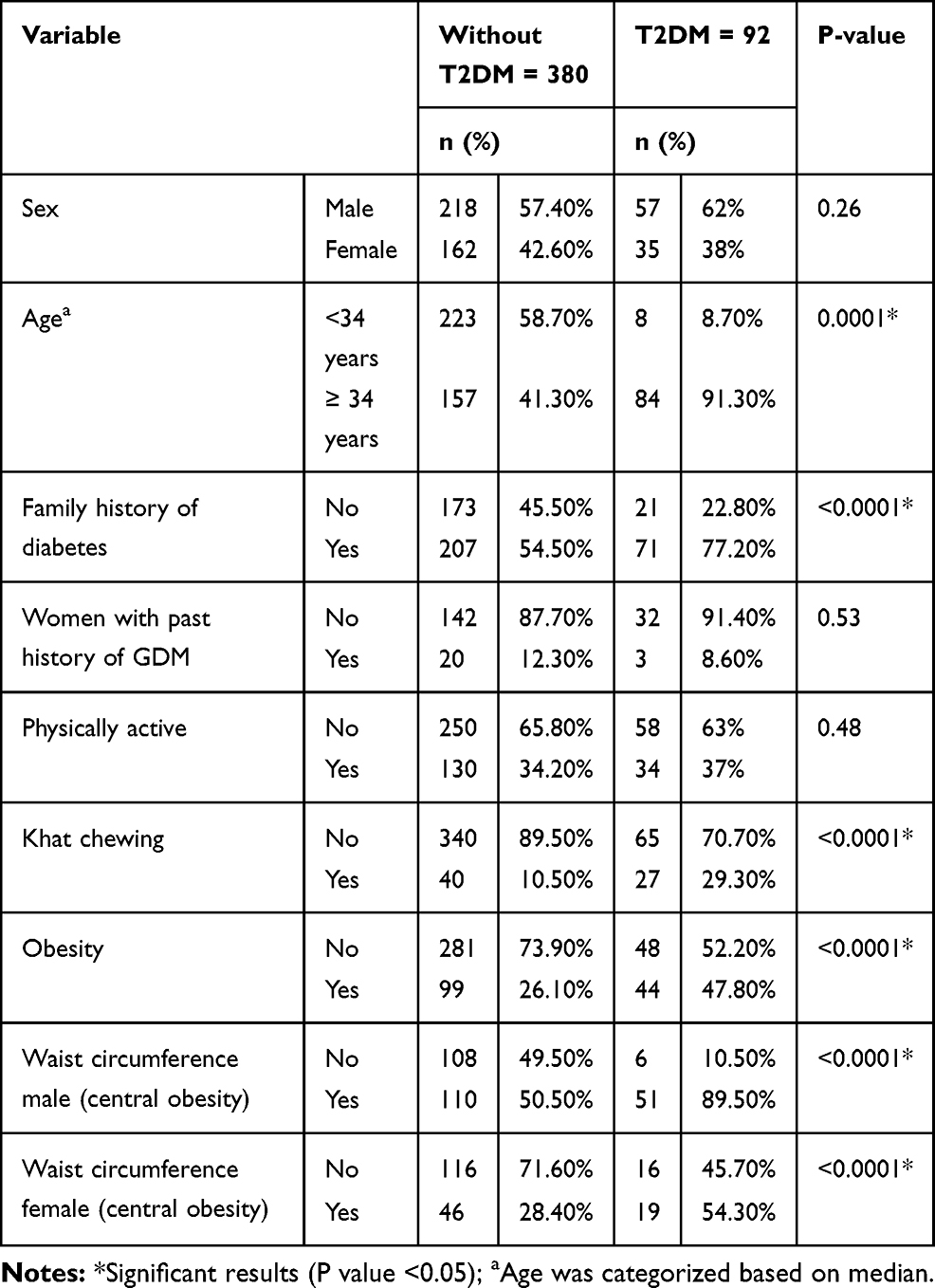 |
Table 1 Sociodemographic Characteristics and Chi-Square Test for Independence Assessed the Association Among Categorical Variables |
The Prevalence of Type 2 Diabetes Mellitus and Associated Factors
The prevalence of T2DM in the studied population was 17.6%. The mean age of non-diabetic participants was 32.1 years ± 12.9 (range 11–89 years), and the mean age of participants with T2DM was 49.7 years ± 11.5, ranging from 31 to 80 years. Age ≥34 years, family history of diabetes, khat chewing, obesity and central obesity are significantly associated with T2DM (Table 1).
