")
Back to Journals » Journal of Asthma and Allergy » Volume 17
Progress in Research into the Effectiveness of Pulmonary Rehabilitation in Children with Asthma - A Narrative Review
Received 10 May 2024
Accepted for publication 29 July 2024
Published 7 August 2024 Volume 2024:17 Pages 743—750
DOI https://doi.org/10.2147/JAA.S475367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Ping Wu,1 Yijing Hu,2 Xiaoxia Yan3
1School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Department of Respiratory Medicine, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 3Department of Thoracic Surgery, Shanghai Pulmonary Hospital, Tongji University, Shanghai, People’s Republic of China
Correspondence: Xiaoxia Yan, Department of Thoracic Surgery, Shanghai Pulmonary Hospital, Tongji University, Shanghai, People’s Republic of China, Tel +86 13761286006, Email [email protected] Yijing Hu, Department of Respiratory Medicine, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China, Tel +86 18917180737, Email [email protected]
Abstract: Asthma is the most common chronic respiratory disease in children. It has a serious impact on children’s physical and mental health. Pulmonary rehabilitation is a multidisciplinary and comprehensive intervention for patients with chronic respiratory disease, whose major components include breathing training, inspiratory muscle training and exercise training. Pulmonary rehabilitation is a multidisciplinary and comprehensive intervention for patients with chronic respiratory diseases, the main components of which are breathing training, inspiratory muscle training and exercise training. Pulmonary rehabilitation can improve the physical and mental condition of patients with chronic respiratory diseases and promote healthy behaviors. However, there is little research on pulmonary rehabilitation in children with asthma. This review comprehensively evaluated the effect of pulmonary rehabilitation in children with asthma at home and abroad, aiming to provide reference for clinical research on pulmonary rehabilitation in children with asthma.
Keywords: bronchial asthma, pulmonary rehabilitation, breathing training, inspiratory muscle training, exercise training
Bronchial asthma, namely asthma, is a respiratory disease characterized by chronic airway inflammation. Asthma has a long course and is prone to recurrent attacks that can cause irreversible damage to the airways.1 Asthma usually begins in childhood and in the last decade the prevalence of asthma in children has increased from 11.1% to 13.2% worldwide, which is much higher than the prevalence of asthma in adults.2 It is responsible for considerable global morbidity and health-care costs.3 It is defined by the history of respiratory symptoms such as wheezing, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation.4 Restricted expiratory airflow results in the lung expansion, which subsequently alters the shape and position of the diaphragm and impairs the functionality of the respiratory muscles.5
Rational and standardized medication is an important measure in the current management of asthma.6 However, Asthma remains poorly controlled in some children even after receiving standardized treatment. At present, at least 20% of children with asthma cannot get good control of their symptoms.7 Therefore, it is necessary to add complementary therapies to standardized treatment. Pulmonary rehabilitation, as a measure of adjuvant therapy, can develop comprehensive interventions for children based on a comprehensive assessment of the child patients. Specifically, Pulmonary rehabilitation includes exercise training, respiratory exercise, and health education, etc. Recently, Zampogna et al indicated pulmonary rehabilitation plays an important role in the treatment of asthma.8 This review evaluated the effect of pulmonary rehabilitation in asthmatic children at home and abroad, aiming to help clinical practice of pulmonary rehabilitation in the later stage.
Application of Pulmonary Rehabilitation
We used the following words to systematically retrieve relevant literature: pulmonary rehabilitation, asthma, Bronchial Asthma, children. There is the extensive scope of research on the rehabilitation of chronic respiratory diseases. The types of diseases suitable for pulmonary rehabilitation include various chronic respiratory diseases, such as COPD, pulmonary hypertension, interstitial lung disease, etc.9 The corresponding rehabilitation models mainly consist of hospital-centered pulmonary rehabilitation training, home-centered pulmonary rehabilitation training, and telemedicine rehabilitation training. These primarily focus on the exercise training and physical activities of these patients.
