")
Back to Journals » International Journal of General Medicine » Volume 17
Knowledge, Attitudes, and Practices of Physicians Regarding Targeted Drug Therapy for Lung Cancer
Authors Nie D, Ma H, Huang G, Zhao T, Li W
Received 21 February 2024
Accepted for publication 28 May 2024
Published 10 June 2024 Volume 2024:17 Pages 2681—2689
DOI https://doi.org/10.2147/IJGM.S465079
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Di Nie,1,2,* Haozhi Ma,1,2,* Guosheng Huang,1 Tianzeng Zhao,1 Wenxian Li1
1Thoracic Surgery Department, The First Affiliated Hospital of Nanyang Medical College, Nanyang, People’s Republic of China; 2Graduate Division Department, Xinxiang Medical University, Xinxiang, Chian
*These authors contributed equally to this work
Correspondence: Wenxian Li, Thoracic Surgery Department, The First Affiliated Hospital of Nanyang Medical College, Nanyang, People’s Republic of China, Tel +86-15565269994, Email [email protected]
Purpose: This study aimed to examine the KAP of physicians regarding targeted drug therapy for lung cancer in China.
Methods: This cross-sectional study enrolled physicians working in hospitals in Nanyang. A self-administered questionnaire was developed (Cronbach’s α=0.912) to collect the demographic information and KAP.
Results: This study included 191 valid questionnaires. Most participants were male (70.2%) and aged 36– 50 (55.5%). The median knowledge score was 29 (24– 31) (/36, 80.6%), the mean attitude score was 42 (39– 44) (/50, 84.0%), and the mean practice score was 28 (26– 29) (/30, 93.3%), indicating sufficient knowledge, positive attitudes, and proactive practice. The female gender (OR=5.291, 95% CI: 1.426– 19.634, P=0.013), working in non-public tertiary hospitals (OR=0.053, 95% CI: 0.008– 0.360, P=0.003), and working in medical oncology (OR=10.764, 95% CI: 2.638– 43.922, P=0.001) were independently associated with adequate knowledge. Only the knowledge scores (OR=1.121, 95% CI: 1.036– 1.212, P=0.004) were independently associated with a positive attitude. Only the attitude scores (OR=1.895, 95% CI: 1.333– 2.694, P< 0.001) were independently associated with proactive practice.
Conclusion: Physicians working in thoracic surgery, respiratory medicine, or medical oncology displayed sufficient knowledge, positive attitude, and proactive practice toward targeted therapy for lung cancer.
Keywords: knowledge, attitude, practice, lung cancer, targeted therapy, physician
Introduction
Lung cancer is the most common cancer worldwide, with an estimated 2,480,301 new cases in 2022 (12.4% of all cancers), and with the highest contribution to cancer-related mortality, with 1,817,172 deaths (18.7% of all cancer-related deaths).1 Lung cancer is an umbrella term that encompasses several types of disease with different biology (mainly non-small cell lung cancer (NSCLC), with 85–90% of cases, and small cell lung cancer (SCLC)), and patients with the same cancer subtype display different tumor biology due to the presence of various driver mutations (eg, EGFR, ALK, PI3K/AKT/mTOR, RAS-MAPK, RET, MET, BRAF, and NTRK/ROS1) in the tumor.2–4 Fortunately, in the era of precision medicine, several of those mutated genes are actionable and can be targeted with drugs against EGFR (erlotinib, gefitinib, afatinib, dacomitinib, and osimertinib), ALK (crizotinib, ceritinib, alectinib, brigatinib, ensartinib, and lorlatinib), RET (selparcatinib and pralsetinib), MET (capmatinib and repotinib), BRAF (dabrafenib and trametinib), NTRK (larotrectinib and entrectinib), and ROS1 (crizotinib, ceritinib, lorlatinib, and entrectinib).2–4 Despite the efficacy of such drugs, in 33 states in the United States of America (USA), only 66% of the patients with EGFR- or ALK-mutated lung cancer in 2020–2021 received a targeted therapy.5 Immunotherapy is also a novel type of targeted therapy that specifically inhibits the tumor’s immune escape (ie, the ability of a tumor to induce immune tolerance toward cancer cells).3,4 The 5-year survival of patients with NSCLC is 19%, while the 5-year survival of patients with SCLC is 6.3%.6,7
Still, appropriate knowledge of these drugs is necessary for their correct use or to consider referring a patient to a specialist who will provide targeted therapy. The prescription of targeted therapy is based on the indications, the mutations, resistance development, and prognosis.8 Knowledge, attitude, and practice (KAP) is a structured survey method used to investigate the gaps, misunderstandings, and misconceptions toward a specific subject that can constitute barriers to the correct application of the subject in a specific population.9,10 Very little data are available in the literature regarding the KAP toward targeted therapies among specialists. Even for traditional chemotherapy, very few studies examined the oncologists’ KAP toward specific subjects such as resistance.11–13 Previous studies revealed variable KAP toward lung cancer biomarker testing among pulmonologists in the United States of America (USA)14,15 and Canada.16 The KAP toward targeted therapy among physicians is unknown.
