")
Back to Journals » International Journal of General Medicine » Volume 17
Quality of Life in the Management of Anaphylaxis in Food-Allergic Adults
Authors Alotiby A
Received 9 March 2024
Accepted for publication 9 July 2024
Published 11 July 2024 Volume 2024:17 Pages 3047—3055
DOI https://doi.org/10.2147/IJGM.S467915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandul Yasobant
Amna Alotiby
Department of Hematology and Immunology, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Amna Alotiby, Department of Hematology and Immunology, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia, Email [email protected]
Background: Anaphylaxis is a life-threatening allergic reaction that can significantly affect the quality of life of those affected. Factors including undiagnosed allergies, lack of allergen information, and insufficient emergency training can impact the quality of life for food-allergic individuals. Well-informed patients are less likely to experience severe allergic responses, ensuring their safety and quality of life.
Aim: This study aims to evaluate the effectiveness of following preventive behavior, focusing on routine counseling and training provided by healthcare professionals in preventing anaphylaxis and assessing the impact of strict adherence to an allergen avoidance regimen against anaphylaxis.
Methods: This study was a descriptive, cross-sectional survey conducted in the Makkah region of Saudi Arabia. It involved adults aged 18 and above who had food allergies. A structured online questionnaire of seven items was developed and distributed to achieve the study’s goals from October 2023 to January 2024. The data collected was automatically exported to Excel and then analyzed using the Statistical Package for the Social Sciences.
Results: The study involved 93 participants, 65.6% female and 34.4% male. Among those with food allergies, 34.4% had experienced anaphylaxis, with 50% allergic to eggs and seafood. The study found no significant association between specific food allergens and a history of anaphylaxis, but strict allergen avoidance was linked to lower anaphylaxis rates. Counseling or training for managing food allergy reactions also showed potential benefits. The research indicated that males were less likely to have anaphylaxis than females, and age increased the severity of anaphylaxis reactions regardless of gender.
Conclusion: The study emphasizes the importance of preventive behaviors and healthcare professional support in reducing the risk of anaphylactic reactions for food-allergic adults. Future research could focus on improving their quality of life through education programs, policy development, and better access to emergency medications and psychosocial support strategies.
Keywords: managing anaphylaxis, anaphylaxis, food allergy, personalized care, quality of life
Introduction
Anaphylaxis, a severe hypersensitivity reaction of the immune system, is primarily triggered by the interaction between an allergen and allergen-specific immunoglobulin E (IgE).1 This interaction occurs when IgE binds to high-affinity IgE receptors that naturally express on mast cells and basophils, leading to a potentially life-threatening condition. Common triggers for these IgE-dependent responses include Hymenoptera venom, food, medications, and latex rubber.2
The anaphylaxis condition is often encountered in individuals with food allergies (FA) or their family members. The unpredictable onset and intensity of these reactions significantly compromise the quality of life for those affected.3 Recent research indicates infrequent fatalities among food-allergic patients, with an annual occurrence of 1.8 in adults and 3.25 in children per million person-years. In affected individuals, minor symptoms may suddenly manifest, progressing at varying rates to severe, potentially fatal conditions such as abdominal cramping, respiratory distress, or impaired consciousness.4
Anaphylaxis patients need to be managed with a focus on both immediate emergency intervention and continuing care. Even if preventative measures are not followed, the objective is to improve outcomes and reduce the likelihood of recurring responses. It is still difficult to predict how severe a response would be, and in catastrophic situations, death can happen in a matter of minutes, highlighting the critical importance of effective emergency treatment.5 The focus extends beyond preventing fatalities; treating and informing at-risk individuals also involves addressing their everyday behavior.4
Many factors can affect the food-allergic individuals’ quality of life (QoL), such as being undiagnosed with the type of allergen that they are allergic to by a doctor or not being well informed about the possibility of cross-reactivity of the allergen with other kinds of foods or not receiving training in how to deal with emergencies or not receiving medical treatments.3,6,7 Well-informed patients are less likely to experience severe allergic responses.3,7,8 Subsequently, the diagnosis of a food allergy by a doctor will significantly impact patients’ QoL, not only resulting in dietary restrictions but also reducing the risk of sudden allergic reactions. In addition, FA patients must receive comprehensive training on handling emergencies and making informed decisions regarding using emergency medication such as Epinephrine autoinjectors. This training and the emergence of food allergen-specific therapies, including oral, sublingual, and epicutaneous immunotherapies, offer hope for a better quality of life for FA patients.3,6,9,10 Addressing these aspects will ensure the FA patient’s safety and help maintain their overall QoL.3
Previous studies on QoL in individuals with food allergy and anaphylaxis have focused on prevalence, allergen types, treatment, cross-reactivity between allergens, knowledge and attitude, mental health, and medication use.3,5,7–13 However, these studies have yet to explore the crucial role of patient behavior in daily life. Importantly, they did not study how targeted counseling, education, and training can significantly enhance these individuals’ QoL by reducing adverse effects and improving adherence to allergen avoidance measures. Therefore, this study aims to evaluate the effectiveness of routine counseling and training sessions provided by healthcare professionals in preventing anaphylaxis and to assess the impact of strict adherence to an allergen avoidance regimen as a preventive measure against anaphylaxis. By addressing these aspects, the current study will help provide healthcare professionals and individuals with food allergies with valuable insights into the pivotal role of daily behavior in mitigating the risk of anaphylactic reactions through simple changes in behavior, offering a hopeful outlook for improved quality of life.