Pulmonary Rehabilitation in Childhood Asthma
The asthma process includes acute exacerbation, chronic persistence, and clinical remission.10 The chronic persistent and clinical remission phases of asthma are relatively stable and thus children in these two stages have few or no respiratory symptoms. An expert consensus11 indicates that the strengthening and standardisation of treatment and rehabilitation management of children with chronic airway inflammatory diseases in remission is important for reducing the risk of acute exacerbations, improving motor function, facilitating the restoration of a normal developmental trajectory of lung function, reducing irreversible airflow limitation, and improving the quality of life. It is also recommended that once childhood asthma has stabilised into remission, rehabilitation and management can be initiated for different diseases.12
Impact of Pulmonary Rehabilitation on Children with Asthma
The study by Liu et al suggested that the pulmonary rehabilitation programme can effectively improve exercise tolerance and lung function in children with asthma improve their asthma control and quality of life, and reduce the number of acute exacerbations and hospitalisation in the later stages of asthma, which is of high value for promotion and application.13 Currently, pulmonary rehabilitation programmes for children with asthma include respiratory training, exercise training, inspiratory muscle training, health education, psychological and nutritional guidance. Table 1 summarized basic information of the relevant studies, including study design, sample characteristics follow-up time, etc.
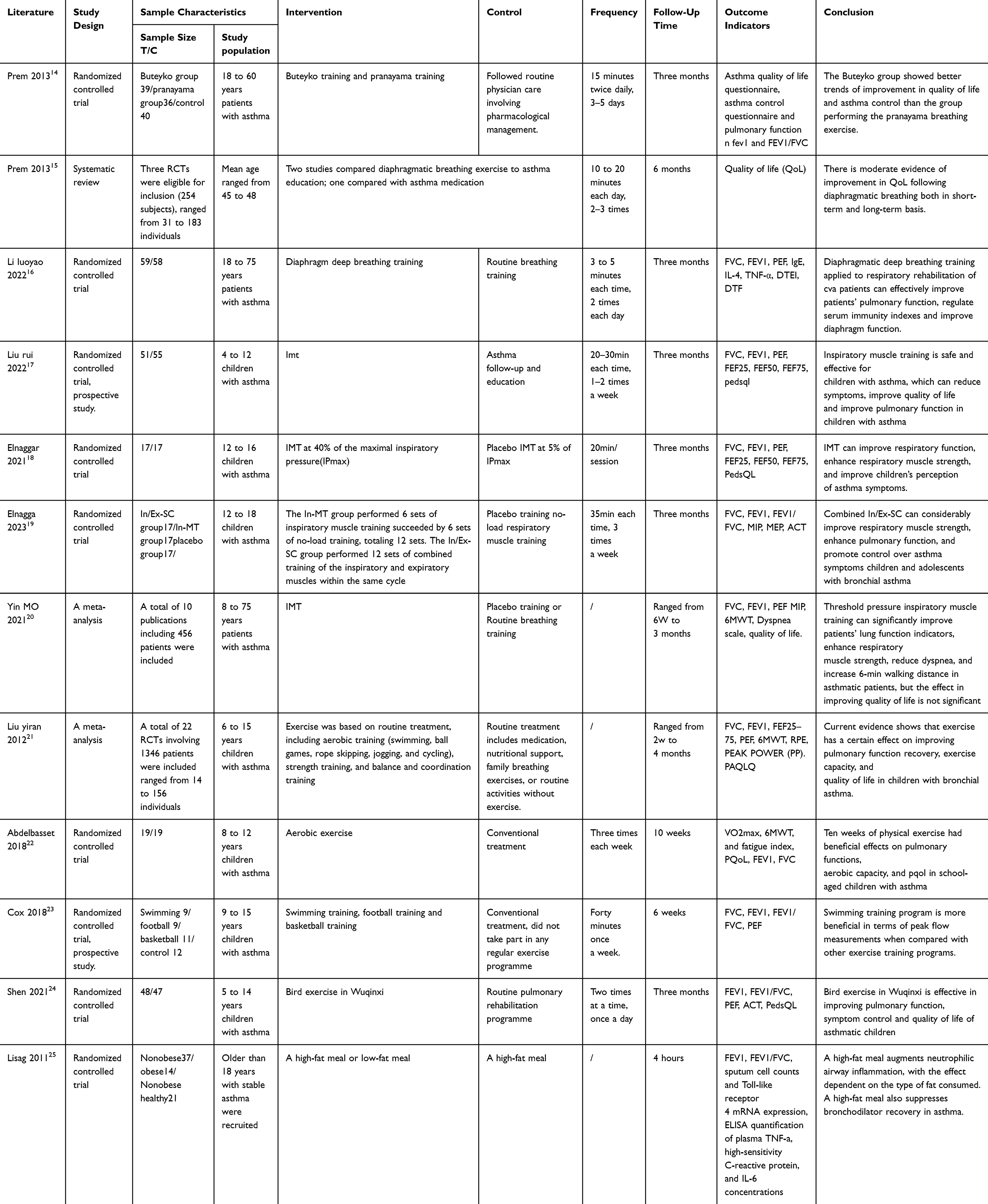 |
Table 1 Basic Characteristics of Relevant Studies |
Breathing Training
Breathing training is one of the main training programmes in pulmonary rehabilitation, and studies have shown that children with asthma have expiratory difficulties and movement limitations. Restricted expiratory airflow causes the lungs to expand, thus changing the shape and position of the diaphragm and decreasing the function of the respiratory muscles.26 Breathing training is the training of muscles with respiratory function by applying a certain load resistance during expiration and inhalation of the body, adjusting the respiratory rate, increasing muscle strength and endurance, and increasing the coherence of the mental, neural, immune, and cognitive systems, which can positively affect the patient’s recovery. Breathing training mainly includes lip-contraction breathing, abdominal breathing and partial breathing.