Therefore, this study aimed to examine the KAP of physicians regarding targeted drug therapy for lung cancer in China. The results could identify gaps in knowledge that could be addressed to improve the KAP of the specialists, including patient management.
Materials and Methods
Study Design, Setting, and Target Population
This cross-sectional study enrolled physicians working in hospitals of Nanyang between February and March 2023. Nanyang is a prefecture-level city in the southwest of Henan province, China, with a four-season humid subtropical climate. It has a population of 9,713,112 and a per-capita gross domestic product of CNY 31,010 (about USD 4669). Nanyang has a long history of education and academia.
Sample Size
The sample size was determined based on the requirement of 5–10 participants per survey item.17 Hence, this survey had 34 items, and the required sample size was 170–340 participants.
Ethical Considerations
The study was approved by the medical ethics committee of the First Affiliated Hospital of Nanyang Medical College. All participants provided informed consent.
Questionnaire Design
The questionnaire was designed with reference to published relevant literature and guidelines.6,18–21 A questionnaire had to be developed because no prior studies with similar questionnaires were available. In addition, KAP questionnaires have to be adapted to the local practice and policies. The first draft of the questionnaire was designed and revised based on the comments from three experts. The three experts were thoracic surgeons with >20 years of experience. The results of a small pretest (n=32) had a Cronbach’s α of 0.912, suggesting good consistency.
Final Questionnaire
The final questionnaire was in Chinese and included 44 items over four dimensions (Supplement material). The basic information consisted of 10 items, the knowledge dimension consisted of 18 items, the attitude dimension consisted of 10 items, and the practice dimension consisted of six items. For the knowledge items, K1-12 were scored 2 points for “know well”, one point for “partially know”, and 0 points for “do not know”; K13-18 were multiple choice questions, with 2 points for choosing all correct answers, 1 point for choosing some of them, and 0 points for choosing wrong answers or “not sure”. The total knowledge scores ranged 0–36. The attitude and practice items were mainly scored on a 5-point Likert scale, ranging from very positive (5) to very negative (1), with scores ranging 10–50 for the attitude dimension and 6–30 for the practice dimension. Scores ≥80% of the total theoretical score of knowledge, attitude, and practice were considered “adequate knowledge”, “positive attitude”, and “proactive practice”.22
Recruitment Process
The participant inclusion criteria were 1) obtained a degree certificate from junior college or above, 2) fully qualified physician, 3) working in thoracic surgery, respiratory medicine, or medical oncology, and 4) agreed to participate in this scientific research. The exclusion criteria were 1) rotating physicians or 2) trainees.
The questionnaire was uploaded to the Wenjuanxing platform, an electronic questionnaire link was generated, and the participants were recruited by convenience sampling through WeChat groups, phone calls, and face-to-face invitations to disseminate the questionnaire link. If the participant was enrolled online, he/she had to read the text explaining the study. Then, the participant had access to the electronic consent form. Signing the consent form was necessary to have access to the survey itself. If the participant was approached in person, the investigator explained the study to the potential participant. The individual was then invited to scan the QR code. The remaining steps were the same as above. If questions were encountered in the process of answering the questionnaire, members of the research team were responsible for answering them in time.
Quality Control
Participants who participated in the questionnaire through the WeChat group were verified by telephone and confirmed genuine. Once all data were collected, the questionnaires were checked for quality by a member of the research team. The questionnaires with obvious logical errors or a pattern of choosing the same options were considered invalid.