Methodology
Study Design and Population
This cross-sectional study, conducted in the Makkah region of Saudi Arabia between October 2023 and January 2024, focused on individuals with food allergies. At least 18-year-old adults with a history of food allergies participated in the study. Individuals under 18 and those without a diagnosed food allergy were excluded from participation. Participants in the study were asked to provide their informed consent online on the first page of the online Google survey, which was used to gather the data. The participants are asked to fill out the surveys if they decide to participate in the study after carefully reading and understanding the informed consent section on the front page of the survey.
Regarding the required sample size, previous studies conducted in the Makkah region indicated a prevalence ranging from 70 to 100 individuals diagnosed with food allergies.14,15 Based on the number of food-allergic adults in the existing literature, the required sample size was calculated using OpenEpi software version 3.0.16 Therefore, a minimum of 80 participants is required; 93 individuals were included in the study.
Data Collection Tool and Method
The data collection process employed a structured questionnaire inspired by previous studies.3,17 Three experts in medical immunology, family medicine, and clinical nutrition assessed and validated the questionnaire’s style and content for its appropriateness, relevance, clarity, and adequacy.
The questionnaire consisted of seven items distributed across three distinct sections. In the first section, participants were presented with yes/no questions designed to assess inclusion criteria for subsequent parts of the questionnaire. This section asked the participants if they were diagnosed with food allergies. Then, if the participants were food-allergic individuals, they were included in the study and moved to the second part of the questionnaire. The second section focused on gathering personal information from food-allergic patients, including age, gender, and the specific types of food allergens affecting them. The third section assessed the quality of life of food-allergic adults, examining their practices, experiences, and healthcare interactions. Participants were questioned about regular visits to healthcare professionals for counseling/training on managing food allergy reactions, adherence to allergen avoidance regimens, and any history of anaphylaxis.
Statistical Analysis
The data was collected, assessed, and input into the Statistical Package for the Social Sciences version 25 software. All statistical procedures employed were two-tailed, utilizing an alpha level of 0.05. Significance was established if the p-value was less than or equal to 0.05. Descriptive analysis involved the use of frequency distribution and percentage calculations for various research variables, including adults’ history of food allergies, age, gender, and specific food allergens. The analysis carried out were frequencies, and cross-tabulation was employed to illustrate the distribution of reported food allergies among adults, categorized by age and gender.
Results
Socio-Demographic Characteristics of Study Participants
The study aims to assess the safety of food-allergic adults who visit the doctor for routine counseling and training in dealing with food allergy reactions and those who practice a strict regimen to avoid allergens in relation to anaphylaxis. Data was collected from 93 participants using a questionnaire.
The demographic distribution of the participants with food allergies is presented in Table 1. The majority of participants, 65.6%, were female, while 34.4% were male. Participant ages were grouped as follows: 28% were between 18 and 28 years, 18.3% between 29 and 39 years, 37.6% between 40 and 59 years, and 16.1% between 60 and 80 years. Out of the 93 participants with food allergies, only 34.4% had a history of anaphylaxis, 12.9% had visited a doctor for routine counseling or training in dealing with food allergy reactions, and 48.4% had adhered to a strict regimen to avoid allergens. Regarding the distribution of food allergens, the most common food allergens among adults are eggs and seafood, reported by 44.1% of the participants each. Following closely is fruit, reported by 39.8% of individuals. Other notable allergens include tree nuts and milk/dairy products, each reported by 24.7% of the participants. Additionally, peanuts, vegetables, and nuts are also identified as common allergens, reported by 20.4%, 17.2%, and 11.8% of the participants, respectively. Less frequently reported allergens include wheat (8.6%), sesame (6.5%), chili pepper (2.2%), and olive (1.1%), as seen in Table 2.