Type 2 Diabetes Mellitus and Khat Chewing
The prevalence of khat chewing was 29.3% in patients with T2DM in the studied population. Most of the khat chewers had approximately similar dose and duration of khat chewing. There was a significant association between khat chewing and T2DM (Table 1). After adjusting for covariates (Table 2), khat chewer participants were more likely to have T2DM (odds ratio (OR) = 3.5), which indicated that participants with T2DM who chewed khat had approximately a more than three times greater risk than non-diabetic participants for T2DM development.
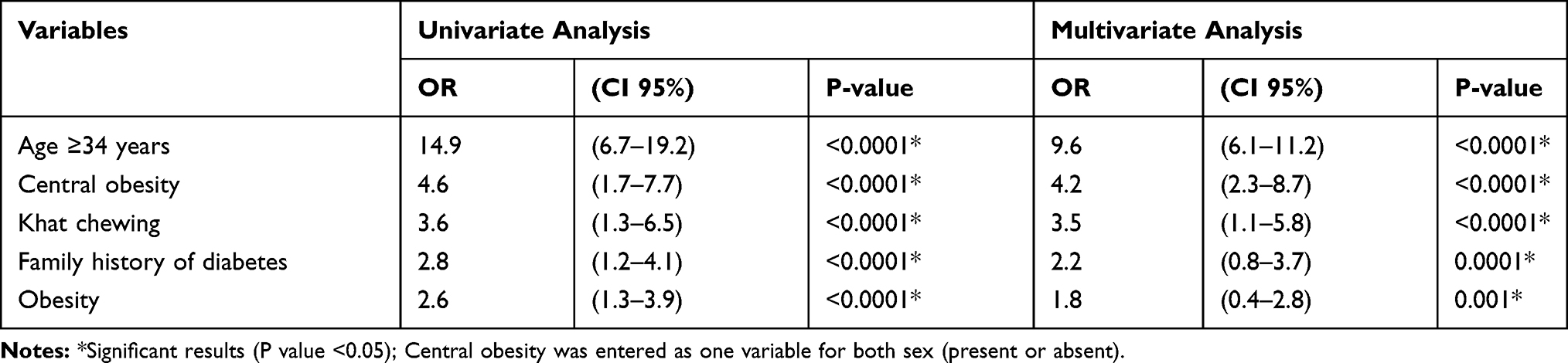 |
Table 2 Predictors of Diabetic Mellitus Development in Multivariate Binary Logistic Regression |
Khat Chewing and Glycemic Control
The prevalence of poor glycemic control was 71% in participants with T2DM in the studied population. Medication adherence was accounted, and the majority of participants were adherent to medication regimen (98.3%). About 83% of khat chewers reported that they take sugary drinks during khat chewing. There was no statistically significant association between khat chewing and glycemic control in the result of the chi-square test. For another analysis, an independent t-test was also performed to compare the A1C mean difference between participants with T2DM who were khat chewers and those who were non-khat chewers. The results also revealed that there was no significant difference in mean A1C for khat chewers (8.8 ±2.3) and non-khat chewers (8.6 ±1.9) P = 0.68.
Discussion
Type 2 Diabetes Mellitus and Its Associated Factors
T2DM is prevalent in Jazan, Saudi Arabia. In 2015, Bani28 reported that the prevalence of T2DM was 12.3% in Jazan. However, the current study estimated the prevalence of T2DM in Jazan to be 17.6%, which indicates that the prevalence of T2DM has increased dramatically in Jazan. We focused on T2DM in this study, as it is the most common type of diabetes mellitus in Jazan28 and is associated with preventable risk factors. The study revealed that there are several potential factors associated with T2DM development. Subjects with T2DM in this study were older than 34 years, which reflects that this could be due to insulin sensitivity decreasing with age.29 Family history of diabetes, central obesity and obesity were also significant predictors of T2DM, as is well established in previous studies.30–32
Type 2 Diabetes Mellitus and Khat Chewing
To our knowledge, this study is the first study in Saudi Arabia that assessed the prevalence of khat chewing in patients with T2DM and its association with T2DM. Thus, the current study focused on khat chewing as an interesting outcome. Our study findings revealed that khat chewing was prevalent (29.3%) and significantly associated with T2DM of Saudi participants. Khat chewers had more risk of developing T2DM than those who do not chew khat. These findings are consistent with that reported by other studies.16,33 A systemic review and meta-analysis study included 25 studies from 1976 to 2016, its results suggested that khat is predisposing factor contributing to the development of T2DM.33 Moreover, an experimental study in Malaysia suggested that the cytotoxic effect of khat induced diabetes mellitus through the destruction of pancreatic β-cells and changing the structures of the islets of Langerhans.16 However, the effect of khat chewing on the risk of T2DM development has not yet been elucidated. Further studies are needed to clarify the effect of khat and its chemical substances on pancreatic cells.