Statistical Analysis
SPSS 22.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. The continuous variables were expressed using means ± standard deviations and analyzed using Student’s t-test (comparisons between two groups) or ANOVA (comparisons among multiple groups). The categorical variables were expressed using n (%) and analyzed using the chi-square test. Univariate and multivariate logistic regression analyses were used to identify factors associated with adequate knowledge, positive attitude, and proactive practice. Variables with a P<0.05 in the univariable logistic regression analyses were included in the multivariable regression analyses. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated. Two-sided P-values <0.05 were considered statistically significant.
Results
Demographic Characteristics
A total of 204 questionnaires were returned (response rate of 100%). Sixty participants were enrolled from WeChat groups, 40 by phone calls, and 104 by face-to-face invitations. After excluding eight invalid and five incomplete questionnaires, 191 valid questionnaires (93.6%) were included in the analysis. Table 1 presents the characteristics of the participants. The participants were working in thoracic surgery (39.3%), respiratory medicine (18.3%), or medical oncology (42.4%). Most participants were male (70.2%), aged 36–50 (55.5%), with a junior college or undergraduate degree (53.9%), working in tertiary public hospitals (87.6%), working in medical oncology departments (42.4%), with a vice senior or senior title (56.5%), with ≥10 years of working experience (74.4%), with a history of administering target therapy (91.6%), with a history of conducting research on targeted therapy (57.6%), and received training on targeted therapy in lung cancer (89.0%).
 |
Table 1 Characteristics of the Participants and KAP Scores |
Knowledge, Attitudes, and Practice
The distribution of the scores is shown in Table 2. The median knowledge score was 29 (24–31) (/36, 80.6%), the mean attitude score was 42 (39–44) (/50, 84.0%), and the mean practice score was 28 (26–29) (/30, 93.3%), indicating sufficient knowledge, positive attitudes, and proactive practice (Tables 1 and 2).
 |
Table 2 Distribution of the KAP Scores |
In the knowledge dimension, the item with the highest correct rate was K9 (know: 83.8%; know a little: 14.14%; “Targeted drugs have some toxic side effects, including rash, diarrhea, liver damage and, in some patients, interstitial pneumonia”). The item with the lowest correct rate was K8 (do not know: 10.0%, “There are several fourth-generation targeted drugs for lung cancer that have already been tested in clinical trials”. (Supplementary Table S1). Supplementary Tables S2 and S3 present the distributions of the answers to the attitude and practice items.
Multivariable Analyses