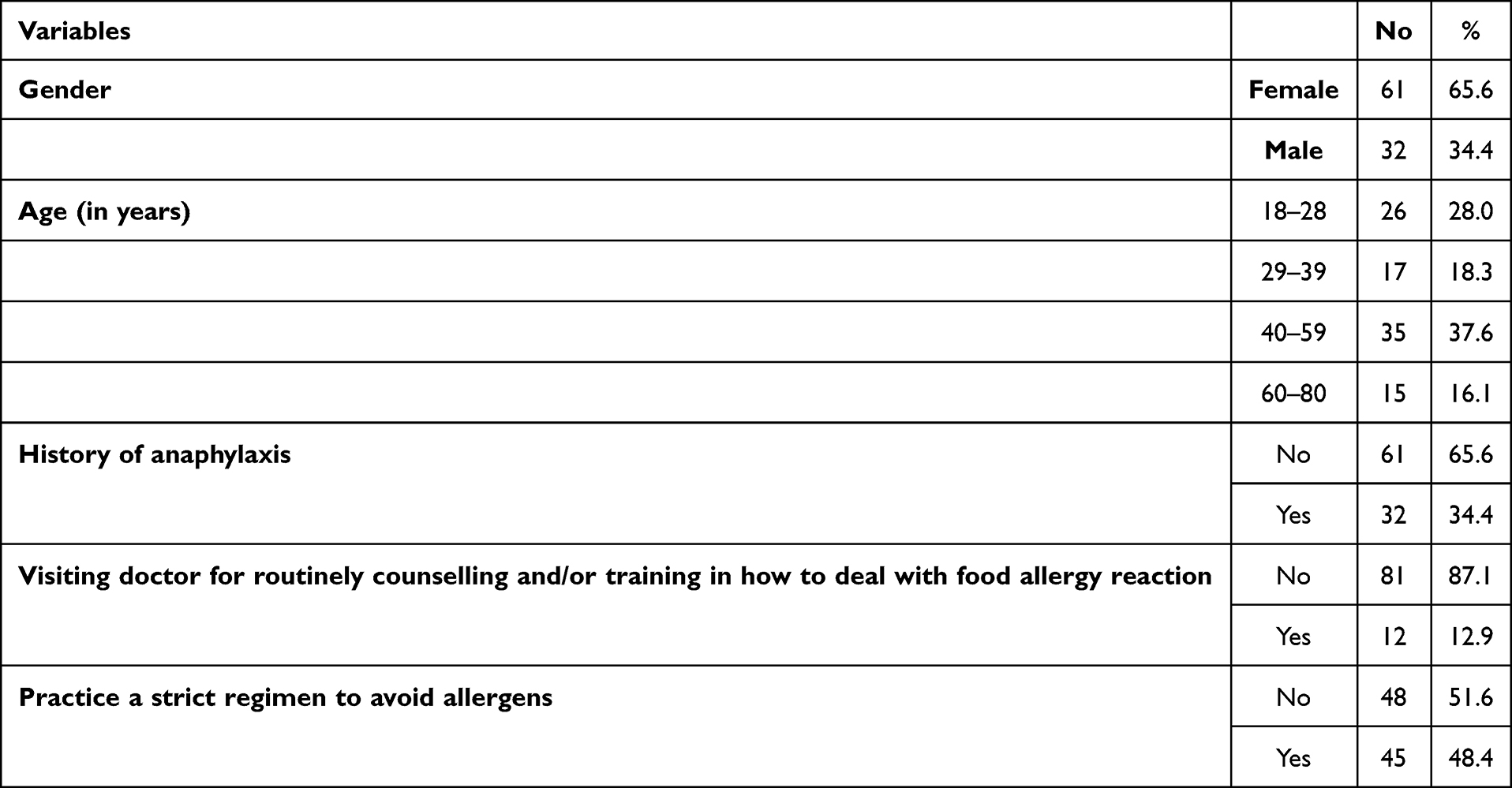 |
Table 1 Socio-Demographic Characteristics of Study Participants |
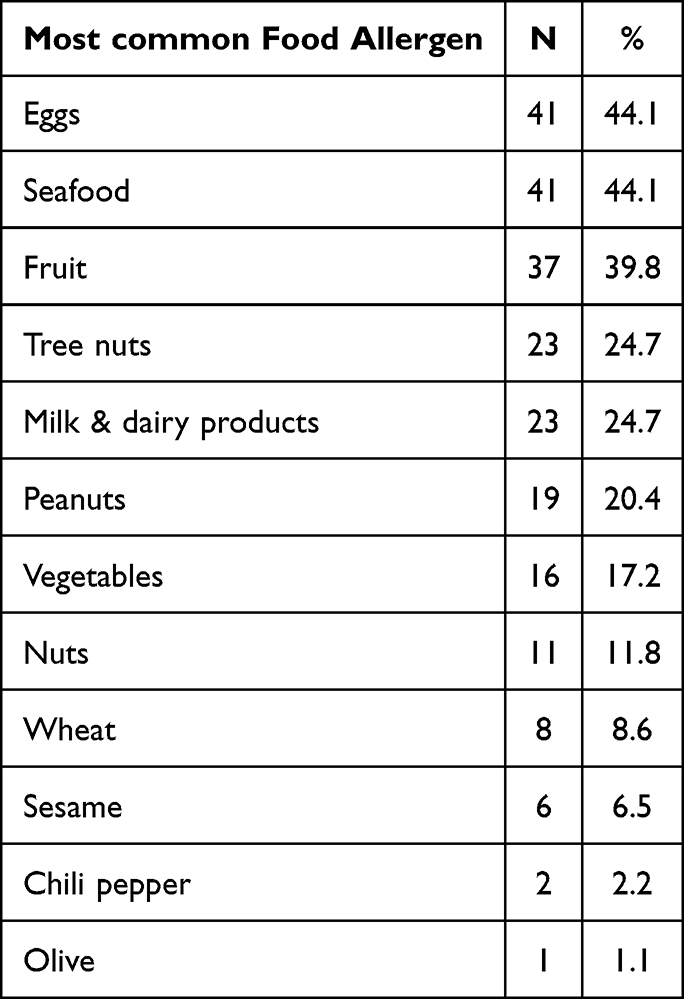 |
Table 2 Most Common Food Allergen Among Adults |
Association Between Food Allergen Types and History of Anaphylaxis
The distribution of food allergens by history of anaphylaxis and the most common allergic food are presented in Table 3. Among them, 50.0% of the participants had eggs and seafood who had a history of anaphylaxis, and 41.0% of the participants were allergic to eggs and seafood who had no history of anaphylaxis. All differences were statistically insignificant (P=0.694>0.05), indicating that there is no significant association between the type of food allergen and the history of anaphylaxis.