Khat and Glycemic Control
In the present study, the prevalence of poor glycemic control in patients with T2DM was 71%. This percentage is not far from what was found in a previous study about the poor glycemic control in T2DM that was conducted in Jazan.34,35 The current study finding also revealed that there was no significant association between khat chewing and glycemic control. This result was supported by other studies that reported similar findings.16,19,35 A systemic review and meta-analysis study included 25 studies, its results also show that khat had no effect in reducing blood glucose levels.35 Another experimental study in Malaysia also showed no association between khat chewing and glycemic control.16 Similarly, a study was conducted in Somalia reported that khat had no influence on blood glucose levels.19 However, two studies carried out in Yemen found that khat chewing increased the blood glucose levels in patients with T2DM.15,18
Study Limitation
The current study was an analytical, cross-sectional study. Establishing the causal association of khat chewing with T2DM development and glycemic control and clarifying the biological role of khat in T2DM are important aims for future studies. Furthermore, the dose and duration of khat chewing were difficult to be accounted precisely, however, most of the khat chewers had approximately similar dose and duration of khat chewing.
Conclusion
Khat chewing is highly prevalent in Saudi people with T2DM in Jazan, Saudi Arabia. There is an association between khat chewing and the development of T2DM. Khat chewers have a more than three times higher risk of developing T2DM than those who do not chew khat. Furthermore, khat chewing is not associated with glycemic control.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, [Mohammed Badedi].
Acknowledgments
We would like to express our gratitude to the team who helped us in completing this research. To begin with, we would like to thank Jazan Diabetes & Endocrine Center staff; endocrinologists, family and community medicine consultants, technicians in the registry department for their help. Finally, we would like to thank all participants for their response and cooperation.
Disclosure
The authors report no conflict of interests in this work.
References
1. World Health Organization (WHO). Definition, diagnosis and classification of diabetes mellitus and its complications. WHO/NCD/NCS/99.2 Geneva: WHO. Report number: 1, 1999.
2. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–853. doi:10.1016/S0140-6736(98)07019-6
3. International Diabetes Federation. IDF Diabetes Atlas.
4. Kalix P, Khan I. Khat: an amphetamine-like plant material. Bull World Health Organ. 1984;62(5):681–686.
5. Brenneisen R, Fisch HU, Koelbing U, Geisshusler S, Kalix P. Amphetamine-like effects in humans of the khat alkaloid cathinone. Br J Clin Pharmacol. 1990;30(6):825–828. doi:10.1111/bcp.1990.30.issue-6
6. Hassan NA, Gunaid AA, El-Khally FM, Murray-Lyon IM. The effect of chewing Khat leaves on human mood. Saudi Med J. 2002;23(7):850–853.
7. Sheikh KA, El-Setouhy M, Yagoub U, Alsanosy R, Ahmed Z. Khat chewing and health related quality of life: cross-sectional study in Jazan region, Kingdom of Saudi Arabia. Health Qual Life Outcomes. 2014;12:44. doi:10.1186/1477-7525-12-44
8. Klein A. Khat in the neighbourhood–local government responses to khat use in a London community. Subst Use Misuse. 2008;43:819–831. doi:10.1080/10826080701738976
9. Osman FA, Soderback M. Perceptions of the use of khat among Somali immigrants living in Swedish society. Scand J Public Health. 2011;39:212–219. doi:10.1177/1403494810384908