The female gender (OR=5.291, 95% CI: 1.426–19.634, P=0.013), non-public tertiary hospitals (OR=0.053, 95% CI: 0.008–0.360, P=0.003), and medical oncology (OR=10.764, 95% CI: 2.638–43.922, P=0.001) were independently associated with adequate knowledge (Table 3). Only the knowledge scores (OR=1.121, 95% CI: 1.036–1.212, P=0.004) were independently associated with a positive attitude (Table 4). Only the attitude scores (OR=1.895, 95% CI: 1.333–2.694, P<0.001) were independently associated with proactive practice (Table 5).
 |
Table 3 Analysis of the Factors Associated with Adequate Knowledge |
 |
Table 4 Analysis of the Factors Associated with Positive Attitude |
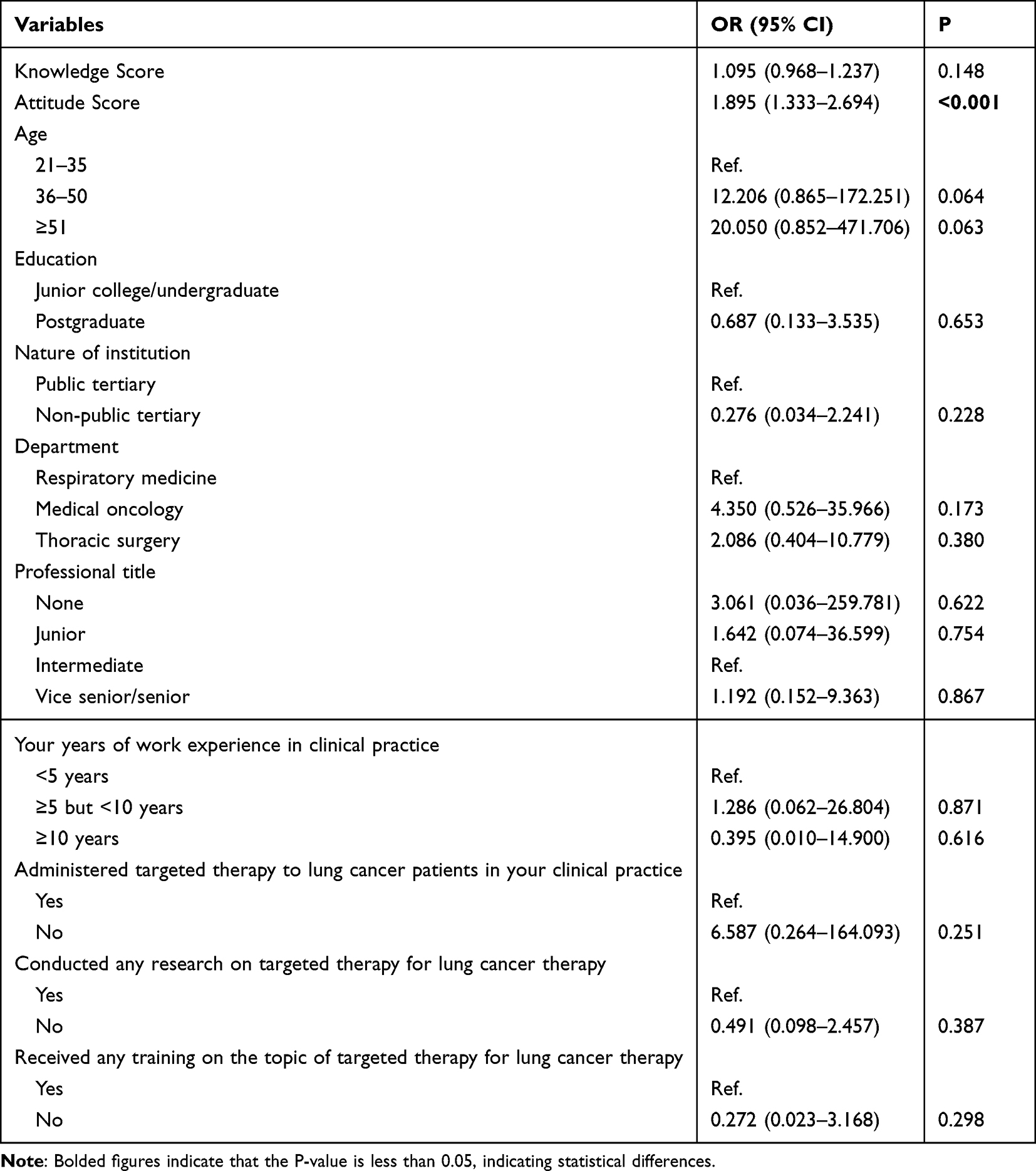 |
Table 5 Analysis of the Factors Associated with Good Practice |
Discussion
The results indicate that physicians working in thoracic surgery, respiratory medicine, or medical oncology displayed sufficient knowledge, positive attitude, and proactive practice toward targeted therapy for lung cancer.
Combined with the high attitude and practice scores but the insufficient knowledge scores, these results suggest that the physicians could be performing some acts based on experience and habits without knowing exactly why they do it. Indeed, KAP increased with participants’ age group, education, and years of experience, as previously observed.14–16 Most participants were undergraduates but were administering targeted therapies to their patients, participated in research on targeted therapy, and received training on targeted therapy. Such training is essential to grasp the subtleties of treatment resistance and how to deal with it.23 The knowledge items on treatment resistance scored relatively low, but the physicians with ≥10 years of experience scored better than the less experienced ones for many of these items. Previous studies revealed variable KAP toward lung cancer biomarker testing among pulmonologists in North America.14–16 Testing for biomarkers is primordial to the selection of adequate targeted therapy. Unfortunately, the present study did not include items on biomarkers and their testing.
In the present study, several knowledge items were found to be insufficient, including items about the molecular indications for targeted therapy, the mutations involved in therapy resistance, the drugs that can be used in case of resistance, and the state of development of new targeted therapies. Understanding treatment resistance is crucial since treatment failure is often due to inadequate strategy preparation.24 In the multivariable analyses, the knowledge score was independently associated with the attitude score, and the attitude score was independently associated with the practice score. Hence, improving knowledge (through lectures, simulations, apprenticeship, and other relevant training) should improve the attitudes and practice toward targeted therapy in lung cancer. Physicians in the medical oncology department had higher knowledge scores, which is unsurprising considering the nature of their job and patient population. Physicians in non-public tertiary hospitals had lower knowledge scores, but it might be due to the nature of their tasks and responsibilities.