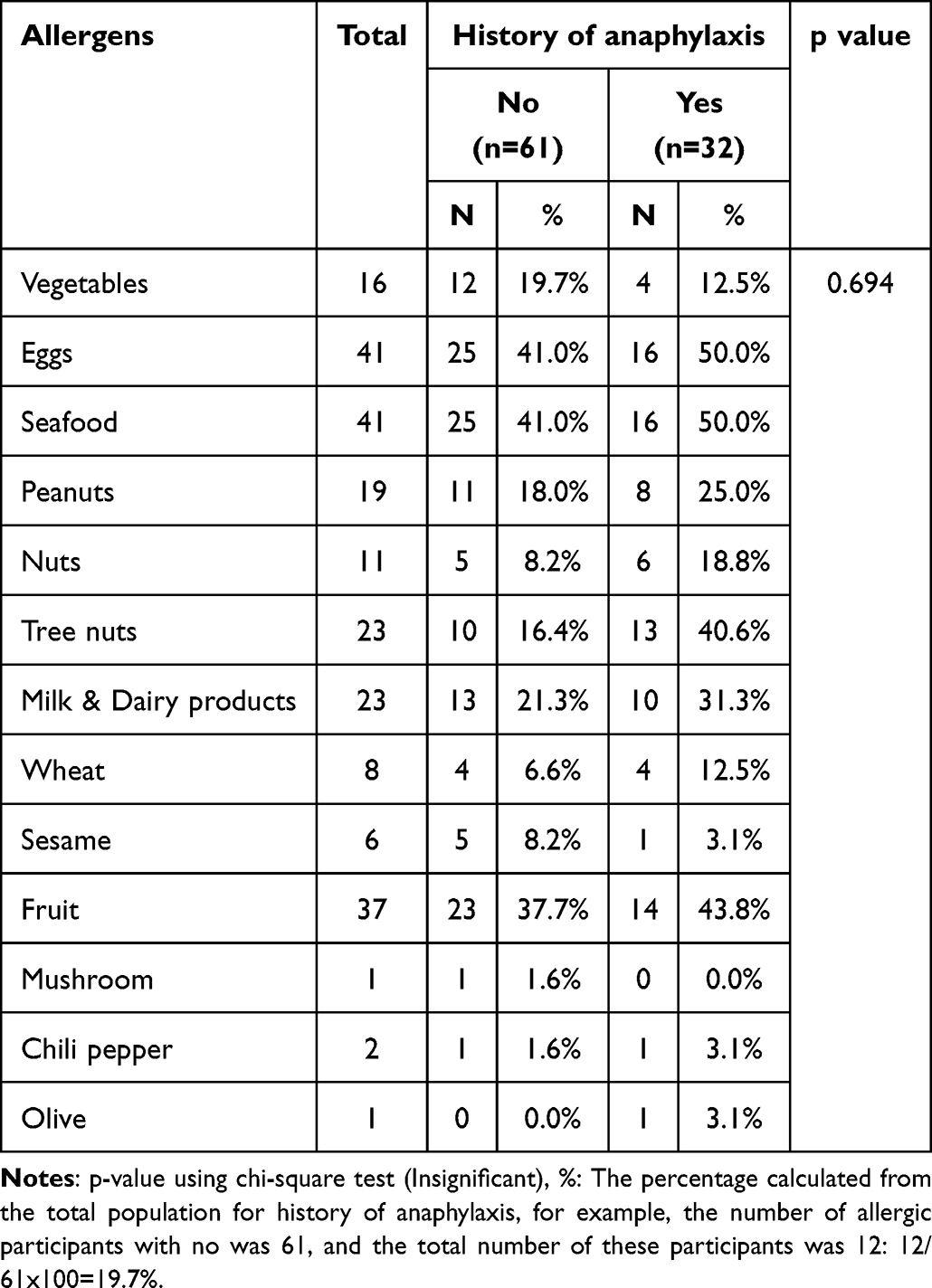 |
Table 3 Association Between Allergens and History of Anaphylaxis |
Association Between Visiting Doctors for Routine Counseling, Practicing a Strict Regimen to Avoid Allergens, and Having a History of Anaphylaxis
In Table 4, this study examined the relationship between a history of anaphylaxis and specific behaviors or practices, specifically focusing on visiting a doctor for counseling/training and adhering to a strict regimen to avoid allergens. The result found that individuals who adhere to a strict regimen to avoid allergens are statistically less likely to have a history of anaphylaxis compared to those who do not (p=0.049<0.05). There is a trend (p=0.062>0.05) that suggests individuals who visit a doctor for counseling/training may also be less likely to have a history of anaphylaxis, but this result is not statistically significant.