Prem et al14 studied the effect of Buteyko breathing training on children with asthma and the results showed that in children with asthma, the addition of Buteyko training to conventional treatment improved results in spirometry and parental emotional functioning, but there was no significant difference between the two groups in terms of changes in the dose of bronchodilator medication, which may be related to the shorter duration of the intervention and requires continued attention at a later stage.
A systematic review of diaphragmatic breathing exercises and quality of life in children with asthma showed that respiratory training using the diaphragm slowed down one’s breathing, thus reducing excessive ventilation, and improving quality of life in asthmatics.15 To study the effect of diaphragmatic breathing exercise applied in patients with cough variant asthma, the results showed that diaphragmatic breathing exercise can effectively improve patients’ lung function, regulate serum immune indexes and improve diaphragm function.16
Current studies have shown that different respiratory training methods can improve lung function to different degrees, but there are no studies comparing which respiratory training methods can bring the best results for asthmatic children, and future studies can further explore this. There is a wide variation in the description of the duration of respiratory training between national and international studies, and no guidelines have been issued to recommend this.
Inspiratory Muscle Training
The increased work done by the inspiratory muscles may cause fatigue of the inspiratory muscles, which over time may result in a decrease in the child’s maximal respiratory capacity and maximal exercise tolerance.27 Inhalation muscle training (IMT) is an important form of exercise in pulmonary rehabilitation. Inspiratory muscle training (IMT) is an important form of exercise in pulmonary rehabilitation that improves the strength and tolerance of the thoracic and extrathoracic muscles, thereby relieving the symptoms of asthma.
Current studies have shown that inspiratory muscle training can improve the symptoms of asthma in children, but the effect on the quality of life is still controversial. In the study of Liu Rui et al, 17, 106 children with asthma aged 4 to 12 years were selected as the research objects and divided into 2 groups by the method of randomized control. 51 children in the experimental group received inspiratory muscle training and routine asthma health education and follow-up. 55 children in the control group received routine asthma health education and follow-up. After 3 months, the subjects were followed up for daytime symptoms, nighttime symptoms, quality of life scores, pulmonary function indexes and adverse reactions during training. The results showed that FVC (%pred), FEV1 (%pred), PEF (%pred), FEF25 (%pred), and the total score of quality of life in the inspiratory muscle training group were significantly higher than those in the control group (P < 0.05). Compared with the control group, the scores of daytime and nighttime symptoms in the experimental group were lower. All were statistically significant (P<0.05). The results show that inspiratory muscle training can reduce the symptoms, improve the quality of life and improve lung function in children with asthma. This is consistent with the findings of Elnaggar18,19 et al.
A total of 10 randomized intervention studies were included in the study of Imer,20 including 456 patients with asthma aged 8 to 75 years. The effect of threshold pressure load inspiratory muscle training on pulmonary rehabilitation and quality of life of asthma patients was evaluated through meta-analysis. The results showed that: Threshold pressure loading inspiratory muscle training improved forced vital capacity [SMD=0.90, 95% CI (0.68, 1.11), P<0.001], forced expiratory volume in one second [SMD=0.62, 95% CI (0.41, 0.83), P<0.001], P<0.001], peak expiratory flow rate [WMD=0.32, 95% CI (0.01, 0.62), P=0.040], maximum voluntary ventilation [WMD=11.89, 95% CI (6.42, 17.37), P<0.001], enhanced maximum inspiratory pressure [SMD=29.76, 95% CI (18.15, 41.36), P<0.001], reduced the degree of dyspnea [SMD=−0.51, 95% CI (−0.95, −0.06), P<0.001], prolonged the 6-minute walking distance [WMD=77.13, 95% CI (24.58, 129.67), P=0.004], but there was no significant difference in improving the quality of life of patients [SMD=1.21, 95% CI (−2.11, 4.52), P=0.480].