10. Stefan J, Mathew B. Khat chewing: an emerging drug concern in Australia? Aust N Z J Psychiatry. 2005;39:842–843.
11. Douglas H, Boyle M, Lintzeris N. The health impacts of khat: a qualitative study among Somali-Australians. Med J Aust. 2011;195:666–669. doi:10.5694/mja2.2011.195.issue-11-12
12. Kroll J, Yusuf AI, Fujiwara K. Psychoses, PTSD, and depression in Somali refugees in Minnesota. Soc Psychiatry Psychiatr Epidemiol. 2011;46:481–493. doi:10.1007/s00127-010-0216-0
13. El-Menyar A, Mekkodathil A, Al-Thani H, Al-Motarreb A. Khat use: history and heart failure. Oman Med J. 2015;30(2):77–82. doi:10.5001/omj.2015.18
14. Mahfouz M, Rahim B, Solan Y, Makeen A, Alsanosy R, Mazza M. Khat chewing habits in the population of the Jazan Region, Saudi Arabia: prevalence and associated factors. PLoS One. 2015;10(8):e0134545. doi:10.1371/journal.pone.0134545
15. Al-Sharafi BA, Gunaid AA. Effect of habitual khat chewing on glycemic control, body mass index, and age at diagnosis of diabetes in patients with type 2 diabetes mellitus in yemen. Clin Med Insights Endocrinol Diabetes. 2015;8:47–53. doi:10.4137/CMED.S26045
16. Alsalahi A, Alshawsh MA, Chik Z, Mohamed Z. Effect of Catha edulis (khat) on pancreatic functions in streptozotocin-induced diabetes in male Sprague-Dawley rats. Exp Anim. 2018;67(4):517–526.
17. Ramadan M, Abudl-Khair F, Labib S. Effects of Catha edulis (khat) on glucose tolerance in diabetes. Dirrassat Yamanyyah. 1979;3:15–23.
18. Saif-Ali RAl-Qirbi A, Al-Geiry A, AL-Habori M. Effect of Catha edulis on plasma glucose and C-peptide in both type 2 diabetics and non-diabetics. J Ethnopharmacol. 2003;86(1):45–49.
19. Elmi A. Khat and blood glucose levels in man. J Ethnopharmacol. 1983;8:331–334. doi:10.1016/0378-8741(83)90071-5
20. Dean A, Arner T, Sunki G, et al. Epi Info Program for Public Health Professionals. Atlanta: CDC; 2011.
21. World Health Organization (WHO). Physical status: the use and interpretation of anthropometry: report of a WHO expert committee. Technical report series 854. Geneva: WHO; 1995.
22. American Diabetes Association (ADA). Introduction: standards of medical care in diabetes 2019. Diabetes Care. 2019;42(1):61–66. doi:10.2337/dc19-S006
23. American Diabetes Association (ADA). Introduction: standards of medical care in diabetes 2019. Diabetes Care. 2019;42(1):104. doi:10.2337/dc18-2581
24. Diabetes Canada. Gender and Ethnic-Specific Waist Circumferences. Canada; 2018.
25. American Diabetes Association (ADA). Introduction: standards of medical care in diabetes 2019. Diabetes Care. 2019;42(1):30. doi:10.2337/dc18-2581
26. Jazan Hospital IRB. National committee of bio ethics. King Abdulaziz City for Science & Technology (KACST): H-10-Z-068.
27. BM Corp. IBM SPSS Statistics for Windows. NY: IBM Corp; 2012.
28. Bani I. Prevalence, knowledge, attitude and practices of diabetes mellitus among Jazan population, Kingdom of Saudi Arabia (KSA). JDM. 2015;5(2):115–122. doi:10.4236/jdm.2015.52014
29. Evans J, Goldfine I. Aging and insulin resistance: just say iNOS. Diabetes. 2013;62(2):346–348. doi:10.2337/db12-1239
30. Scott R, Langenberg C, Sharp S, et al. The link between family history and risk of type 2 diabetes is not explained by anthropometric, lifestyle or genetic risk factors: the EPIC-InterAct study. Diabetologia. 2013;56(1):60–69.
31. Huang T, Qi Q, Zheng Y, et al. Genetic predisposition to central obesity and risk of type 2 diabetes: two independent cohort studies. Diabetes Care. 2015;38(7):1306–1311. doi:10.2337/dc14-3084
32. Al-Goblan A, Al-Alfi M, Khan M. Mechanism linking diabetes mellitus and obesity. Diabetes Metab Syndr Obes. 2014;7:587–591. doi:10.2147/DMSO.S67400
33. Alsalahi A, Alshawsh M, Mohamed R, et al. Conflicting reports on the role of the glycemic effect of Catha edulis (Khat): A systematic review and meta-analysis. J Ethnopharmacol. 2016;20;186:30–43.
34. Badedi M, Solan Y, Darraj H, et al. Factors associated with long-term control of type 2 diabetes mellitus. J Diabetes Res. 2016;2016:1–8. Article ID 2109542: 8. doi:10.1155/2016/2109542
35. Darraj H, Badedi M, Poore K, et al. Vitamin D deficiency and glycemic control among patients with type 2 diabetes mellitus in Jazan City, Saudi Arabia. Diabetes Metab Syndr Obes. 2019;12:853–862. doi:10.2147/DMSO.S203700
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.