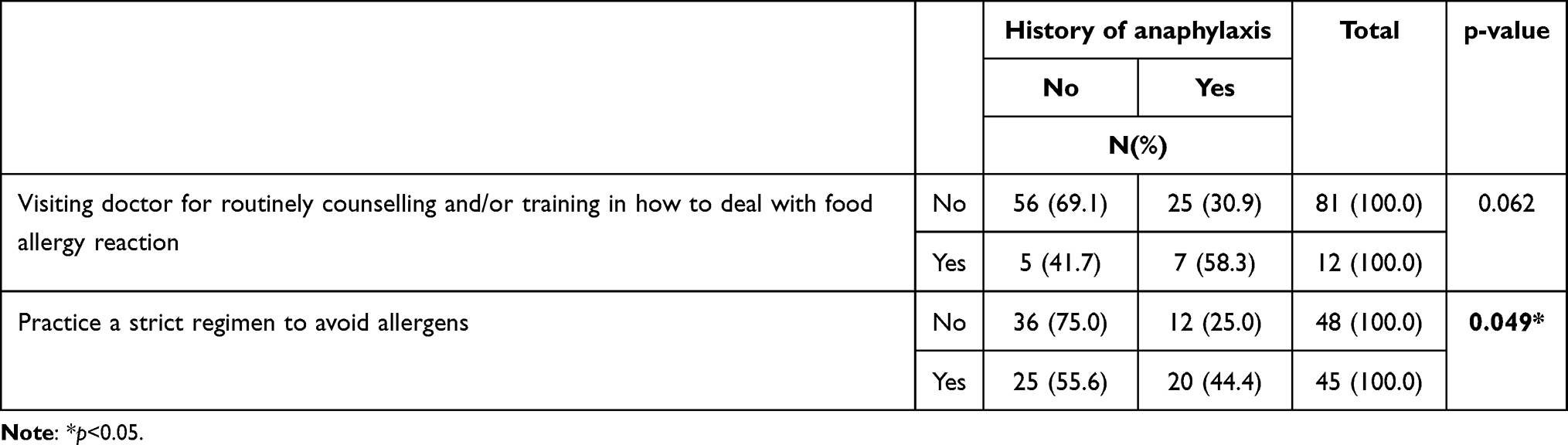 |
Table 4 Association Between Visiting Doctor for Routine Counselling, Practice a Strict Regimen to Avoid Allergens and History of Anaphylaxis |
Association Between a History of Anaphylaxis and Various Demographic Factors, Including Age, Gender, and Adherence to Preventative Behaviors
The association between gender, age, and adherence to specific preventative behaviors, visiting a doctor for routine counseling, and practicing a strict regimen to avoid allergens based on the history of anaphylaxis were analyzed using binary logistic regression. The results of the logistic regression analysis with several independent variables, including coefficients, odds ratios (OR) with 95% confidence intervals (CI), and p-values, are presented in Table 5. In the analysis, males were chosen as the reference category, with a coefficient (β) of −0.371 and a p-value of 0.544 (>0.05). The odds ratio (OR) is 0.690, indicating that being male is associated with 31% lower odds of the outcome compared to the reference category. For the different age groups, individuals aged 29–39 and 40–59 showed coefficients of 0.346 and 0.349, respectively, with p-values of 0.569 and 0.704 (>0.05). The corresponding odds ratios are 1.414 and 1.417, suggesting an increase in the odds of the outcome as the age group increases compared to the reference category (18–28 years). Moreover, individuals who visit a doctor for counseling/training have 2.504 times the odds of the outcome compared to those who do not. The coefficient for practicing a strict regimen to avoid allergens is 0.687, with a p-value of 0.157 (>0.05) and an odds ratio of 1.988, indicating that individuals who follow a strict allergen avoidance regimen have almost 1.988 times the odds of the outcome compared to those who do not.