More high quality clinical studies are needed to further validate the effectiveness of inspiratory muscle training in the management of childhood asthma.
Sports Training
Some asthmatic children and their parents reduce exercise for fear that it will trigger an acute asthma attack. According to the Global Initiative for Asthma (GINA)21 Regular exercise of moderate or higher intensity is more beneficial to children with asthma than to the general population, and promotes mental recovery and respiratory function in children with asthma. The study found that22,23 Standardised treatment with exercise training can improve children’s exercise tolerance, quality of life and lung function. Aerobic training in children with asthma promoted asthma control, quality of life, asthma symptoms, psychological distress, physical activity and airway inflammation.
Regarding the form of exercise, Cox24 et al compared the effects of three sports such as swimming, football and basketball on children with asthma, and the results suggest that swimming is more advantageous in improving maximal expiratory flow compared to other sports. Other forms of exercise, eg, resistance exercise, have not attracted enough attention for asthma control, such as the five birds and the eight danjins.28
Short-term exercise is not conducive to the improvement of cardiorespiratory fitness, and long-time exercise can easily lead to fatigue accumulation, which not only affects the effect of exercise, but also may cause accidental injury. Therefore, exercise for children with asthma should start with a preliminary plan that is suitable for the individual characteristics of the child, and gradually reach the exercise goal, which includes the frequency of exercise, intensity of exercise, mode of exercise, time of exercise, total amount of exercise, and the process of implementing the exercise prescription.29 The following is an example of the process of implementing an exercise prescription. However, the descriptions of exercise time and frequency in children with asthma in the current study are inconsistent,30 and a more reasonable exercise training programme for pulmonary rehabilitation needs to be developed at a later stage.
Health Education
An Italian croup survey31 found that about 40% of caregivers (mainly mothers) believe that asthma medication should be used only when the child has symptoms (cough, congestion or wheezing); a survey conducted in China for parents of 2960 asthmatic children showed that only 18.31% of parents answered more than 60% of the asthma-related questions correctly, and the lack of parental awareness of asthma and the lack of attention to asthma directly leads to a gap between the actual management of asthma and the expected level of control. Inadequate parental knowledge and attention to asthma will directly lead to a gap between actual management and expected control.25 The lack of parental awareness and attention to asthma will directly lead to a gap between actual management and expected control.
Health education, as part of comprehensive rehabilitation for children with asthma, can change the medication behaviour of children and primary caregivers, help improve treatment adherence, enhance acute attack management ability and avoid triggers, thus facilitating asthma control. The content of health education includes the principles of asthma prevention and treatment, the methods and purposes of pulmonary rehabilitation, etc. The form of education is based on oral explanation by medical staff in the hospital, popular science magazines and books, and with the advent of the Internet era, there has been a gradual shift to the Internet of Things, artificial intelligence technology and social software (Jitterbugs, WeChat Groups), and so on.
Nutritional Guidance
Food and nutrition play a role in the development, progression and control of asthma. Obesity is a risk factor for the development of asthma and increases dyspnoea and dyskinesia. High fat intake exacerbates respiratory inflammation, and studies have shown that that sputum neutrophil counts increase in asthmatics 4 h after consumption of high-fat foods.32 A diet rich in vitamins C and E, carotenoids, flavonoids and selenium provides antioxidants that reduce oxidative stress, assist in anti-inflammatory effects, and help to reduce asthma symptoms; vitamin D protects against respiratory infections and inflammatory diseases, and has an immunomodulatory and airway remodelling effect in children with asthma. Vitamin D can protect against respiratory infections and inflammation, and has an immunomodulatory and airway remodelling effect in children with asthma. The above studies suggest that establishing and providing a rational dietary and nutritional programme for children with asthma and evaluating the role of diet in asthma, as well as actively intervening in obesity, is necessary for children with asthma.