This study has some limitations. Although some physicians had a major practice in other hospitals, most had their main practice at the study hospital. Including only the hospitals in Nanyang led to a relatively small sample size when considering the number of physicians involved in lung cancer management in China. It is possible that directly contacting some participants could have introduced bias, but it was necessary to ensure participation. The questionnaire was designed by local investigators based on international guidelines from authoritative institutions, but it was inevitably biased by local practice, policies, and guidelines. Finally, all KAP studies are affected by the social desirability bias, in which the participants can be tempted to answer what they know to be the desired response instead of what they are actually doing.25,26 Considering that most participants were experienced physicians and the attitude and practice scores were high, that bias must be considered.
Conclusion
The results indicate that physicians working in thoracic surgery, respiratory medicine, or medical oncology display sufficient knowledge, positive attitudes, and proactive practice toward targeted therapy for lung cancer. Nevertheless, the take-home message is that despite generally sufficient knowledge, specific items require improvement. Educational and motivational interventions should be designed to improve the KAP of physicians regarding targeted therapies for lung cancer. Since this study only included physicians involved in the treatment of respiratory diseases, the results raise questions regarding whether or not other physicians have sufficient KAP for targeted therapy for lung cancer.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. This study was approved by the Neurosurgery Medical Ethics Committee of the First Affiliated Hospital of Nanyang Medical College [2023-xxghk046], and all participants provided written informed consent.
Author Contributions
All authors made a significant contribution to the study, including study conception, study design, study execution, or acquisition of data, analysis, interpretation, or in all these areas. All authors participated in drafting, writing, substantially revising, or critically reviewing the article. All authors have agreed on the journal to which the article will be submitted. All authors reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. All authors agree to take responsibility and be accountable for the contents of the article.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Majeed U, Manochakian R, Zhao Y, Lou Y. Targeted therapy in advanced non-small cell lung cancer: current advances and future trends. J Hematol Oncol. 2021;14(1):108. doi:10.1186/s13045-021-01121-2
3. Zulfiqar B, Farooq A, Kanwal S, Asghar K. Immunotherapy and targeted therapy for lung cancer: current status and future perspectives. Front Pharmacol. 2022;13:1035171. doi:10.3389/fphar.2022.1035171
4. Xiao Y, Liu P, Wei J, Zhang X, Guo J, Lin Y. Recent progress in targeted therapy for non-small cell lung cancer. Front Pharmacol. 2023;14:1125547. doi:10.3389/fphar.2023.1125547
5. Roberts TJ, Kesselheim AS, Avorn J. Variation in use of lung cancer targeted therapies across state Medicaid programs, 2020–2021. JAMA Network Open. 2023;6(1):e2252562. doi:10.1001/jamanetworkopen.2022.52562
6. NCCN Clinical Practice Guideliknes in oncology (NCCN Guidelines). Non-Small Cell Lung Cancer Version 3.2023. Fort Washington: National Comprehensive Cancer Network; 2023.
7. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Non_Small Cell Lung Cancer. Version 3.2024. Fort Washington: National Comprehensive Cancer Network; 2024.
8. Zhong L, Li Y, Xiong L, et al. Small molecules in targeted cancer therapy: advances, challenges, and future perspectives. Signal Transduct Target Ther. 2021;6(1):201. doi:10.1038/s41392-021-00572-w
9. Andrade C, Menon V, Ameen S, Kumar Praharaj S. Designing and conducting knowledge, attitude, and practice surveys in psychiatry: practical guidance. Indian J Psychol Med. 2020;42(5):478–481. doi:10.1177/0253717620946111
10. World Health Organization. Advocacy, communication and social mobilization for TB control: a guide to developing knowledge, attitude and practice surveys. Available from: http://whqlibdoc.who.int/publications/2008/9789241596176_eng.pdf.