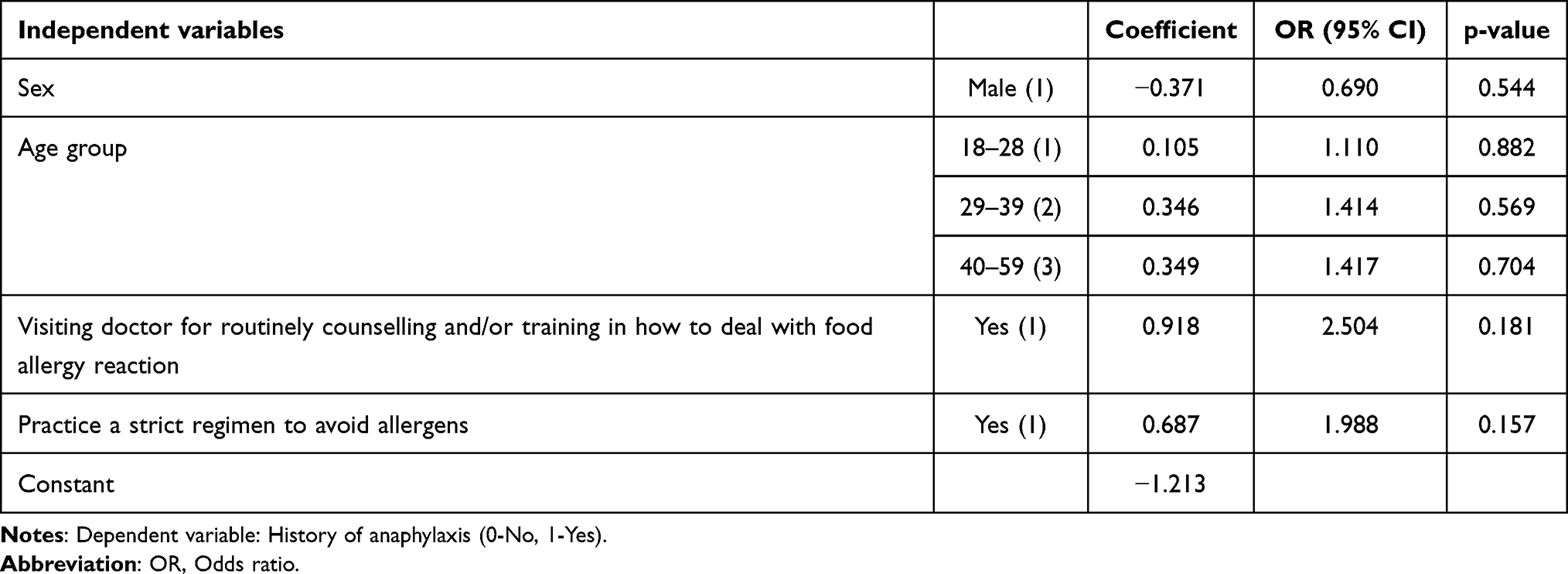 |
Table 5 Association Between Gender, Age, Visiting Doctor for Routinely Counselling, Practice a Strict Regimen to Avoid Allergens on History of Anaphylaxis Using Binary Logistic Regression |
Discussion
Anaphylactic shock, a severe hypersensitivity reaction, presents a substantial threat to the well-being of adults with food allergies. The varying degrees of severity, ranging from mild to life-threatening, emphasize the imperative nature of addressing this issue. The health-related quality of life, encompassing adherence to preventive measures, is pivotal for individuals with conditions such as food allergies.1,7,18 This research thus highlights the correlation between specific preventative behaviors (such as seeking medical counsel and rigorously avoiding allergens) and the incidence of anaphylactic episodes. Furthermore, it delves into the association between the frequency of anaphylactic reactions and the types of allergens encountered.
The incidence of life-threatening anaphylactic reactions is less likely in well-educated adults with food allergies or those trained in dealing with emergencies, significantly enhancing their overall quality of life, as indicated by a study conducted by Lange L.3 Furthermore, the current research supports this finding by indicating that adults with food allergies who visit a doctor for consultation or training are less likely to experience anaphylaxis than those who did not see a doctor. However, this difference is insignificant; the reason might be due to the limitation of this study regarding the sample size. Despite the insignificant, the study’s findings offer a promising perspective on the potential benefits of medical consultation for adults with food allergies.
Avoiding allergens is still considered the primary preventive strategy that keeps food-allergic adults safe from anaphylaxis. Numerous research studies have indicated that obtaining a precise diagnosis and clear recommendations regarding allergen avoidance is crucial in managing emergencies. These elements collectively play a vital role in ensuring not only the safety of the patient but also in maintaining their overall quality of life.3,6,9,10,19 The results of the present study further validate this, indicating that FA individuals who strictly adhere to an allergen avoidance regimen significantly reduce their likelihood of anaphylaxis compared to those who do not. However, avoiding certain foods due to allergies may lead to inadequate nutrient intake, potentially resulting in nutritional deficiencies. Therefore, physicians must play a central role in accurately diagnosing and managing food allergies, which is essential to facilitating the avoidance of triggering foods and preventing unnecessary food avoidance.