Psychological Support
Asthma is a physical and mental disease, psychological factors in the occurrence and development of asthma plays an important role in the whole process. Overseas scholars of more than 7000 children and adolescents cross-sectional survey analysis found that the total prevalence of asthmatic adolescents with anxiety disorders as high as 22.7%, which is three times as high as the healthy population.33 The prevalence of anxiety disorders among adolescents with asthma was 22.7%, three times that of the healthy population. The study shows that [34] among children with asthma, anxiety- and depression-related psychological disorders can lead to emergency room visits and a higher frequency of asthma attacks in children with asthma. Academics recommend that healthcare providers make appropriate referrals to mental health services as part of developing and monitoring asthma treatment plans for adolescent patients. Psychological interventions, which can be delivered in a variety of ways, including boot camps, phone calls, and the Internet, after assessment of psychological status with a specialist medical (nurse) practitioner, can increase the child’s sense of security and improve treatment adherence. The psychological state of the child and his/her parents can facilitate or hinder the management of childhood asthma. For children with poorly controlled asthma, healthcare professionals should conduct psychological assessment of the child and his/her family for psychological support and intervention.
Discussion and Summary
Above all, the implication of this study is as follows:
- Several studies have shown that pulmonary rehabilitation is effective in controlling asthma symptoms, reducing asthma exacerbations, improving children’s quality of life, and improving lung function.
- It is noted that there are still some deficiencies and controversies in pulmonary rehabilitation research. At present, a unified pulmonary rehabilitation training method and effect assessment method have not been developed, and the results present a large variability.
- More high-quality, large-sample randomised controlled trials are needed to confirm the therapeutic effect of pulmonary rehabilitation on children with asthma.
- Pulmonary rehabilitation should be individualised and comprehensive, but how to develop individualised pulmonary rehabilitation programmes and training plans, and how to standardise the evaluation of the efficacy of pulmonary rehabilitation are problems that need to be solved in the treatment of children with asthma.
Funding
This study was funded by the Diagnostic and Treatment Technology Promotion And Optimisation Management Project of ShangHai Shenkang Hospital Development(SHDC22023236); Clinical Science and Technology Innovation Project of Shanghai Shenkang Hospital Development Centre (SHDC22022225).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Jones H, Lawton A, Gupta A. Asthma attacks in children-challenges and opportunities. Indian J Pediatr. 2022;89(4):373–377. doi:10.1007/s12098-021-04069-w
2. Licari A, Brambilla I, Marseglia A, et al. Difficult vs. severe asthma: definition and limits of asthma control in the pediatric population. Front Pediatr. 2018;6:170. doi:10.3389/fped.2018.00170
3. Pavord ID, Beasley R, Agusti A, et al. After asthma: redefining airways diseases. Lancet. 2018;391(10118):350–400. doi:10.1016/S0140-6736(17)30879-6
4. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention; 2022.
5. Silva IS, Fregonezi GA, Dias FA, Ribeiro CT, Guerra RO, Ferreira GM. Inspiratory muscle training for asthma. Cochrane Database Syst Rev. 2013;2013(9):CD003792. doi:10.1002/14651858.CD003792.pub2
6. Rehman A, Amin F, Sadeeqa S. Prevalence of asthma and its management: a review. J Pak Med Assoc. 2018;68(12):1823–1827.
7. Editorial Committee of Chinese Journal of Paediatrics, Respiratory Group of Paediatrics Branch of Chinese Medical Association, Children’s Respiratory Committee of Paediatricians Branch of Chinese Physicians Association. Recommendations for standardised diagnosis and treatment of childhood bronchial asthma (2020 version). Chin J Paediatr. 2020;58(9):708–717.
8. Zampogna E, Spanevello A, Visca D. Pulmonary rehabilitation: promising nonpharmacological approach for treating asthma? Curr Opin Allergy Clin Immunol. 2020;20(1):80–84. doi:10.1097/ACI.0000000000000597
9. Huang Q, Liu H, Rong X, et al. Visual analysis of domestic and international rehabilitation of chronic respiratory diseases in the past 10 years. Chin Rehabil Theory Pract. 2022;28(08):939–959.
10. Liu C, Li S, Shao M. Characteristics of pulmonary function changes in children with bronchial asthma. Chin J Pract Paediatr. 2021;36(06):412–416.
11. Cao L, Chen X, Fu Z, et al. Expert consensus on treatment and rehabilitation management of chronic airway inflammatory diseases in children during remission. J Clin Paediatr. 2022;40(10):770–781.
12. Gong Y, Chen J, Li P, et al. Expert consensus on pulmonary rehabilitation nursing care for chronic respiratory diseases. Chin J Nurs. 2020;55(05):709–710.
13. Liu Y, Tang Y, Zhang L. A randomised controlled and longitudinal follow-up observational study of the mid- and long-term efficacy of a multimodal pulmonary rehabilitation programme in paediatric asthma. Int J Med Health. 2022;28(16):2303–2306.