11. Kim ES. Chemotherapy Resistance in Lung Cancer. Adv Exp Med Biol. 2016;893:189–209.
12. Pokhriyal R, Hariprasad R, Kumar L, Hariprasad G. Chemotherapy resistance in advanced ovarian cancer patients. Biomark Cancer. 2019;11:1179299X1986081. doi:10.1177/1179299X19860815
13. Hassan BAR, Mohammed AH, Alsammarraie AZA, et al. Knowledge, attitude, and practice of oncologists toward chemotherapy resistance: a questionnaire development and pilot testing. Asian Pac J Cancer Prev. 2022;23(12):4275–4284. doi:10.31557/APJCP.2022.23.12.4275
14. Fox AH, Jett JR, Roy UB, et al. Knowledge and practice patterns among pulmonologists for molecular biomarker testing in advanced non-small cell lung cancer. Chest. 2021;160(6):2293–2303. doi:10.1016/j.chest.2021.06.027
15. Munoz-Antonia T, Simmons VN, Sutton SK, et al. Use of biomarker testing in lung cancer among Puerto Rico and Florida physicians: results of a comparative study. J Clin Pathw. 2019;5(8):33–40.
16. Zer A, Cutz JC, Sekhon H, et al. Translation of knowledge to practice-improving awareness in NSCLC molecular testing. J Thorac Oncol. 2018;13(7):1004–1011. doi:10.1016/j.jtho.2018.03.005
17. Ni P, Chen JL, Liu N. Sample size estimation for quantitative studies in nursing research. Chinese Journal of Nursing. 2010;45(04):378–380.
18. Eberhardt WE, De Ruysscher D, Weder W, et al. 2nd ESMO consensus conference in lung cancer: locally advanced stage III non-small-cell lung cancer. Ann Oncol. 2015;26(8):1573–1588. doi:10.1093/annonc/mdv187
19. Owen DH, Singh N, Ismaila N, et al. Therapy for stage IV non-small-cell lung cancer with driver alterations: ASCO living guideline, version 2022.2. J Clin Oncol. 2023;41(5):e10–e20. doi:10.1200/JCO.22.02124
20. Wu YL, Planchard D, Lu S, et al. Pan-Asian adapted Clinical Practice Guidelines for the management of patients with metastatic non-small-cell lung cancer: a CSCO-ESMO initiative endorsed by JSMO, KSMO, MOS, SSO and TOS. Ann Oncol. 2019;30(2):171–210.
21. Soo RA, Anderson BO, Cho BC, et al. First-line systemic treatment of advanced stage non-small-cell lung cancer in Asia: consensus statement from the asian oncology summit 2009. Lancet Oncol. 2009;10(11):1102–1110. doi:10.1016/S1470-2045(09)70238-4
22. Bloom BS. Learning for mastery. Instruction and curriculum. Regional Education laboratory for the Carolinas and Virginia, topical papers and reprints, number 1. Evalu Comm. 1968;1:2.
23. Chen D, Liu D, Chen Z. Potential therapeutic implications of miRNAs in osteosarcoma chemotherapy. Tumour Biol. 2017;39(9):1010428317705762. doi:10.1177/1010428317705762
24. Maeda H, Khatami M. Analyses of repeated failures in cancer therapy for solid tumors: poor tumor-selective drug delivery, low therapeutic efficacy and unsustainable costs. Clin Transl Med. 2018;7(1):11. doi:10.1186/s40169-018-0185-6
25. Bergen N, Labonte R. “Everything is perfect, and we have no problems”: detecting and limiting social desirability bias in qualitative research. Qual Health Res. 2020;30(5):783–792. doi:10.1177/1049732319889354
26. Latkin CA, Edwards C, Davey-Rothwell MA, Tobin KE. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addict Behav. 2017;73:133–136. doi:10.1016/j.addbeh.2017.05.005
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Managing Pain in Low Resource Settings: Healthcare Professionals’ Knowledge, Attitude and Practice Regarding Pain Management in Western Nepal
Thapa P, KC B, Lee SWH, Dujaili JA, Gyawali S, Mohamed Ibrahim MI, Alrasheedy AA
Journal of Pain Research 2022, 15:1587-1599
Published Date: 2 June 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Critical Care Nurses’ Knowledge, Attitudes, and Practices Regarding Pressure Injury Treatment: A Nationwide Cross-Sectional Survey
Li J, Zhu C, Liu Y, Song B, Jin J, Liu Y, Wen X, Cheng S, Wu X
Risk Management and Healthcare Policy 2022, 15:2125-2134
Published Date: 16 November 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Role of Community Pharmacist in Asthma Management: Knowledge, Attitudes and Practice
Jarab AS, Al-Qerem W, Alzoubi KH, Almomani N, Abu Heshmeh SR, Mukattash TL, Al Hamarneh YN, Al Momany EM
Journal of Multidisciplinary Healthcare 2024, 17:11-19
Published Date: 3 January 2024