Regarding the association between the type of allergen and the incidence of anaphylaxis, this study’s finding indicates that the frequency of anaphylactic reactions is higher in adults allergic to eggs or seafood than other food allergen types. However, it is important to note that this difference is nonsignificant, indicating no direct association between the type of food allergen and the history of anaphylaxis. These findings are consistent with Gargano et al, who demonstrate that any food has the potential to induce anaphylaxis.20 Therefore, it is crucial to understand the potential risks of various food allergens and the need for caution with all food items that cause allergies, regardless of their prevalence.
Anaphylaxis is less prevalent in males than in females. Consistent with this observation, research by Salvati L. et al, and Ellingwood SS. et al, has revealed a higher incidence of anaphylaxis across all causes in adult females than in males.21,22 This difference is due to the hormone estrogen in females, which worsens anaphylactic severity by increasing vascular permeability and leading to systemic consequences through the upregulation of endothelial nitric oxide synthase and mast cell degranulation.22
The current study suggests that the likelihood of experiencing an anaphylactic reaction may rise with age, but this prediction is not statistically significant due to limitations in sample size. Therefore, further research with a larger sample size is necessary to confirm this finding. Despite its lack of significance, previous studies have supported this conclusion and shown that the average severity of reactions tends to increase with age, regardless of the trigger. Additionally, the same research team noted that severe anaphylactic reactions tended to occur between the ages of 39 and 62.23,24 The present study aligns with this observation, finding that severe reactions were most prevalent between 29 and 59 years old. The increased likelihood of food-allergic adults developing allergic reactions as they age may be due to changes in their innate and adaptive immune system. This shift could lead to an uptick in allergic inflammation by upregulating mast cells and favoring an inflammatory and T lymphocyte helper-2 (Th2) profile.25,26
Conclusion
The present study addresses anaphylactic shock in adults with food allergies, specifically emphasizing the importance of preventive behaviors such as allergen avoidance, early diagnosis, and emergency preparedness. It also examines the correlation between specific behaviors and the incidence of anaphylactic episodes in order to mitigate the risk of anaphylactic reactions and ultimately enhance the quality of life for individuals with food allergies. The research highlights the critical role of physicians in accurately diagnosing and managing food allergies. It also discusses the absence of a significant association between the type of food allergen and the history of anaphylaxis, indicating that each food item that causes allergies should be approached cautiously, as even rarely allergenic foods can lead to life-threatening conditions. It also examines gender and age differences in anaphylactic reactions.
Strength, Limitations, and Future Studies
The current study demonstrates strength in addressing the gaps left by previous research by examining the effectiveness of regular counseling and training sessions in preventing anaphylaxis. Additionally, the study assesses the impact of strictly adhering to an allergen avoidance regimen among food-allergic adults in the Makkah region. Despite these advantages, it is important to take into account certain limitations. The primary limitation is the narrow geographic scope, limited to Makkah, and the restriction to participants with access to the online questionnaire. This limited scope may impact the generalizability of the study’s findings. To address this, conducting a comprehensive national study encompassing all regions of Saudi Arabia is recommended. Furthermore, the study relied on self-reported data through an online questionnaire, potentially introducing bias due to variations in participant understanding, standards, and emotional states. Therefore, future research is advised to adopt a qualitative approach, incorporating semi-structured interviews to validate the results of the current study. Future research initiatives could explore varied approaches to enrich the quality of life for food-allergic individuals in Makkah. These may include improved education programs and materials, the development of policy and guidance, enhanced access to emergency medications, training for handling emergencies, and the use of various strategies for psychosocial support.
Acknowledgments
The author is grateful to Umm Al-Qura University, Makkah, Saudi Arabia, for its continuous support.
Ethics Statement
The study received ethical approval from the Faculty of Medicine Biomedical Ethics Committee, Umm Al-Qura University (HAPO-02-K-012-2021-03-631), and was conducted in compliance with the Declaration of Helsinki.