14. Prem V, Sahoo RC, Adhikari P. Comparison of the effects of Buteyko and pranayama breathing techniques on quality of life in patients with asthma - a randomized controlled trial. Clin Rehabil. 2013;27(2):133–141. doi:10.1177/0269215512450521
15. Prem V, Sahoo RC, Adhikari P. Effect of diaphragmatic breathing exercise on quality of life in subjects with asthma: a systematic review. Physiother Theory Pract. 2013;29(4):271–277. doi:10.3109/09593985.2012.731626
16. Luoyao LI, Danying SUN, Xuehan LU. Effectiveness of diaphragmatic deep breathing training in patients with cough variant asthma. Clin Nurs J. 2022;21(4):25–27.
17. Liu R. A Prospective Cohort Study of Inspiratory Muscle Training in Children with Bronchial Asthma. Chongqing Medical University; 2022.
18. Elnaggar RK. A randomized placebo-controlled study investigating the efficacy of inspiratory muscle training in the treatment of children with bronchial asthma. J Asthma. 2021;58(12):1661–1669. doi:10.1080/02770903.2020.1821058
19. Elnaggar RK, Osailan AM, Elbanna MF. The rationale of applying inspiratory/expiratory muscle training within the same respiratory cycle in children with bronchial asthma: a placebo-controlled randomised clinical investigation. J Asthma. 2022;60:1–12.
20. Yimer, Jia Y, Zhao B, et al. Meta-analysis of the effects of threshold pressure-loaded inspiratory muscle training on pulmonary rehabilitation and quality of life in asthma patients. Chin J Nurs. 2021;56(07):1001–1007.
21. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205(1):17–35. doi:10.1164/rccm.202109-2205PP
22. Abdelbasset WK, Alsubaie SF, Tantawy SA, et al. Evaluating pulmonary function, aerobic capacity, and pediatric quality of life following a 10-week aerobic exercise training in school-aged asthmatics: a randomised controlled trial. Patient Prefer Adherence. 2018;12:1015–1023. doi:10.2147/PPA.S159622
23. Carew C, Cox DW. Laps or lengths? The effects of different exercise programmes on asthma control in children. J Asthma. 2018;55(8):877–881. doi:10.1080/02770903.2017.1373806
24. Shen Y, W Y, W C. Effects of bird play on lung function, symptom control and quality of life of children with asthma. Nurs Res. 2021;35(21):3917–3920.
25. Wood LG, Garg ML, Gibson PG. A high-fat challenge increases airway inflammation and impairs bronchodilator recovery in asthma. J Allergy Clin Immunol. 2011;127(5):1133–1140. doi:10.1016/j.jaci.2011.01.036
26. Silva IS, Fregonezi GA, Dias FA, et al. Inspiratory muscle training for asthma. Cochrane Database Syst Rev. 2013;2013(9):D3792.
27. Duruturk N, Acar M, Doğrul MI. Effect of inspiratory muscle training in the management of patients with asthma: a RANDOMIZED CONTROLLED TRIAL. J Cardiopulm Rehabil Prev. 2018;38(3):198–203. doi:10.1097/HCR.0000000000000318
28. Paediatrics Committee of China Medical Education Association. Expert consensus on exercise prescription for children with asthma in China. Chin Clin J Pract Paediatr. 2022;37(08):563–571.
29. Wanrooij VH, Willeboordse M, Dompeling E, et al. Exercise training in children with asthma: a systematic review. Br J Sports Med. 2014;48(13):1024–1031. doi:10.1136/bjsports-2012-091347
30. Fasola S, Malizia V, Ferrante G, et al. Asthma-related knowledge and practices among mothers of asthmatic children: a latent class analysis. Int J Environ Res Public Health. 2022;19(5):2539. doi:10.3390/ijerph19052539
31. Respiratory Group of the Pediatrics Branch of the Shanghai Medical Association, Pudong Shanghai Children’s Medical Centre Paediatric Medical Consortium. Expert consensus on childhood asthma health education in Shanghai. Chin Clin J Pract Paediatr. 2021;36(9):641–646.
32. Dudeney J, Sharpe L, Jaffe A, et al. Anxiety in youth with asthma: a meta-analysis. Pediatr Pulmonol. 2017;52(9):1121–1129. doi:10.1002/ppul.23689
33. Leonard SI, Turi ER, Powell JS, et al. Associations of asthma self-management and mental health in adolescents: a scoping review. Respir Med. 2022;200:106897. doi:10.1016/j.rmed.2022.106897
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.