Informed Consent
Electronic informed consent was collected from each participant before they completed the survey. Participants were given a URL that directed them to the survey page after they agreed to participate, which was preceded by reading the informed consent on the survey’s front page.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Yue D, Ciccolini A, Avilla E, Waserman S. Food allergy and anaphylaxis. J Asthma Allergy. 2018;11:111–120. doi:10.2147/jaa.s162456
2. Peavy RD, Metcalfe DD. Understanding the mechanisms of anaphylaxis. Curr Opin Allergy Clin Immunol. 2008;8(4):310–315. doi:10.1097/aci.0b013e3283036a90
3. Lange L. Quality of life in the setting of anaphylaxis and food allergy. Allergo J Int. 2014;23(7):252–260. doi:10.1007/s40629-014-0029-x
4. Beyer K, Eckermann O, Hompes S, Grabenhenrich L, Worm M. Anaphylaxis in an emergency setting – elicitors, therapy and incidence of severe allergic reactions. Allergy. 2012;67(11):1451–1456. doi:10.1111/all.12012
5. Dhami S, Panesar SS, Roberts G, et al. Management of anaphylaxis: a systematic review. Allergy. 2013;69(2):168–175. doi:10.1111/all.12318
6. Calvani M, Anania C, Caffarelli C, et al. Food allergy: an updated review on pathogenesis, diagnosis, prevention and management. Acta Biomed. 2020;91(11–S):e2020012. doi:10.23750/abm.v91i11-S.10316
7. Höfer V, Martini M, Dölle‐Bierke S, Worm M, Bilò MB. Health‐related quality of life in food and venom induced anaphylaxis and role of influencing factors. Clin Exp Immunol. 2022;53(3):295–306. doi:10.1111/cea.14268
8. Grabenhenrich L, Hompes S, Gough H, et al. Implementation of anaphylaxis management guidelines: a register-based study. PLoS One. 2012;7(5):e35778. doi:10.1371/journal.pone.0035778
9. Licari A, Manti S, Marseglia A, et al. Food Allergies: current and Future Treatments. Medicina. 2019;55(5):120. doi:10.3390/medicina55050120
10. Eduardo Olivier C, Dos santos lima RP, Pinto Argentão DG. Group-specific multi-allergen sublingual/swallow immunotherapy improves the quality of life of polysensitized children and adults with allergic rhinitis. J Allergy Ther. 2013;04(06). doi:10.4172/2155-6121.1000148
11. Gupta RS, Warren CM, Smith BM, et al. Prevalence and severity of food allergies among US Adults. JAMA Network Open. 2019;2(1):e185630. doi:10.1001/jamanetworkopen.2018.5630
12. Alotiby AA, Alrashidi HE. Prevalence of food allergy and common food allergen among Saudi adults in Makkah region, Saudi Arabia. J Asthma Allergy. 2022;15:1851–1859. doi:10.2147/jaa.s394526
13. Knibb R, Huissoon A, Baretto R, et al. The impact of anaphylaxis on the quality of life and mental health of adults. Clin Exp Immunol. 2023;53:121. doi:10.22541/au.166028958.80617586/v1
14. Tayeb MMS, Koshak EA, Qutub MMA. Sensitization to common food allergens in Makkah city. Egypt J Hosp Med. 2009;35(1):288–294. doi:10.21608/ejhm.2009.17575
15. Althumiri NA, Basyouni MH, AlMousa N, AlJuwaysim MF, BinDhim NF, Alqahtani SA. prevalence of self-reported food allergies and their association with other health conditions among adults in Saudi Arabia. Int J Environ Res Public Health. 2021;18(1):347. doi:10.3390/ijerph18010347
16. Sullivan KM, Dean A, Soe MM. OpenEpi: A web-based epidemiologic and statistical calculator for public health. Public Health Rep. 2009;124(3):471–474. doi:10.1177/003335490912400320
17. Alosaimy R, Almaghrabi M, Basahal A, et al. Assessing the quality of life and environment safety for Saudi food allergic patients in the Makkah region, Saudi Arabia. Int J Med Develop Count. 942–949. doi:10.24911/IJMDC.51-1650156401
18. Knibb RC, Huissoon AP, Baretto R, et al. “It’s not an illness, it’s just bad luck”: The impact of anaphylaxis on quality of life in adults. Clin Exp Immunol. 2019;49(7):1040–1046. doi:10.1111/cea.13410
19. Saab IN, Jones W. Trends in Food Allergy Research, Regulations and Patient Care. Nutr Today. 2022;57(2):64–69. doi:10.1097/NT.0000000000000530
20. Gargano D, Appanna R, Santonicola A, et al. Food allergy and intolerance: a narrative review on nutritional concerns. Nutrients. 2021;13(5):1638. doi:10.3390/nu13051638
21. Salvati L, Vitiello G, Parronchi P. Gender differences in anaphylaxis. Curr Opin Allergy Clin Immunol. 2019;19(5):417–424. doi:10.1097/ACI.0000000000000568
22. Ellingwood SS, Kovalszki A. Effect of gender and special considerations for women in mastocytosis and anaphylaxis. Immun All Clin North Am. 2023;43(4):763–776. doi:10.1016/j.iac.2023.04.004
23. Francuzik W, Kraft M, Hofmeier KS, et al. Anaphylaxis in middle-aged patients. Allergol Select. 2021;5(01):133–139. doi:10.5414/ALX02216E
24. Aurich S, Dölle-Bierke S, Francuzik W, et al. Anaphylaxis in elderly patients—data from the European anaphylaxis registry. Front Immunol. 2019:10. doi:10.3389/fimmu.2019.00750
25. Nadhim LI. Investigation on the effect of age and gender on hypersensitivity reactions due to allergens injection in Iraqi population. Arch Razi Inst. 2022;77(1):359–365. doi:10.22092/ARI.2021.356679.1892
26. De Martinis M, Sirufo MM, Ginaldi L. Allergy and aging: an old/new emerging health issue. Aging Dis. 2017;8(2):162. doi:10.14336/AD.2016.0831
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.